

Abstract
Background & objectives:
Studies conducted to assess the prevalence of cardiovascular (CV) risk factors among different regions of the country show variation in risk factors in different age groups and urban and rural population. We undertook this study to determine the prevalence of cardiovascular risk factors among urban adults in a north Indian city.
Methods:
In a cross-sectional survey, 2227 subjects aged ≥ 20 yr were studied from April 2008 to June 2009 in Urban Chandigarh, a north Indian city. Demographic history, anthropometry and blood pressure were assessed. Fasting, and 2 h capillary plasma glucose after 75 g glucose load, HDL-C and triglycerides were estimated.
Results:
The most prevalent cardiovascular risk factors in the age group of 20-29 yr was sedentary lifestyle (63%), while from fourth decade and onwards, it was overweight/obesity (59-85%). The second most common prevalent cardiovascular risk factor in the age group of 20-29 yr was overweight/obesity, in 30-49 yr sedentary lifestyle, in 50-69 yr hypertension and in subjects ≥70 yr, it was hypertriglyceridaemia. The prevalence of overweight/obesity, hypertension, dysglycaemia and smoking was almost double in subjects in the fourth decade of life, as compared to those in the third decade of life. The prevalence of CV risk factors significantly increased with age irrespective of gender and prevalence of low HDL-C was significantly more common in women as compared to men.
Interpretation & conclusions:
Sedentary lifestyle, obesity and low HDL-C are the most prevalent CV risk factors in subjects in the third and fourth decade of life in this north Indian population and clustering of these cardiovascular risk factors increases with advancing age. Strategies need to be formulated to target this population to prevent the epidemic of cardiovascular disease.
Keywords: Asian Indians, diabetes, hypertension, obesity, prevalence, sedentary lifestyle
The prevalence of cardiovascular disease (CVD) is rising worldwide and it accounts for 17 per cent of the total mortality1. This escalation in the prevalence of CVD has been attributed to the paradigm shift in life style including the changes in dietary pattern particularly more consumption of refined carbohydrates and saturated fats, and physical inertia associated with progressive economic growth and urbanization.
South Asians and Asian migrants are at unusually high risk for developing coronary artery disease (CAD)2 and diabetes3. Coronary artery disease occurs almost a decade earlier in South Asians as compared to western counterparts4. Coronary artery disease and diabetes are preceded by constellation of risk factors which include abdominal obesity, hypertension, dyslipidaemia, prediabetes and sedentary lifestyle3 as shown in various epidemiological and observational studies5,6,7. There is no dearth of data regarding the prevalence of risk factors for CVD and metabolic syndrome in various populations8,9,10,11. However, various studies show marked differences in the prevalence of various CV risk factors, among different regions in India8,10,11. Chandigarh, a north Indian city is unique as it has a high literacy rate with an urban population of 76 per cent, therefore, the prevalence data from the rest of the country cannot be extrapolated to this population. Moreover, there are limited number of studies examining the distribution of various CV risk factors among different age groups8,10,11. Hence, the objective of this study was to assess the prevalence of various cardiovascular risk factors in different age groups and to find out any gender specific differences, in urban Chandigarh.
Material & Methods
This was a cross-sectional population survey using multi-stage cluster randomized sampling conducted from April 2008 to June 2009 in Chandigarh, north India, involving 2227 subjects. Chandigarh city is divided into three zones by two main roads. Two sectors from each of the three zones were selected by simple random sampling. The first house was selected from within each selected sector by simple random sampling. Starting from that house, all the eligible people ≥20 yr of age were screened from the consecutive houses till a sample size of at least 375 was reached in that sector. Subjects having any acute illness like fever and/or on medications likely to increase plasma glucose such as glucocorticoid, and pregnant females were excluded from the study. The study protocol was approved by Institutes Ethics Committee. The procedure was explained to the participants at least a day prior to the study and informed written consent was obtained from each.
