

Abstract
Objective:
Androgen deprivation therapy (ADT) is a common treatment for prostate cancer with numerous side effects. We assess primary care physicians’ (PCPs) knowledge of ADT side effects and their interest in increasing their knowledge in this area.
Methods:
A list of active Canadian PCPs was obtained using the Canadian Medical Directory. A cross-sectional survey was distributed to 600 randomly selected physicians. We collected PCPs’ demographic information, experience with ADT management, knowledge regarding ADT side effects and desired sources for obtaining knowledge on ADT management.
Results:
In total, we received 103 completed questionnaires. Of these, 89% of PCPs had patients on ADT. One-third of respondents prescribed ADT and over half of them administered ADT annually. Thirty-eight percent felt their knowledge of ADT side effects was inadequate and 50% felt uncomfortable counselling patients on ADT. Many PCPs were less familiar with the incidence of functional side effects of ADT (i.e., hot flashes, fatigue and erectile dysfunction) compared to life-threatening side effects (i.e., cardiovascular events, metabolic syndrome, fractures). In terms of increasing their knowledge of ADT side effects, 82% of PCPs would use educational resources if they were available (52% and 32% preferred continued medical education [CME] events and educational pamphlets, respectively).
Conclusions:
PCPs play an important role in managing ADT side effects. There is poor awareness of the prevalence of ADT side effects, and many are uncomfortable in managing these side effects. These areas may be addressed through CME programs and educational pamphlets.
Introduction
In Canada 26 500 men are diagnosed with prostate cancer annually.1 Primary care physicians (PCPs) play a pivotal role in population screening and continue to play a significant role in routine and cancer-specific patient care after diagnosis.2,3 Androgen deprivation therapy (ADT) is a mainstay treatment. About 50% of prostate cancer patients will use ADT at some point during their therapeutic journey.
ADT targets the hypothalamus-pituitary-gonadal axis, which controls several metabolic and hormonal pathways. Alterations in these pathways can lead to many treatment side effects. Significant adverse outcomes, such as increased diabetes, deep vein thrombosis and osteoporosis, can have a major impact on a patient’s quality of life. Fortunately these side effects are relatively rare. However, in select populations with predisposing risk factors these side effects can be a major issue.4–8 Other side effects, such as weight gain, hot flashes, fatigue, erectile dysfunction, and gynecomastia, are commonly reported by patients.5,9
Given the prevalence of prostate cancer and ADT use, it would be expected that PCPs would have many of their patients on ADT. There is little information on PCPs’ experience with monitoring and managing ADT side effects. The objective of this pilot study was to assess and describe the current knowledge of PCPs across Canada regarding ADT side effect management. A secondary objective was to identify potentially helpful educational strategies surrounding ADT side effect management for PCPs.
Methods
This study was approved by the Research Ethics Board (Study #26393). In May 2011, a list of 27 015 active practicing PCPs in Canada was collected from the Canadian Medical Directory (MD Select, Toronto, ON). This list was divided into 3 geographic regional cohorts: Eastern (Quebec, New Brunswick, Nova Scotia, Prince Edward Island, Newfoundland and Labrador), Central (Ontario) and Western (British Columbia, Alberta, Saskatchewan, Manitoba). We selected 200 physicians from each region using a random number generator. Each selected physician was checked against online information from the available provincial colleges to ensure that he/she was practicing primary care and not subspecialty medicine. We excluded 17 physicians who retrained into different specialties. A final list of 200 physicians per group (n = 600 total) was selected.
Survey
The study questionnaire was designed through expert opinion (i.e., an internist, a PCP, a radiation oncologist, and a urologist) as no previously validated instruments existed for the purposes of our study (Appendix 1). In the questionnaire ADT included agents: gonadotropin-releasing hormone antagonists (GnRH) agonists (e.g., leuprolide, goserelin), GnRH antagonists (e.g., abarelix), oral androgen ablation agents (e.g., ketoconazole), oral non-steroidal antiandrogens/androgen receptor antagonists (e.g. flutamide, bicalutamide) and 5α-reductase inhibitors (e.g., finasteride, dutasteride). Demographic data were collected on gender, age, number of years in practice, type and size of practice, as well as the number of patients actively on ADT. These questions employed binary or Likert scales where appropriate (e.g., information on age was collected on the questionnaire using a Likert scale of <30, 30–40, 40–50, 50–60 and >60).
