

Abstract
Background:
Poor freestyle stroke biomechanics is a suggested risk factor for shoulder pain and pathology, but this has not been proven in biomechanical or clinical studies. Furthermore, the prevalence of these theoretical errors has not been identified, which would help coaches, athletic trainers, and researchers determine the most appropriate errors to focus on and develop interventions.
Hypothesis:
The majority of swimmers will present with at least 1 freestyle stroke error.
Study Design:
Cross-sectional study.
Level of Evidence:
Level 4.
Methods:
Stroke biomechanics for 31 swimmers from a collegiate swimming team were captured using underwater/above-water cameras. Each video was evaluated for biomechanical errors: a dropped elbow during the pull-through phase, a dropped elbow during the recovery phase, an eyes-forward head-carrying angle, incorrect hand position during hand entry, incorrect hand entry angle, incorrect pull-through pattern, and inadequate body roll. Error prevalence was calculated, and relationships among the errors were evaluated using chi-square statistics.
Results:
A dropped elbow during the pull-through phase (61.3%) and a dropped elbow during the recovery phase (53.2%) had the highest prevalence. A dropped elbow during the recovery phase was significantly associated with a thumb-first hand entry angle (P = 0.027) and incorrect hand entry position (P = 0.009). An eyes-forward head-carrying angle was associated with an incorrect pull-through pattern (P = 0.047).
Conclusion:
Biomechanical errors potentially detrimental to the shoulder are prevalent among swimmers. Many of the errors were interrelated, suggesting that one error may lead to other errors.
Clinical Relevance:
These errors highlight the need for proper stroke instruction and evaluation to decrease the risk of shoulder injury in competitive swimmers.
Keywords: swimming, biomechanics, shoulder injury, injury prevention
The freestyle stroke places significant stress on the shoulder. Continual repetition and intense demand are placed on the shoulder causing frequent injury in swimming athletes.11 A major cause of these shoulder problems experienced by freestyle swimmers is subacromial impingement.16
To date, high training volume is a suggested risk factor for shoulder injuries in competitive swimmers.10,12,13 On average, swimmers at the collegiate level train between 40,000 and 50,000 yards per week, and an elite swimmer may log up to 20,000 yards in 1 day.5,11 To complete this yardage during practice time, 80% is freestyle,1 regardless of stroke specialty. This places tremendous stress on the shoulder. Competitive swimmers average approximately 18,000 shoulder revolutions per week, mostly from freestyle training.1,6
Current research on swimming biomechanics is limited, making it difficult for any coach, swimmer, or investigator to identify correct freestyle stroke technique that improves performance and decreases the risk of shoulder injury. There are studies that provide a theoretical basis for identifying errors in freestyle biomechanics that may place the swimmer in a vulnerable position for injury.3,4,7,15,16 The freestyle stroke is traditionally broken down into 3 distinct phases: hand entry, pull-through, and recovery (Figure 1). Stroke errors during each of these phases have been linked to the development of shoulder injury (Table 1).
Figure 1.
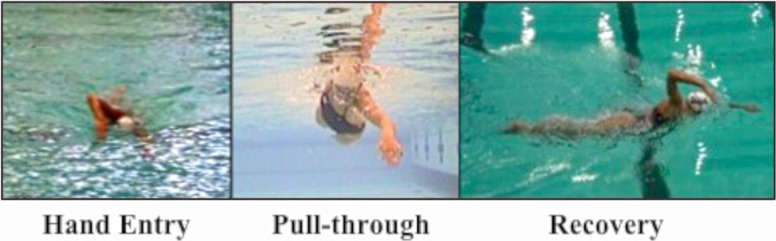
Phases of the freestyle stroke.
Table 1.
