

Abstract
Objective:
To record prevalence of malocclusion among 2,400 adolescents in Karnataka state, India and to define difference in malocclusion status in urban and rural population.
Design:
Randomized cross-sectional study.
Setting:
School students of Karnataka state, 24 August 2011 to 30 March 2012.
Participants:
School students in the age group of 13-17 years.
Materials and Methods:
Each individual was assessed for occlusal traits - sagittal occlusion, overjet, overbite, crowding, midline diastema, and crossbite.
Statistical Analysis Used:
Examinations were computerized and analyzed using Statistical Package for Social Sciences version 16. Chi-square test was used for computing statistical significance.
Results:
87.79% of population had malocclusion. Out of which 89.45% had class I, 8.37% had class II, and 2.14% had class III malocclusion. Normal overjet and overbite was seen in 48.22 and 49.87% of subjects, respectively. Frequency of crowding was 58.12% and 15.43% of subjects had midline diastema. Anterior crossbite was present in 8.48% and posterior crossbite in 0.99%. Urban population had twice the class II sagittal occlusion, and increased overjet as compared to rural population.
Conclusions:
Malocclusion is widely spread among population of Karnataka state, with greater prevalence in urban population. Early exfoliation of deciduous teeth and refined diet can be considered as viable etiological factors.
Keywords: Buccal occlusion, crossbite, crowding, malocclusion, midline diastema, overjet, overbite, prevalence, saggital occlusion
INTRODUCTION
Significance of any disease in particular area can be gazed by its prevalence. This becomes even more important for developing country like India where oral health program and preventive measures are far from satisfying needs.
Prevalence of malocclusion has been studied in adolescents of Cicero,[1] Negro children of Columbia,[2] Black American children in the Evanston-Oak Park of Illinois[3] Minnesota,[4] Indiana and Kikuyu tribe of Kenya,[5] Korean cleft patients,[6] Hvar Island Croatia,[7] Italian students,[8] Hungarian population,[9] Naples,[10] Iranian school children,[11] and Tanzanian school children.[12]
Karnataka state, is an active agriculture place with people from a wide spectrum of cultural and religion background. To date there is no available data on status of prevalence of malocclusion in Karnataka. Thus aim of the study was to record prevalence of malocclusion and to define difference in malocclusion status in urban and rural population.
MATERIALS AND METHODS
The sample size was determined from a pilot study conducted at Hassan district. Thus, the study was conducted among 2,400 school students in the age group of 13-17 years. The study group was taken both from urban and rural areas in the proportion of 1:2, respectively from 30 districts of Karnataka using simple random sampling procedure. [Table 1 and Figure 1]
Table 1.
Distribution of sample
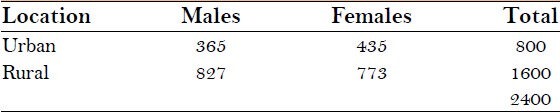
Figure 1.
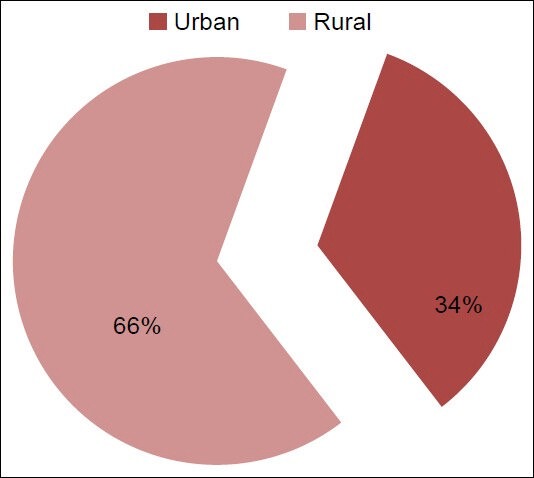
Normal population distribution
Inclusion criteria
No previous orthodontic treatment done
Secondary dentition present with no remaining deciduous teeth
All had their first permanent molars.
The criterion was limited to occlusal anterio-posterior (A-P) relationship, crowding,[13] overjet,[13] overbite,[13] midline diastema,[13] and crossbite.
Informed consent was taken and was confirmed by one of the parent.
