

Abstract
This article reviews the present indicators, trends, and recent solutions and strategies to tackle major global and country problems in safety and health at work. The article is based on the Yant Award Lecture of the American Industrial Hygiene Association (AIHA) at its 2013 Congress. We reviewed employment figures, mortality rates, occupational burden of disease and injuries, reported accidents, surveys on self-reported occupational illnesses and injuries, attributable fractions, national economic cost estimates of work-related injuries and ill health, and the most recent information on the problems from published papers, documents, and electronic data sources of international and regional organizations, in particular the International Labor Organization (ILO), World Health Organization (WHO), and European Union (EU), institutions, agencies, and public websites. We identified and analyzed successful solutions, programs, and strategies to reduce the work-related negative outcomes at various levels. Work-related illnesses that have a long latency period and are linked to ageing are clearly on the increase, while the number of occupational injuries has gone down in industrialized countries thanks to both better prevention and structural changes. We have estimated that globally there are 2.3 million deaths annually for reasons attributed to work. The biggest component is linked to work-related diseases, 2.0 million, and 0.3 million linked to occupational injuries. However, the division of these two factors varies depending on the level of development. In industrialized countries the share of deaths caused by occupational injuries and work-related communicable diseases is very low while non-communicable diseases are the overwhelming causes in those countries. Economic costs of work-related injury and illness vary between 1.8 and 6.0% of GDP in country estimates, the average being 4% according to the ILO. Singapore's economic costs were estimated to be equivalent to 3.2% of GDP based on a preliminary study. If economic losses would take into account involuntary early retirement then costs may be considerably higher, for example, in Finland up to 15% of GDP, while this estimate covers various disorders where work and working conditions may be just one factor of many or where work may aggravate the disease, injury, or disorders, such as traffic injuries, mental disorders, alcoholism, and genetically induced problems. Workplace health promotion, services, and safety and health management, however, may have a major preventive impact on those as well. Leadership and management at all levels, and engagement of workers are key issues in changing the workplace culture. Vision Zero is a useful concept and philosophy in gradually eliminating any harm at work. Legal and enforcement measures that themselves support companies and organizations need to be supplemented with economic justification and convincing arguments to reduce corner-cutting in risk management, and to avoid short- and long-term disabilities, premature retirement, and corporate closures due to mismanagement and poor and unsustainable work life. We consider that a new paradigm is needed where good work is not just considered a daily activity. We need to foster stable conditions and circumstances and sustainable work life where the objective is to maintain your health and work ability beyond the legal retirement age. We need safe and healthy work, for life.
Keywords: burden of injury and illness at work, global estimates, mortality, occupational accidents, occupational exposures, work-related disease
INTRODUCTION
Based on different starting points the International Labor Organization (ILO) and the World Health Organization (WHO), have made estimates of occupational injuries and illnesses or burden of disease. ILO has made global estimates from the point of view of occupational burden and WHO from the health point of view. Both of them have come to the conclusion that of all fatalities in industrial countries some 5–7%(1,2) is attributed to work-related illnesses and occupational injuries. This percentage is somewhat smaller in developing countries where non-occupational health problems have a bigger share.(3) While new information gradually becomes available from various sources, and when work processes, work environment, and working populations change quantitatively and qualitatively, updates of the estimates become important. Better evidence is needed for policy and practices in countries, companies, and organizations. This article and related presentation provide the latest updated information for such purposes. The article is based on the Yant Award Lecture of the American Industrial Hygiene Association (AIHA) at its 2013 Congress.
Economic cost studies related to injuries and illnesses have been carried out using different methods. The most appropriate method has been the incidence approach where new injuries, diseases, and disorders occurring in a particular year are counted. Once this is known— e.g., by using the attributable fraction (AF) method—all direct and indirect costs can be calculated, including costs that are extended to the expected total work life starting from an incidence in the year under consideration. Usually long term disabilities, reduced work ability and capacity due to partial disabilities, premature retirement from work, and deaths cause a lion share of economic costs. Studies and estimates by many countries and the ILO have shown that economic costs of work-related illness and injury would be equivalent to a range from 1.8%–6% of GDP.
The objective of this article is to provide an overall view of the latest data and knowledge on workplace safety and health—as yet more evidence for policy and practice.
MATERIALS AND METHODS
Member states of ILO and WHO report their own statistics regularly and these are collected, recorded, and reported by these United Nations (UN) bodies. Reports from developed countries are usually more comprehensive but a large number of countries do not properly report their data on occupational injuries and illnesses. Such missing data for occupational injuries may be replaced by a proxy, a country, or an average of several countries that have closely resembling economic structures and methods of production and work cultures, and that have reported such data well.
