

Abstract
Aim:
Evaluation and co-relation of the caries susceptibility using Oratest, colorimetric Snyder's test and salivary Streptococcus mutans count amongst children in the age group of 6-8 years.
Materials and Methods:
A total of 120 healthy children were grouped into control and test groups according to their dmft/DMFT scores. Snyder's test, salivary S. mutans count and Oratest were performed for each individual.
Results:
The relationship of three caries activity tests with each other and with existing caries status was found out.
Conclusion and Clinical Implications:
The present study has shown that Oratest has a definite clinical relationship with caries status and microbiological relationship with S. mutans count of the individual.
Keywords: Caries activity test, dental caries, Oratest
Why this article is important
Understanding caries etiology and its progression has been made easy with concomitant advances in science and technology. However, utilization of those advances in community practice is still difficult. Although most of the population in developing countries live in indigence, it is must for the clinician to develop rapid, inexpensive and yet effective methods for caries control and progress. This article provides an insight of how a simple oral rinse test can be used for detection of caries activity.
INTRODUCTION
In a period marked by brilliant achievements in the prevention and treatment of disease, dental caries still remains one of the most widely spread afflictions in human populations.[1] Dental caries is one of the most prevalent infectious diseases and for practical purposes it can be considered ubiquitous in civilized population.[2]
The dental caries prevalence in the child population is increasing at an alarming rate, the prevalence varying from 33.7% to 90%.[3] Furthermore, the inequalities in the distribution of dental care in rural and urban areas correlate well with the difference found in caries prevalence for the respective populations. Given the harsh realities of the maldistribution of resources and variations in individual susceptibility, dental caries is not about to become another extinct disease.[4,5]
Dental caries gets established in the mouth long before it becomes clinically manifested in the form of visible lesions. This means it should be possible to assess the seriousness of the caries in a patient or in a population. Such an assessment is rather like making a weather forecast.[6]
The concept of prediction of human dental caries risk has existed for many years. Particularly, during the past 10-15 years, there has been a surge of interest in this issue. This appears to reflect recent advances in our knowledge of the etiology of dental caries, the potential promise of certain risk factors or combinations thereof for caries prediction. There should be incessant desire to prevent rather than to treat dental caries, but at the same time the increasing need of cost containment should be understood.[7]
Even though, dental caries is known to be a multifactorial disease process, the vast number of caries susceptibility tests developed so far is based on the microbiological aspects of dental caries.[8]
Caries activity can generally be defined as the occurrence and the rate at which, teeth are destroyed by acid produced by the plaque bacteria.[9]
A good caries activity test should possess at least three characteristics, i.e. validity, reliability and feasibility. It should also have good sensitivity and specificity.
It is very difficult to measure all the factors responsible for caries using one caries activity test. Hence until date, the ideal method to evaluate caries activity in terms of sensitivity, specificity and reliability has not been found.[10] Currently, there are many caries activity test kits available in the market, e.g. Dentocult SM, Mucount, GC Saliva Buffer Check etc., Unfortunately, many of these caries activity tests require extensive work-up time and special equipments. In developing countries simple, inexpensive and quick techniques, which do not demand sophisticated skills or consume a substantial amount of chair-side time, are required for the caries activity tests. These deserve the status in the routine clinical practice and epidemiological screening programs. However, very few studies have been reported regarding their sensitivity and specificity to assess caries risk.
In this study, an attempt has been made to explore the co-relation of simple oral rinse technique (Oratest) with the other caries activity tests in children.
MATERIALS AND METHODS
This study was carried out in the Department of Pedodontics and Preventive Dentistry in association with the College of Microbiology.
