

Abstract
Objective
To examine factors that influence the amount of time and information pharmacy personnel provide to patients at the drive-through and walk-in counseling areas.
Methods
On-site observational data collection in 22 community pharmacies by pharmacy students. Information included observable patient characteristics such as gender, age range, English proficiency, and mobility impairment; encounter characteristics such as the type of prescription, and whether the patient was acknowledged; and counseling characteristics such as the types of counseling information conveyed and length of time for each encounter.
Key findings
Patient-pharmacist encounters were documented at the drive-thru and walk-in counseling areas 961 and 1098 times, respectively. Pharmacists spent less time, and technicians more time, with patients at the drive-through counseling area. The amount of information provided to patients was significantly affected by the type of prescription the patient was receiving (new vs. refill). Patients who had a new prescription were two times more likely to receive more information from the pharmacy personnel. There was a significant difference between the amount of counseling provided to patients at the drive-through and walk-in counseling area (RR 0.92, 95% CI: 0.86-1.00). Patients at the drive-through received a lower amount of information relative to patients using the walk-in. The amount of information provided to patients was affected by the level of pharmacy busyness (RR 0.96, 95% CI: 0.95-0.99).
Conclusions
Providing patient care at the drive-through counseling area may negatively influence quality of patient care. To improve quality of pharmacy drive-through services, there may be a need for standardization of drive-through services in pharmacies.
Keywords: Drive-through counseling areas, community pharmacy, patient encounters, Andersen behavioral model of health services utilization
Introduction
Drive-through services are commonly used in many industries such as fast food restaurants and banks to promote efficiency and render faster services. The use of drive-through community pharmacies began in the 1990s in the United States to promote faster dispensing of medications and improve patient satisfaction. However, faster services do not always translate to safer and higher quality patient care.Despite years of experience with drive-through services in community pharmacies, little is known about pharmacy-patient encounters at the drive-through counseling area. There is limited research on the use of drive-through services in community pharmacies. Studies exploring the differences between patient-pharmacist interaction at the drive-through and traditional walk-in counseling area of a pharmacy found that pharmacist interaction with patients might be richer when the walk-in counseling area is used, particularly for patients with limited English proficiency [1], [2] and [3].
Several studies have reported a positive link between pharmacist counseling and patients’ adherence to medications [4-7]. Findings from these studies suggest that a lack of patient counseling by pharmacists may result in reduced medication adherence, treatment failure and waste of health resources [8]. Another important aspect of patient-pharmacy encounters is the amount of time spent with patients by pharmacists and technicians. Although these findings may not be generalized to community pharmacies,Tarn et al., found that the amount of time a physician spent on communication with the patient, and quality of the communication, was positively correlated with a more comprehensive discussion of important counseling elements [9]. Provision of poor counseling at the drive-through and hurried patient care may not afford patients the opportunity to obtain necessary information to appropriately use their medications. Inappropriate counseling could negatively impact patient care or even lead to adverse drugs events or drug interactions [10]. Another study has suggested a possible relationship between time spent with patients at the drive-through in community pharmacies and quality of patient counseling [1].
The aim of this study was to explore the factors that are associated with the amount of information provided to patients and amount of time pharmacists or technicians spend with patients at the drive through compared to the walk-in counseling area. This study will provide insight on the factors that are associated withthe quality of patient interaction in community pharmacies at the drive-through and walk-in counseling area to improve pharmacy practice.
This study had two objectives. The first objective was to describe the factors that might influence the time spent with patients at the drive-through and walk-in counseling area. The second objective was to determine the factors that could influence the amount of information patients received at the drive-through and walk-in counseling area.
Methods
For this study, a walk-in counseling area was denoted as pharmacy interaction with patients inside the pharmacy typically at the pharmacy counter or semi-private counseling area as opposed to use of the drive-through counseling area where patients drive up in their cars and interact with pharmacy personnel via a microphone or an opening counseling area.
Community pharmacists, with both walk-in access for at least one individual and drive through access for at least one car at a time, and who were University of Wisconsin rotation site preceptors, were invited via a telephone call and follow-up mailed letter to take part in this study. Fourth year students from the University of Wisconsin, School of Pharmacy were invited to participate in the study if they were assigned to a participating pharmacy during July 2009 through May 2010. The students were required to complete human subjects and one-on-one data collection training prior to participating in the study.
Observations
An observation form, pilot tested in a previous study [1], was revised to include information that may be conveyed during patient counseling, and perceived pharmacy busyness [8]. (see appendix A).