Examination procedure
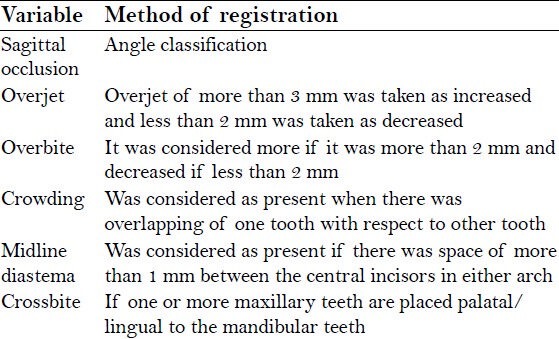
Each subject was examined by a single examiner with aid of natural light. Torch was used whenever required. Occlusal characteristics were assessed with the help of mouth mirror and metallic scale [Table 2].
Table 2.
Method of registration
The study was conducted over a period of 7 months starting from 24 August 2011 - 30 March 2012.
RESULTS
12.21% had class I normal occlusion. 15.43% of rural and 9% of urban population had class I normal occlusion with statistically significant difference between rural and urban population (P = 0.000) [Figure 2]. Class I sagittal occlusion was found in 89.45% of the subjects, Class II in 8.37%, and Class III in 2.14% with statistically significant difference (P = 0.00) between two groups [Table 3 and Figure 3].
Figure 2.
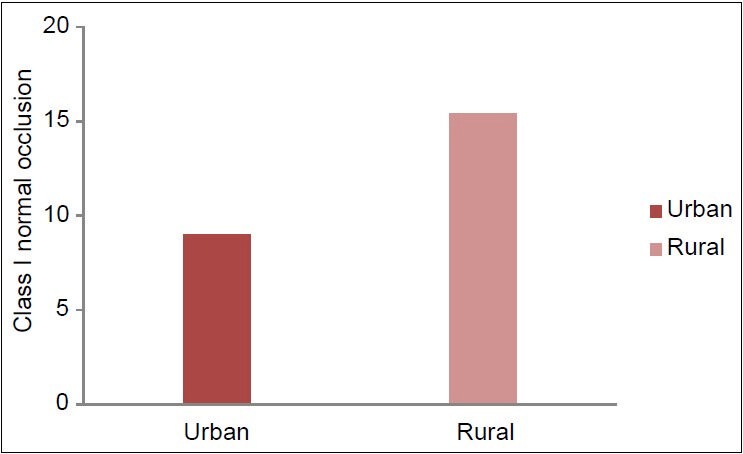
Prevalence of normal occlusion
Table 3.
Prevalence of occlusal traits
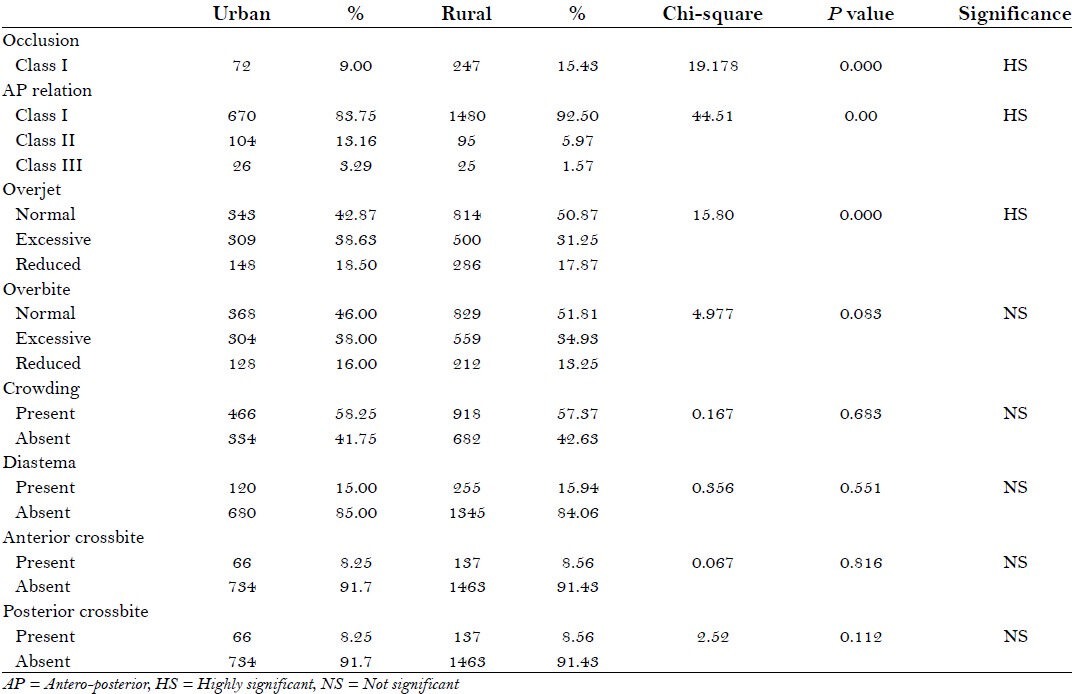
Figure 3.
