

Abstract
Although lectures are one of the most common methods of knowledge transfer in medicine, their effectiveness has been questioned. Passive formats, lack of relevance and disconnection from the student's needs are some of the arguments supporting this apparent lack of efficacy. However, many authors have suggested that applying adult learning principles (i.e., relevance, congruence with student's needs, interactivity, connection to student's previous knowledge and experience) to this method increases learning by lectures and the effectiveness of lectures. This paper presents recommendations for applying adult learning principles during planning, creation and development of lectures to make them more effective.
Keywords: Active Learning, Adult-Learning, Lectures
INTRODUCTION
For centuries, lectures have been the most frequently used method for delivering knowledge in academic teaching. Lectures are used in a variety of situations for teaching theoretical knowledge in medicine, ranging from classrooms for medical students and residents, to symposia, conferences and congresses for continuing medical education.1 Lectures have many advantages:2,3,4 knowledge can be taught simultaneously to a significant number of students; they are inexpensive (in their most basic form they only require a classroom, seats and an instructor); and they can be adapted to any audience and topic. In the hands of a skilled instructor, lectures allow for the presentation of difficult topics, reduce the ambiguity of controversial topics and can be used to pique students’ interest in the subject matter, as well as offer them the instructor's perspective and experience.
Lectures have proved to be as effective as other teaching methods for delivering knowledge and information.5,6 However, the effectiveness of lectures has been questioned.1,7,8,9 A lecture's passive nature,1 the lack of clear objectives and organized structure, the irrelevance of topics, their disconnection from a student's real-life practice, the lack of articulation between new and previous knowledge and the effort required to maintain attention,10,11 are some of the elements that challenge learning by this method.
Despite these challenges lectures are still among the cornerstones of academic teaching. Many authors have recommended the inclusion of strategies to make them more effective1,6,12,13,14,15,16,17,18,19,20,21,22 – from more active student involvement to variations on the lecture itself. These strategies would allow an evolution from static, passive formats (in which students sit for an hour only to listen to what the instructor has to say) to more dynamic and interactive formats, allowing more student participation and involvement in their own learning. An adequate instructional design for combining texts and images in audio-visual aids would also be necessary to make these more effective for learning.6,11,23,24,25,26,27,28
This article will present a summary of adult learning principles and how they should guide the design, content and format of lectures. Additionally, it will offer recommendations for creating organized, relevant, interactive and effective lectures.
Adult learning principles
Since, Eduard C. Lindeman's pioneer paper in 1926, The Meaning of Adult Education, which awakened interest in and set the basis for the systematic research about how adults learn, educators and psychologists have contributed to the development of many varied theories and hypothesis about the learning characteristics of adults. Taylor and Hamdy summarized the learning theories and classified them in the following categories:29
-
Instrumental learning theories - these focus on the learner's individual experience
- Behavioural learning theories - Stimuli in the environment can produce changes in behaviour
- Cognitive learning theories - Learning is focused on mental and psychological processes, perception and processing of information not in behaviour
- Experiential learning - Learning is focused on the development of competencies and skills in a specific context
-
Humanistic theories - Centered on the learner, these theories focus on an individual's potential for self-actualization, self-direction and internal motivation
- Andragogy - The explanation of adults’ motivation and disposition to learning.
- Self-directed learning - The suggestion that students can plan, conduct and assess their own learning30
Transformative learning theory - Explores how critical reflection can be used to challenge a learner's beliefs and assumptions
Social theories of learning - These require the “two crucial” elements of context and community. They include cognitive situated theories that consider learning and thinking as social activities taking place in a community and influenced by context3
Motivational models - These emphasize the value of internal motivation and reflection as necessary for learning
Reflective models - These hold that reflection lends to change. Reflective learning31 and deliberate practice32,33 theories are examples of these models.
As shown by this classification, the theories are numerous. Elements from all of them may be applied to explain how adults learn; although none of them is complete on its own (all of them have limitations).29,30,34
Below we provide some examples on how these theories apply to the preparation and development of lectures.
