

Abstract
Aim:
The aim of the following study is to compare the evaluation of different irrigation activation system-F-File, CanalBrush (CB) and EndoActivator (EA) in removing smear layer from root canal.
Materials and Methods:
Root canals of eighty single rooted decoronated premolar teeth were instrumented using crown-down technique and then equally divided into four groups on basis of irrigation activation methods used: Without irrigation - control group, irrigation with F-File, CB, EA into Group I, II, III respectively. Samples were then longitudinally sectioned and examined under scanning electron microscope by three qualified observers using score from 1 to 4. Data was analyzed using Statistical Package for Social Sciences (SPSS), version 15.0 (SPSS Inc., Chicago IL) at significance level of P ≤ 0.05.
Results:
Minimum mean score was observed in Group II at coronal, apical locations. Group III had minimum score at middle third. Groups difference in score were found to be significant statistically for all three locations as well as for overall assessment (P < 0.001).
Conclusion:
CB remove smear layer more efficiently from the root canal than F-File and EA in coronal and apical region.
Keywords: Biomechanical preparation, irrigation activation, root canal, scanning electron microscope, smear layer
INTRODUCTION
The success of endodontic treatment is directly influenced by proper debridement of root canal including smear layer.[1] Smear layer acts as a barrier and prevents bacterial invasion of the dentinal tubules.[2] However, bacteria might survive and multiply in the smear layer and can also penetrate into dentinal tubules. In addition, smear layer might decrease antimicrobial effectiveness of medicaments or sealing ability of root canal filling. Therefore, it becomes mandatory to remove smear layer from root canal for optimum success of treatment.[3]
Published literature showed that regardless of instrumentation and irrigation techniques, effectiveness of irrigating solution remains limited in prepared root canals.[4,5] Therefore, improvement of irrigating protocols is essential during root canal treatment in order to achieve better cleaning efficiency in very complex area.[6]
Although Sodium Hypochlorite (NaOCl) remains gold standard as a result of its antimicrobial effect and tissue dissolution properties, it has no effect on inorganic portion of smear layer. Therefore, NaOCl has been used in association with ethylenediaminetetraacetic acid (EDTA) which acts on inorganic debris formed in instrumented root canals. These irrigants can be used with conventional syringe irrigation or with activation of different new and emerging irrigation activation devices. There are limited published scientific data to compare new and emerging devices and methods for disinfection with conventional syringe irrigation. Therefore, this study was planned to evaluate the efficacy of recently introduced irrigation activation devices EndoActivator (EA), F-File and CanalBrush (CB) on removal of smear layer in coronal, middle and apical third of instrumented root canal.
MATERIALS AND METHODS
A sample of 80 single rooted premolar teeth extracted for periodontal and orthodontic reasons were used in the study. Inclusion criteria were permanent teeth, with intact apices, no previous endodontic treatment and small restoration. Exclusion criteria were root length shorter than 17 mm, extensive restoration, root caries, cracks and fracture.
Specimens were decoronated by diamond disc to get root of 17 mm and thus working length of 16 mm. Root canals were instrumented using crown-down technique with Protaper nickel-titanium (NiTi) rotary (Dentsply — Tulsa Dental, York, PA) F2 to working length. During instrumentation, irrigation was done with 1 ml of 5.0% NaOCl. Upon completion of canal preparation, apexes were sealed with wax to prevent extrusion during final irrigation. Now irrigation was done with 5 ml NaOCl and 5 ml EDTA, with each irrigant being activated according to their assigned group such as:
Control group (n = 20): No irrigation activation
Group I (n = 20): Irrigation activation with F-File
Group II (n = 20): Irrigation activation with CB (CB; Coltene Whaledent, Langenau, Germany)
Group III (n = 20): Irrigation activation with EA (Dentsply, Tulsa, Okla).
Sample preparation
Each root were longitudinally sectioned with diamond disk and number 15 blade into mesial and distal part and dried for 24 hrs in vacuum desiccator. Only one part, i.e., either mesial or distal half was chosen for SEM analysis.