Occupational injuries (accidents) are followed and recorded in many countries and the ILO, European Union (EU), and to some extent other regional organizations collect and record such national data. However, national systems are usually poorly standardized and international comparisons are difficult. The best recorded data involves fatal injuries and this is also the starting point for estimating the number of less severe injuries. The methodology on establishing more comparable estimates for occupational deaths and injuries has been described in several papers while the methodology has gradually been improved.(4–6)
Reliable and comparable occupational disease statistics based on compensated cases are not available at the global level. This lack has been compensated for by the population attributable fractions (AF) for work-related illnesses—a wider concept than the usually legally defined term of “occupational diseases.” The AFs are commonly used to measure the component or fraction of such illnesses and deaths that are related to work. Those fractions have been extensively studied in developed countries but very limited information from developing countries exists. WHO mortality tables by different regions provide background data and by using the AF component as a percentage, it is possible to provide a rough estimate of the fatalities for each disease or group of diseases. ILO and WHO data and complementary data from individual member states and from the EU have been used. These data are based on latest possible sources from the years 2008–2011. Updating is done regularly.(7)
The most important AF values used by the ILO study were as follows(8):
-
(i)
work-related cancer: AF = 8.4% (13.8% male, 2.2% female) of all cancer deaths
-
(ii)
asbestos: lung cancer and mesothelioma 12.2% (14.0% male, 0.6% female)
-
(iii)
external tobacco (passive) smoke, lung cancer, and circulatory diseases: AF lung cancer = 3.0 − 2.0% m/f
-
(iv)
circulatory system diseases: AF=12.4% (14.4% male, 6.7% female)
-
(v)
respiratory system diseases: AF = 4.1% (6.8% male, 1.1% female)
-
(vi)
communicable diseases: AF = 8.8% (4.8% male, 32.5% female, the latter being high due to occupational infections in the health sector). This high AF value was adjusted for developing countries where health sector exposure is small compared to other exposures in agriculture and elsewhere, such as tropical diseases, bacteria, viruses, and vector-borne diseases.
Studies adapted by ILO for use as global estimates state that the overall AF for work-related causes was 6.7% (2005).(5) The AF method is widely used to assess work-relatedness of a broad range of diseases and disorders.
These AF values have been adapted from those used originally in Finland.(9) These have been used in other parts of the world, in particular, by ILO and in Australia,(10) New Zealand,(11) and Alberta, Canada.(12) Estimates based on these AF values have been reviewed to be the most representative globally(13) so far. While somewhat different AF values have been used, such as those by Steenland (2003),(14) new information has come much closer to the above-mentioned AF values used by the ILO. For example, Rushton et al.,(15) have demonstrated that occupational cancer in the U.K. kills 8010 people annually. After this study a group from the International Agency for the Research of Cancer (IARC), led by MacGormack(16) have shown that the number of mesothelioma cases can be used as an indication and proxy for asbestos exposures that do cause both mesothelioma and lung cancer. The number of deaths caused by lung cancer could be 2–10 times that of mesothelioma. So far much lower lung cancer estimates have been used in past studies. Asbestos alone causes 112,000 deaths annually (Takala/ILO/EU(17)) and 90,000 deaths according to WHO(18) and Nishikawa et al.(19) A comparative list of AF values is given in the Table I enclosed.(20)
TABLE I.
Examples of Attributable Fractions
| Attributable fraction | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nurminen and Karjalainen(9) |
Rushton et al.(15) |
Steenland et al.(14) |
Driscoll et al.(13)A |
Morrel et al.21,B |
Leigh et al.(22)C |
||||||||
| Causes | Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | Men | Women | |
| Communicable diseases | 4.8 | 32.5 | |||||||||||
| Tuberculosis | 0.6 | 75 | 5–6 | ||||||||||
| Malignant neoplasms | 13.8 | 2.2 | 8.0 | 1.5 | 3.3–7.3 | 0.8–1.0 | 6–10 | ||||||
| Bladder | 14.2 | 0.7 | 11.6 | 2.0 | 7–19 | 3–19 | 10 | 5 | |||||
| Kidney | 4.7 | 0.8 | 0–2.3 | 1 | 0.5 | ||||||||
| Larynx | 9.3 | 0.5 | 1.0–20.0 | 2 | 1 | ||||||||
| Leukemia | 18.5 | 2.5 | 2.7 | 0.8 | 0.8–2.8 | 2(b) | 2(b) | 10 | 5 | ||||
| Liver | 3.5 | 5.3 | 0.4–1.1 | 4 | 1 | ||||||||
| Lung | 29.0 | 5.3 | 21.6 | 5.5 | 8.0–19.2 | 2 | 10(b) | 5(b) | 15 | 5 | |||
| Mesothelioma | 90.0 | 25.0 | 98.0 | 90.0 | 85–90 | 23–90 | |||||||
| Non-melanoma skin cancer | 13.1 | 3.8 | 11.8 | 3.0 | 1.2–6.0 | 10 | 2 | ||||||
| Sinonasal | 24.0 | 6.7 | 64.3 | 18.4 | 33.0–46.0 | 30.0–42.0 | 25 | 5 | |||||
| Respiratory diseases | 6.8 | 1.1 | 10c | ||||||||||
| Asthma | 17.8 | 18.4 | 11–12 | 21(c) | 13(c) | 2.0 | 2.0 | ||||||
| COPD | 14.0 | 3.8 | 5–24 | 18(c) | 6(c) | ||||||||
| Pneumoconioses | 100 | 100 | 100 | 100 | 100 | 100 | 100 | ||||||
| Circulatory diseases | 14.4 | 6.7 | 6.3 | 1.0 | 1.0 | 5–10 | |||||||
| Neuropsychiatric conditions | 6.6 | 1.8 | 1.0 | 1.0 | 1–3 | ||||||||
| Digestive diseases | 2.3 | 1.5 | |||||||||||
| Genitourinary system | 3.0 | 0.4 | 1.0 | 1.0 | 1–3 | ||||||||
Note: COPD = chronic obstructive pulmonary disease.
Attributable fractions have been taken from two papers of Driscoll et al.
Covers only deaths due to occupational exposure to hazardous substances
Pneumoconiosis is not included in the figure of Leigh at al.