Andragogy
In the 1970s, Malcolm S. Knowles developed a model to explain the characteristics of learning in adults based in the following assumptions:4,35
The need to learn
Adults need to know why they need to learn something before undertaking to learn it. They need to know how learning will be conducted, what learning will occur and why learning is important. The pedagogical implications of this assumption are that:
It is important to know and understand the learner's expectations and needs through needs assessments (an evaluation of what the learner needs to know about the subject matter, performed prior to the teaching intervention by asking teachers and/or students). These allow for appropriate planning, in order to avoid the mistake of teaching content so basic that students already know it (the lecture is viewed as a waste of time) or so difficult that they find it impossible to understand (they lack the knowledge base to understand the content) or they find it irrelevant to their needs
It is fundamental to introduce goals and objectives at the beginning of the lecture - what learners will be able to know or do with the knowledge acquired during the lecture
It is good practice to present an outline at the beginning of the lecture to give the learners a preview of what they will learn.
The learner's self-concept
Adults have the self-concept of being responsible of their own decisions and their own lives and consequently need to be considered by others as capable of self-direction. Teachers should help their adult students become self-directed learners: Learners that are able to control, motivate, supervise and adjust their own learning.36 Encouraging active learning (where students actively participate in their learning – through debates, questioning, case resolution) over passive learning (where students just sit back and expect to be ‘fed’ by the teacher) is one strategy for helping students make a transition from dependent to self-directed learners.
The role of learner's experiences
Adults come to learning situations with accumulated experience; therefore, in any group of adults there is a wide range of individual differences regarding background, learning styles, motivation, needs, interests and goals. Also, adults tend to develop mental habits, biases and assumptions that usually make them resistant to new ideas and alternative methods of learning.
This concept suggests the inclusion of techniques that take into consideration the learner's’ experience. Group discussions, debates, case-based methods, etc., are examples of techniques in which students may evaluate, reflect and review their own experience in light of what is being taught. Additionally, constructivist learning theories suggest that new information must connect to previous knowledge in order to be understood, retained and then utilized.37
Readiness to learn
Adults are ready to learn what they need to know to cope with the situations they face in their real lives. This principle supports the relationship between the content to be taught and the learner's developmental stage. For example, a lecture about phacoemulsification with premium intraocular lenses might not be relevant for first-year residents, although it would be useful for third-year residents.
Orientation to learning
Adults will be motivated to learn as long as they perceive the learning as useful to help them perform tasks or solve problems they face in their lives. They will learn more effectively when new knowledge, skills, attitudes and values are presented in the context of their application to real life situations.
This concept implies that the content of lectures should be relevant to what learners need to cope with in their daily practice. The instructor's experience on the subject matter (presented through personal stories or cases) adds to the relevance that the audience may find in the content.
Motivation
Although adults respond to external motivators (better jobs, promotions, higher salaries, etc.) the most powerful motivators for learning are internal pressures (the desire for increased job satisfaction, self-esteem, quality of life, etc.).
Letting learners know why they need to know a topic or what they will be able to do with the knowledge acquired from the lecture (i.e., to present goals and objectives) can increase motivation during lectures, as well as the inclusion of activities, debates and question.37
Active learning
In this teaching model, the learner actively participates in his/her learning.38 Active learning implies that:
Learners are involved in more than listening
Less emphasis is placed on transmitting information and more on developing a student's skills
Learners are involved in higher order thinking (analysis, synthesis and evaluation)
Students are engaged in activities (e.g., reading, discussion and writing)
Greater emphasis is placed on the student's exploration of his/her own values and attitudes.
Strategies promoting active learning include questions and debates, reflective activities and small group discussions, case studies, role-playing and more. Several authors suggest that active learning techniques may have greater effectiveness in medicine and other disciplines.23,39,40,41,42,43,44,45
Experiential learning
This model, developed by David A. Kolb, considers the learning process as a “cycle of experience”, which consists of 4 steps:46
The learner lives a concrete experience
He/she observes and reflects on the experience from different perspectives
He/she forms abstract concepts and generalizations
He/she assesses the implications of the new concepts in new situations.