Detailed history regarding age, gender, education, occupation, any chronic illness in the participants or their family was recorded. History regarding smoking, alcohol consumption and diet was also recorded. Physical activity of the participants was recorded in a proforma adapted from Global Physical Activity - Questionnaire 2 (GPAQ-2) of World Health Organization (WHO)12, and classified as high, moderate or low physical activity. Subjects having low physical activity were labelled to have sedentary lifestyle. The socio-economic status (SES) scale as described by Kuppuswamy which takes into account the education of the head of the family, occupation of the head of the family, and monthly income of the family was followed13. Height, weight and waist circumference (WC) were measured thrice and mean was noted. Height was recorded on a stadiometer to the nearest mm. Weight was measured by a digital weighing machine to the nearest 100 g and was calibrated using standard weight every day. Waist circumference was measured with a non-stretchable tape at the midpoint between lower border of rib cage and upper border of iliac crest. High WC was defined based on criteria modified for Asian Indians (WC ≥90 cm in men and ≥80 cm in women14. BMI ≥ 23 kg/m2 was defined as overweight)14. Blood pressure was measured twice with mercury sphygmomanometer in sitting position in the right arm after 5 min of rest, to the nearest 2 mmHg and average of systolic and diastolic blood pressure was recorded. Hypertension was defined as blood pressure ≥ 140/90 mmHg. After an overnight fast of 8-14 h, capillary plasma glucose estimation was done with a glucometer using glucose-oxidase method (One Touch Ultra 2, Johnson and Johnson, Mumbai). The glucometer had in-built calibration to convert whole blood capillary glucose values to plasma glucose values. The coefficient of variation for this glucometer was 3.2 per cent. To strengthen the validity of the study external quality control was ensured by every 10th sample sent to the reference laboratory in an oxalate sodium fluoride vial, for glucose estimation using Hitachi auto analyzer 902 (Tokyo, Japan) based on the glucose oxidase-peroxidase method. The agreement between capillary plasma glucose and laboratory glucose values was calculated using Bland Altman methodology. The mean difference for fasting plasma glucose was 5.2 mg⁄ dl (0.29 mmol⁄ l) (95% CI 3.7-6.7) and for 2 h plasma glucose post-glucose load was 3.4 mg ⁄ dl (0.19 mmol⁄ l) (95% CI 2-4.8), with capillary glucose being higher than laboratory glucose values. Triglycerides and HDL-C was measured in venous blood by in vitro enzymatic colorimeter method using commercial kits (FAR Srl, Verona, Italy). The blood samples were transferred from the place of collection to the laboratory in insulated containers packed with ice bags and were processed within 4-6 h. HbA1c was estimated from venous blood on National Glycohaemoglobin Standardization Program-certified Bio-Rad D-10 system (Bio-Rad Laboratories, Hercules, CA, USA) based on ion-exchange high performance liquid chromatography. For the diagnoses of diabetes and prediabetes, the1999 WHO criteria for capillary plasma glucose15 were used. Diabetes was defined as fasting plasma glucose (FPG) ≥126 mg/dl (≥7 mmol/l) or 2 hPG ≥220 mg/dl (≥12.2 mmol/l), or both. Prediabetes was diagnosed as the presence of isolated impaired fasting glucose (IFG), defined as FPG ≥110 mg/dl (≥6.1 mmol/l) and <126 mg/dl (<7 mmol/l), and 2 hPG <160 mg/dl (< 8.8 mmol/l) or isolated impaired glucose tolerance (IGT), defined as 2 hPG≥160 mg/dl (≥8.8 mmol/l) and <220 mg/dl (<12.2 mmol/l) and FPG<110 mg/dl (<6.1 mmol/l), or both IFG and IGT (as defined above).
Statistical analysis: In the sampling design employed, the probability of selecting a sector within each of the three zones varied, and so did the probability of selecting a study subject within each selected sector. Consequently, the probability of selecting each study subject from the total population was not uniform - i.e. the design was not a ‘self-weighing’ one. The inverse of the probability of selection was, therefore, employed as a weight for that subject, and all subsequent statistical estimations were undertaken using STATA 9.0 (Texas, USA). Quantitative characteristics were summarized by arithmetic mean and standard deviation. Numerical trends in various cardiovascular risk factors across different age groups were assessed using regression analyses. Regression coefficients, standard deviations, standardized regression coefficients (beta), and P values were estimated. Multivariate logistic regression analysis was performed to determine the significance of association of different cardiovascular risk factors with age, BMI and waist circumference. All statistical tests were two-sided and performed at a significance of α=0.05.