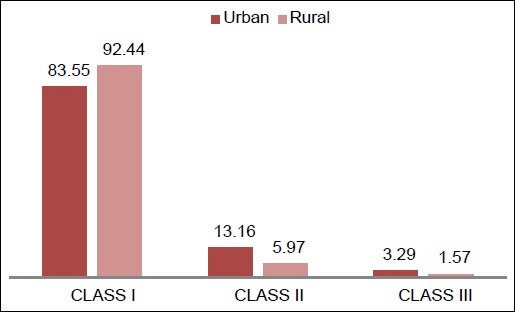
Anteroposterior molar relation
Normal overjet was seen in 48.22%, excessive in 33.71%, and reduced in 18.07% [Figure 4]. The difference between urban and rural population was statistically significant (P = 0.000) with urban population having more of increased overjet. Normal overbite was seen in 49.87%, deep in 35.97%, and reduced in 14.15% of total sample with no statistically significant difference between urban and rural population (P = 0.083) [Table 3 and Figure 5].
Figure 4.
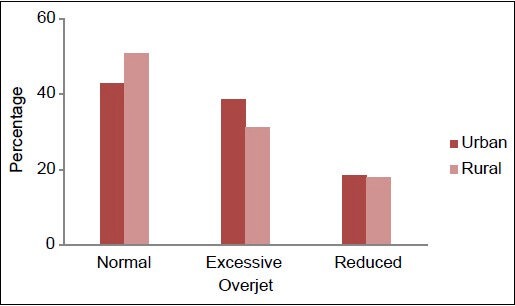
Distribution of overjet
Figure 5.
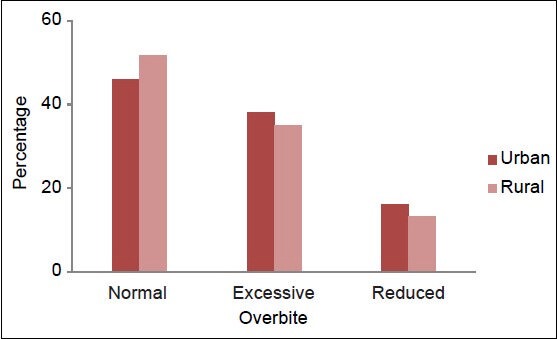
Distribution of overbite
The frequency of crowding was 58.12%. Urban population had 58.25% and rural had slightly less (57.37%), but difference was not statistically significant (P = 0.683) [Figure 6]. Midline diastema was present in 15.43% with no statistically significant difference (P = 0.551) between urban and rural population [Table 3 and Figure 7].
Figure 6.
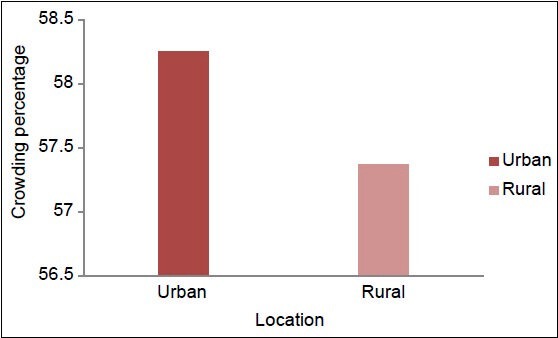
Prevalence of crowding
Figure 7.
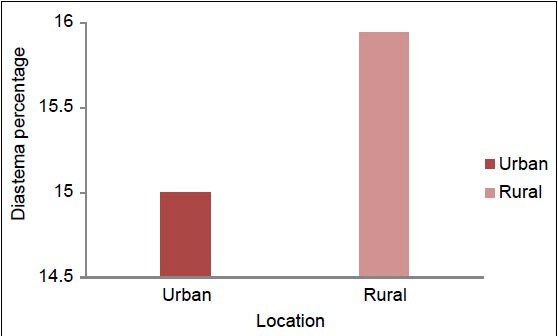
Prevalence of midline diastema
Anterior crossbite was present in 8.48% of subjects. Urban population had 8.25% and rural had 8.56% anterior crossbite with no statistically significant difference (P = 0.816) [Figure 8]. Posterior crossbite was present in 0.99%. Urban population had 1.25% and rural population of 0.69% had posterior cross bite with no statistically significant difference (P = 0.112) between two groups [Table 3 and Figure 9].
