

Abstract
Aim:
The aim of this study is to compare the different caries diagnostic thresholds under epidemiological and clinical settings among 7-15 year old school children.
Materials and Methods:
A cross-sectional study was undertaken among 7-15 years old school children of Bangalore city. Total 738 children were enrolled in the study. General information was collected regarding oral hygiene practice and personal habits of the schoolchildren. Subsequently, examination was done under both the settings to record Decayed, missing and filled surfaces index for permanent teeth (DMFS) and Decayed, missing and filled surfaces index for deciduous teeth (dmfs) using the World Health Organization (WHO) and WHO + IL criteria.
Results:
The present study showed that both the settings (clinical and epidemiological) and diagnostic thresholds (WHO and WHO + IL), could influence the detection of carious lesions. Mean Ds under WHO + Initial lesions (IL) criteria (3.92 + 3.49) was nearly double of WHO criteria (1.88 + 2.73,) and the influence observed was more in 14 years of age, where mean Ds under WHO + IL criteria (5.43 + 2.5) which was more than double of WHO criteria (2.02 + 1.9).
Conclusion:
The choice of a diagnostic threshold (WHO and WHO + IL) and the conditions of examination (epidemiological and clinical) are important for the detection of caries.
Keywords: Caries diagnostic thresholds, dental caries, initial carious lesion
INTRODUCTION
Dental caries has been described as a disease involving the localized destruction of the tooth tissue by microorganisms. It is a chronic disease process that usually progresses slowly and infrequently is self-limiting. Dental caries can affect enamel, dentine, and cementum. It manifests clinically along a continuum from initial loss of mineral to the complete tooth destruction.[1] Over the last few decades, the pattern of dental caries has undergone a profound change, and consequently, there has been a large number of initial lesions (IL), a reduction in cavitated lesion and the predominance of activity on the occlusal surfaces. These modifications in the pattern of the dental caries are very relevant, not only for clinicians, but also for epidemiologists and oral health service planner.[2] Not all non cavitated lesions progress to become dentinal lesions requiring restorative treatment; and, a good proportion of them remain static or even rematerialize, especially the smooth surface lesions. These lesions are thus reversible, as opposed to a dentinal lesion, which is generally considered irreversible. Because there are usually more non cavitated than cavitated lesions, at any one time in both high-caries and low -caries population,[3,4] the decision as to whether to include or exclude them, can make a substantial difference in the oral health profile obtained.
Scientific literature has discussed epidemiological studies which use diagnostic criteria that consider caries as a cavitated lesion, e.g. the World Health Organization (WHO) diagnostic criteria. The point is that these studies have underestimated the dental caries in populations/groups, since initial lesion have been more prevalent than cavitated lesions. Dental health programs that focus only on the treatment of cavitated lesions are not enough to re-establish health in an individual/ population because they do not consider the different stages of carious lesion progression.[5] Surveys that include IL could be very relevant to show distinct preventive and operative needs. The present study aims to investigate the influence of different diagnostic thresholds and different settings (epidemiological and clinical) on caries detection in the primary and permanent teeth of 7-15 year old school children of Bangalore city, India.
MATERIALS AND METHODS
The study was approved by the Ethical Committee in Research at M. S. Ramaiah Dental College, Bangalore (India). The schools granted permission for the study and informed consent was obtained from the parents.
Sample and examiners
The sample was calculated by the age group, based on caries experience of pilot survey carried out in a school of Bangalore City. The highest sampling error was 5% in a confidence level of 95%. The final sample was of 738 participants, 7-15 year-old children who were randomly selected from the schools. Children with oral or general problems, such as children with fixed orthodontic treatment, severe dental fluorosis, and serious systemic disease were excluded from the sample. Two examiners with clinical experience and epidemiological experience in surveys using WHO criteria (WHO, 1997) participated in the study.
