

Abstract
Objective:
To investigate whether greater cardiorespiratory fitness (CRF) is associated with better cognitive function 25 years later.
Methods:
We studied 2,747 participants in the community-based Coronary Artery Risk Development in Young Adults Study of black and white men and women aged 18 to 30 years at recruitment in 1985–1986 (baseline year 0). Symptom-limited maximal treadmill test durations at years 0 and 20 provided measures of CRF. Cognitive tests at year 25 measured verbal memory (Rey Auditory Verbal Learning Test [RAVLT]), psychomotor speed (Digit Symbol Substitution Test [DSST]), and executive function (Stroop Test).
Results:
Per minute of baseline CRF, the RAVLT was 0.12 words recalled higher (standard error [SE] = 0.03, p < 0.0001), the DSST was 0.92 digits higher (SE = 0.13, p < 0.0001), and the Stroop Test score was 0.52 lower (better performance, SE = 0.11, p < 0.0001), after accounting for race, sex, age, education, and clinical center. Compared with the lowest quartile of CRF, each cognitive test was 21% to 34% of an SD better in the highest CRF quartile. Further adjustment for lifestyle and clinical measures attenuated coefficients for RAVLT and DSST slightly, while the coefficient predicting the Stroop Test lost more than half its value (p = 0.07). Analysis in the subset of 1,957 participants who also completed the year-20 treadmill test showed that 20-year change in CRF was positively associated only with DSST (p < 0.001).
Conclusions:
Better verbal memory and faster psychomotor speed at ages 43 to 55 years were clearly associated with better CRF 25 years earlier.
Cardiorespiratory fitness (CRF), which may be modified by physical activity and weight changes,1,2 is a potential target for intervention to prevent cognitive function decline with aging. Recent studies showed a positive association between CRF and cognitive function. In participants older than 55 years, higher baseline CRF was associated with smaller decline over 6 years on a modified Mini-Mental State Examination and better performance on cognitive tests 6 years later.3 In a meta-analysis of 18 studies, CRF improvement through exercise training was associated with better executive, spatial, and speed function among healthy adults aged 55 and older or those with mild mental disorders and cardiopulmonary obstructive.4 In addition, lower CRF correlated with progression of dementia severity in Alzheimer disease.5
By age 55 years, pathophysiologic changes underlying both loss of CRF and loss of cognitive function may already have occurred.2,6–8 No longitudinal studies have investigated the relation between CRF and cognitive function in healthy young and middle-aged adults. Therefore, investigating the association between CRF and cognitive function in the Coronary Artery Risk Development in Young Adults (CARDIA) Study would allow us to gain a better understanding of the pathogenesis of cognitive function in adulthood. We hypothesized that baseline CRF, defined by symptom-limited maximal treadmill test duration, and its change over 20 years are associated with cognitive function in midlife.
METHODS
Study design.
CARDIA is a multicenter longitudinal study of cardiovascular risk factors in adults between the ages of 18 and 30 years when recruited in 1985–1986 (year 0, Y0). Recruitment was at random from the general population in Birmingham, AL, Chicago, IL, and Minneapolis, MN, and from members of the Kaiser Permanente Medical Care Plan in Oakland, CA. The full CARDIA sample at Y0 was balanced by age (45% aged 18–24 years; 55% aged 25–30 years), race (52% black; 48% white), sex (46% men; 54% women), and education (40% completed ≤12 years; 60% >12 years).9–11 Seven follow-up examinations occurred at years 2, 5, 7, 10, 15, 20, and 25, with 91%, 86%, 81%, 79%, 74%, 72%, and 72% of the surviving cohort returning, respectively. Our analysis includes men and women who did symptom-limited treadmill exercise tests at Y0 and cognitive testing at Y25. In addition, we studied the subset who also did the treadmill test at Y20 as part of the ancillary CARDIA Fitness Study.
Standard protocol approvals, registrations, and patient consents.
The institutional review boards for the protection of human subjects for all study sites provided approval for the study, and written informed consent was obtained from all participants.
Data collection.
Graded exercise testing.
The graded symptom-limited maximal exercise test followed a modified Balke protocol, consisting of nine 2-minute stages of gradually increasing difficulty (see e-Methods on the Neurology® Web site at Neurology.org).12 Maximal duration of symptom-limited exercise on a treadmill (Maxdur) was the primary exposure. Maxdur is a close approximation of cardiovascular fitness and of the true physiologic maximum oxygen consumption per unit time (V̇o2max) on a treadmill.13
Cognitive function assessment.