Knowledge was assessed regarding the estimated incidence of 7 ADT side effects (diabetes, deep vein thrombosis, cardiovascular events, erectile dysfunction, hot flashes, depression and reduced cognition) after 1 year of use. These outcome measures were chosen based on feedback from the focus group of expert clinicians, as some represent the most medically serious side effects, whereas others were chosen based on the results of a previous survey study that had examined common ADT side effects reported by patients.9 Based on a list of 15 ADT side effects, PCPs were asked to rank the 3 most significant ADT side effects and the 3 most commonly reported ADT side effects by their patients.10
Using a Likert scale, participants rated their knowledge and comfort level in counselling patients regarding ADT side effects; they also indicated the frequency of these patient discussions. They were asked about their expectation for who should monitor ADT side effects (participants were given the choice of “specialist, PCP, both, or other.”). Using a Likert scale, PCPs also rated the perceived utility of an educational resource on ADT side effects, as well as their preferred form of education (e.g., continuing medication education [CME] programs, pamphlets, consultant letters, validated internet sources, conferences). We conducted a pilot test of the survey with external prostate cancer experts and PCPs to ensure face validity, appropriateness, and clarity.
The survey was mailed to 600 physicians. After 6 months, a second survey was mailed to non-responders. All recruited physicians provided informed consent.
Results
In total 134 surveys were returned after the second mail-out. In the final analysis we used responses from 103 PCPs (31 respondents were excluded because they no longer practiced primary care). This represented a total response rate of 18%. Regional response rates were equally distributed across Eastern, Central and Western Canada and there was no substantial variation in the responses we received from these different regions. Therefore, given the relatively small number of responses, the cohorts were compiled into a single group.
Description of study population
Most respondents were male (67%), over 40 years old (80%) and had more than 11 years in practice (80%) (Table 1). Furthermore, most of them worked in group practices (61%), in communities with over 100 000 people (56%) and had practices with 1001 to 2000 patients (38%). There was no significant demographic variability among respondents across the 3 regions (data not shown).
Table 1.
Description of PCP respondents (n=103)
| Total (%) | |
|---|---|
| Gender | |
| Male | 65 (63%) |
| Female | 38 (37%) |
| Age group (years) | |
| <40 | 21 (20%) |
| 41–60 | 55 (53%) |
| >60 | 27 (26%) |
| Years in practice | |
| <10 | 21 (20%) |
| 11–20 | 23 (22%) |
| 21–30 | 32 (31%) |
| >30 | 27 (26%) |
| Type of practice | |
| Group | 63 (61%) |
| Single | 28 (27%) |
| Teaching/university | 11 (11%) |
| Other | 1 (1 %) |
| Size of community | |
| <99,999 | 45 (44%) |
| 100,000–1,000,000 | 35 (34%) |
| >1,000,000 | 23 (22%) |
| Size of practice | |
| 1–1,000 | 30 (29%) |
| 1,001–2,000 | 39 (38%) |
| >2,000 | 29 (28%) |
| Missing | 5 (5%) |
| Patients currently on ADT | |
| 0 | 11 (11%) |
| 1–10 | 74 (72%) |
| 11–20 | 13 (13%) |
| >20 | 5 (5%) |
PCP: primary care physicians; ADT: androgen deprivation therapy.
Of the respondents, 89% currently had patients on ADT. Thirty-five percent of PCPs reported having written prescriptions for ADT and 53% reported having administered ADT in their office over a 1-year period (Table 1).
