

Abstract
Background:
Alopecia is a common complaint in dermatology clinics, and can be caused by a number of conditions, and has patterns that are different from that seen in adults.
Aim of Study:
No previous studies investigating the clinical types of hair loss in Jordan and its epidemiology. The ultimate aim was to provide a guide for the evaluation of hair loss commonly occurring in childhood in our environment.
Patients and Methods:
A total of 2800 children were seen at the dermatology clinics (Karak teaching hospital and Mutah university medical center) during January 2009 to October 2013 complaining of various clinical dermatological symptoms.
Results:
Of these patients, 210 children were complaining of hair loss and scalp disorders (7.5% of pediatric dermatology cases seen in Jordan). The most common presentation was asymptomatic patchy hair loss (40%). Other symptoms were scaly scalp (22.9%), diffuse hair loss (21.4%), change in hair texture and color (8.1%), pruritus (5.7%), and pain in the scalp (1%). Tinea capitis was the commonest causes of hair loss (40.0%) followed by alopecia areata (26.2%) and telogen effluvium (17.6%). Other common causes of hair loss were observed in this study, these include chronic diffuse form of hair loss, trichotillomania, and traction alopecia.
Conclusions:
As has been observed in this study, hair problem may be due to important nutritional deficiency such as iron and zinc elements, and this is very important problem to think of especially in developing countries. Therefore, hair examination by a pediatrician or dermatologist is an important part of the physical examination.
Keywords: Hair loss, no scarring alopecia, pattern of hair loss
INTRODUCTION
Alopecia or hair loss is a common complaint in dermatology clinics, and this can be caused by a number of conditions, reflected in a specific diagnosis. Although androgenetic alopecia is by far the most common forms of hair loss in adults, [1] dermatologists also see many people with other forms of alopecia. Similarly, hair loss is not uncommon problem in pediatric group [2] but has patterns that are different from that seen in adults. [2] In addition, this problem is of particular concern in pediatric group, as it is associated with more significant psychological consequences in this growing age group.
Common causes of hair loss in children [3,4] include telogen effluvium, tinea capitis, bacterial infections, traction alopecia, trichotillomania, alopecia areata. In addition to the previous, other less common causes of hair loss can be seen including [5] thyroid disorders, illnesses, such as systemic lupus erythematosus, diabetes mellitus, or iron deficiency anemia, malnutrition, structural abnormalities of the hair shaft that usually results in easy breakage and dry brittle hair.
Hair types are influenced by ethnic groups [6] and this varies from region to region and subsequently this may reflect itself on the variation of common and uncommon causes of hair loss. Therefore, this study was conducted to determine clinical types of hair loss in Jordan. There are no previous studies investigating the clinical types of hair loss in Jordan and its epidemiology. The ultimate aim was to provide a guide for the evaluation of hair loss commonly occurring in childhood in our environment.
MATERIALS AND METHODS
A total of 2800 children were seen consecutively at the dermatology clinics (Karak teaching hospital and Mutah university medical center) during January 2009 to October 2013 complaining of various clinical dermatological symptoms. Of these patients, 210 children who were complaining of hair loss and scalp disorders were included in the study. Informed consent was obtained from all patient parents. The data collected included age, sex, and clinical presentations (patchy or diffuse hair loss, presence of itching or scales, affected site, and the progression of the problem, and hair loss in the body other than the scalp). In addition, detailed history was taken about and hair grooming/habit tics, nail changes, other cutaneous changes, systemic diseases, family history of similar condition or autoimmune disease, and drug history.
Scalp examination included the skin of the scalp (presence of erythema, scales, and follicular plugging). Hair examination included the recording of hair color, texture, fragility, and examination of the hair root. In addition, Wood's light examination, skin and scalp scrapings for KOH (potassium hydroxide) smear and mycologic studies, and bacteriology were done for specific diagnostic cases. Microscopy for the shed hair and dermoscopy was done in some cases.
In addition to the scalp, other hairy sites were examined for hair loss (including eyebrows, eyelashes). Nail and teeth were examined for any abnormalities.
Other investigations carried out included complete blood count (CBC), serum iron, serum zinc, thyroid function test, antinuclear antibody (ANA), and autoantibodies, which were performed for further confirmation where necessary in some cases.