At the Y25 examination, 3 standardized tests were conducted to measure cognitive function, including verbal memory, psychomotor speed, and executive function, which are typically impaired in people with cardiovascular risk factors.14 Selection of these tests considered the feasibility of delivering standardized tests in multiple sites by trained lay staff in accommodation with scheduled time flow, good distribution of the scores in the CARDIA cohort age group, and being previously used in other large studies of cognition.15,16 The Rey Auditory Verbal Learning Test (RAVLT) assesses memory, including the ability to memorize and retrieve words (verbal memory).17 The long delay (10 minutes) free recall (range 0–15 words) was analyzed. More words recalled indicates better performance. The Digit Symbol Substitution Test (DSST) mainly assesses psychomotor speed. It evaluates visual motor speed, sustained attention, and working memory.18 The range of digits correctly substituted by symbols is 0 to 133; more correct digits indicates better performance. The Stroop Test evaluates executive function, including the ability to view complex visual stimuli and respond to one stimulus dimension while suppressing the response to another dimension.19 The test was scored by seconds to state spelled out color words printed in a different color ink, plus number of errors (score range: 1–160); thus, higher seconds + errors indicates worse performance.
Measurements of other variables.
Covariates have been described previously20–27; details are in e-Methods.
Analytic sample and exclusion criteria.
The exercise test was performed by 4,966 and 2,871 participants at Y0 and Y20 across all CARDIA clinics, respectively. For the main analysis of the Y0 Maxdur (minutes), we excluded 34 tests of participants with concurrent β-blocker medication use and 299 tests that were terminated for medical reasons not relevant to fitness. Some participants met more than one exclusion criteria, leaving 4,637 treadmill tests for data analysis. Of these 4,637 participants, 3,036 who completed Y25 cognitive function tests were initially considered for the analysis; 289 tests with missing covariates were further excluded. Therefore, 2,747 participants were analyzed for the association between Y0 Maxdur and cognitive function. The excluded were more likely than those included to be black, to be smokers, and to have lower educational attainment, although all of those groups were well represented among those included. The 1,957 of 2,747 participants with both eligible Y0 and Y20 treadmill tests were included in the analysis involving change of Maxdur over 20 years. As we previously noted,6 poor treadmill performance at baseline predicted failure to perform the test at Y20. Thus, although the CARDIA Study tested a broad range of people at Y20, the Y20 sample is biased toward people with somewhat better fitness as evidenced by a higher baseline Maxdur in participants who attended both Y0 and Y20 tests (n = 1,957) compared with those who only attended Y0 tests (n = 790) (10.2 [2.8] vs 9.5 [2.9] minutes, p < 0.0001). Overall, participants who performed both Y0 and Y20 treadmill tests were slightly healthier in lifestyle, weight, blood pressure, and kidney function at Y0 than those who performed only the Y0 treadmill test (data not shown).
Statistical analysis.
Assumptions of normality of fitness, cognitive function measurements, and covariates were checked. Baseline characteristics and means of Y25 cognitive function tests were examined across race- and sex-specific quartiles of Maxdur. The t and χ2 tests were used to compare the differences in the means and percents between groups. Multiple linear regressions were applied to assess the associations of baseline Maxdur and change of Maxdur over 20 years with cognitive function at Y25. Baseline Maxdur was analyzed as a continuous variable as well as in race- and sex-specific quartiles, and linearity was tested for these associations. Three models were tested subsequently to account for potential confounding. Age, sex, race, education, and clinical center were adjusted in minimally adjusted models; diet, physical activity, smoking, drinking, body mass index (BMI), and forced expiratory volume in 1 second were further adjusted in moderately adjusted models; and blood pressure, cholesterol, diabetes status, and glomerular filtration rate were additionally adjusted in fully adjusted models. However, blood pressure, cholesterol, diabetes status, and glomerular filtration rate may be causally linked to cognitive function with Maxdur, so adjustment for them might represent an explanation of the mechanism of association. Sensitivity analysis of the Y0 treadmill test was conducted by replacing missing covariates with the corresponding value at a later examination or race- and sex-specific means (thus, n = 3,036). Interactions between Y0 Maxdur and race, sex, and education level on cognitive function tests were tested.
All statistical testing was performed using 2-sided tests with the significance level of type I error (α) set at 0.05. Statistical analyses were performed using PC-SAS 9.2 (SAS Institute Inc., Cary, NC).