Freestyle biomechanical parameters
| Stroke Phase | Correct Freestyle Biomechanics | Incorrect Freestyle Biomechanics | Relevance of Incorrect Biomechanics to Shoulder Pain |
|---|---|---|---|
| Hand entry | Hand enters water forward and lateral to the head, medial to the shoulder.6 Figure 2a | Hand enters further away from or crosses the midline of the long axis of the body.4,8,14 Figure 2b | Increases impingement to the anterior shoulder.4 Mimics Neer impingement testing position.14 |
| Little finger– or fingers-first hand entry.4 Figure 3a | Thumb-first hand entry.4 Figure 3b | Stresses the biceps attachment to the anterior labrum.4 | |
| Pull-through | Elbow kept higher than hand and points laterally throughout pull.2 Figure 4a | Dropped elbow during pull-through.15 Figure 4b | Increases external rotation, placing muscles of propulsion at mechanical disadvantage.7 |
| Swimmer should use a straight back pull-through.2 Figure 5a | S-shaped pull through or excessive horizontal adduction past body midline during pulling.4 Figure 5b | Increases time spent in the impingement position.4 Mimics Hawkins Kennedy impingement testing position of horizontal adduction, flexion, and internal rotation. | |
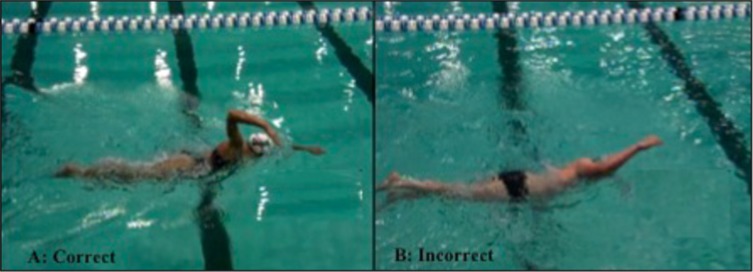
| Recovery | Elbow kept higher than the wrist throughout the recovery phase.4,15 Figure 6a | Dropped elbow during recovery phase.14Figure 6b | Leads to an improper entry position with the elbow entering the water before the hand. The water will cause an upward force on the dropped humerus, leading to its superior translation and subacromial impingement in the shoulder.14 |
| Body roll of ~45° along the longitudinal axis of the body.2,4 Figure 7a | Body roll that is greater or less than 45°.4 Figure 7b | Excessive roll can lead to crossover entry position during the hand entry and/or pull-through phase. A lack of roll during recovery can increase mechanical stress on the shoulder and lead to improper hand entry position.4 | |
| All phases | Head in neutral position. Imagine line through center of head and extending length of the spine.4 Figure 8a | Head carriage is in eyes-forward position.4 Figure 8b | Eyes-forward head position increases impingement by impeding normal scapulothoracic motion.4 |
Swim volume–induced supraspinatus tendinopathy with associated supraspinatus tendon thickening may be an intrinsic risk factor for the development of swimmer’s shoulder.11 Individuals with supraspinatus tendinopathy also had significantly greater supraspinatus tendon thickness associated with the hours swum and yardage completed per week. The volume of training is a significant contributor to the changes within the supraspinatus tendon and potentially the development of shoulder pain. Although this study did not evaluate stroke biomechanics, stroke biomechanics that decrease subacromial space can increase compression of the supraspinatus tendon and can result in supraspinatus tendon thickening.
The prevalence of each biomechanical error could guide research of biomechanical risk factors for shoulder pain in the swimmer. Understanding the relationships between the stroke errors is important because each part of the freestyle stroke can affect the other phases. Therefore, the purpose of this study was to examine the prevalence of incorrect freestyle biomechanics among collegiate swimmers and to evaluate the relationships between the errors.