Both the drive-thru and walk-in counseling areas were observed for each pharmacy. Twenty-three student observers recorded encounters on the standardized form and timed encounters using a stop watch. The elements observed included patient, encounter, and counseling characteristics. The variables for patient characteristics that were observed and recorded included gender, age range, mobility impairment, limited English proficiency, accompanying passengers, smoking status during the encounter, and cell phone use during the encounter. Encounter characteristics included type of prescription, level of pharmacy busyness, whether the patient was acknowledged and by whom. Counseling characteristics included information items conveyed to patients during counseling, number of questions patients asked, and time. The amount of information provided to each patient during counseling was aggregated as a composite score of information items provided to the patient during each pharmacy-patient interaction.
Student observers were each asked to collect 50 encounters at the walk-in counseling area, and 50 encounters at the drive-thru counseling area. While student observers were asked to dedicate periods of time to collect data, the days of the week and the length of time were not prescribed. During data collection periods, data was recorded for every sequential patient who approached the drive-thru or walk-in counseling areas, and observers were dedicated exclusively to data collection (i.e., did not have dispensing or patient care responsibilities).
Patients were observed when they arrived at the drive-thru counseling area or came to the front of the line at the walk-in counseling area. Students recorded whether the patient was acknowledged upon approaching the counseling area and by whom. A stop watch was started when pharmacy personnel first made verbal contact with the patient. If a non-pharmacist first made verbal contact, the student made note of the time at which the patient began interacting with the pharmacist. When the encounter was concluded, the observer stopped timing and recorded the start and stop times.
Measures
Conceptual framework
The Andersen Behavioral Model of Health Services utilization [11] was used as the guiding framework for this study. As shown in figure 1, this framework stipulates how use of health care is explained by predisposing, enabling, and needs factors. We hypothesized there are different factors that are associated withpharmacy-patient interactions at the drive-through and walk-in counseling area pharmacy services, and this relationship is explained by predisposing, enabling, and needs factors.
Figure 1.
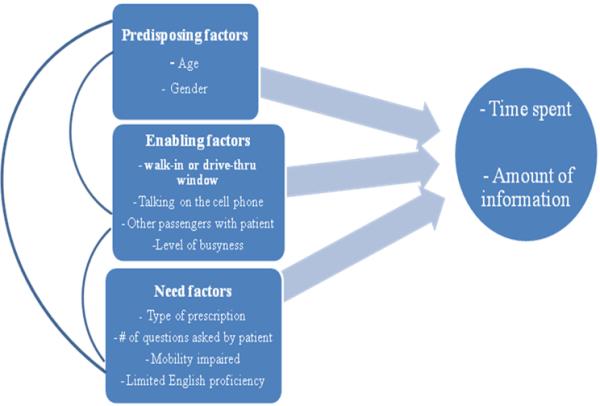
Adaptation of Andersen Behavioral Model to Pharmacy Services Utilization
Dependent variables
Our primary outcome variables include time (in seconds) spent by the pharmacist or technician with the patient and a total count of the amount of information provided to patients. The amount of information was measured by the total number of counseling points for each patient,includingverification of patient name, medication name, indication or drug purpose, drug directions for use, possible adverse effects, onset of action and other precautions. These outcome variables were the indicators for quality of pharmacy-patient interactions at the drive-through or walk-in counseling area based on the Omnibus Budget Reconciliation Act of 1990 (OBRA ’90) [12] and has been used in a previous study on drive-through pharmacies [1].
Independent variables
The primary study independent variable was the location of interaction,which was coded as walk-in or drive-through.
Predisposing variables were patient characteristics that might affect the pharmacy-patient interaction at the drive-through or walk-in counseling area. This study included observed age range and gender which are categorical variables. Observed age range was coded into younger than forty years old, between forty and sixty, and older than sixty.Gender was coded as dummy variable (Male =1, female = 0).
Enabling variables were factors that either facilitate or impede pharmacy-patient interaction at the drive-through or walk-in counseling area, including talking on the cell phone, presence of accompanying people with the patient, and level of pharmacy busyness. The variable “level of pharmacy busyness” was initially conceptualized in a study by Svarstad et al. in 2004 [8] and was estimated in this study using a scale ranging from 0 (no patients are waiting, pharmacy is calm and workflow is slow or non-existent) to 6 (rush hour during a holiday and the pharmacy has many outstanding issues to address). In order to interpret level of pharmacy busyness, the variable in the dataset wasclassified into low (0-1), medium (2-3), and high (4-5). Other enabling variables, including talking on the cell phone and presence of accompanying people with the patient, were coded as dummy variables (yes =1, no = 0).
Need variables were variables that may necessitate more pharmacy-patient interaction at the drive-through or walk-in counseling area. The need variables were estimated by type of prescription, mobility impaired, and limited English proficiency. Type of prescription was categorized into having at least one new prescription and refills only. If patients had at least one new prescription this was coded as “1” and if the patients had all refills as “0”. Limited English proficiency was coded as a dummy variable (yes = 1, no = 0).