RESULTS
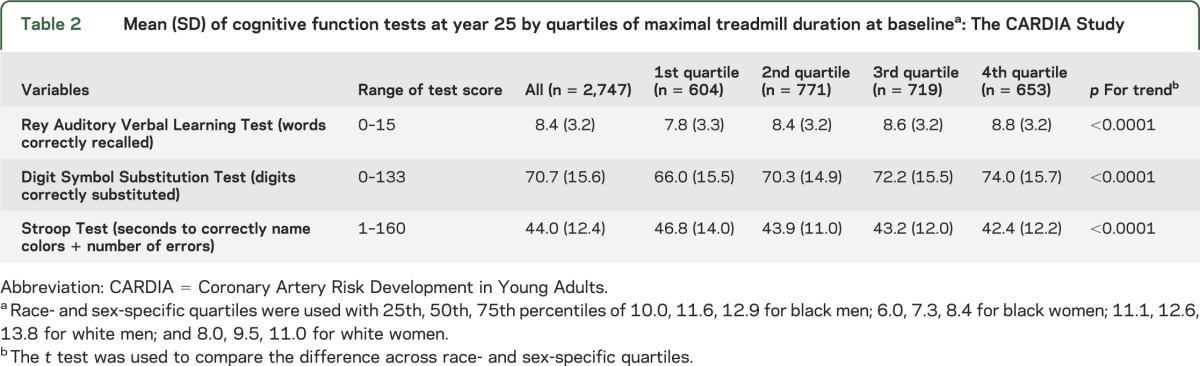
At Y0, the average age of the cohort was 25 years, with 45% black participants and 56% women. The cohort was apparently healthy regarding lifestyle and clinical measures at Y0. Baseline Maxdur differed across race-sex groups (p < 0.001). Maxdur (mean ± SD) was 10.0 ± 2.8 minutes for all participants at Y0; 11.3 ± 2.1 for black men, 7.3 ± 1.9 for black women, 12.4 ± 2.1 for white men, and 9.5 ± 2.1 for white women. The decrease of Maxdur over 20 years was 2.9 ± 2.0 minutes for the 1,957 participants; 3.6 ± 2.1 for black men, 2.5 ± 1.8 for black women, 3.1 ± 1.8 for white men, and 2.5 ± 1.9 for white women (p < 0.001). Specifically, differences in Y0 characteristics were observed across race- and sex-specific quartiles of Y0 Maxdur. Those who were more fit were more likely to be better educated, nonsmoker, physically active, and normotensive. They watched less TV, had a lower BMI, higher quality of diet, and lower total cholesterol (table 1). At Y25, mean number of words correctly recalled after a long delay was 8.4 ± 3.2; 70.7 ± 15.6 digits were correctly substituted in DSST, and 44.0 ± 12.4 seconds + errors was the score for correctly naming colors in the Stroop Test 3 (table 2).
Table 1.
Baseline characteristics by quartiles of maximal treadmill duration at baselinea: The CARDIA Study

Table 2.
Mean (SD) of cognitive function tests at year 25 by quartiles of maximal treadmill duration at baselinea: The CARDIA Study
For each additional minute attained on the treadmill at Y0, there were 0.12 (standard error [SE] = 0.03, p < 0.0001) more words correctly recalled 10 minutes after 5 presentations of a list of 15 words in RAVLT; 0.92 (SE = 0.13, p < 0.0001) more digits correctly substituted in DSST; and 0.52 (SE = 0.11, p < 0.0001) fewer seconds + errors during the Stroop Test, after accounting for race, sex, age, attained education level at Y0, and clinical center (table 3). The difference in this model between the fourth and first quartiles of Maxdur corresponds to 21%, 34%, and 25% of the sample SD of the test score in the RAVLT, DSST, and Stroop Test, respectively (figure). Further adjustment for dietary pattern, physical activity, smoking, BMI, alcohol consumption, and forced expiratory volume in 1 second attenuated the associations slightly. Additional adjustment for blood pressure, cholesterol, diabetes status, and glomerular filtration rate yielded a similar trend for each of these cognitive function tests and maintained statistical significance for the RAVLT and DSST (table 3, figure). The full models account for 23%, 30%, and 21% of the variance in RAVLT, DSST, and Stroop Test scores, although the treadmill duration measures added <0.03 to r2. Although the figure visually suggests that the slope of the cognitive function tests is greater from the lowest to the second lowest quartile than it is across the higher quartiles, tests for nonlinearity were all nonsignificant. An additional model adjusting for history of cardiovascular disease (positive in 67 of the 2,747 participants) did not substantively alter conclusions (data not shown). Sensitivity analysis of the Y0 treadmill test with missing covariates replaced by the corresponding value at a later examination or race- and sex-specific means (n = 3,036) yielded similar findings (data not shown). No interactions were identified between Y0 Maxdur and either race-sex groups (see table e-1) or education level on cognitive function tests (all p > 0.05 with df = 3 for Maxdur/race-sex interaction, and df = 2 for Maxdur/education interaction).