Results
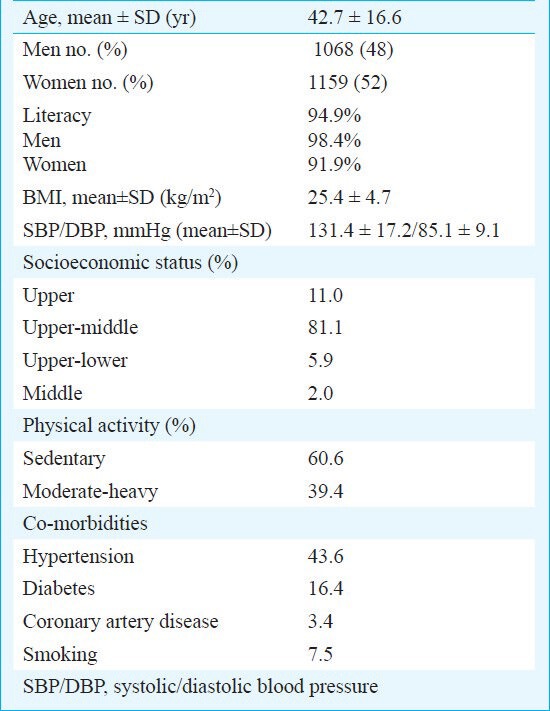
A total of 2368 subjects aged ≥20 yr, were approached based on multistage cluster randomized sampling in different sectors of urban, Chandigarh. Of them, 123 were non-responders. However, these subjects were similar to the study subjects, in terms of age, gender and body mass index (BMI). Of the remaining 2245 subjects, 18 subjects were excluded since HDL-C/TG levels were not available. Finally, 2227 subjects were evaluable in the study with a response rate of 94 per cent. The study population included 1068 men and 1159 women (1:1.08) with mean age of 42.7±16.6 yr (range 20-94 yr). The baseline demographic characteristics of the study population are shown in Table I.
Table I.
Baseline characteristics of the study population (n=2227)
The prevalence of cardiovascular (CV) risk factors among the study population in various age groups is shown in Table II. Among the parameters studied, the most prevalent CV risk factor in the age group of 20-29 yr was sedentary lifestyle (63.2%), while from fourth decade and onwards, overweight/obesity was the most common risk factor with a prevalence varying from 58.9 to 84.7 per cent. The second most common cardiovascular risk factor in the age group of 20-29 yr was overweight/obesity, in 30-49 yr sedentary lifestyle, in 50-69 yr hypertension and in subjects ≥70 yr, it was hypertriglyceridemia (Fig.).
Table II.
Prevalence of cardiovascular risk factors among the study population in various age groups
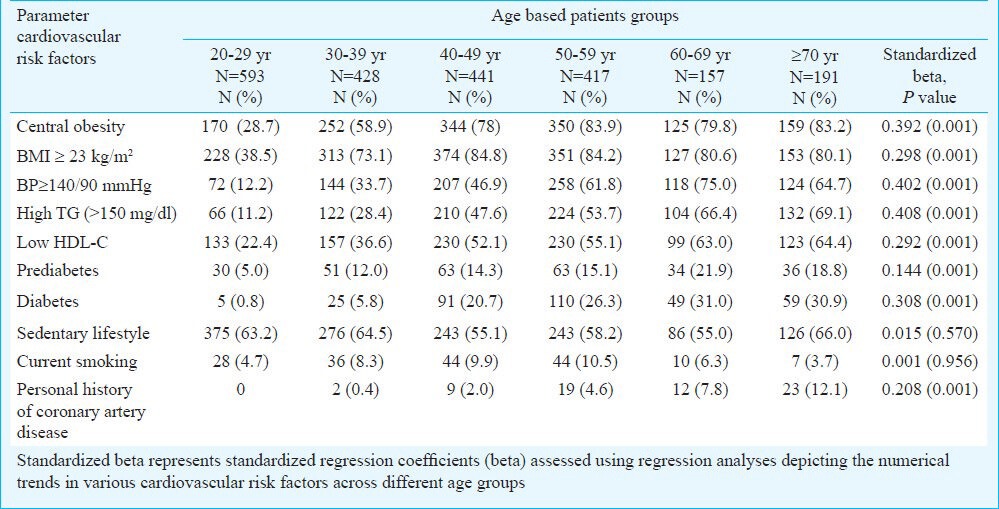
Fig.