The models shown below were used to examine which variables may affect pharmacy-patient interactions at the drive through or walk-in counseling area.
Model 1: Pharmacist time = Predisposing variables + Enabling variables + Need variables
Model 2: Technician time = Predisposing variables + Enabling variables + Need variables
Model 3: Amount of information = Predisposing variables + Enabling variables + Need variables
Data analysis
STATA 11.1 (Stata, College Station, TX)wasused to conduct the descriptive statistics for all variables and to conduct all multivariate models.Descriptive analysis was first conducted to compare the patient characteristics and pharmacy encounters between drive-through and walk-in counseling areas. Bivariate and stepwisenegative binomial regression analysis were further used to identify the relationship between pharmacy services location and outcome variables, and how this relationship was associated with predisposing, enabling, and needs variables. A negative binomial regression was used in this study due to overdispersion, which indicates that the Poisson regression assumption was violated [13] and [14].
To assess the different factors that are associated withpharmacy personnel time and amount of information provided to patients at the drive-through and walk-in counseling area, this analysis reports rate ratios as the exponentiated values of the regression coefficients and the 95 % confidence intervals of the rate ratios.
Results
Data on patient-pharmacist encounters were collected from 23 community pharmacies from July 2009 through May 2010. However, one data collection binder with recorded information was lost in the postal mail, resulting in a total of 22 community pharmacies. Of the 22 community pharmacies, 12 (55%) were chain and 10 (45%) were independently owned.
The data collected consisted of 2,059 patient-pharmacy encounters, where encounter is the unit of analysis. Of the anticipated 1,100 drive-through and 1,100 walk-in counseling area encounters, a total of 961 (87%) and 1,098 (99%) encounters were documented for the drive-through and walk-in counseling areas, respectively. Table 1 presents basic characteristics of patients using both counseling areas. According to the descriptive statistics, there were significant differences in pharmacy personnel interactions with patients at the drive-through and walk-in counseling area. Patients using the drive-through and walk-in counseling areas were similar in terms of gender but patients older than 60 years were more likely to use the walk-in than drive-through counseling areas (28% vs. 15.7%). There were more encounters at the drive-through with patients with other companions such as children or adults than at the walk-in counseling area (27.9% vs. 13.7%). Patients using their cell phone during the interactions were more likely to use the drive-through counseling area (3.5% vs. 1.2%). On average, pharmacists interactions with patients was 32 seconds longer at the walk-in counseling area (97.2±114.1 seconds) than at the drive-through counseling area (P < 0.001). Technicians spent an average of 36 seconds longer with patients at the drive-through counseling area (84.4±108.7 seconds) than at the walk-in counseling area (P < 0.001). The average amount of drug information provided to the patient by pharmacy personnel was higher at the walk-in counseling area.
Table 1.
Differences in patient encounters at the drive-through and walk-in windows
| Drive-through window | Walk-in window | P | |
|---|---|---|---|
| (n= 961) | (n=1098) | ||
| % | % | ||
| Gender | 0.083 | ||
| Women | 62.9 | 59.2 | |
| Men | 37.1 | 40.8 | |
| Observed age range (years) | <0.001 | ||
| <40 | 37.4 | 27.1 | |
| >60 | 15.7 | 28.2 | |
| Mobility impaireda | <0.001 | ||
| Yes (required assistance) | 0.9 | 1.4 | |
| No (ambulatory without assistance) | 81.1 | 97.2 | |
| Unknown | 18 | 1.5 | |
| Individual accompanying patient (in the store or in the car) | <0.001 | ||
| Children or adults | 27.9 | 13.7 | |
| Patient was alone | 72.1 | 86.3 | |
| Limited English proficiency | 0.024 | ||
| Yes (able to counsel) | 0.6 | 1.8 | |
| Yes (needed interpreter) | 0 | 0.2 | |
| No | 99.4 | 98 | |
| Accepted patient counseling when offereda | 0.005 | ||
| Yes | 86.7 | 90.9 | |
| No | 13.3 | 9.1 | |
| Talking on cell phone during encounter | 0.001 | ||
| Yes | 3.5 | 1.2 | |
| No | 96.5 | 98.8 | |
| Type of prescription | 0.323 | ||
| At least one new prescription | 21.9 | 24.5 | |
| All refill prescriptions | 69.9 | 66.6 | |
| Unknown | 8.2 | 8.9 | |
| Level of pharmacy busyness | 0.001 | ||
| Low | 52 | 54.1 | |
| Medium | 38.7 | 41 | |
| High | 9.3 | 4.9 | |
| Technician time with patient ( in seconds) | <0.001 | ||
| Mean | 84.4 | 47.5 | |
| S.D | 108.7 | 90.5 | |
| C.I | 77.3 - 91.4 | 41.9 - 52.9 | |
| Pharmacist time with patient( in seconds) | <0.001 | ||
| Mean | 65.4 | 97.2 | |
| S.D | 78.7 | 114.1 | |
| C.I | 60.3 - 70.5 | 90.2 - 104.1 | |
| Amount of information provided to patient | <0.001 | ||
| Mean | 1.9 | 2.2 | |
| S.D | 1.8 | 1.8 | |
| C.I | 1.8 - 2.1 | 2.1-2.4 | |
Abbreviations used:
100% of patients were offered counseling by pharmacy personnel.