PCPs’ knowledge of ADT side effects
Many PCPs estimated that the likelihood of cardiovascular events, diabetes, depression and reduced cognition was less than 10% (Table 2). With regards to erectile dysfunction and hot flashes, there was a greater heterogeneity of PCP responses; 41% to 60% of respondents estimated that erectile dysfunction and hot flashes were more prevalent after 1 year on ADT (Table 2).
Table 2.
PCPs’ estimates of side-effect prevalence after 1 year on ADT (n=103)
| Side effect | ≤10% | 11%–20% | 21%–40% | 41%–60% | 61%–80% | 81%–100% | Unanswered |
|---|---|---|---|---|---|---|---|
| Diabetes | 58 | 25 | 9 | 0 | 0 | 0 | 11 |
| Deep vein thrombosis | 73 | 18 | 0 | 0 | 0 | 0 | 12 |
| Cardiovascular events (i.e., MI, stroke) | 58 | 24 | 3 | 2 | 0 | 0 | 16 |
| Erectile dysfunction | 8 | 12 | 21 | 25 | 17 | 9 | 11 |
| Hot flashes | 13 | 18 | 17 | 19 | 16 | 7 | 13 |
| Depressed mood | 23 | 24 | 27 | 12 | 6 | 0 | 11 |
| Reduced cognition | 46 | 28 | 12 | 4 | 1 | 0 | 12 |
PCP: primary care physicians; ADT: androgen deprivation therapy; MI: myocardial infarction.
In comparison to actual prevalence statistics, most PCPs had an appropriate estimate of the prevalence for deep vein thrombosis, cardiovascular events and depression (Table 3). For other side effects, such as diabetes, erectile dysfunction and hot flashes, most respondents underestimated the actual prevalence. Actual prevalence for each side effect was verified by a literature search.11–15
Table 3.
Actual vs. perceived incidence of side effects in prostate cancer patients receiving ADT for at least 1 year
| Disease | Actual incidence | Perceived incidence |
|---|---|---|
| Diabetes | 15.9% on GnRH agonist therapy vs. 8.8% not on GnRH agonist therapy11 | Most (58/103) perceived incidence to be <10% |
| Deep vein thrombosis | 7.0% on ADT vs. 4.0% not on ADT12 | Most (73/103) perceived incidence to be <10% |
| Cardiovascular events (MI) | 1.3% on GnRH agonist therapy vs. 0.7% not on GnRH agonist therapy11 | Most (58/103) perceived incidence to be <10% |
| Cardiovascular events (stroke) | 1.9% on GnRH agonist therapy vs. 1.1% not on GnRH agonist therapy11 | |
| Erectile dysfunction | 80% on ADT vs. 30% not on ADT13 | Highest proportion (25/103) perceived incidence to be 41–60% |
| Hot flashes | 84% on Leuprolide vs. 29% not on leuprolide14 | Highest proportion (19/103) perceived incidence to be 41–60% |
| Depressed mood | 22% on Leuprolide vs. 3% not on leuprolide14 | Highest proportion (27/103) perceived incidence to be 21–40% |
| Reduced cognition | No consistent evidence that ADT use has an adverse effect on cognitive function15 | Most (46/103) perceived incidence to be <10% |
ADT: androgen deprivation therapy; MI: myocardial infarction; GnRH: gonadotropin-releasing hormone.
Significant side effects as reported by PCPs and patients
We illustrate the most common ADT side effects (Fig. 1). PCPs were asked to rate the 3 most side effects reported by their patients, as well as the top 3 which they thought were most concerning (Fig. 2). The most frequently reported side effects included fatigue (50%), hot flashes (43%), erectile dysfunction (35%), gynecomastia (33%), and depression (19%). The most concerning ADT side effects included cardiovascular events (60%), metabolic syndrome/diabetes (56%), depression (41%), loss of bone mineral density/osteoporosis (35%), and erectile dysfunction (23%).
Fig. 1.

Side effects of androgen deprivation therapy.
Fig. 2.