The ILO has estimated that 4%% of annual global GDP, or US$2.8 trillion, is lost due to the direct and indirect costs of occupational accidents and diseases, including lost working time, workers’ compensation, interruption of production, and medical expenses.(21)
Many studies on the economic cost of workplace injuries and diseases have been conducted. Leigh(22) estimated that the national cost of work-related injuries and diseases in the United States amounted to US$250 billion (1.8% of GDP). Safe Work Australia estimated that the costs of work-related injuries and illnesses for Australia were AU$57.5 billion (5.9% of GDP)(23) for 2005–2006 and AU$60.6 billion (4.8% GDP) for 2008–2009.(24) The European Agency for Safety and Health at Work made a Member State Survey on the estimated economic costs: some results are as follows(25)
Norway(26) 6.0% of GDP (not in the EU report)
Sweden 4.0% of GDP
Finland(27) 3.8% of GDP
Italy 3.2%
Denmark 2.7%
New Zealand(28) 3.4% of GDP (financial cost, not in the EU report)
The report on New Zealand stated that only 10% of the financial cost is compensated and the cost of suffering and premature death was 77% of total costs while the financial costs were 21% of total costs and compensated costs were 2% of all costs.
In estimating the economic costs the Workplace Safety and Health (WSH) Institute in Singapore reviewed the methodologies and cost models from different countries and global estimates when developing a preliminary economic cost model for Singapore. In this model, Figure 1, the Institute determined the cost of work-related injuries and ill health that would be borne by employers, workers, and the community. Cost items linked to staff turnover, training of replacement workers, loss of worker output, insurance premiums, and legal costs incurred were computed as costs borne by employers. The costs borne by workers included expenses beyond those covered by compensation for medical treatment, rehabilitation, and loss of future earnings. Cost items like social payouts, costs of investigation, inspection, and promotion activities, and loss of human capital for fatal cases and medical subsidy were considered as costs borne by community. The adopted incidence model does not take into account the cost from property damage and human pain and suffering.
FIGURE 1.
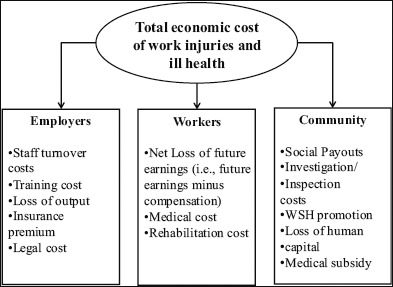
Cost items borne by employers, workers, and the community
RESULTS
Globally 2.3 million deaths take place(29) due to occupational injuries (318,000 deaths) and work-related diseases (2,022,000 deaths) annually, see Figure 2. The biggest killers are work-related cancer (32%); work-related circulatory diseases (23%), cardiovascular and stroke; communicable diseases (17%), in particular, in developing countries and farming, and occupational accidents (18%). The last two causes, however, are less common in the established market economy countries (see Figure 3). The main reason for the difference is that the overall number of communicable diseases has been relatively low in high-income countries, and that pattern seems to continue also in rapidly developing countries such as China.
FIGURE 2.
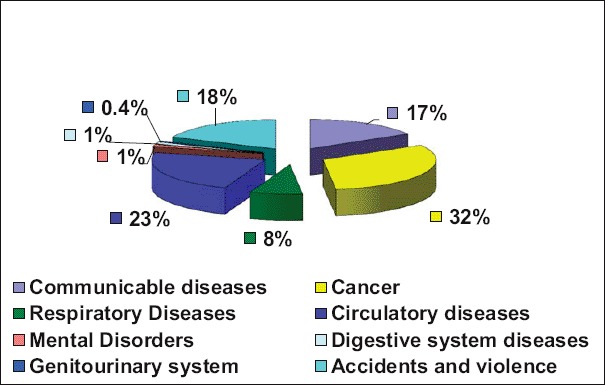
Work-related annual deaths – World (Sources: Hämäläinen P, Takala J, Saarela KL; TUT, ILO, EU-OSHA, 2008).
FIGURE 3.
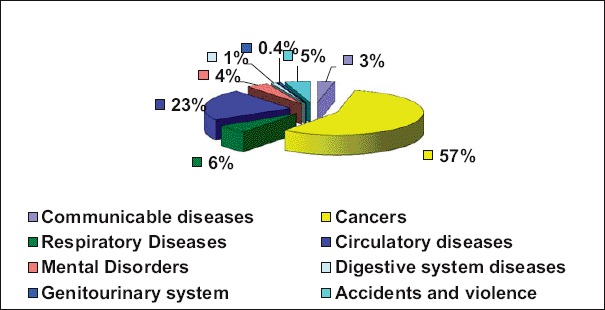
Work-related annual deaths – EU and the pattern in other industrialized countries (Sources: Hämäläinen P, Takala J, Saarela KL; TUT, ILO, EU-OSHA).
However, while there has been a clear long-term declining trend for occupational injuries, in global terms this has been offset by the increase in occupational injury fatalities due to shifting of manufacturing, construction, mining, and agriculture in rapidly industrially progressing countries, in particular Asian countries.
While industrialized economies have gained through better leadership, management, and cultures and reduced the number of industrial injuries, another major part of the gain is caused by the gradual move of hazardous industries to Asia. Furthermore, in many high-income countries that positive development has become increasingly difficult to continue. Fatal injuries have stagnated and another quantum leap or paradigm change is required.