A total of 120 healthy school going children of both sexes falling in the age group of 6-8 years were selected by randomized sample technique.[11] Out of 120 children, 30 caries free children were randomly selected through a survey carried out in a Public School, Pimpri. An informed consent was obtained from the child's parents/guardians for the subjects who were fulfilling the inclusion criteria. Care was taken to ensure ethical protection of human subjects at all stages of the study. All the necessary ethical guidelines were followed as prescribed by the Institutional Ethical Committee in accordance with the Central Ethics Committee on Human Research, India.[12]
Inclusion criteria
Oral examination
All the participating subjects received a thorough oral examination using a mouth mirror and World Health Organization (WHO) probe in adequate illumination. The decayed, missing and filled teeth (dmft/DMFT) were recorded as per WHO criteria. Radiographs were not obtained. The caries experience was calculated as the dmft + DMFT.[12,14] All the subjects were divided into two groups according to their dmft/DMFT scores.
Group I: Control group (dmft/DMFT = 0): 30 subjects.[13]
Group II: Test group (dmft/DMFT > 0): 90 subjects.
The Test group was further subdivided into 3 subgroups:[13]
Sub-group A: (dmft/DMFT = 1-5): 30 subjects
Sub-group B: (dmft/DMFT = 6-10): 30 subjects
Sub-group C: (dmft/DMFT = 11-18): 30 subjects.
All the subjects were taken for the study only after a gap of 90 min after the last intake of food or drink.[15] Prepared Snyder's test medium was melted in the microcentrifuge tubes, which were then kept in hot water bath at 50°C. The fluid thioglycollate medium was prepared and poured in test tubes and kept ready.
Collection of saliva
A standardized protocol was followed for saliva collection.[16] The child was made to sit comfortably on the dental chair in an erect position. After swallowing the pre-existing saliva in the oral cavity, a standardized piece of gum base (∼1 g) was given to the child. The stimulated saliva secreted in the subsequent 3 min was collected while the child chewed on the same block of gum base. The child was made to spit and drool in a disposable sterile cup held near the mouth.
Salivary sampling for estimation of Streptococcus mutans
By means of a sterile disposable syringe, 1 ml aliquot of collected saliva was removed from the measuring cup and injected in a previously labeled sterile test tube containing 4 ml of transport medium. These test tubes were kept in a box containing ice packs for transport.
Procedure for Snyder's caries activity test
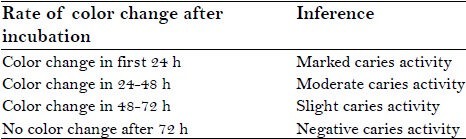
0.2 cc of saliva was pipetted into the melted Snyder's medium at 50°C. After the addition of saliva into the medium, tube was rotated for proper mixing of saliva and the medium. The microcentrifuge tube incubated at 37°C for up to 72 h[17] . An un-inoculated tube was used as a negative control. The observations for color change were made every 24 h for a period of 72 h. The rate of color change of Snyder's medium from green to yellow is indicative of caries activity. The interpretation of Snyder's test observation was made according to following:[18]
Procedure for oratest
Oratest was carried out in the same patients after the collection of salivary sample for the microbiological method [Figure 1].
Figure 1.

Materials for Oratest
Each patient was given 10 ml of ultra-high temperature sterilized cow milk in a beaker and asked to rinse the mouth vigorously for 30 s. The expectorate was collected in the same beaker and 3 ml of this was aspirated with the help of a disposable syringe. 0.12 ml of 0.1% methylene blue was added to a sterile screw cap test tube the expectorate was transferred to the test tube and thoroughly mixed. It was placed on a stand in a well-illuminated area over a mirror at room temperature. Test tubes were observed every 10 min for color change at the bottom, which would easily be discernible in the mirror. Time taken for initial color change within a 6 mm diameter circle on the bottom of the test tube was recorded[19] [Figure 2].
Figure 2.

Color change at bottom of test tubes
Culturing on mitis-salivarius bacitracin agar
A total volume of 10 μl of the vortexed sample was streaked in duplicate on MSB agar selective for mutans Streptococci. The colony count was performed with digital colony counter.[20]
RESULTS
Results were analyzed by Software Package for Statistical Analysis [SPSS] version 17.
The Oratest time in the control group had shown a range of 200-305 min and in test groups shown a range of 24-200 min. A statistically significant difference revealed with the mean Oratest scores revealed a statistically significant difference (P < 0.001) between the control and individual test groups. The Oratest time observed in the control group was significantly higher than the individual test groups [Table 1].