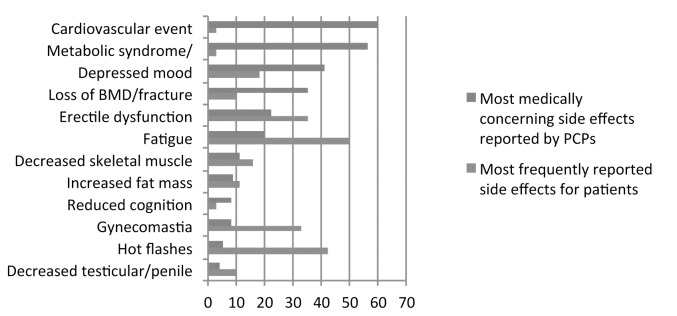
Androgen deprivation therapy side effects profile in primary care practitioners’ practice (most frequently reported vs. most medically concerning).
Knowledge perception and information needs
Thirty-eight percent of PCPs regarded their ADT knowledge to be below average and 50% rated themselves as uncomfortable counselling patients regarding ADT side effects. Forty percent of PCPs were interested in playing a role in monitoring ADT side effects (solo or with a specialist colleague), whereas 59% expected this role to be filled by the specialist (Table 4).
Table 4.
Knowledge perception and information needs (n=103)
| Total (%) | |
|---|---|
| Perceived knowledge regarding ADT side effects | |
| Below average | 39 (38%) |
| Average | 61 (59%) |
| Above average | 2 (2%) |
| Expert | 1 (1%) |
| Comfort level in counselling patients regarding ADT side effects | |
| Not very | 52 (50%) |
| Somewhat | 41 (40%) |
| Very | 10 (10%) |
| Frequency of discussing ADT side effects with patients | |
| Rarely | 47 (46%) |
| Sometimes | 31 (30%) |
| Most of the time | 20 (19%) |
| Always | 3 (3%) |
| Unanswered | 2 (2%) |
| Expectation as to who should monitor ADT side effects | |
| Specialist | 61 (59%) |
| PCP | 28 (27%) |
| Both (Specialist + PCP) | 13 (13%) |
| Other (Pharmacist) | 1 (1%) |
| If a resource on ADT side effects were available, how frequently would it be used | |
| Rarely | 14 (14%) |
| Sometimes | 63 (61%) |
| Often | 22 (21%) |
| Unsure/unanswered | 4 (4%) |
ICU: intensive care unit. Adapted from Hasson HM. Am J Obstet Gynaecol 1971.7
Most PCPs (82%) would use educational material on ADT side effects if it were readily available. Preferred forms of education included CME programs (53%), education pamphlets (33%), and specialist letter or consultation (20%) (Fig. 3).
Fig. 3.

Educational modalities chosen to be most useful by primary care physicians.
Discussion
We surveyed 103 PCPs across Canada to examine their current knowledge and information needs regarding ADT side effect management. We found the following 4 results. First, we confirm the high prevalence of PCPs who care for patients on ADT. Second, we suggest that PCPs are aware of the low incidence of life-threatening side effects (diabetes, deep vein thrombosis and cardiovascular events); however, there is a concern that PCPs are likely to place less emphasis on more common, functional side effects (erectile dysfunction, hot flashes and depression). Third, we also suggest that few PCPs feel comfortable managing ADT side effects, even the common ones. Finally, we recommend that targeted educational interventions should be considered.
There is some concern that PCPs are less familiar with the incidence of the more common side effects of ADT (erectile dysfunction, hot flashes and depression). The literature suggests that most patients suffer from erectile dysfunction,16 but only 9% of the PCPs correctly identified the incidence of erectile dysfunction as greater than 81%. Furthermore, hot flashes are known to occur in 80% of patients on ADT;17 however, we found that only 22% of the PCPs correctly identified the incidence of hot flashes as greater than 61%.