RESULTS
Of 2800 patients attending dermatology clinics at Karak teaching hospital and Mutah University Medical Center, 210 children (females, 120 (57.1%); males, 90 (42.8%)) had scalp and hair disorders. The age range was from 2 month to 16 years. This has been summarized in Table 1 and correlated with some of known clinical differential diagnosis for each symptom.
Table 1.
Presenting symptoms of hair loss in children (210 cases), correlated with the differential diagnosis for each presenting symptom
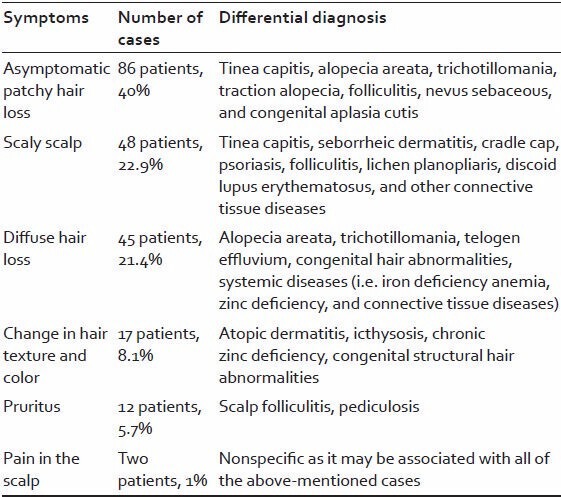
The most common presentation was asymptomatic patchy hair loss (86 patients, 40%). Other symptoms were scaly scalp (48 patients, 22.9%), diffuse hair loss (45 patients, 21.4%), change in hair texture and color (17 patients 8.1%), pruritus (12 patients, 5.7%), and pain in the scalp (two patients, 1%).
Tinea capitis was the most prevalent form of hair loss (85 patients, 40.5%). Males were affected more than females (males 49 cases, females 36 cases) with mean age of 6.4 years. The presentation was commonly as patchy hair loss with scales and erythema and solitary or multiple patches. Other presentations of tinea capitis were hair loss with black dot, seborrheic form, and kerion formation. Some of these patients had some elements of scarring due to delay in diagnosis and proper management. The diagnosis of these cases of tinea capitis was confirmed by KOH scrapping for the scales. Concurrent dermatophytosis affecting other parts of the body (face, trunk, and nails) occurred in 28% of cases.
Alopecia areata was the second form of hair loss, affecting (52 patients) 26.2% of the cases, with a male:female ratio of 3:2 and with mean age of 3.6 years. The earliest age of reporting alopecia areata in this study was 3 months (presented with multiple patches). The duration of the disease varied from 1-3 months at presentation. The presentation of patients was commonly with single or multiple patches of hair loss with no scales or erythema and with normal scalp appearance. Five cases of them had a diffuse hair loss at the time of the diagnosis of alopecia areata. Family history was positive for alopecia areata in 12 cases (seven of them had brothers or sisters with the same complaint). All cases were examined for body involvement with alopecia areata, which was positive in 10% of cases. Nail changes with pitting was seen in 27% of cases with the disease. All of the cases with alopecia areata were examined for other autoimmune diseases. Hypothyroidism was seen in three cases, diabetes mellitus in one case. Other autoimmune disease like vitiligo was seen in three cases.
Telogen effluvium, which occurs as diffuse non-scarring alopecia characterized by the shedding of hair resulting from the early entry of hair in the telogen phase, occurred in 37 children (17.6%). The concern in the study was to report the cases of telogen effluvium other than the cases of “telogen effluvium of the newborn,” which is common phenomena and considered as a physiological one. All of the cases had normal scalp and normal hair texture. This complaint was commonly from the females, as this problem more noticeable due to the habit of keeping hair long comparing to the males. The mean age of the presentation was 8 years and with duration of 4-6 months before the presentation to the clinic. To confirm the diagnosis of telogen effluvium, a microscopic examination of the shed hair revealed a typical bulb (i.e. depigmented bulb) of telogen hair. All the cases were investigated well for the causes of this. The most common cause was the frequent illnesses and high-grade fever that preceded the hair loss by 2-3 months, followed by iron deficiency anemia.