Diagnostic thresholds and diagnostic criteria
Two diagnostic thresholds were used in the study: WHO diagnostic thresholds (WHO, 1997), where caries was defined as cavitated lesions only; and WHO + IL diagnostic threshold, where active IL were also defined as caries. The unit of evaluation used in examination was the DMFS and dmfs (decayed, missing, and filled surfaces for permanent and primary dentition, respectively). The criteria were those based on the WHO recommendations (WHO, 1997). Active caries with intact surfaces were recorded as IL: an adaptation of the criteria according to Nyvad et al. (1999) and Fyffe et al. (2000). Thus, IL are defined as active caries which, through visual assessment by a calibrated examiner, indicate an intact surface, no clinically detectable loss of dental tissue, a whitish-/yellowish coloured area of increased opacity, rough surface with loss of lustre and surfaces presumed to be carious; and, when the probe is used, its tip moves gently across the surface. For the smooth surface, the caries lesion is typically located close to gingival margin. For the occlusal surface, the lesion extends along the walls of the fissure.
Calibration of examiners
Three examiners were calibrated prior to the study. Examinesr were trained and calibrated in the diagnosis of IL using similar criteria as in other studies by Biscaro et al., 2000 and Assaf et al., 2004. The training and calibration exercise was carried out in both the settings. Mean inter-examiner agreement, measured using a Kappa calculation (Landis and Koch, 1977) were, Kappa = 0.87 for the WHO + IL, and Kappa = 0.95 for the WHO diagnostic threshold under epidemiological conditions, and Kappa = 0.90 for the WHO + IL diagnostic threshold under a traditional clinical setting.
Examination procedures for the epidemiological and clinical settings
All subjects were examined using a dental mirror and ball-ended probes with a diameter of 0.5 mm for removing the debris and assessing presence of fissure sealants, and to check the surface texture of IL, associated with previous dental drying in both the epidemiological and clinical settings by the two examiners. Prior to examination, dental drying was carried out for approximately 5 seconds per tooth with the use of compressed air through a dental compressor. All clinical examinations followed the epidemiological examinations due to practical reasons. A minimum interval of 15 days between the epidemiological and clinical examinations was established to avoid examiners' familiarity to the clinical conditions of the volunteers.
Epidemiological examinations
The examinations of cleaned and dried teeth were carried out in an outdoor setting under standardised conditions using natural light. Examinations were only performed on days with an appropriate natural luminosity.
Examinations in clinical settings
The examinations were carried out using the same method of exam and diagnostic adjuncts as the epidemiological examinations, except for the additional use of artificial light. Children were positioned in the dental chair as closely as possible to that used in the epidemiological setting, so that the dental chairs were not fully reclined. Re-examinations were done in 10% of the sample for each epidemiological and clinical examination.
Statistical analysis
Data obtained subjected to statistical analysis using Statistical Package for Social Sciences (SPSS) version 16. Descriptive statistics was used to obtain mean Ds, DMFT, ds, dmfs and One - sample Paired t test was used to compare Ds, DMFT, ds, dmfs means according to different diagnostic thresholds and settings.