Table 1.
Mean values of Oratest and S. mutans count for control and test groups

A statistically significant difference obtained with the mean of salivary S. mutans count between control and individual tests groups [Table 1].
Snyder's test results are recorded for each group. The modal values of Snyder's caries activity test for the control group, sub-group A, sub-group B and sub-group C was found to be negative, slight, moderate and moderate respectively [Graph 1].
Graph 1.
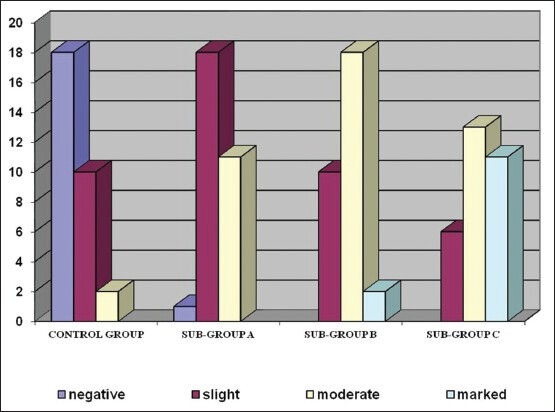
Results for Snyder's caries activity tests
Chi-square test results showed a statistically high significant difference (P < 0.001) between the Snyder's test results of control and individual test groups.
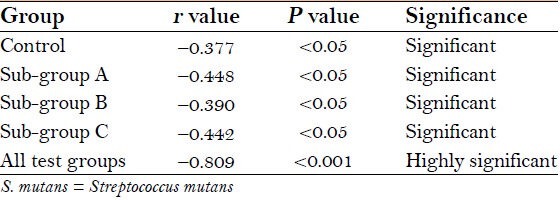
Pearson's correlation analysis revealed, the S. mutans count in a statistically significant negative linear relationship with Oratest time [Table 2].
Table 2.
Pearson's correlation analysis of S. mutans count and Oratest time for control and test groups
All test groups computed together the Oratest time (min) was found to be in a statistically highly significant negative linear relationship with existing caries status.
Thus, Oratest time was found to have a significant negative linear relationship with salivary S. mutans colony count and deft/DMFT of the individual [Graph 2].
Graph 2.
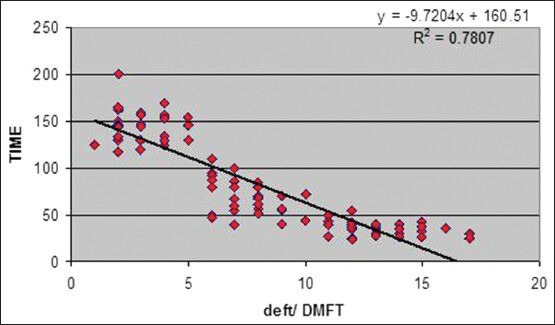
Scatter diagram showing correlation of deft/DMFT and Oratest time for all test groups
DISCUSSION
An overview of changes in dental caries confers a global decline in DMFT levels of individuals. Thanks to the 20th century which has given tremendous knowledge in the understanding of oral diseases and possibilities for preventing and treating these diseases. However, this knowledge cannot be put into action in a developing country like India due to financial constraints and lack of man power.
In a country where 70% population inhabits the villages (Consensus 2001), the Dentist: population ratio is 1:35,000 and only one out of five Dentists return back to the rural area to serve, prevention of caries will be a more viable option than rendering restorative treatment. In the existing situation in India, it calls for real dedicated and strenuous effort to implement caries prevention programs. The cost involved in assessing the high risk group by S. mutans test and other methods in Indian situation is so high that it cannot become a routine procedure in the near future. Western methods for caries prevention as such will not be successful here and they need to be modified to suit the local needs and habits. There is an acute need for simple, robust, inexpensive equipments for use in rural surroundings. Hence, this study was designed to evaluate the caries susceptibility of children using a non-invasive, simple and inexpensive Oratest and to compare it with two other caries activity tests.