Figure 8.
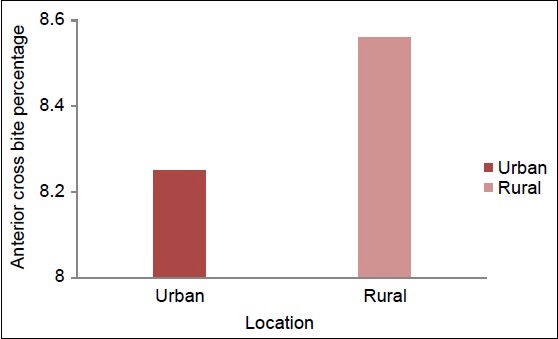
Prevalence of anterior crossbite
Figure 9.
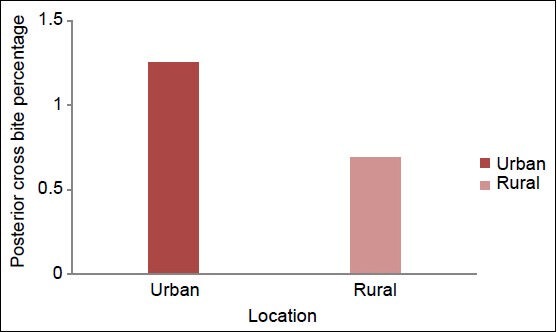
Prevalence of posterior crossbite
DISCUSSION
This survey provides the first estimate of prevalence of malocclusion in Karnataka state. Examination was confined to high school students because of ease of accessibility;[1] with a complete permanent dentition as malocclusion occurring in the mixed dentition is sometimes transitional leading to erroneous conclusions.
Qualitative and quantitative methods available for measuring malocclusion are not truly inclusive of all occlusal criteria,[1,14] thus, an alternative approach was used to register malocclusion by using occlusal characteristics. Angle's classification that is reliable, repeatable,[15] and idealistically oriented for a broad population study[16] was used for checking sagittal occlusion. Malocclusion has often been referred to as a “disease of civilization”, signifying that it is found (or at least reported) primarily in urbanized populations. This calls for rural-urban dichotomy.
Prevalence of malocclusion was high and comparative to studies[2,17,18,19] conducted by Rajendra in Bangalore city, Kharbandha in Delhi, by Altemus in Negro children, and U.S Public Health Survey. Findings of this present study were in disagreement with Guaba (1998)[20] in the district of Ambala (70.8 per cent had normal occlusion). Prevalence of malocclusion was comparatively less (7%) as compared to studies[21] conducted on Chinese.
Class I molar relation was almost the same as found in studies[4] conducted in Minnesota. There was a significantly higher prevalence of Class III occlusion among the Chinese, Malays, and blacks as compared to the Indians.[5,21] Prevalence of overjet and overbite found in present study was same as that in urban Iranian school children, Yoruba adolescents in Ibadan, Nigeria,[11,13] and study conducted on three ethnic races; Chinese, Malay, and Indian in Malaysia.[21]
Crowding was present in 57.69% of subjects. This was similar to the finding of Usha Mohan Das and Ali Borzabadi that crowding anterior was most common finding in subjects with class I malocclusion.[11,22] This was in accordance with study conducted by Woon[21] that stated crowded dentition was also a norm for the three races: Chinese, Malay, and Indian. Prevalence of crowding was same as seen in the Hvar island, Croatia; among Lithuanian school children; in Naples; in Rio de Janeiro State, Brazil; and Jordanian subjects,[7,10,23,24,25] Much less prevalence of crowding was seen among adolescents of Ibadan, Nigeria (20%),[13] Present study found midline diastema in 15.65% of subjects. This prevalence was much more as compared to study[26] conducted by Gnanasundaram and Hashim on prevalence of midline diastema (1.6%) in Chennai city. Prevalence of midline diastema was much less than adolescents of Ibadan, Nigeria (37%).[13] Anterior cross bite was present in 8.46% and posterior cross-bite was present in 0.88%. Posterior crossbite was recorded much more (8.8%) among Lithuanian schoolchildren; Rio de Janeiro State, Brazil (19.2%); urban Iranian school children; and in Lahore city (24%), Pakistan[11,23,24,27] Difference was much more as compared to Lahore city as in their study data was collected from patients who visited department of orthodontics.