More importantly, our respondents reported that functional side effects of ADT are the more frequently cited by patients (Fig. 2). However, this is not in keeping with what PCPs believe to be medically significant side effects. This is notable, as our previous work demonstrated that patients generally tolerated ADT well, but had unexpected difficulties coping with functional side effects, such as hot flashes and fatigue.9 This is further supported by a recent study from the Netherlands that showed that men with prostate cancer presented to their PCPs with adverse drug effects almost twice as often as controls.18 These patients presented with fatigue almost 3 times more often than the control groups; the fatigue was likely secondary to the treatment. This side effect incidence should be recognized and addressed by PCPs.
Furthermore, patient education regarding ADT side effects is important. While our study demonstrated that PCPs are aware of the low incidence of life-threatening side effects (i.e., diabetes, deep vein thrombosis and cardiovascular events), patients have a poor understanding of these outcomes.9 Walker and colleagues found that patients who were not informed about ADT-associated side effects by their physicians did not engage in behaviours to prevent or reduce the risk of adverse effects.19 Moreover, Lebret and colleagues recently demonstrated that 57% of the men on ADT who received an educational toolkit started implementing changes in their overall lifestyle.20 Patients should be actively involved in the primary prevention of ADT’s life-threatening side effects through greater education and lifestyle modifications.
Our study revealed that 38% of PCPs regarded their ADT knowledge as below average and 50% felt uncomfortable counselling patients regarding ADT side effects (Table 4). Furthermore, only 21% of PCPs discussed ADT side effects most of the time or always, and 59% of PCPs expected their specialist colleague to monitor ADT side effects. However, one study from the United Kingdom found that prostate cancer patients visited their PCPs up to 3 times more often compared to controls, with consultation rates staying elevated 15 years post-diagnosis compared to controls.21 A contributing factor is the administration of ADT, as well as a trend towards earlier discharge from the specialist to the primary care physician.Therefore, this underscores the importance of PCPs having a better understanding of prostate cancer treatments and its side effects. Fortunately, as this and other studies have reported, PCPs expressed a willingness and interest in managing patients with prostate cancer throughout their disease.3,22,23 Eighty-two percent of PCPs reported that they would use educational material on ADT side effects if it were readily available. Their preferred methods included CME events (52%) and educational pamphlets (32%). The literature supports the notion that instructor-directed medical education programs and self-directed learning facilitated through appropriate resources are the most popular among physicians; this is especially true when there is a self-identified knowledge or skill gap.24,25
Our study has its limitations. We had a small sample size (n = 103) with a response rate of 18%. Other limitations include a cross-sectional study design, a non-validated questionnaire, a presumably decreased response rate from physicians who were non-English speakers and a broad definition of ADT which does not differentiate between side effects for each of the various drugs. These limitations curb the study’s generalizability. Furthermore, our study did not include an in-depth qualitative assessment of the information needs of PCPs regarding ADT. Based on the results of our pilot study, we suggest that future studies focus on understanding the qualitative aspect of information needs of PCPs regarding ADT, as well as the efficacy of various forms of CME in educating PCPs. We also suggest an assessment of the attitudes of Canadian urologists/radiation oncologists in collaborating with PCPs in managing ADT side effects.
Conclusion
The population of prostate cancer survivors is growing and PCPs have a unique opportunity and a valuable role in monitoring and managing patients on ADT. Our study demonstrated that PCPs have poor awareness of the functional side effects of ADT, and few are comfortable in managing ADT side effects. In the future, we suggest that educational materials, such as CME programs and pamphlets, be trialed to address these deficits.
Appendix 1.