Table 2 reports the results for the stepwise regression analysis of the predisposing, enabling and need factors hypothesized to be associated with the amount of time pharmacists spent with patients at the drive-through and walk-in counseling area. As shown in Table 2, after controlling for all the variables in the model, age as a predisposing variable had a significant effect on amount of time pharmacists spend with patients at the drive-through or walk-in counseling area. The key enabling variables affecting amount of time pharmacists spent with patients were location of interaction (drive-through or walk-in) and level of pharmacy busyness. Pharmacists spent less time with patients at the drive-through compared to the walk-in counseling area (RR: 0.70, 95% confidence interval [CI]: 0.62-0.78). The results also suggest that as the level of pharmacy busyness increased, pharmacists spent less time with the patient (RR: 0.80, 95% [CI]: 0.77 -0.84). After controlling for other variables in the model, the need variable, having a new prescription was significantly associated with the amount of time pharmacists spent with patients (RR 1.72, 95% [CI]: 1.51 -1.95). This suggests that pharmacists spend more time with patients who have new prescriptions than those who have refill prescriptions.
Table 2.
Factors associated with Pharmacist interaction time with patients at the drive-through and walk-in window
| Variable | Unadjusted | P | P/E | P/E/N |
|---|---|---|---|---|
|
Predisposing variables
| ||||
| Observed age range | 1.07 (1.00-1.16) | 1.09* (1.01-1.17) | 1.07 (0.99-1.16) | 1.11 (1.02-1.20) |
| Male | 0.88* (0.79-0.99) | 0.90* (0.78-0.97) | 0.83* (0.75-0.93) | 0.91 (0.81-1.02) |
| Female | - | 1 | 1 | |
| Enabling variables | - | |||
| Drive-through interaction | 0.67* (0.61-0.75) | 0.70* (0.62-0.78) | 0.75* (0.67-0.84) | |
| Walk-in interaction | - | 1 | 1 | |
| Talking on the cell phone | 0.83 (0.58-1.19) | 0.94 (0.65-1.34) | 0.88 (0.60-1.30) | |
| Not talking on the cell phone | - | 1 | 1 | |
| Passengers with the patient | 0.88 (0.77-1.00) | 0.95 (0.82-1.09) | 0.97 (0.83-1.12) | |
| No passengers with the patient | - | 1 | 1 | |
| Level of pharmacy busyness | 0.82* (0.78-0.86) | 0.82* (0.78-0.85) | 0.80* (0.77-0.84) | |
| Need variables | - | - | ||
| New prescription | 1.66* (1.47-1.87) | 1.72* (1.51-1.95) | ||
| Refill prescription | - | 1 | ||
| Mobility impaired | 1.36 (0.82-2.25) | 1.12 (0.66-1.85) | ||
| Non-mobility impaired | - | 1 | ||
| Limited English proficiency | 1.21 (0.76-1.94) | 0.63 (0.38-1.05) | ||
| English proficient | - | 1 | ||
Note: RR = rate ratio; () is 95% confidence interval
is p < .05; P is the model with only predisposing variables, P/E is the model with both predisposing and enabling variables only, P/E/N is the model with the predisposing, enabling, and need variables.
Table 3 reports the results for the stepwise regression analysis for the predisposing, enabling and need factors hypothesized to be associated with the amount of time technicians spent with patients at the drive-through or walk-in counseling area. The unadjusted bivariate analysis of each variable in the model suggests that the significant variables affecting amount of time technicians spent with the patient were interaction at the drive-through, having other passengers with the patient, level of pharmacy busyness, and having a new prescription. When accounting for the predisposing, enabling, and need factors the only significant enabling variables were drive-through interaction (RR 1.54, 95% [CI]: 1.18 −2.00) and level of pharmacy busyness (RR 1.13, 95% [CI]: 1.02 −1.24); and the only significant need variable is having a new prescription (RR 1.43, 95% [CI]: 1.07 −1.91). Introducing the need variables resulted in a greater reduction of the rate ratio of the drive-through interaction than the addition of the enabling variables. According to the multivariate analysis, there was a significant difference in the time technicians spend with patients at the drive-through after controlling for confounding factors in the model. Technicians spend more time with patients at the drive-through compared to the walk-in counseling area.