Methods
All participants read and signed a consent form approved by the University of North Carolina at Chapel Hill’s Institutional Review Board. Thirty-one collegiate swimmers from the university participated in this study. The subject mean age, height, and mass were 20 ± 1.41 years, 179.17 ± 9.65 cm, and 75.43 ± 8.64 kg, respectively. On average, participants had swum competitively for 11.3 ± 3.49 years. Subjects were included in the study if they were between 18 and 24 years of age, were regularly training at least 5 times per week for 1 to 2 hours each practice session, had at least 5 years of competitive swimming experience, and were completing practice with no restrictions at the time of the filming. Although subjects were not evaluated for previous shoulder injury or pain, individuals were excluded if they were unable to complete practices fully due to pain, injury, or illness at the time of the testing session. Because right and left shoulders were treated independently, biomechanical errors were evaluated for a total of 62 shoulders.
Each swimmer was instructed to swim freestyle for 1 length of the swimming pool at a pace 50% to 75% of his or her maximum race speed using his or her natural stroke technique. This was completed twice, resulting in a total of 50 yards swum by each subject. Swimmers were recorded for 2 trials while swimming freestyle to capture both the right and left sides of the athlete. One underwater camera and 1 above-water camera were placed at the end of a 25-yard swimming pool to obtain frontal views of each swimmer’s freestyle biomechanics. The lateral view was obtained from both the underwater and above-water cameras. Both lateral camera views were adjusted to capture the last 15 yards of the pool. Each of the 4 views was uploaded into Dartfish video processing software (Fribourg, Switzerland), which was used to sync the frontal and lateral views to ensure that the same stroke and point in the stroke cycle were being evaluated.
Following the filming of all trials, a stroke cycle was selected for grading. A stroke cycle was considered appropriate for analysis if (1) the cycle was completely within the camera view, (2) the above-water and underwater cameras captured the subject sufficiently well so that his or her body was positioned at the center of each field throughout filming, and (3) the image size of the subject projected on the monitor was large enough to be viewed.15 The first full stroke cycle to enter the camera view and meet the previous criteria was selected for evaluation.
Two experienced swimming coaches and 1 certified athletic trainer with experience with a collegiate-level swimming team and no knowledge of the swimmers’ shoulder injury histories or freestyle strokes were asked to observe and evaluate the selected video clips. All examiners underwent standardized training through the use of still photographs of the 7 biomechanical parameters and sample video examples of correct and incorrect freestyle biomechanics. This served as a practice evaluation before the actual test trial videos (Table 1 and Figures 2-8). Each of the 7 parameters was graded as a yes or no for displaying the associated error. A majority-rules method was used in which the most common response among the 3 observers was chosen for each biomechanical parameter. Interrater reliability was established for the errors. Kappa scores for a dropped elbow during the pull-through phase and the recovery phase, an eyes-forward head-carrying angle, incorrect hand position during hand entry, incorrect hand entry angle, and an incorrect pull-through pattern had moderate to substantial agreement (range, 0.50-0.90) and were included in the analysis. Because of poor agreement between the raters’ kappa scores (<0.40), body roll was not included in the analysis. Body roll was not clearly viewed using 1 camera angle and was therefore dropped (Figure 7).
Figure 2.

Hand entry angle. (a) Correct: fingers-first entry; (b) incorrect: thumb-first entry.
Figure 3.
Hand entry position. (a) Correct: lateral to head and medial to shoulder; (b) incorrect: hand enters too medially or too laterally.
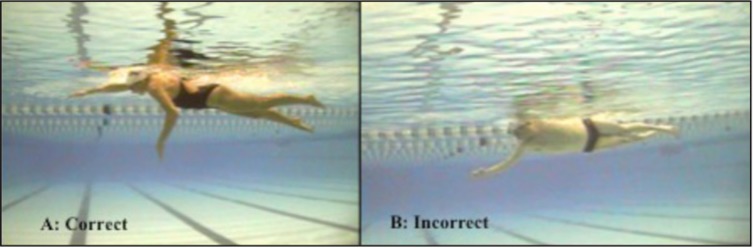
Figure 4.
Pull-through pattern. (a) Correct: straight back pull-through; (b) incorrect: excessive horizontal adduction (S-shaped pattern).