Today, occupational injuries form a small part of the mortality of high-income countries, the goal posts for prevention of risks are moving, and new disorders are becoming more important. Long-term latency disorders continue to grow and cause fatalities—for example lung cancer and circulatory diseases—and long-term absences caused by musculoskeletal disorders and psychosocial factors. These are ranked as major problems by enterprises and organizations in economic sectors employing a large number of people. These are ranked as major problems by enterprises and organizations in economic sectors employing a large number of people, such as government and municipal workers, health and education sectors.
Competitiveness and safety and health go hand-in-hand; the lower the number of accidents the higher is the competitiveness and productivity. Figure 4 illustrates the link between competitiveness as measured by the World Economic Forum(30) in 2013, and total accident rates using data reported to the ILO.(6) While ILO data are from the year 2008, the total global numbers have not changed radically from the past. The United States had 96,000 fatal work-related diseases and 5,300 fatal occupational injuries including an adjustment for under reporting, while the competitiveness ranking was the highest in the world in 2008; today the United States is ranked seventh. Canada had 11,330 fatal work-related illnesses and 479 fatal occupational injuries and its competitiveness ranking today is 12.
FIGURE 4.
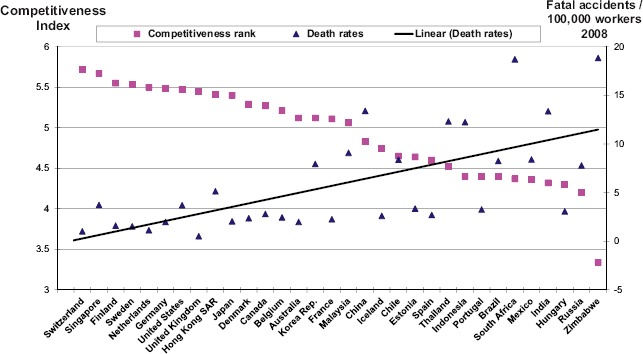
Inverse correlation of competitiveness and occupational safety (Source: WSH Institute and World Economic Forum Lausanne, Switzerland, 2012–2013 http://www3.weforum.org/docs/WEF_GlobalCompetitivenessReport_2012–13.pdf.
Regions follow WHO Regions except for the high-income countries and EU27 that are separately covered and excluded from corresponding WHO Regions in Table II.
TABLE II.
Work-related Injuries and Diseases in the World
| Region | Economically Active Population | Fatal (Reported) | Four or more days absence | Fatal Injuries ILO estimates | Four or more days absence: ILO mid-point estimate | Fatal work-related diseases | Total work-related mortality |
|---|---|---|---|---|---|---|---|
| High-Income Areas | 494,365,003 | 11,850 | 4,959,039 | 14,090 | 14,665,130 | 306,988 | 321,077 |
| African Region | 251,588,449 | 759 | 46,616 | 44,699 | 46,561,176 | 336,144 | 380,843 |
| American Region | 315,509,490 | 1,944 | 657,580 | 25,534 | 8,866,101 | 113,023 | 138,557 |
| Eastern Mediterranean | 152,610,995 | 0 | 0 | 17,912 | 18,657,924 | 117,164 | 135,076 |
| European Region | 213,740,690 | 6,777 | 325,004 | 16,191 | 18,093,167 | 198,366 | 214,557 |
| Southeast Asia | 642,390,831 | 81 | 1,676 | 83,096 | 86,558,781 | 523,355 | 606,451 |
| Western Pacific | 921,078,060 | 193 | 43,756 | 119,058 | 124,019,195 | 427,530 | 546,588 |
| Total | 2,991,283,518 | 21,604 | 6,033,671 | 320,580 | 317,421,473 | 2,022,570 | 2,343,149 |
Notes: WHO Regions in the Region column are listed at: http://www.who.int/healthinfo/global_burden_disease/definition_regions/en/; High-income Areas: see Table III.
High-income countries are listed in Table III.
TABLE III.
Work-related Injuries and Diseases in High-iiincome Countries. (EU27 countries are included in the list and total for EU27 is given separately.)