This model suggests the inclusion of a variety of strategies during lectures, such as simulations, case studies, demonstrations and group discussions. The instructor uses these strategies to help the learner through the different steps of learning from the experience.
This perspective is based on constructivist learning theories, which state that knowledge is linked to the context in which it occurs and that learning occurs from experience according to the personal meaning individuals give to it. The role of teaching is to provide contexts and assistance that helps individuals find meaning in knowledge according to the environment in which they perform.3,47
Reflective learning
Donald A. Schön highlighted the importance of fostering reflection about what happens and why it happens, personal beliefs and feelings, errors, gaps and possible variables, in order to achieve meaningful learning when teaching professionals.31,37,48 Reflection during lectures may be encouraged through dialogues, questions and debates.
Superficial versus deep learning
This concept refers to the preference by which students approach learning. Some prefer a deeper understanding (deep learning); others prefer to acquire only the facts (superficial learning). This preference is usually determined by content, context, needs and previous knowledge of the topic. Students tend to “strategically” choose how they learn topics according to the circumstances.49 Additionally, the evaluation system can condition the learning style. If the evaluation is based on recalling/reciting of facts, students willing to pass will choose a superficial approach. The use of reflection using questions and discussion during lectures promotes a deeper approach to learning.29
The learning process
Taylor and Hamdy propose a 5-stage process to explain how learning occurs:29
Dissonance: The learner's existing knowledge is challenged and found to be incomplete
Refinement: The learner seeks out possible explanations or solutions to a problem (elaboration) and through completing tasks, research, reflection and discussion refines the new information into new concepts
Organization: The learner develops or restructures ideas considering the newly acquired information, making sense of it and organising it into schemata
Feedback: The learner articulates new knowledge and tests it against what his peers and teachers think which reinforces the schema or obliges its reconsideration
Consolidation: New reflection occurs about what was learned and how learning occurred.
Teachers and learners have varied roles according to the stage; providing organizers (objectives, structure), encouraging reflection and giving feedback are key activities that should be integrated into lectures.
In summary, current theories of adult learning emphasize that:
Learners need to have clear goals and objectives of what they will achieve by the teaching intervention (e.g., the lecture)30
Content should be relevant and useful to the learner's real life
Content should be connected to experience and previous knowledge23,43
Learners should reflect about what they learn and how they learn31
Learners should actively participate in their learning23,43,50
Teaching should be learner-centred, i.e., consider theories by which adults learn and implement the most adequate strategies that help them learn, according to their needs, objectives and the context11,12,23,36,50,51
The teacher's role changes from being a “transmitter” of knowledge to a “facilitator”, that assists the students in their own learning, provides relevance to the content, offers examples of application to practice, invites reflection, motivates and helps to provide significant meaning to new knowledge.23,30,50
Recommendations for making lectures more effective
Below we offer some recommendations for making lectures more effective, according to the principles described above and considering three moments: Preparation, delivery and finalization of the lecture.
Preparing the lecture
Preparation is a very important moment - planning what will be said and how. We recommend the following steps:
Perform a needs assessment
It consists of figuring out, reflecting about and considering what the needs of the target audience are. These may be obtained through the use of questionnaires for attendees or by asking the organizer about the audience. Who is the audience? What is their level of knowledge of the subject? How will the lecture be articulated to the rest of the training program? Students may be asked on the day of the lecture and it can be adapted to their responses. This technique requires flexibility and novice speakers may find it difficult and challenging.
Formulate a general goal
This step consists of thinking about the main objective the audience should achieve as a result of the lecture. What do they need to know? For what purpose will they use it? In what context will they use it? A key question for any lecturer to consider is “How can I help my students to learn during my lecture?”52
“Brainstorm”
It consists of thinking and writing down everything that comes to mind on the subject. This process can be performed on a sheet of paper or with mind mapping software. It is important to do it before starting to prepare the slides, as it makes it easier to write, discard, add, delete and get a one-page final document with an outline of the entire lecture.