Assessment of Family Physicians’ knowledge regarding hormone therapy associated side effects
|
Study ID #:________________ Date of Completion (mo/day/yr):____/____/____
|
1. In your medical practice do you provide routine primary care to adults?
|
| In this survey, the ‘hormone therapy’ refer to Androgen Deprivation Therapy, used to treat men with prostate cancer. |
| These agents include GnRH Agonists (e.g. Leuprolide or Lupron, Goserelin or Zoladex), GnRH Antagonist (e.g. Abarelix or Plenaxis), Androgen Ablating Drugs (e.g. Ketoconazole or Nizoral), Androgen Receptor Antagonist (e.g. Flutamide or Euflex, Bicalutamide or Casodex.) and 5α-Reductase inhibitors (e.g. Finasteride or Proscar, Dutasteride or Avodart). |
| Baseline assessment | ||||
| 2. How many of your patients are currently or previously on hormone therapy for treatment of prostate cancer? | ||||
| □ 1–25 | □ 26–50 | □ 51–100 | □ 101–300 | □ >300 |
|
| ||||
| 3. How often do you prescribe hormone therapy yourself? | ||||
| □ 1–25 | □ 26–50 | □ 51–100 | □ 101–300 | □ >300 |
|
| ||||
| 4. How often does your office (yourself or a registered nurse) administer hormone therapy? | ||||
| □ 1–25 | □ 26–50 | □ 51–100 | □ 101–300 | □ >300 |
|
| ||||
| 5. How often do you discuss the possible side effects with your patients on hormone therapy? | ||||
| □ Rarely | □ Sometimes | □ Most of the time | □ Always | |
| 6. What are the top three most frequently reported side effects of hormone therapy by patients that you encounter in your practice? (please check only 3) | |
| □ Increased fat mass | □ Cardiovascular events (i.e., MI, stroke) |
| □ Metabolic syndrome/diabetes | □ Hot flashes |
| □ Loss of bone mineral density | □ Erectile dysfunction |
| □ Fracture | □ Gynaecomastia |
| □ Fatigue | □ Decrease in testicular and penile size |
| □ Decrease in skeletal muscle | □ Loss of body hair |
| □ Reduced cognition | □ Depressed mood |
| □ Other (please specify) | |
|
| |
| 7. In your opinion, what do you think are the three most medically harmful side effects for men on hormone therapy? (please check only 3) | |
| □ Increased fat mass | □ Cardiovascular events (i.e., MI, stroke |
| □ Metabolic syndrome/diabetes | □ Hot flashes |
| □ Loss of bone mineral density | □ Erectile dysfunction |
| □ Fracture | □ Gynaecomastia |
| □ Fatigue | □ Decrease in testicular and penile size |
| □ Decrease in skeletal muscle | □ Loss of body hair |
| □ Reduced cognition | □ Depressed mood |
| □ Other (please specify) | |
| 8. What do you think is the prevalence of these side effects in men on hormone therapy ≥1 year? | ||||||
| Side effect | <10% | 11–20% | 21–40% | 41–60% | 61–80% | 81–100% |
| Diabetes | ||||||
| Deep vein thrombosis | ||||||
| Cardiovascular events (ie. MI, stroke) | ||||||
| Erectile dysfunction | ||||||
| Hot flashes | ||||||
| Depressed mood | ||||||
| Reduced cognition | ||||||
| Individual practice assessment | |||
|
| |||
| 9. How do you perceive your knowledge of hormone therapy side effects compared to other family physicians? | |||
| □ Below average | □ Average | □ Above average | □ Expert |
| 10. Where or from whom do you obtain your knowledge from regarding hormone therapy side effects? | ||
| □ Specialist colleague | □ Conferences | □ Self-directed research |
| □ Family physician colleague | □ CME events | |
| □ Other (please specify) _________________________________________________________________ | ||
| 11. How comfortable do you feel counseling your patients regarding hormone therapy side effects? | ||
| □ Not very | □ Somewhat | □ Very |
|
| ||
| 12. What is your expectation regarding who should monitor for hormone therapy side effects in your patients? | ||