| Region | Economically Active Population | Fatal (Reported) | Four or more days absence | Fatal Injuries ILO estimates | Four or more days absence: ILO mid-point estimate | Fatal work-related diseases | Total work-related mortality |
|---|---|---|---|---|---|---|---|
| Andorra | 42,220 | 1 | 942 | 26 | 27 | ||
| Australia | 11,211,400 | 207 | 98,980 | 213 | 222,094 | 6,962 | 7,175 |
| Austria | 4,252,300 | 115 | 74,142 | 118 | 123,385 | 2,641 | 2,759 |
| Bahamas | 185,100 | 13 | 4,434 | 115 | 128 | ||
| Bahrain | 359,500 | 23 | 952 | 27 | 28,042 | 223 | 250 |
| Belgium | 4,779,600 | 109 | 113,324 | 2,968 | 3,077 | ||
| Brunei | 157,600 | 5 | 5,571 | 98 | 103 | ||
| Canada | 18,245,000 | 465 | 260,097 | 479 | 498,906 | 11,330 | 11,809 |
| Cyprus | 397,400 | 12 | 2,355 | 12 | 12,500 | 247 | 259 |
| Denmark | 2,925,800 | 67 | 69,519 | 1,817 | 1,884 | ||
| Finland | 2,726,000 | 41 | 42,708 | 1,693 | 1,734 | ||
| France | 27,982,000 | 569 | 703,976 | 586 | 610,417 | 17,376 | 17,962 |
| Germany | 41,874,000 | 765 | 1,063,150 | 765 | 796,875 | 26,003 | 26,768 |
| Greece | 4,939,700 | 150 | 156,072 | 3,067 | 3,217 | ||
| Greenland | 27,600 | 1 | 829 | 17 | 18 | ||
| Guernsey | 31,470 | 0 | 20 | 20 | |||
| Iceland | 184,100 | 5 | 4,860 | 114 | 119 | ||
| Ireland | 2,224,000 | 57 | 59 | 61,458 | 1,381 | 1,440 | |
| Isle of Man | 41,800 | 1 | 159 | 1 | 1,042 | 26 | 27 |
| Israel | 2,957,000 | 89 | 69,734 | 61 | 63,748 | 1,836 | 1,897 |
| Italy | 25,097,000 | 780 | 499,210 | 653 | 680,232 | 15,585 | 16,238 |
| Japan | 66,500,000 | 1,268 | 118,023 | 1,306 | 1,360,458 | 41,295 | 42,601 |
| Jersey | 53,560 | 0 | 33 | 33 | |||
| Korea, Republic of | 24,347,000 | 1,332 | 1,872 | 1,949,916 | 15,119 | 16,991 | |
| Kuwait | 1,146,400 | 66 | 68,947 | 712 | 778 | ||
| Liechtenstein | 32,435 | 1 | 990 | 20 | 21 | ||
| Luxembourg | 218,100 | 10 | 10,617 | 10 | 10,417 | 135 | 145 |
| Malta | 171,400 | 3 | 4,023 | 3 | 3,125 | 106 | 109 |
| Monaco | 12,696 | 0 | 8 | 8 | |||
| Netherlands | 8,717,000 | 92 | 95 | 98,958 | 5,413 | 5,508 | |
| New Zealand | 2,283,200 | 90 | 26,482 | 93 | 96,563 | 1,418 | 1,511 |
| Norway | 2,591,000 | 51 | 16,630 | 53 | 55,208 | 1,609 | 1,662 |
| Portugal | 5,624,700 | 170 | 177,050 | 3,493 | 3,663 | ||
| Qatar | 1,171,500 | 61 | 63,948 | 727 | 789 | ||
| San Marino | 22,708 | 1 | 602 | 14 | 15 | ||
| Saudi Arabia | 8,374,900 | 582 | 606,054 | 5,201 | 5,782 | ||
| SingaporeA | 1,928,400 | 67 | 11,005 | 69 | 71,885 | 1,197 | 1,266 |
| Slovenia | 1,033,000 | 27 | 28,196 | 641 | 669 | ||
| Spain | 22,848,200 | 530 | 802,778 | 546 | 568,750 | 14,188 | 14,734 |
| Sweden | 4,896,000 | 68 | 28,327 | 70 | 72,917 | 3,040 | 3,110 |
| Switzerland | 4,375,000 | 42 | 90,259 | 43 | 44,792 | 2,717 | 2,760 |
| United Arab Emirates | 1,923,214 | 130 | 135,557 | 1,194 | 1,324 | ||
| United Kingdom | 31,118,000 | 152 | 158,333 | 19,323 | 19,475 | ||
| United States | 154,287,000 | 5,214 | 1,078,140 | 5,370 | 5,594,188 | 95,808 | 101,179 |
| Virgin Islands, U.S. | 49,000 | 4 | 1,316 | 30 | 34 | ||
| Total | 494,365,003 | 11,850 | 4,959,039 | 14,090 | 14,665,130 | 306,988 | 321,077 |
| EU27 included above | 237,997,300 | 4,706 | 3,409,088 | 5,900 | 7,374,297 | 161,970 | 167,870 |
Singapore details are based on permanent workforce in 2008 (as for other countries); new updated data are available and were used for the economic cost calculations.
The only region or group where the level of accident reporting is relatively close to expected numbers is the group of high-income countries. In contrast, most other regions have low levels of reporting. This will also provide a false picture to decision makers believing that there is no reason to be worried. This in turn will become not only an economic obstacle to increasing competitiveness and productivity but will continue to increase pressures for basic human rights. No country has shown a high level of competitiveness and productivity while maintaining poor safety records. Such links exist for companies and organizations as well while small- and medium-sized enterprises may not have firsthand feedback of poor working conditions in the form of accidents that are statistically not common in smaller populations.
The EU data related to occupational injuries have been separately studied by Eurostat through a self-reported injury and illness survey in all EU Member States. The result of this study concluded that in the EU27 there were 7 million occupational injuries, or 3.2% of the workforce, in 2007.(31) This validated perfectly the ILO estimate, mentioned previously, that arrived at 7.37 million occupational injuries based on ILO data from 2008, data collection must have been earlier than that. On the other hand 8.6% of workers in the EU-27 experienced a work-related health problem in the past 12 months, which corresponds to 20 million workers.
Economic costs in Singapore
The estimated cost in Singapore was equivalent to 3.2% of the Singapore GDP in 2011. This is comparable to similar studies done by other countries, e.g., Australia (4.8%) and the ILO (4%). Workers bore about half of these costs (51%) while the rest is shouldered by employers (22%) and the community (27%).