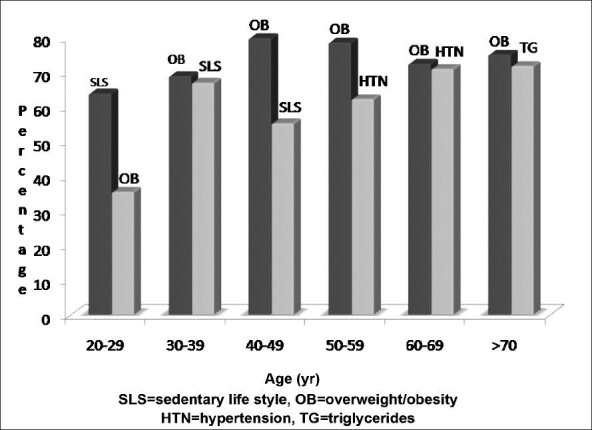
Prevalence of two most common cardiovascular risk factors in different decades of life.
On gender-wise analysis, in women in the age group of 20-39 yr, the most prevalent cardiovascular risk factor was sedentary lifestyle, however, in the age group of 30 yr and onwards overweight/obesity predominated (Table III). The second most frequent cardiovascular risk factors in women was low HDL-C in all age groups except in the third and forth decade where sedentary lifestyle and obesity/overweight were more frequent. However, in men, the trend of prevalence of the two most common cardiovascular risk factors was similar to that of the whole population (Table II). Low HDL-C were characteristically more common in women compared to men and this gender-wise differential trend was observed throughout the various age groups (Table III). Hypertension was more frequently recorded in men younger than 60 yr of age compared to women, however, this gender difference was significant only between 30 to 39 yr.
Table III.
Prevalence of cardiovascular risk factors among men and women in various age groups
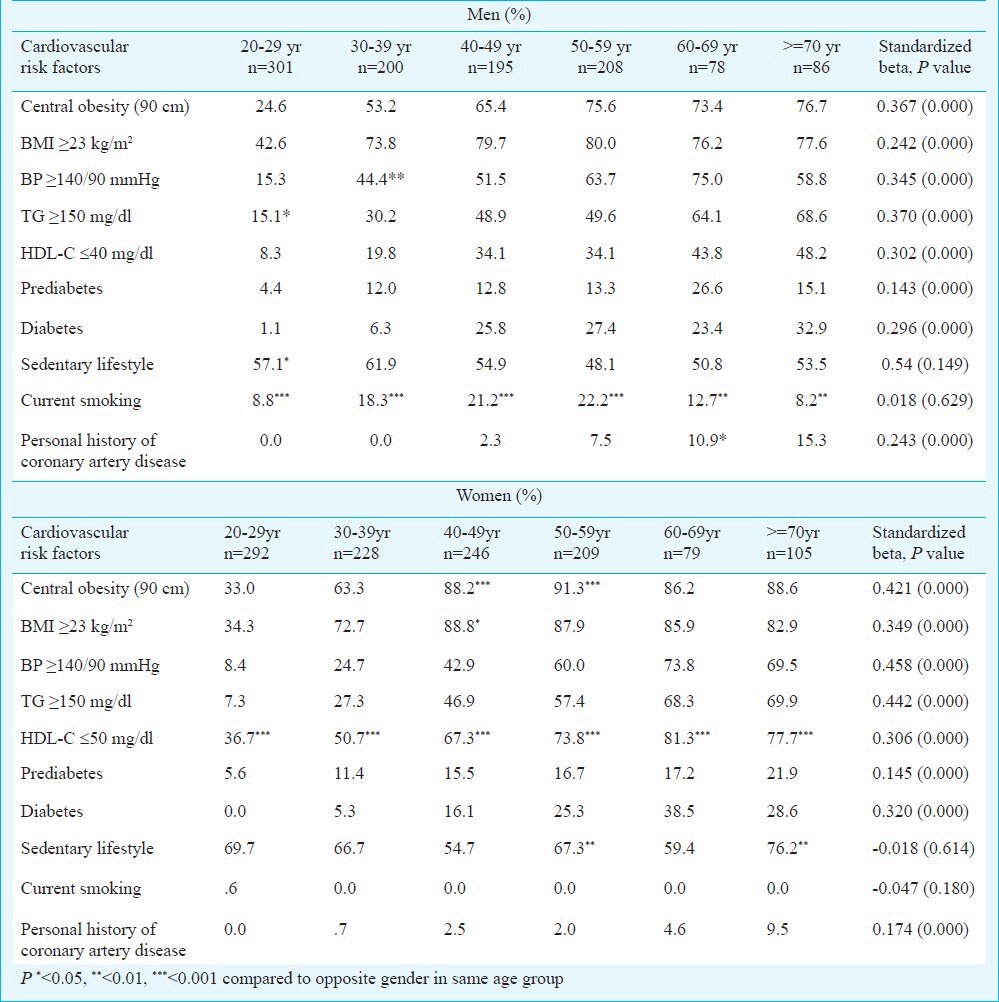
The prevalence of all the studied CV risk factors other than sedentary lifestyle and smoking significantly increased with age (P<0.001). Similar trend was observed on analyzing separately for both the genders (Table III). The prevalence of the studied CV risk factors including overweight/obesity, hypertension, dyslipidaemia, prediabetes and smoking was double in subjects in fourth decade of life, as compared to subjects in third decade of life, whereas prevalence of diabetes showed an abrupt increase by 20-folds during fifth decade (0.8 to 20.7%) followed by a