|
| ||
| □ Specialist | □ Family physician | □ Other (please specify) |
| 13. If a resource regarding hormone therapy side effects was available would you use it? | ||
| □ Yes | □ No | □ Unsure |
| 14. What avenue of information on hormone therapy would you find most useful? | |||
| □ Periodicals | □ Pamphlets | □ CME events | □ Conference |
| □ Specialist consult | □ Other (please specify) | ||
| Demographics | ||||
|
| ||||
| 15. What is your sex? | ||||
| □ Male | □ Female | |||
|
| ||||
| 16. How old are you? | ||||
| □ <30 | □ 30–40 | □ 40–50 | □ 50–60 | □ >60 |
|
| ||||
| 17. How many years have you been practicing? | ||||
| □ 1–5 | □ 6–10 | □ 11–15 | □ 16–20 | □ >20 |
|
| ||||
| 18. What type of practice are you part of (check all that apply)? | ||||
| □ Group | □ Single | □ Teaching or university affiliated | ||
| □ Other (specify) ______________ | ||||
|
| ||||
| 19. What is the city size/catchment area you serve? | ||||
| □ <10,000 | □ 10,000–99,999 | □ 100,000–499,999 | □ 500,000–1,000,000 | |
| □ >1,000,000 | ||||
|
| ||||
| 20. What is the size of your practice? | ||||
| □ 1–500 | □ 501–1000 | □ 1001–2000 | □ 2001 – 3000 | □ >3000 |
Thank you for completing this questionnaire
Footnotes
Competing interests: Dr. Soeyonggo, Dr. Locke, Dr. Del Giudice and Dr. Warde all declare no competing financial or personal interests. Dr. Alibhai has received a grant from Sanofi to study the treatment of ADT-related fatigue. Dr. Fleshner is a member of the Advisory Board for Amgen, Janssen, Astellas and Eli Lily. He has received honoraria from Amgen, Janssen, Astellas and Eli Lily. He is and has participated in clinical trials for Amgen, Janssen, Medivation, OICR, and Prostate Cancer Canada.
This paper has been peer-reviewed.
References
- 1.Statistics Canada. 2011 Http://www.cancer.ca. Accessed March 20, 2014. [Google Scholar]
- 2.Allard CB, Dason S, Lusis J, et al. Prostate cancer screening: Attitudes and practices of family physicians in ontario. Can Urol Assoc J. 2012;6:188–93. doi: 10.5489/cuaj.11290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Cohen Castel O, Ungar L, Alperin M, et al. Family physicians’ perceptions, beliefs, and attitudes regarding information sharing with prostate cancer patients throughout the course of the disease. Support Care Cancer. 2008;16:955–61. doi: 10.1007/s00520-007-0358-0. [DOI] [PubMed] [Google Scholar]
- 4.Kim HS, Moreira DM, Smith MR, et al. A natural history of weight change in men with prostate cancer on androgen-deprivation therapy (ADT): Results from the shared equal access regional cancer hospital (SEARCH) database. BJU Int. 2011;107:924–8. doi: 10.1111/j.1464-410X.2010.09679.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Isbarn H, Boccon-Gibod L, Carroll PR, et al. Androgen deprivation therapy for the treatment of prostate cancer: Consider both benefits and risks. Eur Urol. 2009;55:62–75. doi: 10.1016/j.eururo.2008.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nguyen PL, Je Y, Schutz FA, et al. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: A meta-analysis of randomized trials. JAMA. 2011;306:2359–66. doi: 10.1001/jama.2011.1745. [DOI] [PubMed] [Google Scholar]
- 7.Punnen S, Cooperberg MR, Sadetsky N, et al. Androgen deprivation therapy and cardiovascular risk. J Clin Oncol. 2011;29:3510–6. doi: 10.1200/JCO.2011.35.1494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Saylor PJ, Smith MR. Metabolic complications of androgen deprivation therapy for prostate cancer. J Urol. 2009;181:1998, 2006. doi: 10.1016/j.juro.2009.01.047. discussion 2007–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Soeyonggo T, Warde P, Fleshner N, et al. Information needs of men on androgen deprivation therapy. BJU Int. 2012;109:1503–9. doi: 10.1111/j.1464-410X.2011.10475.x. [DOI] [PubMed] [Google Scholar]