The circumstances in Singapore reflect those of other highly developed countries. As a result of having overcome most communicable diseases as a cause of death, the relative importance of non-communicable diseases and disorders is constantly increasing. Some diseases that have a clear linkage to work are work-related cancers, circulatory diseases, chronic respiratory diseases, musculoskeletal disorders, and psychosocial factors at work, among others.
As a whole the magnitude of economic costs in any country and region is radically different from those of the activities targeted to prevention. Figure 5 demonstrates the imbalance between safety and health action and costs of work-related injuries and illnesses including those caused by absenteeism and involuntary early retirement in the EU.(32) The calculations are based on expenditure calculations by Ahonen(33) in Finland and adapted by authors of this article.
FIGURE 5.
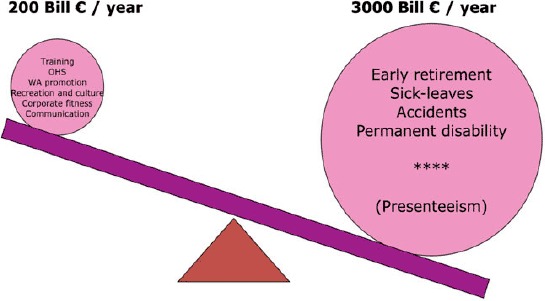
Imbalance between investments into safety and health and costs due to lack of safety and health in the European Union EU27 (Source: Prof. G. Ahonen, adaptation J. Takala).
DISCUSSION: TRENDS, STRATEGIES, AND SOLUTIONS
Taking into account the risks involved and the fact that both traditional and new and emerging risks need to be studied, new innovations and solutions need to be identified. Singapore, based on models in the United States and elsewhere, has decided to concentrate on two aspects:
-
1.
Establishing a Research Agenda setting priorities for the continuous search for evidence for policy and practice(34)
-
2.
Building a Risk Observatory or Observatory for Workplace Landscape (OWL).(35)
Often perceptions drive action more than real evidence and it is important to highlight the difference between media interest, public attention, and real evidence for policy and practice. Media, including social media, are vital for communication, for reaching large number of stakeholders, workers, small and medium-sized enterprises (SMEs), the informal sector, migrant workers, and vulnerable groups, and to foster a safety culture at places of work. Figure 6 illustrates, however, that misperceptions in assessing risks exist. In particular statistical risks are not easy to assess correctly. Further, common everyday risks are underestimated and complicated technologically and risks not easily controlled by individuals are overrated.
FIGURE 6.
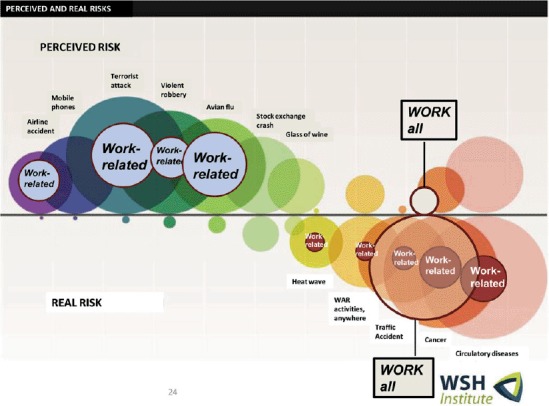
Perceptions of people are different from reality (Sources: S. Hertlich, M. Hamilo, S. Kuvalehti [FI], WHO/ILO/J.Takala).
Leadership, management, and systems thinking at all levels(36) and related worker engagement have been identified as key for efforts to ensure workplace safety and health.(37) Recent experiences from mega-projects such as the London Olympics construction effort were successful exactly because of emphasis on and continuous follow-up of these factors.(38)
The numbers presented in Tables I and II are alarmingly high and often poorly understood, and their importance has been underestimated. One should also keep in mind that the targets or “goal posts” are gradually moving due to changes in work, workplace, and work force. A systems approach is necessary at all levels. An enterprise management system is the strategic component for an organization,(39) but an action program for risk assessment and priority setting for risk management is also needed. Collaboration between management and workers at the organizational (enterprise) level must be followed by a national-level mechanism, such as a tripartite advisory council, that looks after wider issues like new legal measures and better strategic enforcement. Contrary to some perceptions enforcement supports employers in reducing injuries and injury claims, and saving compensation costs, on average 26% or US$355,000, as a result of inspection of the company, and saving employers US$6 billion nationwide. This counts neither the costs of lost production of the injured workers nor the pain and suffering.(39,40)
Several key processes have been gaining momentum, such as design for safety, and control banding based on the new Globally Harmonized System for Classification and Labelling of Chemicals (GHS) labelling requirements. One groundbreaking and new longer-term concept, or philosophy, is Vision Zero. The idea is to change the values and mindset of all stakeholders from business as usual and ensure zero accidents, zero illnesses, zero exposures, zero violence, zero harassment, simply zero harm during an entire working life as the ultimate goal. So far it has been launched for selected special needs already, such as the Swedish traffic vision.(41)
CONCLUSION
K Key action programs should concentrate on finding solutions and reducing exposures for illnesses that have a long latency period. For each injury and illness there are many factors with influence on the negative outcomes. Cultures that start from committed and capable leadership in the organization need to be developed and presently known best practices as well as new innovations at an organization and country levels need to be identified and used. In addition to laws, enforcement, and health and safety services, media including social media should be better used for promotion of safety, health, and well-being at work.