Samples were then coated with gold palladium alloy in Polaran (Bell brook business park, VCK field East Sussex, England) sputter coater for 180 s and then examined under scanning electron microscope (SEM) in ×30000 resolution. Three photomicrographs for each specimen were taken to visualize coronal, middle and apical portion. The areas examine for each sample were standardized as described by Al-Hadlaq et al[7] and Schδfer and Zapke[8] and total 240 images (80 sample × 3 portion, i.e., apical, middle and coronal) were analyzed by three blinded observers who have more than 5 years of experience of SEM study using the following scoring system:
Score 1: Clean surface with very little or no debris, presenting open dentinal tubules throughout canal wall;
Score 2: Clean surface with some scattered debris and/or thin homogenous smear layer with some open or partially occluded dentinal tubules;
Score 3: Mostly surface containing debris and smear layer with few visible open or partially occluded dentinal tubules;
Score 4: Surface with large amount of debris and smear layer with no visible dentinal tubules.
Overall assessment was also done involving coronal, middle and apical portion. When disagreement in scoring occurred, additional analysis was performed with three observers together until a consensus was reached. The data was analyzed using SPSS (Statistical Package for Social Sciences) version 15.0. Ordinal data was analyzed by non-parametric Kruskal-Wallis statistical test and Mann Whitney U-test at significance level of P ≤ 0.05.
RESULTS
Assessment of reliability of scoring by three observers was done by measuring inter-observer agreement. The level of agreement between any two observers did not exceed above fair agreement (κ < 0.4), hence the final scores were taken on basis of consensus of two observers or in case of total disagreement median value of three observations was taken as final score.
Overall as well as for all three locations mean scores were maximum in control group [Table 1a]. Minimum mean score were observed in Group II at coronal and apical locations and overall assessment. Group III had minimum score at middle third. Groups difference in score were found to be significant statistically for all three locations as well as for overall assessment (P < 0.001) [Table 1a].
Table 1a.
Mean score in different groups at different locations

Inter group comparison revealed that control group had significantly higher scores as compared to all three study groups at all locations as well as for overall assessment (P < 0.001) [Table 1b]. Between different study groups, Group I had significantly higher scores when compared with Groups II and III at coronal location (P < 0.05).
Table 1b.
Inter group comparison of scores at different locations as well as for overall assessment (Mann-Whitney U-test)

Intra group comparison showed that except for control group significant difference (P < 0.001) in scores was observed at different locations in all groups [Table 2a]. At all other locations, coronal location had minimum scores while apical location had maximum scores. Scores at coronal level were significantly lower when compared to middle and apical levels; (P < 0.001) whereas scores at middle were significantly lower as compared to those at apical levels in Group I, II and III [Table 2b].
Table 2a.
Mean scores in different groups at different locations

Table 2b.
Inter location comparison of scores in different groups as well as for overall assessment (Mann-Whitney U-test)

DISCUSSION
The removal of any vital and necrotic pulp tissue, microorganisms and their toxins, along with smear layer is essential for endodontic success. Studies have shown that currently used method of instrumentation especially rotary instrumentation technique produce a smear layer that covers root canal walls and block opening of dentinal tubules.[9,10] Therefore, this study evaluated the efficacy of irrigation activation devices F-File, CB and EA on removal of smear layer.
SEM evaluation in control group revealed presence of smear layer in entire root canal wall and very few dentinal tubules were open [Figure 1a] because mechanical flushing action created by conventional handheld syringe needle irrigation is relatively weak [Table 1a]. After conventional syringe needle irrigation, irrigating solution was delivered only 1 mm deeper than tip of needle.[11] Because needle tip is often located in coronal third of narrow canal or, at best, middle third of a wide canal,[12] penetration depth of irrigating solution are therefore limited. Furthermore, irrigating solution may not have been able to penetrate deep into apical part of root canal because of high surface tension.[13]
Figure 1.
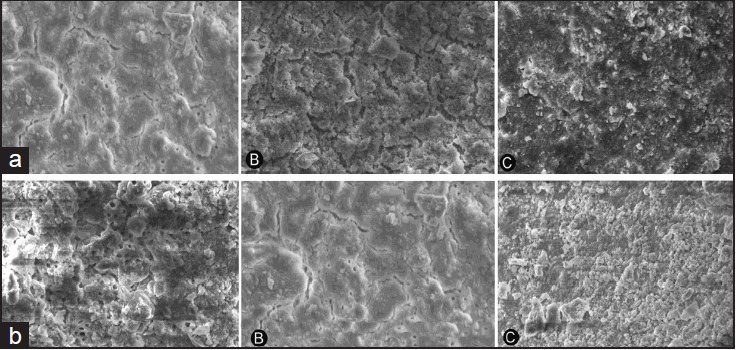
(a and b): Assessment of smear layer removal without irrigation activation (control group) and with F-File: A scanning electron microscopic study
Mean score was maximum in Group I at all three locations except control group [Table 2a; Figure 1b]. F-file is rotated at 600 rpm in order to agitate irrigant solution inside root canal to remove remaining dentine debris without further enlarging the canal.[14] The tip size (20 mm) and taper (0.04) provide a better clinical relationship to rotary NiTi file presently available than do sonic or ultrasonic instruments. These might be the reasons for this improved irrigation than in control group.