Table 3.
Association between cognitive function tests and Maxdur at baseline (n = 2,747) and at year 20 (n = 1,955) and its change over 20 years (n = 1,955): The CARDIA Study
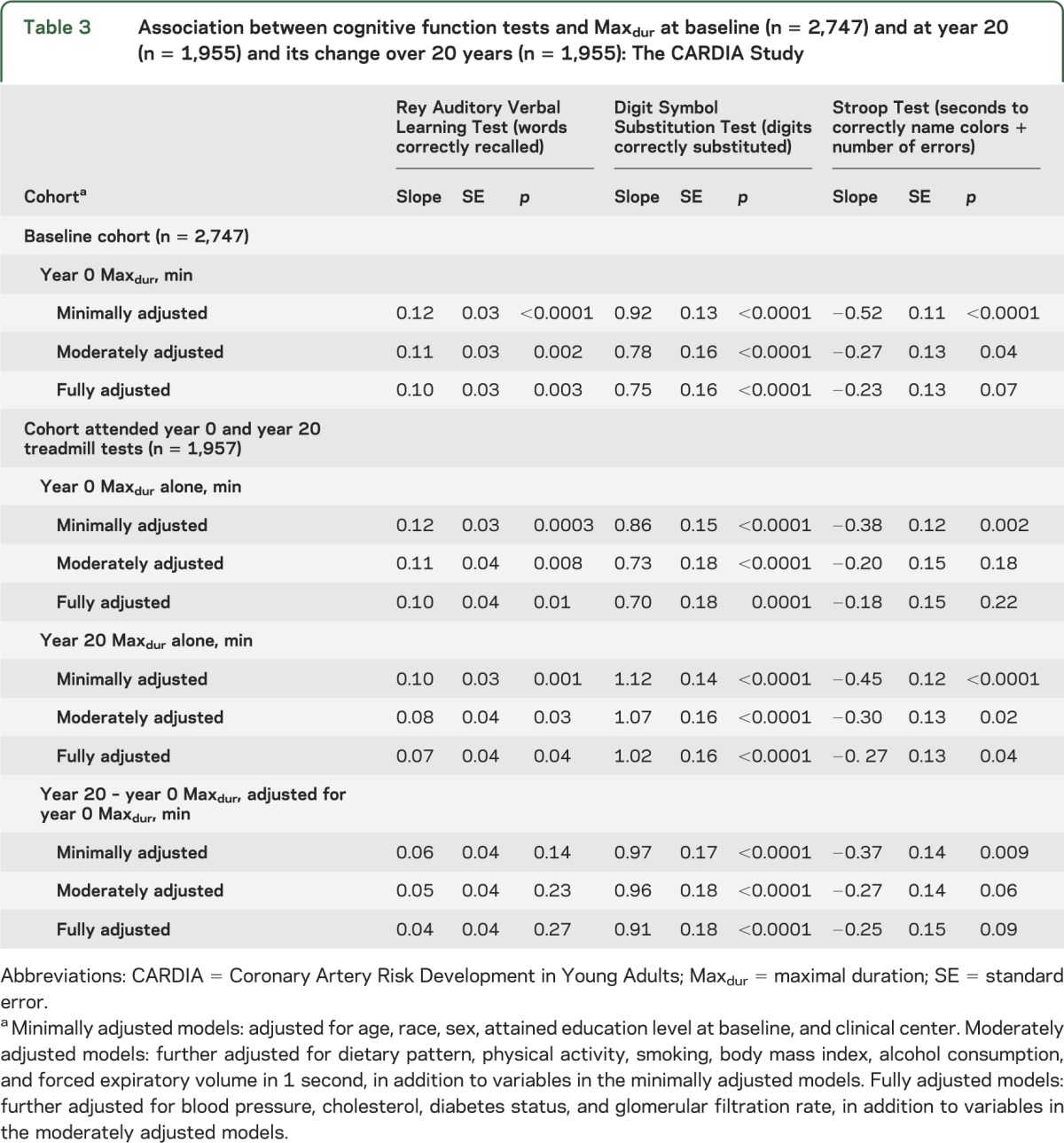
Figure. Linear regression and means of cognitive function tests within quartiles of Maxdur at year 0.