In comparison with the sole use of any one caries activity test, the combination of the information of different parameters has been shown to increase the power in caries prediction.[21] In this study both the subjective and objective evaluation has been carried out for each subject and then compared with each other. The caries process is initiated by activity within the biofilm and manifested in the underlying enamel or dentin.[22] In the present study, the mean salivary S. mutans count for 0 deft/DMFT subjects was 3.12 × 104 . Although in test groups, it ranged from 1.4 × 105 CFU/ml to 1.76 × 106 CFU/ml of saliva. Similar results were also been observed by Loesche et al.[23] and by Straetemans et al.[24]
Lactobacilli being acidogenic as well as aciduric possesses a strong potential to demineralize enamel surfaces. Significant relation between lactobacilli and caries experience was shown by Crossner, Holbrook,[25] Kingman et al.[26] and Zickert et al.[27] A simple colorimetric test, i.e. Snyder's test was developed for practicing Dentist to serve as a valuable aid in detection of lactobacilli. The Snyder's test measures the rapidity of acid formation when a sample of stimulated saliva is inoculated into glucose agar adjusted to pH 4.7-5 and with bromocresol green as color indicator. Indirectly, the test is also a measure of acidogenic and aciduric bacteria. Overall distribution of Snyder's test results in the present study [Graph 1] correlated well with the existing caries status of individual. Such relation had also been supported by Ali YA et al.[13] In a study carried out by Ramesh et al. Sensitivity of Snyder's test was found to be 87.5% along with positive predictive value of 18.9%. Specificity of 18.9% was obtained with negative predictive value of 87.5% in caries free individuals. However, 100% sensitivity was shown in children with caries.[28]
There have been two main schools of thoughts on the role of plaque bacteria in the etiology of caries and periodontal disease. The “specific plaque hypothesis” proposed that, out of the diverse collection of organisms comprising the resident plaque microflora, only a few species are actively involved in disease. In contrast, the “non-specific plaque hypothesis” considered that disease is the outcome of the overall activity of the total plaque microflora. In this way, a heterogeneous mixture of micro-organisms could play a role in disease. More recently, an alternative hypothesis “ecological plaque hypothesis” has been proposed, which stated that plaque-mediated diseases are as a consequence of imbalances in the resident microflora.[29]
Oratest, a whole mouth rinse test in this regard provides a pooled sample of microbiota of oral cavity. Thus, the principle of Oratest is congruent with Philip Marsh's “ecological plaque hypothesis” proposed in early 1990s. In young plaques, streptococci usually predominate, but other organisms such as Neisseria and Actinomyces species may also play a role in the initial development of plaque. Streptococcus sanguis is among the more prominent initial colonizers of tooth surface. As the plaque matures during 7-14 days, the rods and filaments increase proportionally. The changes in the morphological forms of the plaque flora have been attributed to changing metabolic and environmental conditions within the plaque over time. As plaque accumulates and matures it becomes more anaerobic. The degree of anaerobiosis of plaque is reflected in its redox potential (Eh). The Eh of early developing plaque is about + 200 mV, which is similar to aerobically metabolizing tissue. However, several days old plaque will have an Eh of about –100 mV. Growth of anaerobes is encouraged at low Eh levels. Oxygen depletion by aerobic plaque micro-organisms is a prerequisite for the development and progression of anaerobic growth conditions.
Oratest is based on the rate of oxygen depletion by the microorganisms in expectorated milk samples. Once oxygen gets utilized by aerobic micro-organisms, methylene blue acts as electron acceptor and gets reduced to leucomethylene blue reflecting the metabolic activity of the aerobic organisms. In some of the previous studies strong correlations were observed between Oratest scores and counts of aerobic and aerotolerant micro-organisms.[13]
Also studies done by Patalay et al.[13] and Bhasin et al.,[15] Saxsena et al.[30] have suggested that Oratest can be used as chair-side caries activity test. But the literature about its comparative evaluation with other caries activity tests seems to be lacking. Hence, in the present study for the 1st time Oratest has been compared with qualitative and quantitative characteristics of cariogenic bacteria.
