

Abstract
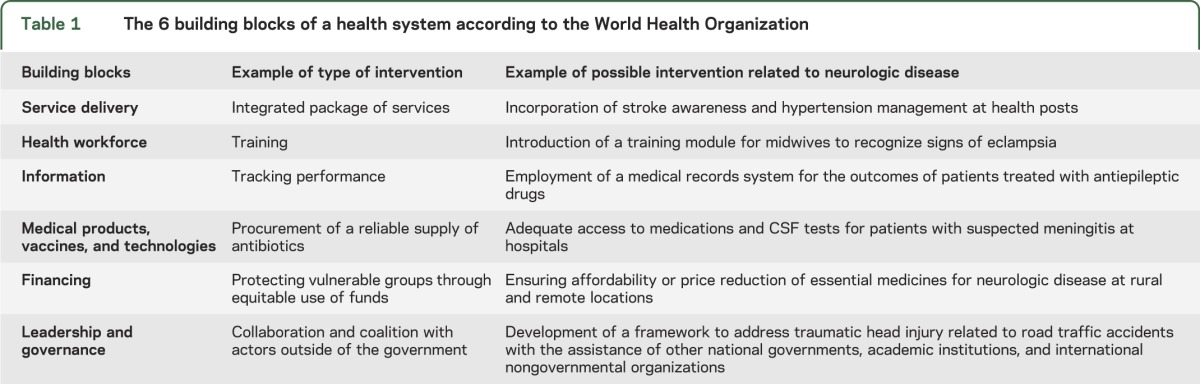
Neurologic care exists within health systems and complex social, political, and economic environments. Identification of obstacles within health systems, defined as “constraints,” is crucial to improving the delivery of neurologic care within its macroclimate. Here we use the World Health Organization's 6 building blocks of a health system to examine core services for priority interventions related to neurologic disease: (1) service delivery; (2) health workforce; (3) information; (4) medical products, vaccines, and technologies; (5) financing; and (6) leadership and governance. We demonstrate the use of a constraints analysis for neurologic disorders using the example of Timor-Leste, a newly sovereign and low-income country, which aims to improve neurologic care in the coming years.
Neurologic care exists within health systems and complex environments. A health system that functions well delivers “quality services to all people, where and when they need them.”1 Unlike traditional disease-, risk factor–, or resource-based approaches, health systems–based analyses permit a comprehensive approach to understanding neurologic care that incorporates economic, social, and political influences on health.
All health systems are imperfect. According to the World Health Organization (WHO), an ideal health system prioritizes equity of service delivery, improves the health of both individuals and communities, engages the participation of end users, and protects against health threats and the negative financial consequences of ill health.1 Identification of obstacles within health systems, defined as constraints, is crucial to improving the delivery of neurologic care within its macroclimate. A constraints analysis provides a conceptual approach to understanding well-known barriers to neurologic care and helps identify which interventions would most succeed at addressing them. For example, an absolute scarcity of resources is one of the most important constraints to neurologic care worldwide. Many scarcity issues can be solved by an infusion of funding; however, relaxation of constraints requires more than just funding. For it is not just the amount of money spent but rather how it is spent that can substantially improve neurologic care. In yet other cases, money itself may be unable to relax constraints on care provision since barriers to neurologic care may exist beyond the health system, including social limits to adoption of new technologies and the time required to achieve collective health goals.2
We are unaware of a constraints analysis for neurologic care in any country. We analyze the WHO's 6 building blocks of a health system and use Timor-Leste as an example to study core interventions and priority interventions (table 1). Timor-Leste was the first new sovereign state of the 21st century after gaining independence from Indonesia in 2002. It currently ranks 147th on the United Nations Human Development Index and is considered the poorest country in Asia. We focus on prevalent conditions to illustrate the building blocks of a health system related to neurologic care.
Table 1.
The 6 building blocks of a health system according to the World Health Organization
SERVICE DELIVERY
This includes raising demand for services, integrating services, organizing and managing providers, and ensuring appropriate infrastructure.1 Several examples of low demand for neurologic care are apparent in Timor-Leste. Awareness of neurologic disorders and their major risk factors is generally limited. Poverty, strong beliefs in traditional medicine and healers, and low levels of education are barriers to people seeking care. The poor condition of roads in mountainous terrain makes transport especially difficult for patients in rural and remote settings. In the Guido Valadares National Referral Hospital in the capital city of Dili, preventable diseases such as tetanus and eclampsia are seen with regularity. Individuals in rural villages do not routinely seek preventive care and often present late in the disease course. Although every major district in Timor-Leste is supplied with carbamazepine, some health districts report zero cases of epilepsy diagnosed in children younger than 5. Other disorders such as poststroke hypertension are treated for 30 days with little follow-up. There remain no targeted programs for neurologic diseases beyond epilepsy, with limited integration of neurologic care into existing community-based health services.
HEALTH WORKFORCE
Timor-Leste, like many low-income countries, has no permanent neurologist. There is 1 visiting Cuban neurologist and no neurology training program. The Faculty of Medicine and Health Sciences was recently established within the Timor-Leste National University. The Cuban Medical Institution trains many Timorese students who will return to Timor-Leste to become physicians. By 2017, it is anticipated there will be approximately 700 newly graduated physicians. The goal is for each village to have at least 1 physician, for a targeted ratio of 1 physician per 2,000 people by 2020. The incorporation of neurologic disease care into the training of physicians, nurses, midwives, pharmacists, and allied specialties will be crucial so that the workforce is aware of common neurologic problems and when to refer to higher levels of care. Currently, medical practitioners in the national hospital are from many different countries outside of Timor-Leste and have no common working language within the Timorese medical system.