(A) RAVLT, (B) Stroop Test, and (C) DSST. Minimally adjusted models were adjusted for age, race, sex, attained education level at baseline, and clinical center. As a measure of goodness of fit, means of Maxdur within each race- and sex-specific quartile of Maxdur at baseline (x-axis) were plotted against adjusted means of cognitive function tests, RAVLT, DSST, and Stroop, respectively (y-axis). Fully adjusted models were further adjusted for dietary pattern, physical activity, smoking, body mass index, alcohol consumption, forced expiratory volume in 1 second, blood pressure, cholesterol, diabetes status, and glomerular filtration rate, in addition to the variables in the minimally adjusted models. Means were plotted as a measure of goodness of fit. DSST = Digit Symbol Substitution Test; Maxdur = maximal duration; RAVLT = Rey Auditory Verbal Learning Test.
Different models including Y0 Maxdur alone and Y20 Maxdur alone were further assessed among the 1,957 participants with both treadmill tests available (table 3). The RAVLT was better predicted by Maxdur at Y0 (25 years earlier) than Maxdur at Y20 (5 years earlier) as evidenced by a relatively smaller effect size with Y20 Maxdur (0.12 vs 0.10, corresponding to 0.6% SD more words correctly recalled for each additional minute attained on the treadmill in the minimally adjusted model). DSST and Stroop Test were better predicted by Maxdur 5 years earlier than Maxdur 25 years earlier (1.12 vs 0.86, corresponding to 1.7% SD more digits correctly substituted and −0.45 vs −0.38, corresponding to 0.6% SD fewer seconds + errors for each additional minute attained on the treadmill in the minimally adjusted model) (table 3). Of the 1,957 participants who also completed the Y20 treadmill test, 1,795 participants decreased Maxdur over 20 years (8.2% had a longer Maxdur at year 20 than at Y0). The change of Maxdur over 20 years was positively associated with number of digits correctly substituted in DSST at Y25. For each additional minute lost on the treadmill over 20 years, there were 0.97 (SE = 0.17, p < 0.0001) fewer digits correctly substituted in DSST, with adjustment for Y0 Maxdur, race, sex, age, attained education level at baseline, and clinical center. Further adjustment retained the association for DSST. No associations were observed between the change of Maxdur over 20 years and the performance for RAVLT and Stroop Test.
DISCUSSION
In the current study, higher CRF measured by Maxdur at the average age of 25 years was positively associated with better performance in cognitive function tests, including the RAVLT and DSST, assessed 25 years later, but not the Stroop Test. The smaller decrease (or improvement in 163 of 1,957 participants) of CRF over 20 years was associated with better DSST performance. Our findings confirm that the previously detected association of CRF with cognitive function in older adults also holds for CRF assessed in young adulthood and cognitive function in middle-aged adults. Furthermore, it is shown for the DSST (psychomotor speed) and Stroop Test (executive function) that the closer in time the treadmill test is to the cognitive tests, the stronger the predictive value of Maxdur on cognitive function test results. However, the magnitude of association with the RAVLT-memory was greater for the earlier measure of CRF.
Our findings of the association between change in Maxdur with DSST accord with previous findings of a meta-analysis of 18 studies in elderly participants showing that fitness improvement after months of exercise training was associated with both psychomotor speed and all types of cognitive function.4 Specifically, one study conducted among 33 elderly participants with mild cognitive function impairment after 6 months of a controlled exercise intervention showed that increasing V̇o2peak, a measure of CRF, was associated with improved performance in DSST specifically in the 17 female participants.28 While the cognitive tests were measured directly after several months of aerobic exercise intervention in the latter trial, the change in CRF observed in our study was registered over 20 years in free-living individuals and 5 years before the measurements of RAVLT, DSST, and Stroop Test. This design difference could have attenuated the putative positive fitness effect on memory and executive function. Another consideration is that memory, psychomotor speed, and executive function may not be equally robust as people age. However, future study with measurement of baseline cognitive function in middle-aged populations is needed to clarify the effect of change in CRF on cognition in this population.