RESULTS
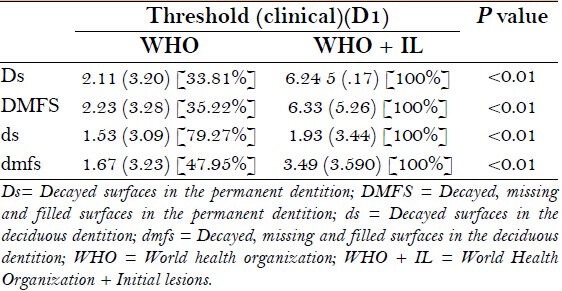
There were total 738 subjects, which included 261 (35%) boys and 477 (65%) girls. All the school children were stratified in to 9 age groups, ranging from 7 to 15 years old. Table 1 depicts comparison of mean Ds, DMFS, ds and dmfs under epidemiological examinations using both the criteria. WHO criteria showed significant differences (P < 0.001). With WHO criteria, the percentages of underestimation observed were 48% for D component and 86% for ds. Table 2 depicts comparison of mean ds, dmfs, Ds and DMFS under both the setting, using WHO + IL criteria. Results showed that epidemiological examinations presented with significant differences (P < 0.001). In epidemiological setting, the percentages of underestimation observed were 62.8% for D, and 81% for ds. Table 3 depicts the comparison of mean Ds, DMFS, ds and dmfs under epidemiological examinations using both the criteria. Result showed significant differences when both the criteria were compared (P < 0.001). The percentage of underestimation observed for D component was maximum for the 8 years age group (35%), followed by the 14 years age group (37%), and least for the 13 years age group (57%). For ds, it varied from 79.7% (for 10 years age) to 94.2% (for 15 years age). Table 4 depicts the comparison of the Mean ds, dmfs, Ds and DMFS of the epidemiological examinations to the clinical setting, both using WHO + IL criteria. Results showed significant differences when both the setting were compared (P < 0.001). The percentages uof nderestimation observed for D component were maximum for 7 years age group (27.4%), followed by the 8 years age group (55.7%) and least for 11 years age group (75%). For ds, it varied from 76.8% (for 11 years age) to 84% (for 12 years age). Table 5 depicts the comparison of mean Ds, DMFS, ds and dmfs under clinical setting using both the criteria. Results show that WHO criteria presented with significant differences when compared to the WHO + IL criteria (p < 0.01). With WHO criteria, the percentages of underestimation observed were 34% for the D component, followed by 35% for DMFS, 48% for dmfs, and 79% for ds.
Table 1.
Comparison of mean Ds, DMFS, ds and dmfs under epidemiological examinations using WHO and WHO + IL diagnostic threshold for all the age groups
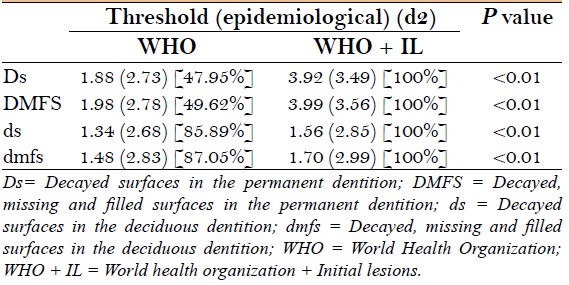
Table 2.
Comparison of mean ds, dmfs, Ds and DMFS under epidemiological setting and clinical setting, both using WHO + IL criteria
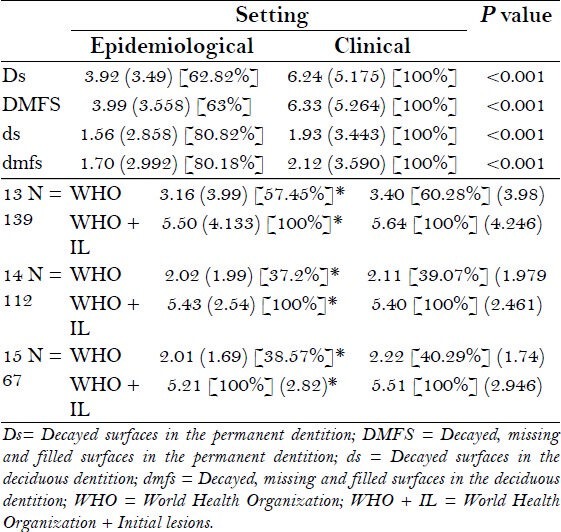
Table 3.