Occupational injuries and work-related diseases and disorders are a bigger problem than estimated earlier. Longer-term risks are gradually increasing in importance at workplaces. A toolbox comprising: (i) legal measures, (ii) enforcement, (iii) knowledge and solutions, (iv) incentives, (v) awareness raising and campaigns, (vi) services available to enterprises and organizations such as occupational health services, and (vii) networking for best exchange of good practice is vital for any successful strategy for safety, health, and well-being at work.
A comprehensive toolbox model is the ILO Convention no. 187 on the Promotional Framework for Occupational Safety and Health.42 Safe work, healthy work is all about decent work, good work, for life.
In the words of the former Secretary General of the United Nations, Kofi Annan: “Health and safety at work is not just sound economic policy it is a basic human right.”
REFERENCES
- 1.International Labor Organization (ILO) Occupational Safety and Health: Synergies Between Security and Productivity. Geneva: WHO; 2006. [Google Scholar]
- 2.Murray C., Lopez A. Global Burden of Disease. Geneva: World Health Organization (WHO)/World Bank/Harvard School of Public Health; 1996. [Google Scholar]
- 3.Elgstrand K., Petersson N. OSH for Development. Stockholm, Sweden: Royal Institute of Technology; 2010. Available at https://osha.europa.eu/en/press/articles/review_osh_for_development (accessed May 16, 2013). [Google Scholar]
- 4.Hämäläinen P., Takala J., Saarela K.L. Global estimates of occupational accidents. Safety Sci. 2006;44:137–156. (). [Google Scholar]
- 5.Takala J. ILO Introductory Report: Decent Work-Safework. Available at http://www.ilo.org/public/english/region/eurpro/moscow/areas/safety/docs/worldcongressreporteng.pdf (accessed January 20, 2014)
- 6.Hämäläinen P., Saarela K.L., Takala J. Global trend according to estimated number of occupational accidents and fatal work-related diseases at region and country level. J. Safety Res. 2009;40(2):125–139. doi: 10.1016/j.jsr.2008.12.010. (). [DOI] [PubMed] [Google Scholar]
- 7.Hämäläinen P., Takala J., Saarela K.L. Global estimates of fatal work-related diseases. Am. J. Ind. Med. 2007;50(1):28–41. doi: 10.1002/ajim.20411. (). [DOI] [PubMed] [Google Scholar]
- 8.Takala J., Urrutia M., Hämäläinen P., Saarela K.L. The global and European work environment—Numbers, trends, and strategies. Scan. J. Work Environ. Health. 2009. pp. 15–23. ().
- 9.Nurminen M., Karjalainen A. Epidemiologic estimate of the proportion of fatalities related to occupational factors in Finland. Scan. J. Work. Environ. Health. 2001;27(3):161–213. doi: 10.5271/sjweh.605. (). [DOI] [PubMed] [Google Scholar]
- 10.Fritschi L., Driscoll T. Cancer due to occupation in Australia. Aust. N. Z. J. Pub. Health. 2006;30(3):213–219. doi: 10.1111/j.1467-842x.2006.tb00860.x. (). [DOI] [PubMed] [Google Scholar]
- 11.Mannetje A., Pearce N. Quantitative estimates of work-related death, disease and injury in New Zealand. Scand. J. Work Environ. Health. 2005;31(4):266–276. doi: 10.5271/sjweh.882. (). [DOI] [PubMed] [Google Scholar]
- 12.Orenstein M.R., Dall T., Curley P., Chen J., Tamburrini A. L., Petersen J. The Economic Burden of Occupational Cancers in Alberta. Calgary: Alberta Health Services; Available at http://www.albertahealthservices.ca/poph/hi-poph-surv-phidseconomic-burden-occup-cancer-2010.pdf (accessed June 10, 2013). [Google Scholar]
- 13.Driscoll T., Takala J., Steenland K., Corvalan C., Fingerhut M. Review of estimates of the global burden of injury and illness due to occupational exposures. Am. J. Ind. Med. 2005;48:491–502. doi: 10.1002/ajim.20194. (). [DOI] [PubMed] [Google Scholar]
- 14.Steenland K., Burnett C., Lalich N., Ward E., Hurrell J. Dying for work: The magnitude of US mortality from selected causes of death associated with occupation. Am. J. Ind. Med. 2003;43(5):461–482. doi: 10.1002/ajim.10216. (). [DOI] [PubMed] [Google Scholar]
- 15.Rushton L., Hutchings S.J., Fortunato L., et al. Occupational cancer burden in Great Britain. Br. J. Can. 2012;107:S3–S7. doi: 10.1038/bjc.2012.112. (). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.McCormack V., Peto J., Byrnes G., Straif K., Boffetta P. Estimating the asbestos-related lung cancer burden from mesothelioma mortality. Br. J. Can. 2012;106(3):575–584. doi: 10.1038/bjc.2011.563. (). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Takala J. EFBWW Conference. Brussels: European Parliament; 2011. Asbestos—Chrysotile, Trends and Numbers.”. June 30. [Google Scholar]
- 18.World Health Organization (WHO) “WHO Mortality Database: World Health Organization Statistical Information System (WHOSIS).” Available at http://www.who.int/healthinfo/morttables/en/index.html (accessed Dec. 10, 2006).
- 19.Nishikawa K., Takahashi K., Karjalainen A., et al. Recent mortality from pleural mesothelioma, historical patterns of asbestos use, and adoption of bans: A global assessment. Environ. Health Perspect. 2008;116(12):1675–1680. doi: 10.1289/ehp.11272. (). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hämäläinen P. Global Estimates of Occupational Accidents and Fatal Work-Related Diseases. Ph.D. thesis, Publication 917. Tampere, Finland: Tampere University of Technology, 2010.