The observed association between CRF and cognitive function may have multiple mechanisms. One possible mechanism is that low CRF leads to morphologic brain changes, including white matter lesions29–32 and brain atrophy in certain regions in gray matter,5 which in turn related to impaired cognitive function in the elderly.33–36 However, CRF may alter cognitive function through regulation of cerebral blood flow37 or a direct molecular pathway beyond vascularization, such as influencing N-acetylaspartate, a metabolite exclusively in cell bodies of neurons, given its identified mediating effect between the association of fitness and Backward Digit Span performance.38
The large population-based sample of young to middle-aged adults who had symptom-limited maximal treadmill tests conducted at 2 examinations 20 years apart and cognitive function tested 25 years later is the main strength of the current study. Our study is the first prospective cohort study in middle-aged adults investigating the association between CRF and cognitive function. Our results are generalizable in young to middle-aged adults because of its sampling at baseline, which was community-based and demographically balanced, and the inclusion of smokers and persons who were obese. In addition, multiple treadmill testing allowed us to study the association between change of Maxdur over 20 years and cognitive function, and to further demonstrate the long-term effect of Maxdur on cognitive function in young and middle adulthood.
Several limitations of this current study should be noted. One is that identical aspects of cognitive function were not assessed at the Y0 examination. Consequently, it was difficult to test the temporality of the association between Maxdur and cognitive function. Indeed, cognitive function may or may not have changed much since early adulthood (CARDIA baseline) or even childhood. Future CARDIA examinations will be needed to look at the time course of cognitive function as participants age. Residual confounding caused by unmeasured confounders may exist even though the CARDIA Study has collected information on a wide range of variables, including physical activity, diet, and clinical variables. Also, caution should be taken when interpreting the independent associations between Y0 Maxdur and cognitive function tests, and Y20 Maxdur and cognitive functions tests, given the strong correlation between Y0 and Y20 Maxdur (r = 0.74). The effect for each additional minute on the treadmill on cognitive tests 25 or 5 years later may be modest, but the effect sizes were larger than the effect sizes associated with 1 year of age difference, which were 0.07 fewer words correctly recalled in RAVLT, 0.82 fewer digits correctly substituted in DSST, and 0.47 more seconds + errors during the Stroop Test. In addition, studies showed that DSST and RAVLT scores were among the strongest predictors of future dementia in older persons without dementia as well as in patients with mild cognitive impairment with memory plus other cognitive domain deficits in verbal memory, psychomotor speed, and executive function. Specifically, one study showed that every additional word provided on the RAVLT was associated with an 18% decrease in the risk of developing dementia after 10 years, while every additional symbol correctly substituted in the DSST was associated with a 5% decrease in the risk of developing dementia after 10 years.39,40 Therefore, our findings in people with average age 50 years are likely to be clinically meaningful in early identification of persons with high risk of developing dementia and potentially to prevent such conversion. Demonstrating such clinical utility is a long-term goal of the CARDIA Study.
CRF predicts aspects of cognitive function including verbal memory measured by RAVLT and psychomotor speed measured by DSST 25 years later, independent of other factors among apparently healthy middle-aged adults. CRF change over 20 years was positively associated with performance on DSST, but not RAVLT or Stroop Test. There is wide variation in cognitive function in our apparently healthy middle-aged sample, well before obviously impaired cognitive function begins to appear. This variation in cognitive function is strongly related to a measure of fitness obtained 25 years earlier.
Supplementary Material
GLOSSARY
- BMI
body mass index
- CARDIA
Coronary Artery Risk Development in Young Adults
- CRF
cardiorespiratory fitness
- DSST
Digit Symbol Substitution Test
- Maxdur
maximal duration
- RAVLT
Rey Auditory Verbal Learning Test
- SE
standard error
Footnotes
Supplemental data at Neurology.org
AUTHOR CONTRIBUTIONS
Dr. Zhu: wrote the manuscript and data analysis. Dr. Jacobs: wrote the manuscript, data analysis, and secured funding. Dr. Schreiner: critical review of the manuscript and secured funding. Dr. Thomas and Dr. Demerath: critical review of the manuscript. Dr. Sidney: critical review of the manuscript and secured funding. Dr. Yaffee, Dr. Bryan, Dr. Launer, Dr. Whitmer, Dr. He, Dr. Reis, and Dr. Sternfeld: critical review of the manuscript.
STUDY FUNDING
The Coronary Artery Risk Development in Young Adults (CARDIA) Study is supported by contracts HHSN268201300025C, HHSN268201300026C, HHSN268201300027C, HHSN268201300028C, HHSN268201300029C, and HHSN268200900041C from the National Heart, Lung, and Blood Institute and the Intramural Research Program of the National Institute on Aging, plus a grant for the CARDIA Fitness Study R01 HL 078972.