Comparison of mean Ds, DMFS, ds and dmfs under epidemiological examinations using WHO and WHO + IL criteria according to 7-15 year-old age group
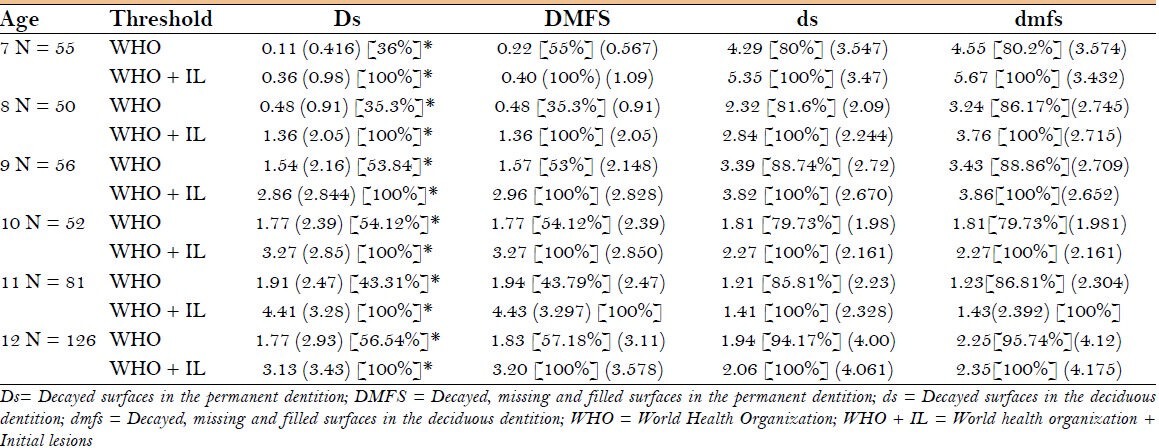
Table 4.
Mean ds, dmfs, Ds and DMFS of the epidemiological examinations compared to examinations done in clinical setting, both using WHO + IL criteria, according to 7-15 years old group
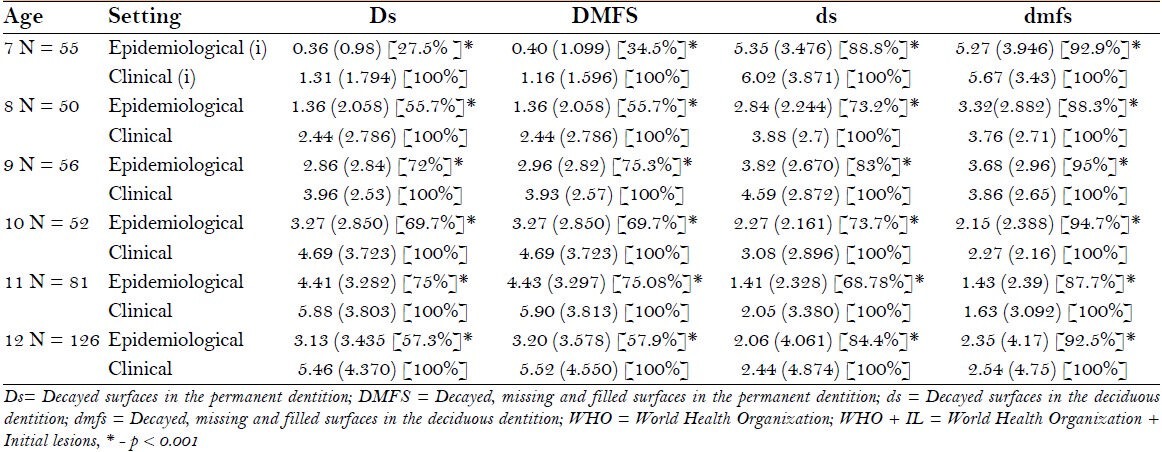
Table 5.