Table 3.
Factors associated with Technician interaction time with patients at the drive-through and walk-in window
| Variable | Unadjusted | P | P/E | P/E/N |
|---|---|---|---|---|
|
Predisposing variables
| ||||
| Observed age range | 0.91 (0.80-1.04) | 0.92 (0.80-1.05) | 1.02 (0.88-1.16) | 1.07 (0.90-1.27) |
| Male | 0.88 (0.72-1.08) | 0.90 (0.73-1.10) | 0.84 (0.68-1.03) | 0.83 (0.64-1.00) |
| Female | - | 1 | 1 | 1 |
| Enabling variables | - | |||
| Drive-through interaction | 1.78* (1.46-2.16) | 1.70* (1.38-2.08) | 1.54* (1.18-2.00) | |
| Walk-in interaction | - | 1 | 1 | |
| Talking on the cell phone | 1.25 (0.65-2.41) | 1.09 (0.56-2.12) | 1.30 (0.54-3.08) | |
| Not talking on the cell phone | - | 1 | 1 | |
| Passengers with the patient | 1.43* (1.12-1.83) | 1.21 (0.94-1.56) | 1.22 (0.88-1.69) | |
| No passengers with the patient | - | 1 | 1 | |
| Level of pharmacy busyness | 1.13* (1.04-1.21) | 1.09* (1.03-1.21) | 1.13* (1.02-1.24) | |
| Need variables | - | - | 1 | |
| New prescription | 1.36* (1.05-1.76) | 1.43* (1.07-1.91) | ||
| Refill prescription | - | 1 | ||
| Mobility impaired | 1.30 (0.51-3.36) | 1.10 (0.36-3.37) | ||
| Non-mobility impaired | - | 1 | ||
| Limited English proficiency | 0.81 (0.34-1.92) | 0.94 (0.31-2.89) | ||
| English proficient | - | 1 | ||
Note: RR = rate ratio; () is 95% confidence interval
is p < .05; P is the model with only predisposing variables, P/E is the model with both predisposing and enabling variables only, P/E/N is the model with the predisposing, enabling, and need variables.
Table 4 shows the results for the multivariate analysis of factors associated with amount of information providedto the patient at the drive-through or walk-in counseling area. After controlling for all variables, there was a significant difference between amount of counseling provided to patients at the drive-through and walk-in counseling area (RR 0.92, 95% CI: 0.86-1.00). Patients at the drive-through counseling area may have received less information relative to patients using the walk-in counseling area. Also, the amount of information provided to patients is affected by level of pharmacy busyness (RR 0.96, 95% CI: 0.95-0.99). The results suggest that the need variable having the most significant effect on the amount of information provided to a patient was having a new prescription (RR 2.74, 95% CI: 2.56-2.94). Patients who had a new prescription were giventwice the amount of information from pharmacy personnel.
Table 4.
Factors associated with amount of information received by patients at the drive-through and walk-in window
| Variable | Unadjusted | P | P/E | P/E/N |
|---|---|---|---|---|
|
Predisposing variables
| ||||
| Observed age range | 0.97 (0.93-1.03) | 0.97 (0.91-1.02) | 0.98 (0.93-1.04) | 1.05 (0.99-1.10) |
| Male | 0.87* (0.81-0.95) | 0.92* (0.85-0.99) | 0.87* (0.80-0.94) | 0.95 (0.88-1.02) |
| Female | - | 1 | 1 | 1 |
| Enabling variables | - | |||
| Drive-through interaction | 0.86* (0.80-0.93) | 0.86* (0.93-1.03) | 0.92* (0.86-1.00) | |
| Walk-in interaction | - | 1 | 1 | |
| Talking on the cell phone | 0.89 (0.69-1.16) | 0.91 (0.70-1.20) | 1.02 (0.77-1.34) | |
| Not talking on the cell phone | - | 1 | 1 | |
| Passengers with the patient | 1.03 (0.93-1.13) | 1.06 (0.97-1.17) | 0.96 (0.88-1.06) | |
| No passengers with the patient | - | 1 | 1 | |
| Level of pharmacy busyness | 0.96* (0.93-0.99) | 0.96* (0.93-0.00) | 0.96* (0.94-0.99) | |
| Need variables | - | - | 1 | |
| New prescription | 2.68* (2.51-2.86) | 2.74* (2.56-2.94) | ||
| Refill prescription | - | 1 | ||
| Mobility impaired | 1.30 (0.94-1.81) | 1.09 (0.81-1.46) | ||
| Non-mobility impaired | - | 1 | ||
| Limited English proficiency | 0.84 (0.60-1.19) | 0.85 (0.61-1.20) | ||
| English proficient | - | 1 | ||
Note: Rate ratios reported; () is 95% confidence interval
is p < .05; P is the model with only predisposing variables, P/E is the model with both predisposing and enabling variables only, P/E/N is the model with the predisposing, enabling, and need variables.