DISCLOSURE
N. Zhu, D. Jacobs, and P. Schreiner report no disclosures relevant to the manuscript. K. Yaffee has served on data safety monitoring boards for Takeda Inc., Pfizer Inc., and Medivation Inc. and served as a consultant for Novartis Inc. N. Bryan, L. Launer, R. Whitmer, S. Sidney, E. Demerath, and W. Thomas report no disclosures relevant to the manuscript. C. Bouchard serves as a scientific adviser to Weight Watchers, PepsiCo, Gatorade, Nike, and Pathway Genomics. K. He, J. Reis, and B. Sternfeld report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
REFERENCES
- 1.Sidney S, Sternfeld B, Haskell WL, Quesenberry CP, Crow RS, Thomas RJ. Seven-year change in graded exercise treadmill test performance in young adults in the CARDIA study. Med Sci Sports Exerc 1998;30:427–433 [DOI] [PubMed] [Google Scholar]
- 2.Zhu N, Jacobs DR, Sidney S, et al. Fat mass modifies the association of fat-free mass with symptom-limited treadmill duration in the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr 2011;94:385–391 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Barnes DE, Yaffe K, Satariano WA, Tager IB. A longitudinal study of cardiorespiratory fitness and cognitive function in healthy older adults. J Am Geriatr Soc 2003;51:459–465 [DOI] [PubMed] [Google Scholar]
- 4.Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci 2003;14:125–130 [DOI] [PubMed] [Google Scholar]
- 5.Vidoni ED, Honea RA, Billinger SA, Swerdlow RH, Burns JM. Cardiorespiratory fitness is associated with atrophy in Alzheimer's and aging over 2 years. Neurobiol Aging 2011;33:1624–1632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zhu N, Suarez-Lopez JR, Sidney S, et al. Longitudinal examination of age-predicted symptom-limited exercise maximum HR. Med Sci Sports Exerc 2010;42:1519–1527 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carnethon MR, Gidding SS, Nehgme R, Sidney S, Jacobs DR, Liu K. Cardiorespiratory fitness in young adulthood and the development of cardiovascular disease risk factors. JAMA 2003;290:3092–3100 [DOI] [PubMed] [Google Scholar]
- 8.Singh Manoux A, Kivimaki M, Glymour MM, et al. Timing of onset of cognitive decline: results from Whitehall II prospective cohort study. BMJ 2012;344:d7622–d7622 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cutter GR, Burke GL, Dyer AR, et al. Cardiovascular risk factors in young adults: the CARDIA baseline monograph. Control Clin Trials 1991;12(1 suppl):1S–77S [DOI] [PubMed] [Google Scholar]
- 10.Friedman GD, Cutter GR, Donahue RP, et al. CARDIA: study design, recruitment, and some characteristics of the examined subjects. J Clin Epidemiol 1988;41:1105–1116 [DOI] [PubMed] [Google Scholar]
- 11.Hughes GH, Cutter G, Donahue R, et al. Recruitment in the Coronary Artery Disease Risk Development in Young Adults (CARDIA) study. Control Clin Trials 1987;8(4 suppl):68S–73S [DOI] [PubMed] [Google Scholar]
- 12.Sidney S, Haskell WL, Crow R, et al. Symptom-limited graded treadmill exercise testing in young adults in the CARDIA study. Med Sci Sports Exerc 1992;24:177–183 [PubMed] [Google Scholar]
- 13.Pollock ML, Bohannon RL, Cooper KH, et al. A comparative analysis of four protocols for maximal treadmill stress testing. Am Heart J 1976;92:39–46 [DOI] [PubMed] [Google Scholar]
- 14.Gorelick PB, Scuteri A, Black SE, et al. Vascular contributions to cognitive impairment and dementia: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011;42:2672–2713 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Launer LJ, Miller ME, Williamson JD, et al. Effects of intensive glucose lowering on brain structure and function in people with type 2 diabetes (ACCORD MIND): a randomised open-label substudy. Lancet Neurol 2011;10:969–977 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Saczynski JS, Jónsdóttir MK, Garcia ME, et al. Cognitive impairment: an increasingly important complication of type 2 diabetes: the age, gene/environment susceptibility—Reykjavik study. Am J Epidemiol 2008;168:1132–1139 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schmidt M. Rey Auditory Verbal Learning Test: A Handbook. Los Angeles: Western Psychological Services; 1996 [Google Scholar]
- 18.Wechsler D. Wechsler Adult Intelligence Scale–III (WAIS-III). New York: Psychological Corporation; 1997 [Google Scholar]
- 19.Stroop J. Studies of interference in serial verbal reaction. J Exp Psychol 1935;18:643 [Google Scholar]