Structure the lecture
While there are different models of lecture structure,1,2 in general terms lectures can be structured as a “three-act play”:4,11,25 the introduction, the body and the conclusion.
The introduction to the lecture
The lecture's objectives, its importance and an outline of the content are presented here. The introduction is a crucial moment to capture the student's attention.11,43,50,52
Objectives are specific and measurable statements about what the student will be able to do as a consequence of an educational intervention, in this case the lecture. Objectives are a guide that allows learners know what they will be able to do with the knowledge they will acquire in the lecture. They help learners understand the relevance of the lecture and articulate the lecture with their previous knowledge.
Learning objectives should be specific, measurable (observable), achievable, realistic and time-bound. Objectives should be written in terms (verbs) that define what the learner will be able to do and that are easy to understand, evaluate and measure by a third party (i.e., open to few interpretations).11
The importance of the lecture is the basis for the relevance of the topic to the learner's practice and real life. Students will be able to see why they need to have that knowledge. In Ophthalmology this aspect is particularly important when teaching medical students, whose interest in the speciality is variable and for whom the connection with real life is not always evident. A clinical problem or case may also be used here as an introduction, to trigger interest about the lecture's content.53
The outline of the content should be included at the beginning to provide students with a preview or “road map”11 of what the lecture will cover. If the lecture is long or the topic difficult it is advisable to periodically review the outline with the students, to reduce the anxiety about how much content remains to be covered.
The body of the lecture
It is here that the content of the lecture is presented. The body does not need to be exhaustive. It is not necessary to cover everything known about the subject matter. Students will be able to get much of this information in books. Time should be used for introducing what is most important, to explain a topic that is difficult to understand or to update new knowledge about a topic. Learning is greater when less, well explained content is presented, than when lots of concepts are introduced superficially or at a fast pace.
Content should be relevant and useful; therefore, cases, personal experiences or references to the importance and/or usefulness of a topic for practice are recommended.43,50,54,55,56 Learners should be assisted in linking the new knowledge with what they already know through discussions, questions, examples, analogies or metaphors.53
Inclusion of activities such as questions or small group discussions should be planned in advance, in order to allow active participation during the lecture. Since attention capacity decreases after 15-20 minutes,10 and human memory is able to process a limited cognitive load it is advisable to include activities after short intervals, alternating short segments of passive explanation with segments of activity.11 This strategy (called “chunking”) facilitates mental creation of schemata and linking of new and previous knowledge.25,26,43,57
The conclusion of the lecture
Another important moment is when learners get the “take home message”.3 It can take the form of a summary or review of the main points or a reminder of the most important concepts that should not be forgotten. If the lecture belongs to a series, the topic of the next lecture may be introduced here. Bad conclusions are those that are superficial or irrelevant, disconnected from the content or inexistent. It is important to allow some time for questions, clarifications and comments.
Design the slides
A proper slide design, including presentation and combination of texts and images (pictures, graphics, and videos) is almost as important for learning as the content being presented. A lecturer that knows the topic but whose presentations are not adequately designed can confuse or distract the audience and prevent or complicate learning.23,26,58
Some general recommendations for slide design include:
Layouts and backgrounds should be kept clear and simple and overcrowding of slides should be avoided [Figure 1]
When possible, it is advisable to use images (pictures, graphics, video) instead of text, as images are easier to remember11,26 [Figure 2]. The number of bullet points on a slide should be limited. Too much text also distracts from the spoken message, since it is difficult to read, listen and understand at the same time.25 Graphics may have explanatory text close to their components to facilitate understanding11,23 [Figure 3]. Irrelevant images (such as logos, landscapes, cartoons, etc.) can distract, make the information difficult to read and prevent learning25
Background and text colours should be harmonious and carefully chosen.28 Colour may be used to emphasize one or two words and contrasting colours should be used in order to make the slides easier to read27
Presentation of data also requires clear graphics that keep unnecessary information to a minimum11 [Figure 4]. Complex graphics should be explained and progressive introduction of data is advisable when large amounts of data are presented
Fonts should have a resolvable size at distance. As a general rule, slide titles should be in 72 to 40 point font size and the text in the body of the slide should be between 40 and 28 point.28 Fonts those are smaller than 24 are very difficult to see especially in a large lecture hall
All-capital words may be used only for emphasis on one or two words; using all capitals for the whole text makes it difficult to read.