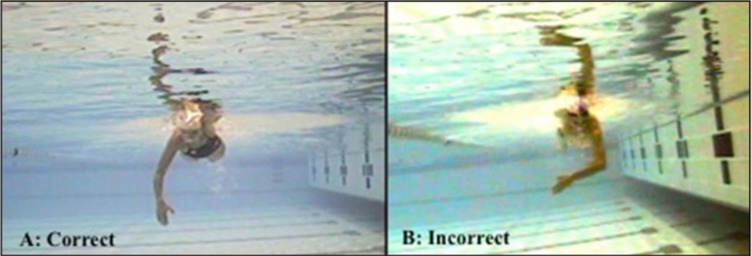
Figure 5.
Elbow position during pull-through. (a) Correct: elbow kept higher than wrist, pointing laterally; (b) incorrect: dropped elbow.
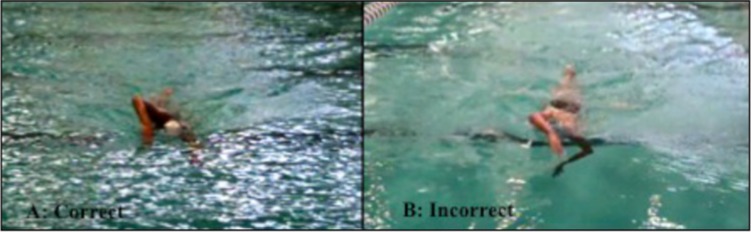
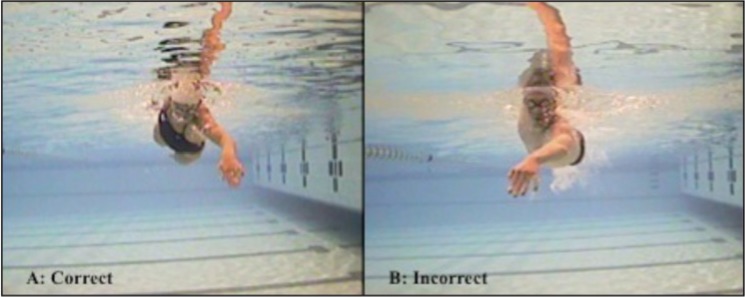
Figure 6.
Elbow position during recovery. (a) Correct: elbow kept higher than wrist; (b) incorrect: dropped elbow.
Figure 7.
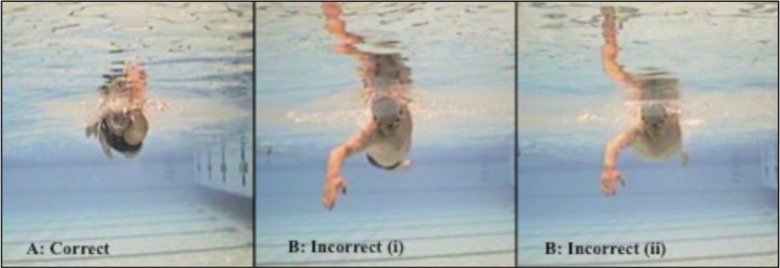
Body roll angle. (a) Correct: body roll of at least 45° occurring along the longitudinal axis of the body; (b and c) incorrect: excessive body roll (i) or lack of body roll (ii).
Figure 8.
Head-carrying angle. (a) Correct: neutral head position; (b) incorrect: eyes-forward head position.
Descriptive statistics were used to describe the prevalence of each freestyle biomechanical error. A chi-square analysis examined associations between the freestyle biomechanical errors. An a priori alpha level was set at 0.05. Statistical analyses were run using SPSS version 19.0 (IBM Corp, Armonk, New York).