Urban population had twice the class II sagittal occlusion and increased overjet as compared to rural population. This difference was similar to the study[28] done to assess occlusal variation in three southwest Pacific populations. Dietary consistency can be considered as viable reason as the posterior region of mandible is associated with muscles of mastication,[29] As far as anterior region is concerned habits can be considered as reason for discrepancy in urban and rural population. Further research is needed to determine whether there is association between above written factors and malocclusion.
This study is limited as it has only recorded malocclusion in age group of 13-17 years which cannot be generalized to entire population. Secondly, orthodontically treated cases were excluded which can underestimate the prevalence of occlusal traits. But the proportion of adolescents who underwent orthodontic therapy and excluded were relatively small and thus does not make statistically significant difference in results. Thirdly, there are considerable variations in figures obtained as different researchers have used different criteria for assessing the same occlusal trait. This lay emphasis on the need to standardize criteria for assessing malocclusion.
CONCLUSION
Malocclusion is widespread in population examined at Karnataka State, India. Prevalence of malocclusion was more in urban population when compared with rural population. Crowded incisors were the most common feature associated with class I malocclusion. Require further studies in area to find etiology for various occlusal traits.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Massler M, Frankel JM. Prevalence of malocclusion in children aged 14 to 18 years. Am J Orthod. 1951;37:751–68. doi: 10.1016/0002-9416(51)90047-4. [DOI] [PubMed] [Google Scholar]
- 2.Altemus LA. Prevalence of malocclusion in American Negro children. Quar Nat Dent A. 1960;18:31. [Google Scholar]
- 3.Enrich RE, Brodie AG, Blayney JR. Prevalence of class 1, class 2 and class 3 malocclusion in an urban population. An epidemiological study. J Dent Res. 1965;44:947–53. doi: 10.1177/00220345650440053301. [DOI] [PubMed] [Google Scholar]
- 4.Grewe JM, Cervenka J, Shapiro BL, Witkop CJ., Jr Prevalence of malocclusion in Chippewa Indian Children. J Dent Res. 1968;47:302–5. doi: 10.1177/00220345680470021701. [DOI] [PubMed] [Google Scholar]
- 5.Garner LD, Butt MH. Malocclusion in black Americans and Nyeri Kenyans. An epidemiologic study. Angle Orthod. 1985;55:139–46. doi: 10.1043/0003-3219(1985)055<0139:MIBAAN>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Baek SH, Moon HS, Yang WS. Cleft type and Angle's classification of malocclusion in Korean cleft patients. Eur J Orthod. 2002;24:647–53. doi: 10.1093/ejo/24.6.647. [DOI] [PubMed] [Google Scholar]
- 7.Lauc T. Orofacial analysis on the Adriatic islands: An epidemiological study of malocclusions on Hvar Island. Eur J Orthod. 2003;25:273–8. doi: 10.1093/ejo/25.3.273. [DOI] [PubMed] [Google Scholar]
- 8.Ciuffolo F, Mnzoli L, Attilio DM, Tecco S, Muratore F, Festa F, et al. Prevalence and distribution by gender of occlusal characteristics in a sample of Italian secondary school students: A cross-sectional study. Eur J Orthop. 2005;27:601–6. doi: 10.1093/ejo/cji043. [DOI] [PubMed] [Google Scholar]
- 9.Gábris K, Márton S, Madléna M. Prevalence of malocclusions in Hungarian adolescents. Eur J Orthop. 2006;28:467–70. doi: 10.1093/ejo/cjl027. [DOI] [PubMed] [Google Scholar]
- 10.Perillo L, Masucci C, Ferro F, Apicella D, Baccetti T. Prevalence of orthodontic treatment need in southern Italian schoolchildren. Eur J Orthop. 2010;32:49–53. doi: 10.1093/ejo/cjp050. [DOI] [PubMed] [Google Scholar]