INFORMATION
Surveillance practices capture neurologic diseases—specifically epilepsy and dementia—with variable success.3 National information systems and records systems are not organized to record most diseases. More importantly, health care workers are unable to fully recognize and diagnose neurologic disorders in many cases, making recorded data imperfect. Relationships with nongovernmental organizations have led to the distribution of information on epilepsy awareness for entry-level health providers at the district and subdistrict levels nationally. Measuring performance of existing efforts, implementing tools to ensure use of International Classification of Disease codes,4 and national surveillance for neurologic infectious diseases are required.
MEDICAL PRODUCTS, VACCINES, AND TECHNOLOGIES
All diagnostic equipment, crucial for neurologic care in most settings, is absent. For example, there is no EEG, EMG, imaging modality other than ultrasound, or functioning laboratory testing. There is 1 CT scanner, which has not been operational for several years in spite of efforts to have it fixed. There are no manufacturers of medicines in the country, requiring importation of all essential medicines. Drug stock outs, including essential antibiotics, are routine. Laboratory testing outside of the capital is even more limited and includes only blood glucose, acid-fast bacillus smear, urine β-human chorionic gonadotropin, and HIV tests. Emergency care is not routine. Donated ambulances exist but were noted to lack fuel in some locations.
FINANCING
Planning and coordination for chronic diseases have been considered important in recent years but fall below priorities to combat diarrhea, tuberculosis, and malaria. Vertical programming initiatives through large global funders emphasize communicable diseases and programs in Timor-Leste. Approaches to maternal-child health have also been major priorities with external financial investment. Reliance on donor funding since the violent breakup of the country in 1999 has created external influences on health priorities. There may be several ways to improve the efficiency of neurologic care in the future and help patients avoid personal financial catastrophe in the face of stroke, acute flaccid paralysis, and trauma.
LEADERSHIP AND GOVERNANCE
In the past 10 years, the government of Timor-Leste and its partners, including many nongovernmental organizations, have expanded health services to reach communities in rural villages through health posts, mobile clinics, and monthly integrated community health services. This model can be expanded to include disorders that will become prominent with the epidemiologic transition, including traumatic brain and spinal cord injury from road traffic accidents and stroke and dementia in the aging population. The need to address postinfectious disabilities, such as the sequelae of cerebral malaria, demonstrates the value of expanding the continuum of care to rehabilitation. Infrastructure available to the Timorese people is limited in general. Focus on the core issues of water and sanitation, telecommunications, and higher education would enable development in general.
FUTURE DIRECTIONS
By articulating the type and level of constraints for neurologic care, it may become easier to address and target the core needs of neurologic patients (table 2). A constraints analysis demonstrates how major international stakeholders can influence the provision of neurologic care, for example by focusing external funding on a disease of local need in the most useful ways. It also demonstrates that merely having available and affordable medications, such as carbamazepine for epilepsy, does not lead to improvements in treatment unless health care workers are educated and neurologic expertise is more permanent. There is a reciprocal relationship between encouraging people to seek care for neurologic disease in Timor-Leste and ensuring adequate care available.
Table 2.
Levels of constraints that may be experienced within a health system

Constraints are identified because they may be rapidly or gradually overcome.5 Since governments in many countries are aware of the ever-increasing burden of neurologic disease, a framework on how best to identify, treat, and prevent neurologic disease through health systems approaches will be crucial to scaling up sustainable care in many locations.
ACKNOWLEDGMENT
The authors thank Professor Robert E. Black, MD, MPH, Department of International Health, The Johns Hopkins University, Baltimore, MD, and Iris Hamelberg, London School of Tropical Medicine and Hygiene and Ministry of Health Timor-Leste, for comments and suggestions during the preparation of this manuscript.
AUTHOR CONTRIBUTIONS
Dr. Mateen was responsible for data acquisition, data interpretation, writing, and editing the manuscript. Dr. Martins was responsible for data acquisition, data interpretation, writing, and editing the manuscript.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
F. Mateen is supported by a grant from the Canadian Institutes of Health Research and the Johns Hopkins Bloomberg School of Public Health Sommer Scholars Program. N. Martins reports no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
REFERENCES
- 1.World Health Organization. Everybody’s business: strengthening health systems to improve health outcomes. In: WHO’s Framework Action. Geneva: WHO; 2007 [Google Scholar]
- 2.Hanson K, Ranson MK, Oliveira-Cruz V, Mills A. Expanding access to priority health interventions: a framework for understanding the constraints to scaling-up. J Int Dev 2003;15:1–14 [Google Scholar]
- 3.Government of Timor-Leste. Nacional Mental Health Strategy 2011-2015 for a Mentally Healthy Timor-Leste. Dili: Government of Timor-Leste; 2011 [Google Scholar]
- 4.Mateen FJ, Dua T, Shen GC, Reed GM, Shakir R, Saxena S. Neurological disorders in the 11th revision of the International Classification of Diseases. Lancet Neurol 2012;11:484–485 [DOI] [PubMed] [Google Scholar]
- 5.Travis P, Bennett S, Haines A, et al. Overcoming health-systems constraints to achieve the Millennium Development Goals. Lancet 2004;364:900–906 [DOI] [PubMed] [Google Scholar]