Results
The most common biomechanical errors were a dropped elbow during the pull-through phase (61.3%) and a dropped elbow during the recovery phase (53.2%). The errors of eyes-forward head-carrying angle and incorrect hand position during hand entry occurred in 46.8% and 45.2%, respectively. Finally, we found low percentages of swimmers display an incorrect hand entry angle (38.71%) and an incorrect pull-through pattern (32.3%).
There were significant associations between the errors of a dropped elbow during the recovery phase and a thumb-first hand entry angle (χ2 = 4.876, P = 0.027), a dropped elbow during the recovery phase and incorrect hand entry position (χ2 = 6.795, P = 0.009), and an eyes-forward head-carrying angle and an incorrect pull-through pattern (χ2 = 3.939, P = 0.047). All other associations were not statistically significant.
Discussion
Stroke errors are potential risk factors for shoulder pain in competitive swimmers.4,8,14,15 Swimmers are subject to shoulder impingement for approximately 25% of their freestyle stroke cycle, even when using proper biomechanics.16
The biomechanical errors of a dropped elbow during the pull-through phase and a dropped elbow during the recovery phase were most prevalent. Dropping the elbow during the pull-through phase places the propulsive muscles of the shoulder at a mechanical disadvantage by placing the shoulder in a more externally rotated position.7 This stroke error is commonly identified by swimming coaches and can result in shoulder external rotation with horizontal adduction, placing the shoulder in an impingement position.15
During the above-water recovery phase, the elbow should be kept higher than the wrist and should avoid a dropped position.2,14 A dropped elbow during this phase may orient the humerus more perpendicular to the water, producing a shorter arc of motion and decreasing time spent in the impinged position.8 This stroke alteration is incorrect, but it may be an attempt to avoid the impingement position of shoulder flexion and internal rotation.8 This error could be the consequence of pain and not the cause. An elbow that enters prior to the hand causes the water to exert an upward force on the dropped humerus, leading to superior translation of the humeral head and subacromial impingement.14
The results indicate a relationship between dropped elbow during the recovery phase and a thumb-first hand entry angle as well as between a dropped elbow during recovery and an incorrect hand entry position. These findings suggest that a dropped elbow may lead to an improper entry position with the elbow entering before the hand.14
The mechanics of these swimmers may be a result of instruction provided by their youth swimming coaches or a stroke technique developed throughout their careers. These findings highlight the importance of proper instruction on stroke technique in youth swimming. The swimming motion is complex, and faulty mechanics may develop because of poor coaching, poor understanding by the swimmer, shoulder pain, or performance factors.
During video grading, the swimming coach evaluators identified a discrepancy between the provided criteria and a poor freestyle stroke technique. While maintaining a “straight back” pull-through during freestyle is considered safest for a swimmer’s shoulder girdle because it avoids excessive horizontal adduction, coaches recognize an S-shaped pull-through pattern (Figure 5b) produces performance gains and increased swimming velocity.9 Utilizing a curvilinear motion during the freestyle pull-through best produces propulsion by constantly pushing water and gaining additional resistance rather than by pushing water, which has already been accelerated by a straight back stroke path.2 While this method of underwater propulsion makes sense for performance purposes, it yields increased risk for the swimmer’s shoulder in a vulnerable impingement position. This curvilinear motion mimics the faulty S-shaped pull-through pattern, which can give rise to increased time in the impingement position. It forces the shoulder to maintain increased muscle recruitment and higher loads over a longer period.2,4,9,14,15
There are limitations to this research. First, the participants were all members of the same collegiate team, which may affect the generalizability. Although all subjects were members of the same collegiate team, they had trained across the country and came from a variety of training clubs. In addition, our sample was limited to the number of healthy subjects currently on the team. Thus, some of the associations were nonsignificant because of the smaller sample size. Finally, each shoulder of the swimmer was treated as independent, with stroke evaluation and pain scores evaluated on the right and the left shoulder independently for the analysis. Paired shoulders were treated independently to understand how stroke biomechanics relate to the development of pain on the ipsilateral shoulder.