- 20.Wagenknecht LE, Perkins LL, Cutter GR, et al. Cigarette smoking behavior is strongly related to educational status: the CARDIA study. Prev Med 1990;19:158–169 [DOI] [PubMed] [Google Scholar]
- 21.McDonald A, Van Horn L, Slattery M, et al. The CARDIA dietary history: development, implementation, and evaluation. J Am Diet Assoc 1991;91:1104–1112 [PubMed] [Google Scholar]
- 22.Dyer AR, Cutter GR, Liu KQ, et al. Alcohol intake and blood pressure in young adults: the CARDIA study. J Clin Epidemiol 1990;43:1–13 [DOI] [PubMed] [Google Scholar]
- 23.Sidney S, Jacobs DR, Haskell WL, et al. Comparison of two methods of assessing physical activity in the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Epidemiol 1991;133:1231–1245 [DOI] [PubMed] [Google Scholar]
- 24.Sidney S, Sternfeld B, Haskell WL, Jacobs DR, Chesney MA, Hulley SB. Television viewing and cardiovascular risk factors in young adults: the CARDIA study. Ann Epidemiol 1996;6:154–159 [DOI] [PubMed] [Google Scholar]
- 25.Standardization of spirometry: 1994 update. American Thoracic Society. Am J Respir Crit Care Med 1995;152:1107–1136 [DOI] [PubMed] [Google Scholar]
- 26.Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J 2005;26:319–338 [DOI] [PubMed] [Google Scholar]
- 27.Carnethon MR, Sternfeld B, Schreiner PJ, et al. Association of 20-year changes in cardiorespiratory fitness with incident type 2 diabetes: the Coronary Artery Risk Development in Young Adults (CARDIA) fitness study. Diabetes Care 2009;32:1284–1288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Baker LD, Frank LL, Foster-Schubert K, et al. Effects of aerobic exercise on mild cognitive impairment: a controlled trial. Arch Neurol 2010;67:71–79 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sen A, Gider P, Cavalieri M, et al. Association of cardiorespiratory fitness and morphological brain changes in the elderly: results of the Austrian Stroke Prevention Study. Neurodegener Dis 2012;10:135–137 [DOI] [PubMed] [Google Scholar]
- 30.Prakash RS, Snook EM, Motl RW, Kramer AF. Aerobic fitness is associated with gray matter volume and white matter integrity in multiple sclerosis. Brain Res 2010;1341:41–51 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Burns JM, Cronk BB, Anderson HS, et al. Cardiorespiratory fitness and brain atrophy in early Alzheimer disease. Neurology 2008;71:210–216 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Honea RA, Thomas GP, Harsha A, et al. Cardiorespiratory fitness and preserved medial temporal lobe volume in Alzheimer disease. Alzheimer Dis Assoc Disord 2009;23:188–197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kuller LH, Shemanski L, Manolio T, et al. Relationship between ApoE, MRI findings, and cognitive function in the Cardiovascular Health Study. Stroke 1998;29:388–398 [DOI] [PubMed] [Google Scholar]
- 34.de Groot JC, de Leeuw FE, Oudkerk M, et al. Cerebral white matter lesions and cognitive function: the Rotterdam Scan Study. Ann Neurol 2000;47:145–151 [DOI] [PubMed] [Google Scholar]
- 35.Mosley TH, Jr, Knopman DS, Catellier DJ, et al. Cerebral MRI findings and cognitive functioning: the Atherosclerosis Risk in Communities Study. Neurology 2005;64:2056–2062 [DOI] [PubMed] [Google Scholar]
- 36.Debette S, Beiser A, DeCarli C, et al. Association of MRI markers of vascular brain injury with incident stroke, mild cognitive impairment, dementia, and mortality: the Framingham Offspring Study. Stroke 2010;41:600–606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Brown A, McMorris C, Longman RS, et al. Effects of cardiorespiratory fitness and cerebral blood flow on cognitive outcomes in older women. Neurobiol Aging 2010;31:2047–2057 [DOI] [PubMed] [Google Scholar]
- 38.Erickson K, Weinstein A, Sutton B, et al. Beyond vascularization: aerobic fitness is associated with N-acetylaspartate and working memory. Brain Behav 2012;2:32–41 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Tabert MH, Manly JJ, Liu X, et al. Neuropsychological prediction of conversion to Alzheimer disease in patients with mild cognitive impairment. Arch Gen Psychiatry 2006;63:916–924 [DOI] [PubMed] [Google Scholar]
- 40.Tierney MC, Moineddin R, McDowell I. Prediction of all-cause dementia using neuropsychological tests within 10 and 5 years of diagnosis in a community-based sample. J Alzheimers Dis 2010;22:1231–1240 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.