progressive rise in the later part of life. Sedentary lifestyle was observed in two-third of the subjects between 20 to 39 yr and a decline in its prevalence was noted between 40 to 69 yr followed by a rise again at ≥70 yr. Smoking was significantly (P<0.001) more prevalent in men than in women. None of the subjects had personal history of coronary artery disease during 20 to 29 yr. However, 2 per cent of subjects had history of coronary artery disease (CAD) during fifth decade and its prevalence significantly increased with age (P<0.001).
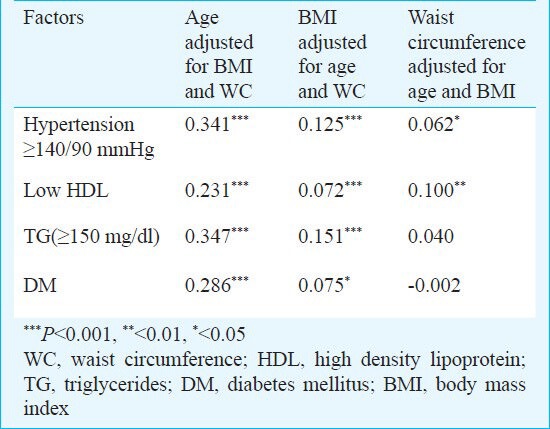
Multivariate regression analysis showed that age, BMI and central obesity were significantly and positively associated with the presence of hypertension, hypertriglyceridaemia and diabetes mellitus and low HDL-C (Table IV). Waist circumference was more strongly associated with the presence of hypertension and low HDL-C as compared to BMI. Adjustment for age subdued the association of various CV risk factors with waist circumference and BMI (Table IV).
Table IV.
Standardized regression coefficient for association of various cardiovascular risk factors with age, BMI and waist circumference
Discussion
This study showed a high prevalence of cardiovascular risk factors including sedentary lifestyle, obesity and low HDL-C in the third and fourth decade of life and the prevalence of these risk factors progressively increased with advancing age. The prevalence of central obesity, hypertension, dysglycaemia and smoking was almost double in subjects in the fourth decade of life, as compared to those in the third decade of life. Throughout all age groups, sedentary lifestyle, overweight/obesity and low HDL-C were more frequent in women as compared to men.