Conclusion
It is crucial that both coaches and medical professionals recognize faulty biomechanics in swimming freestyle. Biomechanical errors are associated with one another in the freestyle stroke cycle. A stroke technique evaluation can identify potentially injurious biomechanics.
Footnotes
The following author declared potential conflicts of interest: Darin A. Padua, PhD, ATC, is a consultant for and has grants/grants pending from the National Academy of Sports Medicine.
References
- 1. Beach ML, Whitney SL, Dickoff-Hoffman S. Relationship of shoulder flexibility, strength, and endurance to shoulder pain in competitive swimmers. J Orthop Sports Phys Ther. 1992;16:262-268 [DOI] [PubMed] [Google Scholar]
- 2. Colwin CM. Breakthrough Swimming. Champaign, IL: Human Kinetics; 2002 [Google Scholar]
- 3. Heinlein SA, Cosgarea AJ. Biomechanical considerations in the competitive swimmer’s shoulder. Sports Health. 2010;2:519-525 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Johnson JN, Gauvin J, Fredericson M. Swimming biomechanics and injury prevention: new stroke techniques and medical considerations. Phys Sportsmed. 2003;31:41-46 [DOI] [PubMed] [Google Scholar]
- 5. McMaster WC, Troup J. A survey of interfering shoulder pain in United States competitive swimmers. Am J Sports Med. 1993;21:67-70 [DOI] [PubMed] [Google Scholar]
- 6. Pink M, Perry J, Browne A, Scovazzo ML, Kerrigan J. The normal shoulder during freestyle swimming: an electromyographic and cinematographic analysis of twelve muscles. Am J Sports Med. 1991;19:569-576 [DOI] [PubMed] [Google Scholar]
- 7. Richardson AB, Jobe FW, Collins HR. The shoulder in competitive swimming. Am J Sports Med. 1980;8:159-163 [DOI] [PubMed] [Google Scholar]
- 8. Scovazzo ML, Browne A, Pink M, Jobe FW, Kerrigan J. The painful shoulder during freestyle swimming. Am J Sports Med. 1991;19:577-582 [DOI] [PubMed] [Google Scholar]
- 9. Seifert LC, Mujika ID, eds. World Book of Swimming: From Science to Performance. New York, NY: Nova Science; 2011 [Google Scholar]
- 10. Sein MW, Walton J, Linklater J, et al. Shoulder pain in elite swimmers: primarily due to swim-volume-induced supraspinatus tendinopathy. Br J Sports Med. 2010;44:105-113 [DOI] [PubMed] [Google Scholar]
- 11. Stocker D, Pink M, Jobe FW. Comparison of shoulder injury in collegiate- and master’s-level swimmers. Clin J Sport Med. 1995;5:4-8 [DOI] [PubMed] [Google Scholar]
- 12. Tate A, Turner GN, Knab SE, Jorgensen C, Strittmatter A, Michener LA. Risk factors associated with shoulder pain and disability across the lifespan of competitive swimmers. J Athl Train. 2012;47:149-158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Walker H, Gabbe B, Wajswelner H, Blanch P, Bennell K. Shoulder pain in swimmers: a 12-month prospective cohort study of incidence and risk factors. Phys Ther Sport. 2012;13:243-249 [DOI] [PubMed] [Google Scholar]
- 14. Wilk KE, Reinold MM, Andrews JR, eds. The Athlete’s Shoulder. Philadephia, PA: Churchill Livingstone; 2009 [Google Scholar]
- 15. Yanai T, Hay JG. Shoulder impingement in front-crawl swimming: II. Analysis of stroking technique. Med Sci Sports Exer. 2000;32:30-40 [DOI] [PubMed] [Google Scholar]
- 16. Yanai T, Hay JG, Miller GF. Shoulder impingement in front-crawl swimming: I. A method to identify impingement. Med Sci Sports Exer. 2000;32:21-29 [DOI] [PubMed] [Google Scholar]