- 11.Borzabadi-Farahani A, Borzabadi-Farahani A, Eslamipour F. Malocclusion and occlusal traits in an urban Iranian population. An epidemiological study of 11 to 14-year-old children. Eur J Orthop. 2009;31:477–84. doi: 10.1093/ejo/cjp031. [DOI] [PubMed] [Google Scholar]
- 12.Mtaya M, Brudvik P, Astrom AN. Prevalence of malocclusion and its relationship with socio-demographic factors, dental caries, and oral hygiene in 12 to 14-year-old Tanzanian schoolchildren. Eur J Orthod. 2009;31:467–76. doi: 10.1093/ejo/cjn125. [DOI] [PubMed] [Google Scholar]
- 13.Onyeaso CO. Prevalence of malocclusion among adolescents in Ibadan, Nigeria. Am J Orthod Dentofacial Orthop. 2004;126:604–7. doi: 10.1016/j.ajodo.2003.07.012. [DOI] [PubMed] [Google Scholar]
- 14.Kerr J, Buchanan IB, McColl JH. The use of PAR in assessing the effectiveness of removable orthodontic appliances. Br J Orthod. 1993;20:351–7. doi: 10.1179/bjo.20.4.351. [DOI] [PubMed] [Google Scholar]
- 15.Silva RG, Kang DS. Prevalence of malocclusion among Latino adolescents. Am J Orthod Dentofacial Orthop. 2001;119:313–5. doi: 10.1067/mod.2001.110985. [DOI] [PubMed] [Google Scholar]
- 16.Graber TM. Orthodontic: Principles and Practice. 3rd ed. Philadephia: WB Saunders Co; 1972. [Google Scholar]
- 17.Peter S. Essentials of Preventive and Community Dentistry. 3rd ed. New Delhi: Arya Publishing House; 2006. [Google Scholar]
- 18.Kharbandha OP, Sidhu SS, Shukla DK, Sunderan KR. A study of etiologic factors associated with the development of malocclusion. J Clin Pediatr Dent. 1994;18:95–8. [PubMed] [Google Scholar]
- 19.Naumann SA, Behrents RG, Buschang PH. Vertical components of overbite change: A mathematical model. Am J Orthod Dentofacial Orthop. 2000;117:486–95. doi: 10.1016/s0889-5406(00)70170-3. [DOI] [PubMed] [Google Scholar]
- 20.Guaba K, Ashima G, Tewari A, Utreja A. Prevalence of malocclusion and abnormal oral habits in North Indian rural children. J Indian Soc Pedod Prev Dent. 1998;16:26–30. [PubMed] [Google Scholar]
- 21.Woon KC, Thong YL, Abdul Kadir R. Permanent dentition occlusion in Chinese, Indian and Malay groups in Malaysia. Aust Orthod J. 1989;11:45–8. [PubMed] [Google Scholar]
- 22.Das UM, Venkatsubramanian, Reddy D. Prevalence of malocclusion among school children in Bangalore, India. Int J Clin Ped Dent. 2008;1:10–2. doi: 10.5005/jp-journals-10005-1002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sidlauskas A, Lopatiene K. The prevalence of malocclusion among 7-15 year-old Lithuanian schoolchildren. Medicina (Kaunas) 2009;45:147–52. [PubMed] [Google Scholar]
- 24.Proffit WR, Fields HW. Contemporary Orthodontics. 4th ed. Chicago: Mosby Year Book; 2007. [Google Scholar]
- 25.Al-Ibrahim HM, Telfah HD, Hyasat AN. Frequency of malocclusion in an orthodontically referred Jordanian population. J R Med Sci. 2010;17:19–23. [Google Scholar]
- 26.Nainar SM, Gnanasundaram N. Incidence and etiology of midline diastema in a population in south India (Madras) Angle Orthod. 1989;59:277–82. doi: 10.1043/0003-3219(1989)059<0277:IAEOMD>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 27.Saqib N, Saad A, Waheed-Ul-Hamid Prevalence of crossbite in orthodontic patients. Pakistan Oral Dental J. 2009;29:2. [Google Scholar]
- 28.Smith RJ, Bailit HL. Variation in dental occlusion and arches among Melanesians of Bougainville Island, Papua New Guinea. I. Methods, age changes, sex differences and population comparisons. Am J Phys Anthropol. 1977;47:195–208. doi: 10.1002/ajpa.1330470202. [DOI] [PubMed] [Google Scholar]
- 29.Mcfaddan LR, Mcfadden KD. Effect of controlled dietary consistency and cage environment on the rat mandibular growth. Anat Rect. 1986;215:390–6. doi: 10.1002/ar.1092150409. [DOI] [PubMed] [Google Scholar]