A total of 22 patients (10.5%) (mean age 6.2 years, 20 females and two males) had chronic diffuse hair loss with abnormal hair texture (with hair dryness and brittleness) with no other cutaneous manifestations. Specific history was taken to rule out other causes of hair loss (such as acute or chronic telogen effluvium). They have been healthy with no significant medical history. Skin examination revealed diffuse patchy alopecia (non-scarred) with very dry hair. Otherwise nothing was significant in the physical examination of these groups of patients, and similarly laboratory results with the exception of zinc level with the mean level of 52.3 μg/dl.
Trichotillomania was another and significant form of patchy hair loss in this study. A total of 15 cases (7%) presented of hair loss with broken hairs of varying lengths arranged in a circular pattern, with unaffected hairs surrounding the area of hair loss. The skin of the scalp was normal with no signs of inflammation. Some of the cases have severe degree of involvement in the entire scalp, sparing only marginal areas at the periphery. The mean age of presentation was 10 years with female predominance (10 cases are females). In addition to the scalp, three cases had eyebrows involvement. All cases of trichotillomania underwent dermoscopy examination. A recent article by Lencastre and Tosti [7] reviewed the role of dermoscopy in childhood hair disorders and noted fraying of ends, breakage at different lengths, and scratching and hemorrhaging as possible signs of trichotillomania. All cases in this study showed positive results by dermoscopy.
Traction alopecia was seen commonly in this study, most of the cases did not present specifically for this problem and all of them are females. But by physical examination, nearly 20% of the cases had some elements of this type of hair loss, occurring mainly around hair line. In some cases, hair cast had been identified. In addition, some cases showed follicular pustules and inflammation along the margin of alopecia.
There are several uncommon causes of hair loss identified in this study: Atopic dermatitis in 10 cases, folliculitis decalvans in 10 cases, congenital icthyosis in eight cases, nevus sebaceous in seven cases, Netherton syndrome in four cases, lichen planopliaris in four cases, aplasia cutis congenita in one, and large congenital melanocytic nevus in one.
DISCUSSION
Hair loss in children is an important complaint in dermatology clinics and considered as a challenge for dermatologists and pediatrician for reaching a proper diagnosis and therapy for their patients. In addition, this problem is annoying problem for the parents who are worrying from the total and irreversible hair loss to their children. There are common and uncommon causes for this complaint, [8,9] and this usually covers a broad differential diagnosis, and correct diagnosis is an important issue for proper diagnosis and prevention of further hair loss. Early management is needed, as this has its effect on development of normal mental and physical growth of children.
There are very few studies investigating the common and uncommon causes of hair loss in children, [9,10] and none to investigate this in Jordan. Specific environmental and cultural factors may reflect itself on the prevalence of specific types of hair loss in children. The clinical manifestations profile including age, sex, and clinical presentation (patchy or diffuse hair loss, presence of itching or scales, affected site, and the progression of the problem, and hair loss in the body other than the scalp) are important factors for the classification of the hair disease. [8,9,10] In this research, a classification of hair loss was based initially on the initial presentation and the differential diagnosis of this [Table 1], and this was considered as a guide for the evaluation of hair loss.
Hair loss and alopecia occur frequently in children. Scalp and hair disorders accounted for 7.5% of pediatric dermatology cases seen in Jordan. Both common and uncommon causes of hair loss were found in our series [Table 2].
Table 2.