Milk is used in this study because it acts as a suitable liquid for dislodging micro-organisms and provides an excellent medium for subsequent metabolism. Furthermore, it is non-toxic and is readily acceptable by children. Moreover, milk being white in color, make it easier to detect the earliest color change from blue to white at the base of test tube, i.e. methylene blue to leucomethylene blue.[31] Milk used for the present study was sterilized using Pasteurization method.
Nearly 1% of methylene blue was used in the present study as suggested by Desai et al. and Rosenberg et al.[19] Since, there is no oxygen in the methylene blue molecule; the reduction of this dye involves transference of hydrogen. Bacterial metabolites have been shown to act as hydrogen donators.[32,33] The corresponding metabolism, which occurs will be a reaction which supplies energy for the growth of the organisms.
Sensitivity is defined as the ability of a test to detect the presence of a disease in patients with the disease, while specificity is the ability of a test to detect the absence of a disease in patients without the disease. The Oratest by virtue of its simplicity and high degree of sensitivity–could be used to screen patients for dental caries. However, the lack of specificity of the Oratest can mean that a high number of false positive readings occurred. Some of the false positive results for the Oratest and S. mutans count could be explained by the presence of interproximal caries that was not diagnosed clinically. In both cases, the number of false positive results would be reduced if radiographs were exposed to detect interproximal caries.
Since, larger sample size and proposed use of Oratest at community level, no radiographs were made for assessing proximal caries in the individuals. However, dmft/DMFT score was used as useful predictor of caries.[34]
Higher levels of cariogenic organisms and higher plaque values in high risk group may have resulted into shortest Oratest time. Thus, in context to the observations of the present study and of earlier studies it is supported that Oratest can be used as one of the tool to estimate caries activity and oral microbial level.
Advantages
Simple, inexpensive, non-invasive, less time consuming, reproducible and required no trained personnel
Can be used to monitor mouth-rinse programs, denture hygiene and gingival inflammation and plaque levels
Can be used as good educational and motivational tool for patients, school and community dental health programs
Vehicle of the test (Milk) is non-toxic and readily accepted by young patients
Can be used to identify high risk population groups
Results can provide the Dentist to command the patients to reinforce motivation, plaque control and behavior.
Limitations
It does not identify a specific group of organism in a specific disease
It cannot accurately differentiate between the healthy state and carrier state and also between initial and progressive carious lesion
It does not approach dental caries in a holistic manner like other caries activity tests
Lack of specificity gives false positive results as positive observations can be obtained in patients with gingival disease and other oral ailments.
CONCLUSION
Oratest is proven to be a simple, inexpensive and a rapid technique for assessment of caries activity according to present study.
We believe that this method will be useful, both at the individual level and community level, in an attempt to identify groups of persons with an increased risk to develop caries.