Minimum mean scores were observed in Group II at coronal, apical and overall assessment [Figure 2a]. It showed that efficiency of CB is more than F-File and EA but the difference was not statistically significant (P > 0.05) [Table 1b]. Similar study[15,16] had showed that Endobrush was significantly better than instrumentation alone in debriding root canal; however, Endobrush was shown to pack debris into apical section of canal after brushing. Our study showed that in all study group, smear layer was found in apical part (represented as high score). It is clear that cleanliness of the coronal part of tooth is more easily achieved than of middle and apical thirds.
Figure 2.
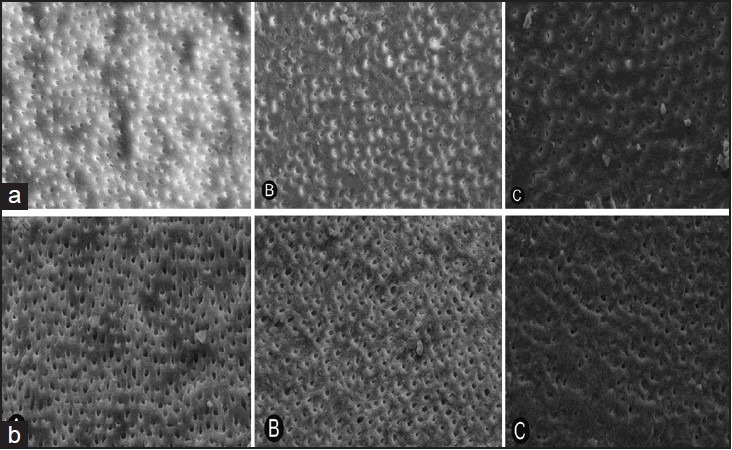
(a and b): Assessment of smear layer removal with Canal Brush and Endo Activator: A scanning electron microscopic study
Group III had minimum scores at middle third. Hence this study revealed that EA also clear more smear layer especially in middle region than CB and F-File [Figure 2b]. So removal of smear layer at different regions is as follows: Coronal > middle > apical. Other study showed that EA was reported to be able to effectively clean debris from lateral canals, remove smear layer and dislodge clumps of simulated biofilm within curved canals of molar teeth.[17] During use, action of EA tip frequently produces a cloud of debris that can be observed within a fluid-filled pulp chamber. Vibrating the tip, in combination with moving tip up and down in short vertical strokes, synergistically produces a powerful hydrodynamic phenomenon.[18]
Inter group comparisons [Table 1b] revealed that control group had significantly higher scores when compared to study groups at three regions and for overall comparison. It was evident that F-File remove more smear layer then control group, which might happened because F-File produce laminar flow[19] and created larger amount of fluid shear stress in clinical motion than in static position. This happened due to fluid was displaced by file forcing rapid fluid flow through small gap between file and canal wall. Between control group and Group II, CB remove smear layer significantly [Table 1b]. Irrigating with CB tended to produce cleaner canal walls, but was not significantly better than irrigation alone in removing the smear layer on canal walls. There were limited studies in relation to CB. Further expanded studies are required to explore role in removing smear layer from root canal.
No difference between score of F-file and EA as irrigant agitation was found. Paragliola et al[20] in their study have assessed only at 1, 3, 5 mm from tip of apex and found similar observation. Another study concluded that EA did not enhance removal of smear layer as compared with conventional Max-I-Probe irrigation with NaOCl and EDTA. A final irrigation with 1 ml of 17% EDTA solution was necessary to remove the smear layer after rotary instrumentation of root canal with or without the use of the EA system.[21]
It has been reported to cause entrapment of gas in apical third, also referred to as vapor lock, thus hindering complete removal of smear layer from this region.[22] This could explain higher debris score for all specimens in apical third. The greater taper of root canal preparation has been shown to result in a better removal of smear layer from apical third. This was attributed to greater penetration of the irrigation needle.[23] In Vapor Lock effect liquid have to penetrate closed-end channels at apical portion of root and is dependent on contact angle of liquid and depth and size of channel.[24] Under all circumstances, these closed-end microchannels will eventually be flooded after sufficient time[24](hours to days). This phenomenon of air entrapment and time frame has practical clinical implications, because endodontic irrigation is performed within a time frame of minutes instead of hours or days, air entrapment in apical portion of canal might preclude this region from contact or disinfection by irrigant.