Shows comparison of mean Ds, DMFS, ds and dmfs under clinical examinations using WHO and WHO + IL criteria for all the age groups
DISCUSSION
Surveys are used to monitor the trends in oral health and disease, to develop policy, to evaluate dental health programmes, and to assess the dental needs.[5] However, when the epidemiological data are compared with those obtained in the standard clinical setting, epidemiological surveys underestimate the prevalence of the disease.[6] Furthermore, authors such as Kassawara et al.[5] Assaf et al.[6] Lindwood et al.[7] have justified that the epidemiological evaluation of dental caries is a poor indicator for determining the number of surfaces that will subsequently be treated[8,9] and has no discriminatory power in the prediction of an individual's future restorative treatment.[10] Difference in the examination methods of both the settings (epidemiological and clinical setting) may be a relevant factor in the accurate estimation of the disease magnitude in the surveys, for instance; artificial light, compressed air, radiographs and other diagnostic aids (Fibre optic transillumination - FOTI) are frequently used by dentists in clinical setting, while epidemiologists usually use only clinical examinations under conditions very different from those found in a clinical setting.[5,6,11]
In addition to these factors, the criteria employed in most of the cross- sectional surveys consider dental caries only at the point of cavitation, excluding the initial lesion, thus resulting in an underestimation of the disease magnitude which interferes with further planning. Many researchers have stressed on the need to introduce modifications in the diagnostic criteria for dental caries, mainly under epidemiological conditions. Because of the significant changes in the manifestation of the dental caries in the last few decades, such as a reduction in the prevalence of caries and decrease in the progressive speed of the lesion[4,8] and remineralisation of initial lesions, recent epidemiological research has shown that initial lesions have become more prevalent than the cavitated dentin lesions[5,12] Therefore, the real condition of the disease in the population has been underestimated, and this can consequently generate inadequacies in the data for implementing e the therapeutic non-invasive measures to control the progression of the disease.[13,14]
Thus, the objectives of the present study were; i) to compare the different caries diagnostic thresholds under epidemiological setting. ii) and, to compare these diagnostic thresholds under the epidemiological and clinical settings. The present study showed that both the settings (clinical and epidemiological) and diagnostic thresholds (WHO and WHO + IL) could influence on the detection of the carious lesions in 6 - 15 years old children. The inclusion of IL in the epidemiological examinations could be an important and relevant factor in the accurate estimation of disease magnitude. Mean Ds under WHO + IL criteria (3.92 ± 3.49) was nearly double of the WHO criteria (1.88 ± 2.73) [Table 3], and the influence observed was more in the age group of 14 year olds, where mean Ds under WHO + IL criteria (5.43 ± 2.5) was more than double of the WHO criteria alone (2.02 ± 1.9). Authors such as Nuttall et al.,[12] Meneghim et al.,[15] Andrea,[16] Ismil[3] have shown the need and justification for including IL in the epidemiological surveys. The reason is that there is a higher prevalence of IL compared to cavitated lesions, particularly in the low caries prevalence areas. Therefore, its inclusion would contribute to a decrease in the level of underestimation of the disease magnitude, and would provide a better classification of the dental caries levels in the population.[14]
Some other researchers demonstrated[14] that the pattern of dental caries has been undergoing profound modifications in the industrialized countries over the last few decades, showing drastic decrease in prevalence and incidence of the disease, and consequently, increase in the number of children who are free of dental caries.[5,10] Most of this epidemiological research still uses the criteria of dental caries as cavitated lesions.
In the present study, examination was also performed in a clinical setting, with variation in the use of the light source and compressed air. In the epidemiological setting, natural light and chip blower were used, whereas artificial light and compressed air were used in the clinical setting. It was observed that when both the settings were compared using same criteria (WHO + IL), clinical examination showed almost 40% more carious lesion than epidemiological examination.[5,17]
This influence of the light source is well evaluated in the previous studies.[13] White spot lesions, loss of discontinuity of the enamel surface, and determination of the depth of penetration can be well appreciated in the artificial light, and therefore helps in the diagnosis of the initial[13] as well as cavitated lesions.[18] In epidemiological examinations, this could be one more reason for the underestimation of IL.[12]
One of the previous studies has shown that the use of diagnostic adjuncts, such as prior tooth brushing and drying were more important than the employment of the Community Periodontal Index (CPI) dental probe, mirror or blade to diagnose non cavitated (NC) carious lesions in the enamel, mainly for the low caries prevalence group.[8,10] However, even with the employment of the diagnostic adjuncts of dental drying and brushing, the results of these studies showed that none of the combinations for the epidemiological examinations approached the diagnosis obtained in the dental setting in relation to the IL diagnosis for any of the two prevalence groups.[6] Such information, once again, confirms the difficulties in examining the dental caries and underestimation in epidemiological examinations. Epidemiological surveys are very important for obtaining the data of the disease magnitude in a population. Such data is frequently used in health care planning, monitor service delivery and track disease trends,[19] to plan preventive programs for the school and community and to assess the effectiveness of heath programs at school and community levels. In spite of this, even with such solid justifications for including IL in epidemiological surveys, continued research is needed so that future epidemiological information may capture the carious conditions more accurately. Thus, such changes can aid in deciding how funds should be directed to adequately meet the needs of the individuals and groups in question.[6,14] Furthermore, this would guide the public health service planning processes, and lead to improvements in the diagnosis and preventive-therapeutic treatments in the dental health programmes.