- 10.Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005;294:238–44. doi: 10.1001/jama.294.2.238. [DOI] [PubMed] [Google Scholar]
- 11.Keating NL, O’Malley A, Freedland SJ, et al. Diabetes and cardiovascular disease during androgen deprivation therapy: Observational study of veterans with prostate cancer. J Natl Cancer Inst. 2012;104:1518–23. doi: 10.1093/jnci/djs376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ehdaie B, Atoria CL, Gupta A, et al. Androgen deprivation and thromboembolic events in men with prostate cancer. Cancer. 2012;118:3397–406. doi: 10.1002/cncr.26623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Potosky AL, Reeve BB, Clegg LX, et al. Quality of life following localized prostate cancer treated initially with androgen deprivation therapy or no therapy. J Natl Cancer Inst. 2002;94:430–7. doi: 10.1093/jnci/94.6.430. [DOI] [PubMed] [Google Scholar]
- 14.Canadian Pharmacists Association. Compendium of pharmaceuticals and specialties. 2012 [Google Scholar]
- 15.Alibhai SM, Breunis H, Timilshina N, et al. Impact of androgen-deprivation therapy on cognitive function in men with nonmetastatic prostate cancer. J Clin Oncol. 2010;28:5030–7. doi: 10.1200/JCO.2010.30.8742. [DOI] [PubMed] [Google Scholar]
- 16.Daly PE, Dunne MT, O’Shea CM, et al. The effect of short term neo-adjuvant androgen deprivation on erectile function in patients treated with external beam radiotherapy for localised prostate cancer: An analysis of the 4-versus 8-month randomised trial (Irish Clinical Oncology Research Group 97-01) Radiother Oncol. 2012;104:96–102. doi: 10.1016/j.radonc.2012.05.001. [DOI] [PubMed] [Google Scholar]
- 17.Schow DA, Renfer LG, Rozanski TA, et al. Prevalence of hot flushes during and after neoadjuvant hormonal therapy for localized prostate cancer. South Med J. 1998;91:855–7. doi: 10.1097/00007611-199809000-00010. [DOI] [PubMed] [Google Scholar]
- 18.Heins MJ, Korevaar JC, Rijken PM, et al. For which health problems do cancer survivors visit their general practitioner? Eur J Cancer. 2013;49:211–8. doi: 10.1016/j.ejca.2012.07.011. . Epub 2012 Aug 14. [DOI] [PubMed] [Google Scholar]
- 19.Walker LM, Tran S, Wassersug RJ, et al. Patients and partners lack knowledge of androgen deprivation therapy side effects. Urol Oncol. 2013;31:1098–105. doi: 10.1016/j.urolonc.2011.12.015. http://dx.org/10.1016/j.urolonc.2011.12.015. Epub 2012 Jan 30. [DOI] [PubMed] [Google Scholar]
- 20.Lebret T, Coloby P, Descotes JL, et al. Educational tool-kit on diet and exercise: Survey of prostate cancer patients about to receive androgen deprivation therapy. Urology. 2010;76:1434–9. doi: 10.1016/j.urology.2010.07.483. [DOI] [PubMed] [Google Scholar]
- 21.Khan NF, Watson E, Rose PW. Primary care consultation behaviours of long-term, adult survivors of cancer in the UK. Br J Gen Pract. 2011;61:197–9. doi: 10.3399/bjgp11X561195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Del Giudice ME, Grunfeld E, Harvey BJ, et al. Primary care physicians’ views of routine follow-up care of cancer survivors. J Clin Oncol. 2009;27:3338–45. doi: 10.1200/JCO.2008.20.4883. [DOI] [PubMed] [Google Scholar]
- 23.Gray RE, Carroll J, Goel VV, et al. Canadian family physicians and prostate cancer: A national survey. Can J Urol. 1999;6:892–7. [PubMed] [Google Scholar]
- 24.Hiramanek N. Self directed learning and continuing medical education. Aust Fam Physician. 2005;34:879–80. [PubMed] [Google Scholar]
- 25.MacLeod S. How GPs learn. Educ Prim Care. 2009;20:271–7. [PubMed] [Google Scholar]