In the classic study by Senia et al[25], Gopikrishna et al[26], Koçani et al.[27] NaOCl did not extend any closer than 3 mm from working length, even after root apex was enlarged to a size 30. This might be attributed to fact that NaOCl reacts with organic material in root canal and quickly forms micro gas bubbles at apical termination that coalesce into an apical vapor lock with subsequent instrumentation. Because apical vapor lock cannot be displaced within a clinically relevant time frame through simple mechanical actions, it prevents further irrigants from flowing into apical region. More importantly, acoustic microstreaming and cavitation can only occur in a liquid phase. Therefore, once a sonic or ultrasonically activated tip leaves the irrigant and enters the apical vapor lock, acoustic microstreaming and/or cavitation becomes physically impossible.
A simple method to disrupt vapor lock might be achieved via use of a hand-activated well-fitting root filling material[24] that is introduced to working length after instrumentation with corresponding NiTi rotary instrument. This method, although cumbersome, eliminates vapor lock because space previously occupied by air is replaced by root filling material, carrying with it a film of irrigant to working length.
Thus, in this in vitro study, all teeth were found to have debris present, especially in apical third. All techniques tested showed different degree of effectiveness in smear layer removal of root canal system. The results demand need for better irrigant protocols to completely remove debris from apical third of canal.
CONCLUSION
CB remove smear layer more efficiently from root canal than F-File and EA. CB remove smear layer better in coronal and apical region and EA in middle third region.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.De Gregorio C, Estevez R, Cisneros R, Heilborn C, Cohenca N. Effect of EDTA, sonic, and ultrasonic activation on the penetration of sodium hypochlorite into simulated lateral canals: An in vitro study. J Endod. 2009;35:891–5. doi: 10.1016/j.joen.2009.03.015. [DOI] [PubMed] [Google Scholar]
- 2.De-Deus G, Reis C, Paciornik S. Critical appraisal of published smear layer-removal studies: Methodological issues. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112:531–43. doi: 10.1016/j.tripleo.2011.01.046. [DOI] [PubMed] [Google Scholar]
- 3.Baumgartner JC, Mader CL. A scanning electron microscopic evaluation of four root canal irrigation regimens. J Endod. 1987;13:147–57. doi: 10.1016/s0099-2399(87)80132-2. [DOI] [PubMed] [Google Scholar]
- 4.Goodman A, Reader A, Beck M, Melfi R, Meyers W. An in vitro comparison of the efficacy of the step-back technique versus a step-back/ultrasonic technique in human mandibular molars. J Endod. 1985;11:249–56. doi: 10.1016/S0099-2399(85)80180-1. [DOI] [PubMed] [Google Scholar]
- 5.Gu LS, Kim JR, Ling J, Choi KK, Pashley DH, Tay FR. Review of contemporary irrigant agitation techniques and devices. J Endod. 2009;35:791–804. doi: 10.1016/j.joen.2009.03.010. [DOI] [PubMed] [Google Scholar]
- 6.Zehnder M. Root canal irrigants. J Endod. 2006;32:389–98. doi: 10.1016/j.joen.2005.09.014. [DOI] [PubMed] [Google Scholar]
- 7.Al-Hadlaq SM, Al-Turaiki SA, Al-Sulami U, Saad AY. Efficacy of a new brush-covered irrigation needle in removing root canal debris: A scanning electron microscopic study. J Endod. 2006;32:1181–4. doi: 10.1016/j.joen.2006.07.019. [DOI] [PubMed] [Google Scholar]
- 8.Schäfer E, Zapke K. A comparative scanning electron microscopic investigation of the efficacy of manual and automated instrumentation of root canals. J Endod. 2000;26:660–4. doi: 10.1097/00004770-200011000-00007. [DOI] [PubMed] [Google Scholar]
- 9.Peters OA, Barbakow F. Effects of irrigation on debris and smear layer on canal walls prepared by two rotary techniques: A scanning electron microscopic study. J Endod. 2000;26:6–10. doi: 10.1097/00004770-200001000-00002. [DOI] [PubMed] [Google Scholar]
- 10.Heard F, Walton RE. Scanning electron microscope study comparing four root canal preparation techniques in small curved canals. Int Endod J. 1997;30:323–31. doi: 10.1046/j.1365-2591.1997.00090.x. [DOI] [PubMed] [Google Scholar]