- 21.Morrell S., Kerr C., Driscoll T., Salkeld G., Corbett S. Best estimate of the magnitude of mortality due to occupational exposure to hazardous substances. Occupational and Environmental Medicine. 1998;55:634–641. doi: 10.1136/oem.55.9.634. (). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Leigh J. P. Economic burden of occupational injury and illness in the United States. Milbank Quarterly. 2011;89(4):728–772. doi: 10.1111/j.1468-0009.2011.00648.x. (). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Australian Safety and Compensation Council. “The Cost of Work-related Injury and Illness for Australian Employers, Workers and the Community.” Available at http://www.safeworkaustralia.gov.au/sites/swa/about/publications/pages/sr200903injuryandillness2005to2006 (accessed January 20, 2014).
- 24.Australian Safety and Compensation Council. “The Costs of Work-related Injury and Illness for Australian Employers, Workers and the Community.” Available at http://www.safeworkaustralia.gov.au/sites/swa/statistics/cost-injury-illness/pages/cost-injury-illness (accessed January 20, 2014).
- 25.European Agency for Safety and Health at Work. “Economic Impact of Occupational Safety and Health in the Member States of the European Union.” Available at https://osha.europa.eu/en/publications/reports/302 (accessed May 16, 2013).
- 26.Rognstad K. Costs of occupational accidents and diseases in Norway. Eur. J. Op. Res. 1994;75(3):553–566. (). [Google Scholar]
- 27.Takala J. International agency efforts to protect workers and the environment. Int. J. Occup. Environ. Health. 1999;5(1):30–37. doi: 10.1179/oeh.1999.5.1.30. (). [DOI] [PubMed] [Google Scholar]
- 28.Pezzulo L., Crook A. The Economic and Social Costs of Occupational Disease and Injury in New Zealand. NOHSAC Technical Report 4, 2006. Available at http://www.dol.govt.nz/publications/nohsac/pdfs/technical-report-04.pdf (accessed May 16, 2013).
- 29.International Labor Organization (ILO) “XIX World Congress on Safety and Health at Work.” Available at http://www.perosh.eu/wp-content/uploads/2013/06/PEROSH_OSH-and-Competitiveness_G_Ahonen_FIOH.pdf (accessed January 20, 2014).
- 30.Schwab K. The Global Competitiveness Report 2012–2013. Geneva: World Economic Forum; 2012. Available at http://www.weforum.org/docs/WEF_GlobalCompetitivenessReport_2012–13.pdf (accessed June 17, 2013). [Google Scholar]
- 31.Eurostat. “Statistics in Focus 63/2009: 8.6% of Workers in the EU Experienced Work-related Health Problems.” Population and Social Conditions. Available at http://epp.eurostat.ec.europa.eu/cache/ITY_OFFPUB/KS-SF-09-063/EN/KS-SF-09-063-EN.PDF (accessed May 16, 2013).
- 32.Takala J. 5th International FOHNEU Congress. Spain: Tarragona; 2012. Future Perspectives in Occupational Health and Safety. Sept. 21. [Google Scholar]
- 33.Ahonen G. OSH and Corporate Competitiveness in a Global Context. PEROSH Seminar at European Parliament. 2010. Brussels.
- 34.Chen Y., Tan S., Lim S. Singapore workplace safety and health research agenda: Research-to-practice. J. Safety Health Env. Res. 2012;8(1):27–32. () [Google Scholar]
- 35.Observatory for WSH Landscape. “OWLinks,” Workplace Safety and Health Institute. Available at http://www.wshi.gov.sg/Observatory-WSHLandscape/OWLinks.html (accessed May 16, 2013).
- 36.Leadership in Singapore: Prime Minister's Statement Through the ILO. Available at http://www.ilo.org/safework/events/meetings/WCMS_211661/lang-en/index.htm (accessed May 16, 2013).
- 37.European Campaignon Leadership and Worker Participation. European Union (EU)-Occupational Safety and Health Administration (OSHA); Available at http://www.healthy-workplaces.eu/en/hw2012 (accessed May 16, 2013). [Google Scholar]
- 38.Takal J. Global estimates of traditional occupational risks. Scan. J. Work Environ. Health Suppl. 2005;2005(1):62–67. (). [Google Scholar]
- 39.Michaels D. OSHA Saves Lives and Jobs. United States Department of Labor; Available at http://social.dol.gov/blog/osha-saves-lives-and-jobs/ (accessed June 17, 2013). [Google Scholar]
- 40.Levine D. I., Toffel M. W., Johnson M. S. Randomized government safety inspections reduce worker injuries with no detectable job loss. Science. 336(6083):907–911. doi: 10.1126/science.1215191. Available at http://www.sciencemag.org/content/336/6083/907 (accessed June 17, 2013). [DOI] [PubMed] [Google Scholar]
- 41.Vision Zero in Traffic. Available at http://en.wikipedia.org/wiki/Vision_Zero (accessed May 16, 2013).
- 42.International Labor Organization (ILO) “Promotional Framework on Occupational Safety and Health Convention.” Geneva: ILO, 2006. No C187. Available at http://www.ilo.org/dyn/normlex/en/f?p=NORMLEXPUB:12100:0::NO::P12100_ILO_CODE:C187 (accessed January 20, 2014)