Table 5 reports a summary of the significant predictors of amount of time spent and amount of information when analyzing the drive-through and walk-in models separately, controlling for all variables in the model. At the drive-through counseling area, the amount of time the pharmacist spent with a patient was influenced mainly by two factors: level of pharmacy busyness (RR 0.75, 95% CI, 0.70-0.81) and having a new prescription (RR 1.68, 95% CI, 1.35-2.09). At the walk-in counseling area, time spent by pharmacist was influenced only by three factors: level of pharmacy busyness (RR 0.84, 95% CI, 0.79-0.89), having a new prescription (RR 1.74, 95% CI, 1.48-2.05), and observed age of the patient (RR 1.13, 95% CI, 1.02-1.25). The pharmacist possibly spent less time with the patient at the drive-through and walk-in counseling area as level of pharmacy busyness increased. The pharmacist also spent more time with patients who had at least one new prescription. There were no significant predictors of amount of time technician spent with patient at the walk-in counseling area. However, technicians spent significantly more time with patients at the drive-through counseling area as the level of pharmacy busyness increased (RR 1.16, 95% CI, 1.04-1.31). At both the drive-through and walk-in counseling area, the variable “having a new prescription” (patients receiving one or more of their medications for the very first time) significantly increased the amount of information that pharmacy personnel provided to patients. When a patient had a new prescription the pharmacist was more likely to spend more time counseling the patients on how to use their medication by providing information such as the purpose of the drug, the name of the drug, possible side effects, and information on how and when to use the drug.
Table 5.
Significant predictors for time spent and amount of information at the drive-through only and walk in window only when controlling for all variables in the models
| Drive-through model only | Walk-in model only | |
|---|---|---|
| Pharmacist time | Level of pharmacy busyness 0.75* (0.70-0.81) | Level of pharmacy busyness 0.84* (0.79-0.89) |
| New prescription 1.68* (1.35-2.09) | New prescription 1.74* (1.48-2.05) | |
| Not significant | Observed age range 1.13* (1.02-1.25) | |
| Technician time | Level of pharmacy busyness 1.16* (1.04-1.31) | Not significant |
| Amount of information | Level of pharmacy busyness 0.93* (0.90-0.98) | Not significant |
| New prescription 2.78* (2.47-3.11) | New prescription 2.73* (2.50-2.98) | |
| Not significant | Observed age range 1.08* (1.02-1.15) | |
Note: Rate ratios reported; () is 95% confidence interval
is p < .05;
Discussion
Main Findings
Results from this study indicate that there are different factors that might influence pharmacy encounters with patients at the drive-through and walk-in counseling areas. Some of the variables in the model were consistently significantly associated with the amount of time pharmacists and technicians spend with patients (having a new prescription, level of pharmacy busyness, and using the drive-through counseling area). The predisposing factor included in the model (observed age) appears to significantly impact time pharmacists spend with patients and the amount of information they receive, particularly at the walk-in counseling area. The enabling variable, drive-through interaction was a significant factor in all of the models analyzed.
Strengths and Limitations of the Study
This study is the first to reveal the key factors, such as pharmacy busyness, that are associated with the time pharmacy personnel spend with patients at the drive-through and the amount of information patients receive about their medications using the Andersen Behavioral Model of Health Services Utilization [11]. However, this study includes only encounters with patients and pharmacy personnel in pharmacies in one state. Also, the time or days when the data were collected, which were not recorded, could impact the results. As a result, the generalizability of findings may be limited.
The design and methods chosen for this study had several advantages. First, by documenting patient encounters at both the drive-through and walk-in counseling areas of each pharmacy, we attempted to hold constant the personnel that would interact with patients as well as any organizational structure or policy that might externally influence the patient interaction. Second, unlike previous studies that surveyed pharmacists regarding their perceptions of advantages and disadvantages of having a drive-through counseling area, this study sought to collect empirical data on characteristics of the pharmacy-patient interaction, recognizing that pharmacists’ perceptions may not be consistent with actual practice. However, one limitation of this design is a Hawthorne effect, in which pharmacy staff may havechanged their behavior as a result of being observed. A second limitation to this design is the potential variability between scorers. These effects were not measured. Lastly, given the amount of time that student observers were provided to collect data, we were unable to record 50 encounters per pharmacy at the drive-through counseling area. This was due to some lower volume pharmacies having significantly less patients presenting at the drive-through counseling area (one observer indicated that only three patients on average received their prescriptions at the drive-through counseling area at his pharmacy).