- 11.Ram Z. Effectiveness of root canal irrigation. Oral Surg Oral Med Oral Pathol. 1977;44:306–12. doi: 10.1016/0030-4220(77)90285-7. [DOI] [PubMed] [Google Scholar]
- 12.Chow TW. Mechanical effectiveness of root canal irrigation. J Endod. 1983;9:475–9. doi: 10.1016/S0099-2399(83)80162-9. [DOI] [PubMed] [Google Scholar]
- 13.Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after “one-visit” endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:231–52. doi: 10.1016/j.tripleo.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 14.Bahcall J, Olsen FK. Clinical introduction of a plastic rotary endodontic finishing file. Endod Pract. 2007;10:17–20. [Google Scholar]
- 15.Garip Y, Sazak H, Gunday M, Hatipoglu S. Evaluation of smear layer removal after use of a canal brush: An SEM study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110:e62–6. doi: 10.1016/j.tripleo.2010.02.037. [DOI] [PubMed] [Google Scholar]
- 16.Keir DM, Senia ES, Montgomery S. Effectiveness of a brush in removing postinstrumentation canal debris. J Endod. 1990;16:323–7. doi: 10.1016/S0099-2399(06)81942-4. [DOI] [PubMed] [Google Scholar]
- 17.Narayan GS, Venkatesan SM, Karumaran CS, Indira R, Ramachandran S, Srinivasan MR. A comparative evaluation on the cleaning and shaping ability of three nickel titanium rotary instruments using computerized tomography - An ex vivo study. Contemp Clin Dent. 2012;3:S151–5. doi: 10.4103/0976-237X.101070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ruddle CJ. Finishing the apical one third. Endodontic considerations. Dent Today. 2002;21:66, 70–72. [PubMed] [Google Scholar]
- 19.Koch J, Borg J, Mattson A, Olsen K, Bahcall J. An in vitro comparative study of intracanal fluid motion and wall shear stress induced by ultrasonic and polymer rotary finishing files in a simulated root canal model. ISRN Dent. 2012;2012:764041. doi: 10.5402/2012/764041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Paragliola R, Franco V, Fabiani C, Mazzoni A, Nato F, Tay FR, et al. Final rinse optimization: Influence of different agitation protocols. J Endod. 2010;36:282–5. doi: 10.1016/j.joen.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 21.Uroz-Torres D, González-Rodríguez MP, Ferrer-Luque CM. Effectiveness of the EndoActivator System in removing the smear layer after root canal instrumentation. J Endod. 2010;36:308–11. doi: 10.1016/j.joen.2009.10.029. [DOI] [PubMed] [Google Scholar]
- 22.Tay FR, Gu LS, Schoeffel GJ, Wimmer C, Susin L, Zhang K, et al. Effect of vapor lock on root canal debridement by using a side-vented needle for positive-pressure irrigant delivery. J Endod. 2010;36:745–50. doi: 10.1016/j.joen.2009.11.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Albrecht LJ, Baumgartner JC, Marshall JG. Evaluation of apical debris removal using various sizes and tapers of ProFile GT files. J Endod. 2004;30:425–8. doi: 10.1097/00004770-200406000-00012. [DOI] [PubMed] [Google Scholar]
- 24.Pesse AV, Warrier GR, Dhir VK. An experimental study of the gas entrapment process in closed-end microchannels. Int J Heat Mass Transf. 2005;48:5150–65. [Google Scholar]
- 25.Senia ES, Marshall FJ, Rosen S. The solvent action of sodium hypochlorite on pulp tissue of extracted teeth. Oral Surg Oral Med Oral Pathol. 1971;31:96–103. doi: 10.1016/0030-4220(71)90040-5. [DOI] [PubMed] [Google Scholar]
- 26.Gopikrishna V, Pare S, Pradeep Kumar A, Lakshmi Narayanan L. Irrigation protocol among endodontic faculty and post-graduate students in dental colleges of India: A survey. J Conserv Dent. 2013;16:394–8. doi: 10.4103/0972-0707.117486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Koçani F, Kamberi B, Dragusha E. Manual sonic-air and ultrasonic instrumentation of root canal and irrigation with 5.25% sodium hypochlorite and 17% ethylenediaminetetraacetic acid: A scanning electron microscope study. J Conserv Dent. 2012;15:118–22. doi: 10.4103/0972-0707.94575. [DOI] [PMC free article] [PubMed] [Google Scholar]