Various epidemiological studies have shown that physical inactivity increases the risk of CVD16,17. Overall, 61 per cent of the subjects in the present study followed sedentary lifestyle. Similar observations have been made from other parts of the country like in Kolkatta, 59 per cent of the subjects including 61 per cent men and 56 per cent women were following sedentary lifestyle18. Sedentary lifestyle was more prevalent in women as compared to men at all ages as shown by others19. This can be attributed to prevalent socio-cultural factors20,21. The present study showed that sedentary lifestyle was opted by almost 63.2 per cent of the population even in the third decade of life and this was higher compared to that observed from Rajasthan where 38.4 per cent of men and 33.6 per cent of women adopted sedentary lifestyle in the third decade of life10. This suggests that there is a need for targeting the population as early as in the third decade of life, so that the incidence of other CV risk factors can be reduced.
Overweight/obesity is an established risk factor for CVD and diabetes as shown previously22,23,24,25. Our study showed a high prevalence of overweight/obesity as compared to previous studies8,11,18 and it was the most prevalent CV risk factor during the fourth decade of life and onward. The varying prevalence of obesity in different studies partly can be attributed to different criteria used to define it8,11,18. In the present study, low HDL-C was a common prevalent CV risk factor in all age groups including the subjects in the third decade of life and was more common in women as compared to men. This observation was similar to another study conducted in north India8. The possible reasons for low HDL-C may be sedentary lifestyle, obesity and ethnicity as shown in previous studies24 and in migrant Asian Indians26,27.
As the age advanced, hypertension became one of the most prevalent CV risk factors both in men and women and the prevalence of hypertension was higher in the present study than that reported previously in other studies from India8,10. The high prevalence of sedentary lifestyle and central obesity in the study population possibly would have contributed to high prevalence of hypertension. Smoking is a well established risk factor for CVD. In the present study, prevalence of current smoking was 7.5 per cent, which was low compared to that reported earlier (32%)10.
The prevalence of almost all the studied cardiovascular risk factors progressively increased with age as has been shown earlier1,8,19. The prevalence of central obesity, hypertension, dysglycaemia and smoking was almost double in subject in the fourth decade of life as compared to the subjects in the third decade of life. Previous studies from India have also reported similar finding7. The prevalence of diabetes was 20-folds higher in subjects in fifth decade of life compared to those in fourth decade of life. This has also been shown in our previous study where the prevalence of diabetes was maximum in the fifth decade of life, which is similar to the observation in other South-east Asian countries but is a decade earlier than the western population28. Increasing age and central obesity are associated with accumulation of multiple metabolic abnormalities1,8,29,30, our study showed a strong association of increasing age, and obesity with prevalence of hypertension, diabetes, low HDL-C, and hypertriglyceridaemia.
The strengths of the study included multistage-cluster randomized study involving a large number of subjects with good response rate from a city with a high literacy rate in India. Limitations of the study included lack of history regarding diet and family history of premature cardiac events, single estimation of glucose values by glucometer and lack of estimation of serum cholesterol. Being a cross-sectional study, it did not provide an opportunity to explore the cause and effect relationship between various risk factors and cardiovascular events.
In conclusion, sedentary lifestyle, obesity and low HDL-C were found to be the most prevalent CV risk factors in subject in the third and fourth decade of life in this north Indian population. A mandate is required to target this population to prevent this epidemic of cardiovascular diseases.
Acknowledgment
Authors thank Shri Shobhit Bhansali for execution of the fieldwork, Drs Pramod Kumar Gupta, Arun Aggarwal, Ananad Srinivasan, Laxmi and Shrimati Kusum Lata for statistical analysis and Miss Bhavna Sharma for secretarial assistance.