Implications of time spent at the walk-in and drive-through counseling areas
This study showed that pharmacists spend more time with patients at the walk-in counseling area, while technicians spend more time with patients at the drive-through counseling area. Our findings are consistent with previous research that found that pharmacists interact with patients for the majority of the total encounter at the walk in counseling areas, whereas they only spent a small proportion of total encounter time with patients at the drive through counseling areas (average of 41 seconds of 187 second total encounter)[1]. These findings support the hypothesis that pharmacists might perceive the drive-through counseling area to be an inefficient means of providing adequate patient counseling and suggest that technicians specifically attend more to the needs of patients at the drive-through. This has important implications, as patients who use the drive-through may be less likely to receive adequate counseling by the pharmacist. This could result in lower quality of care provided to patients at the drive-through counseling area. Future research should confirm this finding in a larger, more generalizable study. This study also helps to identifythe key factors that are associated withpharmacy personnel's interaction with patients at the drive-through or walk-in counseling area. Two important factors that are significantly associated with interactions pharmacy personnel have with patients are the type of prescription and level of pharmacy busyness. A finding not anticipated in this study was that as the level of pharmacy busyness increased, the amount of time pharmacists spent with patients reduced while the amount of time technicians’ spent with patients increased. Pharmacists might perceive the walk-in counseling area to be a more efficient use of their time and frequently delegate drive-through services to technicians. Another key finding of this study was that patients were more likely to be providedless information at the drive-through than at the walk-in counseling area. Pharmacists and technicians spent significantly less time with patients who had refill prescriptions and more time with patients who had at least one new prescription. The differences in time spent with each patient could be influenced by the pharmacy personnel's perceived patient need. It might be necessary to standardize or regulate quality of care at the drive-through counseling area to ensure patient needs are adequately met. Many other factors could influence time spent with patients at the drive-through and walk-in counseling area such as weather conditions, or time when the data was collected [1]. Future research is needed to determine other factors that influence the use of the drive-through counseling area, possibly examining patients’ reasons for selecting the drive-through rather than the walk-in counseling area.
In order to improve quality of pharmacy drive-through services, there may be a need for standardization of drive-through services in pharmacies. This study has important implications because patients who use the drive-through are likely to be providedless counseling by the pharmacist, and thuslower quality of care. Although the drive-through counseling area provides faster access to health care services for patients, the quality of medication communication between the pharmacist and the patient might also be lower. Our findings indicate that pharmacies may need to take steps to ensure pharmacists provide more adequate counseling to patients at the drive-through to improve quality of care especially when the pharmacy is busy. These steps could include a rethinking about the physical layout of the pharmacy as well as additional technician training to provide services at the drive-through location. This could help to ensure that not only technicians attend to patients at the drive-through counseling area. Drive-through encounters should entail more pharmacist-patient interactions to increase the exchange of information and overall patient care. This is important because drive-through services can serve as a valuable resource for particular patient populations such as the disabled and the elderly who have difficulty ambulating and mothers who do not want to bring sick children into the pharmacy.
Conclusion
Despite years of experience with drive-through services in community pharmacies, little is known about pharmacy-patient encounters at the drive-through counseling area. This study found that multiple factors are associated withfor how long pharmacists and technicians interact with patients in pharmacies and raisesconcerns that pharmacists may be delegating care to technicians for patients at the drive-through counseling area which could affect the quality of their care. This study also suggests that the amount of time pharmacists and technicians spend with patients is greatly affected by how busy the pharmacy is, and the type of prescription being dispensed.
Acknowledgement
All authors had complete access to the study data that support the publication this manuscript. All authors participated in writing the manuscript. The corresponding author was responsible for conceptualizing the research questions, conceptual framework, data analysis, and facilitating revisions of the manuscripts. Co-author Michelle Chui, was responsible for conceptualizing data collection methods used and writing and revising parts of the manuscript. Co-author Jia Pu took active part in data analysis and writing and revising parts of the manuscript.
Funding
This research received no specific grant from any funding agency in the public, commercial or notfor-profit sectors. Michelle A. Chui was supported by the Clinical and Translational Science Award (CTSA) program, through the NIH National Center for Advancing Translational Sciences (NCATS), grant UL1TR000427. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Appendix A


Footnotes
Conflict of Interest
The authors declare that they have no conflicts of interest to disclose.