Common and uncommon causes of hair loss in children (210 cases), correlated with the sex, age, common presentation, and specific diagnostic tests
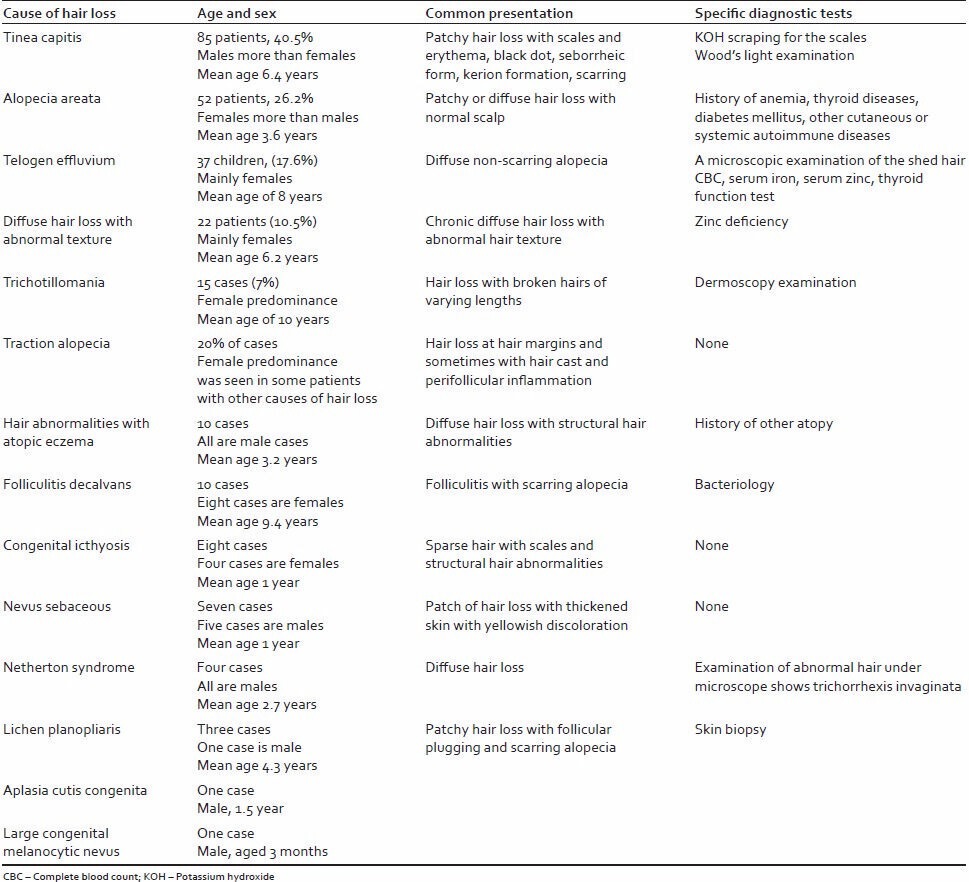
Tinea capitis was the commonest causes of hair loss (40.0%) and followed by alopecia areata (26.2%) and telogen effluvium (17.6%). Other common causes of hair loss were observed in this study but to a lesser degree than the previous three mentioned cases. These causes include chronic diffuse of hair loss, trichotillomania, and structural hair abnormalities. Traction alopecia was seen commonly in this study and was seen in association with other entities.
Tinea capitis (ringworm of the scalp) is one of the more common causes of hair loss, [10] but it is not difficult to recognize because of the association scalp findings (redness, hair loss, and a scaly border that may be itchy). But sometimes signs and symptoms can be more subtle though, with no scaling or itching, and broken hairs instead of hair loss (black dot tinea capitis). For these cases (KOH) mounted preparation may be needed to prove the diagnosis and to differentiate from alopecia areata. [11] Alopecia areata is one of the differential diagnoses of tinea capitis, although the diagnosis is not difficult to be done, as the scalp examination is normal in alopecia areata. But this story is not straightforward in our community in which parents may use some herbal products that may causes changes in the clinical picture and subsequently may affect early diagnosis.
The presentation with hair loss due to telogen effluvium was seen in nearly 17% of cases and was commonly due to preceding history of fever. Generally, telogen effluvium [12] resulting from a traumatic stimulus, which shows diffuse hair loss that does not produce clear areas. There are no broken-off hairs or exclamation-point hairs. There are no previous studies investigating this phenomena in children thoroughly, and it may be higher than what seen in adult population, as the common causes of telogen effluvium and iron deficiency anemia are common in children.
The new thing in this study was the chronic type of hair loss that was observed in this study and was due to zinc deficiency that was seen in our children despite absence of characteristic signs of zinc deficiency, and this may highlight the idea of how much was common the phenomena of zinc deficiency in Jordanian children, and there were no previous studies investigating this deficiency in our children, and this may be a future study investigating zinc deficiency in Jordanian children and the effect of this on the skin and the hair of children.
Trichotillomania was another form of hair loss seen in this research. It is a compulsive hair pulling, [13] which manifests with irregular areas of hair loss, and hairs of different lengths, and with no clear area of baldness. This type of disease has particular concern as it is associated with psychological abnormalities in children with this complain and need to be assessed by psychologist in addition to dermatologist; the skin is a mirror to many of internal disease and one of these is how we think.