Figure 1.
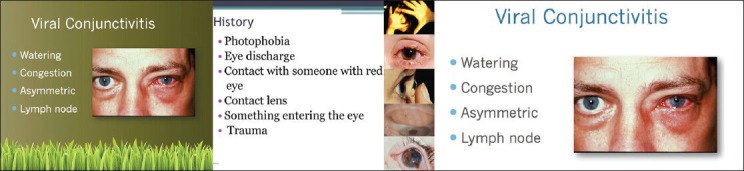
Left: A distractive background. Middle: This slide has too much information. Right: A clear background, an explanatory image and a few words reinforce the speaker's message
Figure 2.
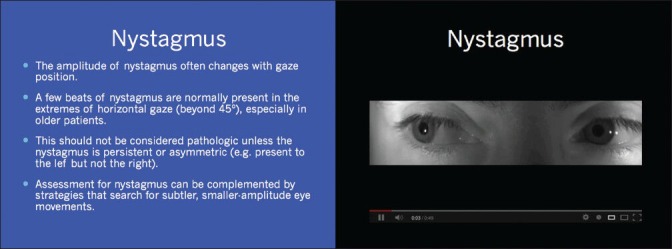
Left: A slide with too much information that could be read in a book. Learning is difficult if attention needs to be simultaneously directed to the speaker and the text. Right: Images (video in this case) are a better strategy for explaining content without overloading memory
Figure 3.
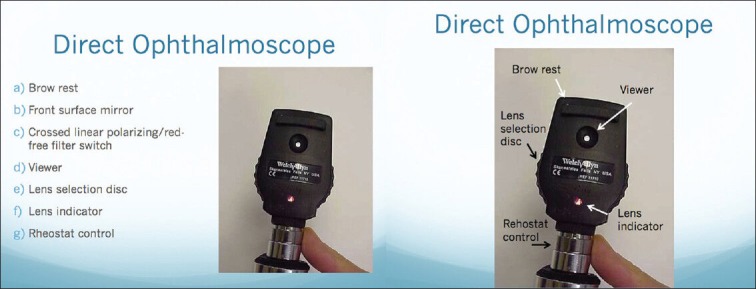
Left: Explanatory text is separated from the image. Right: Explanatory text is close to the parts being explained. This facilitates understanding and learning
Figure 4.
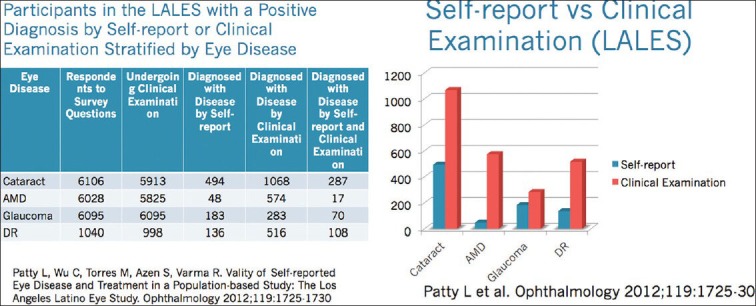
Presenting data in a slide. Left: A slide with too much information, most of it unnecessary for the message being delivered, difficult to follow. Right: Unnecessary data was removed; numbers have been transformed into coloured bars. The visual representation of these data is easier to interpret
Write notes of what you plan to say
When many images and little text are used, writing notes allows mental organization and selection of the right words for what needs to be said. The Notes section of the slide can be used for this purpose.