Ethical Approval
This study was approved by the University of Wisconsin-Madison, Institutional Review Board.
Contributor Information
Olufunmilola K. Odukoya, Social & Administrative Sciences Division, School of Pharmacy, University of Wisconsin, Madison, Wisconsin, USA at 777 Highland Ave, Madison, WI 53705, USA..
Michelle A. Chui, Social & Administrative Sciences Division, School of Pharmacy, University of Wisconsin, Madison, Wisconsin, USA at 777 Highland Ave, Madison, WI 53705, USA. Tel: 608-262-0452. Fax: 608-262-5262..
Jia Pu, Social & Administrative Sciences Division, School of Pharmacy, University of Wisconsin, Madison, Wisconsin, USA at 777 Highland Ave, Madison, WI 53705, USA. Tel: 608-262-4723. Fax: 608-262-5262..
References
- 1.Chui MA, Halton K, Peng JM. Exploring patient-pharmacist interaction differences between the drive-through and walk-in windows. J Am Pharm Assoc. 2009;49(3):427–31. doi: 10.1331/JAPhA.2009.07165. [DOI] [PubMed] [Google Scholar]
- 2.Quinlan C. Drive-thru window advertising system. 2004 Feb 12; Pub. No.: US 2004/00216176 A1. [Google Scholar]
- 3.Lee TA, Larson LN. Evaluating the use and quality of pharmacy drive-up services. J Am Pharm Assoc. 1999;39:338–45. doi: 10.1016/s1086-5802(16)30447-8. [DOI] [PubMed] [Google Scholar]
- 4.Schnipper JL, Kirwin JL, Cotugno MC, Wahlstrom SA, Brown BA, Tarvin E, et al. Role of pharmacist counseling in preventing adverse drug events after hospitalization. Arch Intern Med. 2006;166:565–71. doi: 10.1001/archinte.166.5.565. [DOI] [PubMed] [Google Scholar]
- 5.Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication adherence and persistence, blood pressure, and low-density lipoprotein cholesterol: a randomized controlled trial. JAMA. 2006;296:2563–2571. doi: 10.1001/jama.296.21.joc60162. [DOI] [PubMed] [Google Scholar]
- 6.Simpson RJ., Jr Challenges for improving medication adherence. JAMA. 2006;296:2614–2616. doi: 10.1001/jama.296.21.jed60074. [DOI] [PubMed] [Google Scholar]
- 7.Haynes RB, Yao X, Degani A, Kripalani S, Garg A, McDonald HP. Interventions to enhance medication adherence. Cochrane Database Syst Rev. 2005:CD000011. doi: 10.1002/14651858.CD000011.pub2. [DOI] [PubMed] [Google Scholar]
- 8.Svarstad BL, Bultman DC, Mount JK. Patient counseling provided in community pharmacies: effects of state regulation, pharmacist age, and busyness. J of Amer Pharm Assoc. 2004;44:22–9. doi: 10.1331/154434504322713192. [DOI] [PubMed] [Google Scholar]
- 9.Tarn DM, Paterniti DA, Kravitz RL, Heritage J, Liu H, Kim S, Wenger NS. How much time does it take to prescribe a new medication? Patient Educ Couns. Aug. 2008;72(2):311–9. doi: 10.1016/j.pec.2008.02.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Puspitasari HP, Aslani P, Krass I. A review of counseling practices on prescription medicines in community pharmacies. Res Soc Admin Pharm. 2009;5:197–210. doi: 10.1016/j.sapharm.2008.08.006. [DOI] [PubMed] [Google Scholar]
- 11.Andersen RM, Davidson PL. Improving access to care in America: Individual and contextual indicators. In: Andersen R, Rice T, Kominski J, editors. Changing the U.S. health care system: Key issues in health services, policy and management. Jossey-Bass; San Francisco: 2001. pp. 3–30. [Google Scholar]
- 12.U.S. Senate Special Committee on Aging . Implementation of the Drug Use Review Provisions of the Medicaid Prudent Pharmaceutical Provisions of the Omnibus Budget Reconciliation Act of 1990. Vol. 1991. Senate Special Committee on Aging; Washington, DC: U.S.: pp. 1–6. [Google Scholar]
- 13.Wang J, Zuckerman IH, Miller NA, Shaya FT, Noel JM, Mullins CD. Utilizing new prescription drugs: disparities among non-Hispanic whites, non-Hispanic blacks, and Hispanic whites. Health Serv Res. Aug. 2007;42(4):1499–519. doi: 10.1111/j.1475-6773.2006.00682.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Greene WH. Econometric analysis. Eth ed. Prentice Hall; Upper Saddle River, NJ: 2000. [Google Scholar]