References
- 1.Pagidipati NJ, Gaziano TA. Estimating deaths from cardiovascular disease: A review of global methodologies of mortality measurement. Circulation. 2013;127:749–56. doi: 10.1161/CIRCULATIONAHA.112.128413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.King H, Aubert RE, Herman W. Global burden of diabetes, 1995-2025: prevalence, numerical estimates, and projections. Diabetes Care. 1998;21:1414–31. doi: 10.2337/diacare.21.9.1414. [DOI] [PubMed] [Google Scholar]
- 3.Reddy KS, Yusuf S. Emerging epidemic of cardiovascular disease in developing countries. Circulation. 1998;97:596–601. doi: 10.1161/01.cir.97.6.596. [DOI] [PubMed] [Google Scholar]
- 4.Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (The INTERHEART Study): Case control study. Lancet. 2004;364:937–52. doi: 10.1016/S0140-6736(04)17018-9. [DOI] [PubMed] [Google Scholar]
- 5.Knoflach M, Kiechl S, Kind M, Said M, Sief R, Gisinger M, et al. Cardiovascular risk factors and atherosclerosis in young males: ARMY study (Atherosclerosis Risk-Factors in Male Youngsters) Circulation. 2003;108:1064–9. doi: 10.1161/01.CIR.0000085996.95532.FF. [DOI] [PubMed] [Google Scholar]
- 6.Anand SS, Yusuf S, Vuksan V, Devanesen S, Teo KK, Montague PA, et al. Difference in risk factors, atherosclerosis, and cardiovascular disease between ethnic groups in Canada: the Study of Health Assessment and Risk in Ethnic groups (SHARE) Lancet. 2000;356:279–84. doi: 10.1016/s0140-6736(00)02502-2. [DOI] [PubMed] [Google Scholar]
- 7.Ismail J, Jafar TH, Jafary FH, White F, Faruqui AM, Chaturvedi N, et al. Risk factors for non-fatal myocardial infarction in young South Asian adults. Heart. 2004;90:259–63. doi: 10.1136/hrt.2003.013631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gupta R, Misra A, Vikram NK, Kondal D, Gupta SS, Agrawal A, et al. Younger age of escalation of cardiovascular risk factors in Asian Indian subjects. BMC Cardiovas Disord. 2009;9:28. doi: 10.1186/1471-2261-9-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Joshi P, Islam S, Pais P, Reddy S, Dorairaj P, Kazmi K, et al. Method of establishing risk factors for early myocardial infarction in South Asians compared with individuals in other countries. JAMA. 2007;297:286–94. doi: 10.1001/jama.297.3.286. [DOI] [PubMed] [Google Scholar]
- 10.Haldiya KR, Mathur ML, Sachdev R. Lifestyle-related risk factors for cardiovascular disease in a desert population of India. Curr Sci. 2010;99:190–5. [Google Scholar]
- 11.Reddy KS, Prabhakaran D, Chaturvedi V, Jeemon P, Thankappan KR, Ramakrishnan L, et al. Methods for establishing a surveillance system for cardiovascular diseases in Indian industrial populations. Bull World Health Organ. 2006;84:461–9. doi: 10.2471/blt.05.027037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Geneva, Switzerland: population based prevention, World Health Organization; 2007. [updated 2007 May; cited 2007 November, accessed on March 6, 2008]. Global Physical Activity Questionnaire: Department of chronic diseases and Health promotion surveillance World Health Organization, Geneva. www.who.int/chp/steps. Available from: http://www.int/chp/steps/resources/GPAQ_Analysis_Guide.pdf . [Google Scholar]
- 13.Kumar N, Shekhar C, Kumar P, Kundu AS. Kuppuswamy's socioeconomic status scale-updating for 2007. Indian J Pediatr. 2007;74:1131–2. [PubMed] [Google Scholar]
- 14.Misra A, Chowbey P, Makkar BM, Vikram NK, Wasir JS, Chadha D, et al. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. J Assoc Physicians India. 2009;57:163–70. [PubMed] [Google Scholar]
- 15.Technical report of WHO 1999 part 1: definition, diagnosis, and classification of diabetes and its complications. [accessed on March 6, 2008]. Available from: whqlibdoc.who.int/hq/1999/WHO_NCD_NCS_99.2.pdf .