Traction alopecia, which was seen in 20 of our cases and was associated with other types of hair loss, was usually not associated with internal pathology and was due to habits of traction of hair, and this was common in our environment in which there is trend to keep the hair of girls long and subsequently the hair should be tightened as a rule of the school.
Other uncommon causes of hair abnormalities have been observed in this study, and one of these was the lichen planopliaris in four cases (the sole presentation was scalp redness and hair loss with no involvement of glabrous skin). Atopic dermatitis is common disease in Jordan; 10 cases of our patients had hair abnormalities and three cases diagnosed to have Netherton syndrome (characterized by chronic skin inflammation, universal pruritus, severe dehydration, and a hair shaft defect (trichorrhexis invaginata) also known as “bamboo hair”).
In summary, hair loss in Jordan is not an uncommon problem and results from variety of causes. Early treatment and diagnosis is needed to prevent further hair loss and to avoid the irreversible hair loss and scarring alopecia. As has been observed in this study, hair problem may be due to important nutritional deficiency such as iron and zinc elements, and this is very urgent thing to think of especially in developing countries.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Banka N, Bunagan MJ, Shapiro J. Pattern hair loss in men: Diagnosis and medical treatment. Dermatol Clin. 2013;31:129–40. doi: 10.1016/j.det.2012.08.003. [DOI] [PubMed] [Google Scholar]
- 2.Hamm H. Acquired alopecia in childhood. Hautarzt. 2013;64:371. doi: 10.1007/s00105-013-2554-9. [DOI] [PubMed] [Google Scholar]
- 3.Sch Schroeder TL, Levy ML. Treatment of hair loss disorders in children. Dermatol Ther. 1997;2:84–92. [Google Scholar]
- 4.Mandt N, Vogt A, Blume-Peytavi U. Differential diagnosis of hair loss in children. J Dtsch Dermatol Ges. 2004;2:399–411. doi: 10.1046/j.1439-0353.2004.04044.x. [DOI] [PubMed] [Google Scholar]
- 5.Castelo-Soccio LA. Hair manifestations of systemic disease. Curr Probl Pediatr Adolesc Health Care. 2012;42:198–203. doi: 10.1016/j.cppeds.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 6.Morand JJ. Skin color, hair types and phenotype diversity: Races, ethnic groups and populations in the medical literature. Med Trop (Mars) 2008;68:213–4. [PubMed] [Google Scholar]
- 7.Lencastre A, Tosti A. Role of Trichoscopy in children's scalp and hair disorders. Pediatr Dermatol. 2013;30:674–82. doi: 10.1111/pde.12173. [DOI] [PubMed] [Google Scholar]
- 8.Nnoruka EN, Obiagboso I, Maduechesi C. Hair loss in children in South-East Nigeria: Common and uncommon cases. Int J Dermatol. 2007;46:18–22. doi: 10.1111/j.1365-4632.2007.03457.x. [DOI] [PubMed] [Google Scholar]
- 9.Sarifakioglu E, Yilmaz AE, Gorpelioglu C, Orun E. Prevalence of scalp disorders and hair loss in children. Cutis. 2012;90:225–9. [PubMed] [Google Scholar]
- 10.El-Khalawany M, Shaaban D, Hassan H, Abdalsalam F, Eassa B, Abdel Kader A, et al. A multicenter clinicomycological study evaluating the spectrum of adult tinea capitis in Egypt. Acta Dermatovenerol Alp Panonica Adriat. 2013;22:77–82. [PubMed] [Google Scholar]
- 11.Mochizuki T. Diagnosis of cutaneous fungal infection. Nihon Ishinkin Gakkai Zasshi. 2009;50:195–8. doi: 10.3314/jjmm.50.195. [DOI] [PubMed] [Google Scholar]
- 12.Grover C, Khurana A. Telogen efflivium. Indian J Dermatol Venereol Leprol. 2013;79:591–603. doi: 10.4103/0378-6323.116731. [DOI] [PubMed] [Google Scholar]
- 13.Huynh M, Gavino AC, Magid M. Trichotillomania. Semin Cutan Med Surg. 2013;32:88–94. doi: 10.12788/j.sder.0007. [DOI] [PubMed] [Google Scholar]