In the earlier study carried out by Cardash et al.,[33] patients were supplied with denture hygiene kits consisting of plastic test tubes containing 0.12 ml of methylene blue and plastic pipettes. If such oral hygiene kits made available to children, then it might be possible for parents to monitor oral hygiene. Performance of the test prior to the treatment session not only makes the waiting period interesting for the child, but also test results can provide the Dentist with something to comment upon either to reinforce motivation and plaque control or to reinforce a positive behavior.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Purohit VD, Damle SG. Salivary counts of mutans Streptococci, lactobacilli and caries active children. J Indian Soc Pedod Prev Dent. 1996;14(4):97–106. [Google Scholar]
- 2.Ali YA, Chandranee NJ, Wadher BJ, Khan A, Khan ZH. Relationship between caries status, colony forming units (cfu) of Streptococcus mutans and Snyder caries activity test. J Indian Soc Pedod Prev Dent. 1998;16:56–60. [PubMed] [Google Scholar]
- 3.Prakash H, Sidhu SS, Sundaram KR. Prevalence of dental caries among Delhi School Children. J Indian Dent Assoc. 1999;70:12–4. [Google Scholar]
- 4.Bowen WH. Dental caries: Is it an extinct disease? J Am Dent Assoc. 1991;122:49–52. doi: 10.14219/jada.archive.1991.0268. [DOI] [PubMed] [Google Scholar]
- 5.Munshi AK, Hegde AM, Munshi A. Relationship between the existing caries status, plaque S. mutans and Cariostat caries activity test in children. J Indian Soc Pedod Prev Dent. 1999;17:73–89. [PubMed] [Google Scholar]
- 6.Thylstrup A, Fejereskov O. Text Book of Cariology. Ch. 13. Denmark: Munksgaard Publication; 1989. Current status of caries activity tests; pp. 249–63. [Google Scholar]
- 7.van Houte J. Microbiological predictors of caries risk. Adv Dent Res. 1993;7:87–96. doi: 10.1177/08959374930070022001. [DOI] [PubMed] [Google Scholar]
- 8.Koroluk L, Hoover JN, Komiyama K. The sensitivity and specificity of a colorimetric microbiological caries activity test (Cariostat) in preschool children. Pediatr Dent. 1994;16:276–81. [PubMed] [Google Scholar]
- 9.Wyne AH, Guile EE. Caries activity indicators. A review. Indian J Dent Res. 1993;4:39–46. [PubMed] [Google Scholar]
- 10.Newbrun E. Ch. 8. 3rd ed. Chicago: Quintessence Publishing Company; 1989. Caries activity tests. Cariology; pp. 273–93. [Google Scholar]
- 11.Lui KJ. Estimation of sample sizes in case-control studies with multiple controls per case: Dichotomous data. Am J Epidemiol. 1988;127:1064–70. doi: 10.1093/oxfordjournals.aje.a114882. [DOI] [PubMed] [Google Scholar]
- 12.Chaudhary SD, Chaudhary M, Singh A, Kunte S. An assessment of the cariogenicity of commonly used infant milk formulae using microbiological and biochemical methods. Int J Dent. 2011:1–9. doi: 10.1155/2011/320798. Article ID 320798. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Patalay A, Shubhada C, Nadiger SL. Oratest: A simple, chair-side caries activity test. J Indian Soc Pedod Prev Dent. 1996;14:6–9. [PubMed] [Google Scholar]
- 14.Tal H, Rosenberg M. Estimation of dental plaque levels and gingival inflammation using a simple oral rinse technique. J Periodontol. 1990;61:339–42. doi: 10.1902/jop.1990.61.6.339. [DOI] [PubMed] [Google Scholar]
- 15.Bhasin S, Sudha P, Anegundi RT. Chair side simple caries activity test: Ora test. J Indian Soc Pedod Prev Dent. 2006;24:76–9. doi: 10.4103/0970-4388.26020. [DOI] [PubMed] [Google Scholar]
- 16.Dawes C, Tsang RW, Suelzle T. The effects of gum chewing, four oral hygiene procedures, and two saliva collection techniques, on the output of bacteria into human whole saliva. Arch Oral Biol. 2001;46:625–32. doi: 10.1016/s0003-9969(01)00017-6. [DOI] [PubMed] [Google Scholar]
- 17.Snyder ML, Clarke MK. Evaluation of the colorimetric (Snyder) test; comparison of positive color reactions with the Lactobacillus counts of respective specimens of saliva routinely submitted for culture. J Dent Res. 1950;29:298–303. doi: 10.1177/00220345500290030701. [DOI] [PubMed] [Google Scholar]