Some of the studies have evaluated the conventional clinical examination by using a method of validation, such as the determination of the depth of the lesion by minimal operative intervention. Such validation methods are currently not used in clinical research, although, this is a ‘gold standard’ for detecting caries. In the present study, this was not possible due to the practical and ethical issues, such as the ethical problem of opening a lesion.
Some epidemiologists consider that one of the major problems lies in the difficulty of diagnosing dental caries in epidemiological surveys because of the examination conditions, the resources employed, the inherent difficulties in diagnosing initial lesions, the time spent on the evaluation, as well as the high cost of diagnostic adjuncts.[20,21] At the present time, it is necessary to make the changes in the caries diagnostic threshold, and in the examination conditions (good quality light such as FOTI, additional diagnostic adjuncts like brushing and drying during examinations), for the development of epidemiological survey techniques and to evaluate the accurate magnitude of the disease in different groups. In addition, further studies should be directed to analyze the feasibility of adopting this new measure.
CONCLUSION
Overall, it was found that both the settings (clinical and epidemiological) and diagnostic thresholds (WHO and WHO + IL), could influence the detection of carious lesions in the 7- 15 year old children.
The major conclusions from the study are
The choice of a diagnostic threshold (WHO and WHO + IL) and the conditions of examination (epidemiological and clinical) are important for the detection of caries.
The inclusion of IL in the epidemiological examinations contributed to the reduction of caries underestimation among children aged 7-15 years old. Influence was more evident for the decayed component in the deciduous and permanent dentition.
In the present study, examination was also done in a clinical setting, the only source of variation being use of artificial light, with only natural light used in the epidemiological setting. This had a great influence on detecting the decayed component of the permanent teeth, with clinical examination showing almost 40% more carious lesions than the epidemiological examination.
The examination adjuncts, such as dental drying and artificial light, improved the dental caries diagnosis significantly.
It was observed that some of the major problems in correctly diagnosing the dental caries in epidemiological surveys are the examination conditions, the resources employed, the inherent difficulties in diagnosing the initial lesions, the time spent on the evaluation, as well as the high cost of diagnostic adjuncts.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Oral Health Surveys – Basic Methods. 4th ed. Geneva: World Health Organization Publications; 1997. [Google Scholar]
- 2.Harris NO. Primary Preventive Dentistry. 6th ed. 2004. pp. 46–54. [Google Scholar]
- 3.Ismail AI. Visual and Visuo-tactile Detection of Dental Caries. J Dent Res. 2004;83:C56–66. doi: 10.1177/154405910408301s12. [DOI] [PubMed] [Google Scholar]
- 4.School of Dentistry. Course: Operative Dentistry IV: Current concepts in Operative Dentistry: An evidence-based approach. 2001. Aug 28, Available from: http://www1.umn.edu/dental/courses/dent_6806fall03/paper2/incipientcaries03.PDF .