- 16.Warren TY, Barry V, Hooker SP, Sui X, Church TS, Blair SN. Sedentary behaviors increase risk of cardiovascular disease mortality in men. Med Sci Sports Exerc. 2010;42:879–85. doi: 10.1249/MSS.0b013e3181c3aa7e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Aadahl M, Kjaer M, Jorgensen T. Associations between overall physical activity level and cardiovascular risk factors in an adult population. Eur J Epidemiol. 2007;22:369–78. doi: 10.1007/s10654-006-9100-3. [DOI] [PubMed] [Google Scholar]
- 18.Das M, Pal S, Ghosh A. Prevalence of cardiovascular disease risk factors by habitat: a study on adult Asian Indians in West Bengal, India. Anthropol Anz. 2011;68:253–64. doi: 10.1127/0003-5548/2011/0099. [DOI] [PubMed] [Google Scholar]
- 19.Ghosh A, Bhagat M, Das M, Bala SK, Goswami R, Pal S. Prevalence of cardiovascular disease risk factors in people of Asian Indian origin: Age and sex variation. J Cardiovasc Dis Res. 2010;1:81–5. doi: 10.4103/0975-3583.64441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Marmot M. Multilevel approaches to understanding social determinants. In: Berkman LF, Kawachi I, editors. Social epidemiology. Oxford: Oxford University Press; 2000. pp. 349–67. [Google Scholar]
- 21.Ramanathan S, Crocker PR. The influence of family and culture on physical activity among female adolescents from Indian diaspora. Qual Health Res. 2009;19:492–503. doi: 10.1177/1049732309332651. [DOI] [PubMed] [Google Scholar]
- 22.Misra A, Vikram NK. Insulin resistance syndrome (metabolic syndrome) and obesity in Asian Indians: evidence and implications. Nutrition. 2004;20:482–91. doi: 10.1016/j.nut.2004.01.020. [DOI] [PubMed] [Google Scholar]
- 23.Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation. 1983;67:968–77. doi: 10.1161/01.cir.67.5.968. [DOI] [PubMed] [Google Scholar]
- 24.Jousilahti P, Tuomilehto J, Vartiainen E, Pekkanen J, Puska P. Body weight, cardiovascular risk factors, and coronary mortality. 15-year follow-up of middle-aged men and women in eastern Finland. Circulation. 1996;93:1372–9. doi: 10.1161/01.cir.93.7.1372. [DOI] [PubMed] [Google Scholar]
- 25.Yarnell JW, Patterson CC, Thomas HF, Sweetnam PM. Comparison of weight in middle age, eight at 18 years, and weight change between, in predicting subsequent 14 year mortality and coronary events: Caerphilly Prospective Study. J Epidemiol Community Health. 2000;54:344–8. doi: 10.1136/jech.54.5.344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chandalia M, Mohan V, Adams-Huet B, Deepa R, Abate N. Ethnic difference in sex gap in high-density lipoprotein cholesterol between Asian Indians and Whites. J Investig Med. 2008;56:574–80. doi: 10.2310/JIM.0b013e31816716fd. [DOI] [PubMed] [Google Scholar]
- 27.Halodkar NC, Blum S, Rana T, Bhalodkar A, Kitchappa R, Kim KS, et al. Comparison of levels of large and small high-density lipoprotein cholesterol in Asian Indian men compared with Caucasian men in the Framingham Offspring Study. Am J Cardiol. 2004;94:1561–3. doi: 10.1016/j.amjcard.2004.08.040. [DOI] [PubMed] [Google Scholar]
- 28.Ravikumar P, Bhansali A, Ravikiran M, Bhansali S, Walia R, Shanmugasundar G, et al. Prevalence and risk factors of diabetes in a community-based study in North India: the Chandigarh Urban Diabetes Study (CUDS) Diabetes Metab. 2011;37:216–21. doi: 10.1016/j.diabet.2010.10.004. [DOI] [PubMed] [Google Scholar]
- 29.Snehalatha C, Ramachandran A, Satyavani K, Vallabi MY, Viswanathan V. Computed axial tomographic scan measurement of abdominal fat distribution and its correlation with anthropometry and insulin secretion in healthy Asian Indians. Metabolism. 1997;46:1220–4. doi: 10.1016/s0026-0495(97)90221-3. [DOI] [PubMed] [Google Scholar]
- 30.Vague J. The degree of masculine differentiation of obesities: a factor determining predisposition to diabetes, atherosclerosis, gout, and uric calculous disease. Am J Clin Nutr. 1956;4:20–34. doi: 10.1093/ajcn/4.1.20. [DOI] [PubMed] [Google Scholar]