- 18.Snyder ML. A simple colorimetric method for the estimation of relative numbers of lactobacilli in the saliva. J Dent Res. 1940;19:349–55. [Google Scholar]
- 19.Rosenberg M, Barki M, Portnoy SA. A simple method for estimating oral microbial levels. J Microbiol Methods. 1989;9:253–57. [Google Scholar]
- 20.Hamada S, Masuda N, Shimamoto T. Some biological properties of Streptococcus mutans isolated from human mouths, with reference to the correlation with serotypes. Arch Oral Biol. 1979;24:627–31. doi: 10.1016/0003-9969(79)90025-6. [DOI] [PubMed] [Google Scholar]
- 21.Pienihäkkinen K, Scheinin A, Bánóczy J. Screening of caries in children through salivary lactobacilli and yeasts. Scand J Dent Res. 1987;95:397–404. doi: 10.1111/j.1600-0722.1987.tb01630.x. [DOI] [PubMed] [Google Scholar]
- 22.Kidd EA, Fejerskov O. What constitutes dental caries. Histopathology of carious enamel and dentin related to the action of cariogenic biofilms? J Dent Res. 2004;83:C35–8. doi: 10.1177/154405910408301s07. Spec No C. [DOI] [PubMed] [Google Scholar]
- 23.Loesche WJ, Rowan J, Straffon LH, Loos PJ. Association of Streptococcus mutants with human dental decay. Infect Immun. 1975;11:1252–60. doi: 10.1128/iai.11.6.1252-1260.1975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Straetemans MM, van Loveren C, de Soet JJ, de Graaff J, ten Cate JM. Colonization with mutans Streptococci and lactobacilli and the caries experience of children after the age of five. J Dent Res. 1998;77:1851–5. doi: 10.1177/00220345980770101301. [DOI] [PubMed] [Google Scholar]
- 25.Holbrook WP. Dental caries and cariogenic factors in pre-school urban Icelandic children. Caries Res. 1993;27:431–7. doi: 10.1159/000261575. [DOI] [PubMed] [Google Scholar]
- 26.Kingman A, Little W, Gomez I, Heifetz SB, Driscoll WS, Sheats R, et al. Salivary levels of Streptococcus mutans and lactobacilli and dental caries experiences in a US adolescent population. Community Dent Oral Epidemiol. 1988;16:98–103. doi: 10.1111/j.1600-0528.1988.tb01852.x. [DOI] [PubMed] [Google Scholar]
- 27.Zickert I, Emilson CG, Krasse B. Streptococcus mutans, lactobacilli and dental health in 13-14-year-old Swedish children. Community Dent Oral Epidemiol. 1982;10:77–81. doi: 10.1111/j.1600-0528.1982.tb00367.x. [DOI] [PubMed] [Google Scholar]
- 28.Ramesh K, Kunjappan S, Ramesh M, Shankar S, Reddy S. Comparative evaluation of predictive value of three caries activity tests-snyder, lactobacillus count and cariostat in mixed dentition children with and without caries. J Pharm Bioallied Sci. 2013;5:S63–8. doi: 10.4103/0975-7406.113299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Marsh PD. Dental plaque as a biofilm and a microbial community-Implications for health and disease. BMC Oral Health. 2006;6(Suppl 1):S14. doi: 10.1186/1472-6831-6-S1-S14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Saxsena S, Pundir S, Aena J. Oratest: A new concept to test caries activity. J Indian Soc Pedod Prev Dent. 2013;31:25–8. doi: 10.4103/0970-4388.112400. [DOI] [PubMed] [Google Scholar]
- 31.Desai VB, Chiranjeevi, Thakur L. A clinico-pathological study; Evaluation of gingival inflammation using Oratest. J Indian Soc Periodontol. 1997;21:68–70. [Google Scholar]
- 32.Thorntol HR, Hastings EG. Studies on oxidation and reduction in milk. J Bacteriol. 1929;19:293–318. doi: 10.1128/jb.18.5.293-318.1929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Cardash HS, Rosenberg M. An innovative method of monitoring denture hygiene. J Prosthet Dent. 1990;63:661–4. doi: 10.1016/0022-3913(90)90323-5. [DOI] [PubMed] [Google Scholar]
- 34.Motohashi M, Yamada H, Genkai F, Kato H, Imai T, Sato S, et al. Employing dmft score as a risk predictor for caries development in the permanent teeth in Japanese primary school girls. J Oral Sci. 2006;48:233–7. doi: 10.2334/josnusd.48.233. [DOI] [PubMed] [Google Scholar]