- 5.Kassawara AB, Assaf AV, Meneghim Mde C, Pereira AC, Topping G, Levin K, et al. Comparison of epidemiological evaluations under different caries diagnostic thresholds. Oral Health Prev Dent. 2007;2:137–44. [PubMed] [Google Scholar]
- 6.Assaf AV, Meneghim MC, Zanin L, Mialhe FL, Pereira AC, Ambrosano GM. Assessment of different methods for diagnosing dental caries in Epidemiological surveys. Community Dent Oral Epidemiol. 2004;34:418–25. doi: 10.1111/j.1600-0528.2004.00180.x. [DOI] [PubMed] [Google Scholar]
- 7.Lindwood M, Long JR, Richard G, Long LM, Jr, Rozier RG, Bawden JW. Estimation of actual caries prevalence and treatment needs from field survey caries information on a child population in U.S.A. Community Dent Oral Epidemiol. 1979;7:322–9. doi: 10.1111/j.1600-0528.1979.tb01241.x. [DOI] [PubMed] [Google Scholar]
- 8.Amarante Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Community Dent Oral Epidemiol. 1998;26:87–94. doi: 10.1111/j.1600-0528.1998.tb01933.x. [DOI] [PubMed] [Google Scholar]
- 9.Assaf AV, de Castro Meneghim M, Zanin L, Tengan C, Pereira AC. Effect of different diagnostic thresholds on dental caries calibration - a 12 month evaluation. Community Dent Oral Epidemiol. 2006;34:213–9. doi: 10.1111/j.1600-0528.2006.00278.x. [DOI] [PubMed] [Google Scholar]
- 10.Sköld UM, Klock B, Rasmusson CG, Torstensson T. Is caries prevalence underestimated in today's caries examination. A study on 16-year-old children in the county of Bohuslän, Sweden? Swed Dent J. 1995;19:213–7. [PubMed] [Google Scholar]
- 11.Bader JD, Daniel A, Arthur J. Bonito. Systematic Review of the Performance of Methods for Identifying Carious Lesions. J Public Health Dent. 2002;62:201–13. doi: 10.1111/j.1752-7325.2002.tb03446.x. [DOI] [PubMed] [Google Scholar]
- 12.Nuttall NM, Deery C. Predicting the experience of dentinal caries or restorative dental treatment in adolescents using D1 and D3 visual caries assessments. Community Dent Oral Epidemiol. 2002;30:329–34. doi: 10.1034/j.1600-0528.2002.300502.x. [DOI] [PubMed] [Google Scholar]
- 13.Nyvada B, Machiulskienec V, Baelumb V. Reliability of a New Caries Diagnostic System Differentiating between Active and Inactive Caries Lesions. Caries Res. 1999;33:252–60. doi: 10.1159/000016526. [DOI] [PubMed] [Google Scholar]
- 14.Assaf AV, Tengan C, da Silva Tagliaferro EP, Meneghim ZP, de Castro Meneghimo M, Pereira, et al. Influence of initial carious lesion on oral health planning. Braz J Oral Sci. 2006;5:1217–22. [Google Scholar]
- 15.Meneghim C, Assaf AV, Zanin L. Comparison of diagnostic methods for dental caries. J Dent Child (Chic) 2003;70:115–9. [PubMed] [Google Scholar]
- 16.Zandoná AF, Zero DT. Diagnostic tools for early caries detection. J Am Dent Assoc. 2006;137:1675–84. doi: 10.14219/jada.archive.2006.0113. [DOI] [PubMed] [Google Scholar]
- 17.Ismile AI. clinical diagnosis of precavitated carious lesions. Community Dent Oral Epidemiol. 1997;25:13–23. doi: 10.1111/j.1600-0528.1997.tb00895.x. [DOI] [PubMed] [Google Scholar]
- 18.Seppä L, Hausen H. Frequency of initial caries lesions as predictor of future caries increment in children. Scand J Dent Res. 1988;96:9–13. doi: 10.1111/j.1600-0722.1988.tb01401.x. [DOI] [PubMed] [Google Scholar]
- 19.Burt BA. How useful are cross-sectional data from surveys of dental caries? Community Dent Oral Epidemiol. 1997;25:36–41. doi: 10.1111/j.1600-0528.1997.tb00897.x. [DOI] [PubMed] [Google Scholar]
- 20.Pitts NB. Safeguarding the quality of epidemiological caries data at a time of changing disease patterns and evolving dental services. Community Dent Health. 1993;10:1–9. [PubMed] [Google Scholar]
- 21.Howat AP, Holloway PJ, Brandt RS. The effect of diagnostic criteria on the sensitivity of dental epidemiological data. Caries Res. 1981;15:117–23. doi: 10.1159/000260510. [DOI] [PubMed] [Google Scholar]