Rehearse what you plan to say
This step helps to ensure an adequate use of the allotted time and is the key to arrive psychologically prepared to speak to the audience. Practice helps improve fluency, polish verbal tics, mannerisms, stumbles, hesitations and decreases anxiety and “stage fright”.11
Delivering the lecture
Explaining the content
An organized structure as well as clear and interesting explanations, are the key features to increase the effectiveness of the lecture.1,2,54 Brown1 describes four moves in clear explanations: Signposts, frameworks, foci and links. Signposts indicate the structure and direction of an explanation: “Today we will discuss the most frequent causes of acute visual loss, according to their localization: Refractive media, retina and optic nerve”. Frames indicate the beginning and end of a section of the explanation: “We have discussed the retinal causes, now we’ll focus in the optic nerve causes”. Inclusion of summaries or synthesis at the end of each frame is important in difficult or long topics.2 Foci emphasize the key points of an explanation: “Among all the causes, those most important to remember are central artery occlusion and arteritic anterior ischaemic optic neuropathy”. Links are those between topics of the explanation and between the explanation and the learner's knowledge: “You can see how important it is to refer any patient with acute visual loss to the ophthalmologist. As you can imagine, the implications of these diseases are completely different than those of chronic visual loss, as we discussed earlier today”.
It is important to monitor student's reactions and modify explanations accordingly. Repeat what was not understood, rephrase it, explain it with analogies, examples, counter-examples or similes,1,2,6,25,59,60 and stimulate reflection with a question.
Communication skills
Communication skills needed for a lecture vary and a complete analysis is beyond the scope of this article. Generally, we suggest the following:3,4,11,43
Delivery of content includes verbal (what is said), extra-verbal (emphasis, fluency, hesitations, stumbles, rate of speech, pitch, modulation, repetitions, enthusiasm) and non-verbal (eye contact and fixation, body language, proximity, posture, movement, facial expression). Although we will not discuss all of the details of these factors, it is important to emphasize that the clear, enthusiastic, fluid and cheerful professor, who uses an audible tone of voice (without yelling), pauses appropriately (without being slow), alternates eye contact with different members of the audience, repeats what is difficult or important and is approachable,50 is more effective than the one who speaks fast, in a monotonous and almost inaudible tone of voice, immobile behind the podium and looking only at his/her notebook
Use of humour can be beneficial, but it should be done carefully. Humour used appropriately can regain a student's attention or help fixate a concept. Rude, discriminative, difficult to understand or irrelevant humour can offend, distract and predispose the audience against the speaker
It should be remembered that audio-visuals reinforce the message and facilitate learning, but they are not the core of the presentation. The core of the lecture, what students need to learn, is the message the instructor is intending to transmit. Recitation of slides full of written text and bullet points is an inefficient and ineffective teaching strategy. Students would learn the topic more fully by reading about it in a book. What the teacher has to say is important and useful and this is what he/she should transmit with his/her discourse and reinforce with audiovisuals.1,28,58
Strategies for increasing student activity during lectures
There are numerous strategies for making lectures more active in order to keep students’ attention on the topic, engage them and involve them in their own learning.1,43,50,52,55,61,62 Variations of the “Socratic dialogue”, where the instructor questions students and helps them to reflect, discover their knowledge gaps, gain their interest on the subject and provide meaning to the new knowledge, remain among the most widely used.3,13
Several authors have proved that the inclusion of automated response systems (“clickers” technology, online polling software and webinars) can be used to engage the audience and facilitate learning.11,13,23,50,63,64 Software allows creation of different kinds of questions (multiple choice, open ended, short answers) and immediate provision of feedback by the instructor. In our experience the active participation of residents and feedback was favoured by this method.65
A variation of the traditional lecture, Peer Instruction,14,50 consists of interspersing lectures with conceptual questions, designed to expose common difficulties in understanding the material. Students have to think and formulate their own answers; they then discuss in groups of three to four, attempting to reach consensus on the correct answer. This process forces students to think through the arguments being developed and enables them (as well as the instructor) to assess their understanding of the concepts.
Another possibility is to alternate short segments of lectures with small group discussions and tasks (e.g., “buzz groups”, brainstorming).1 These formats that allow a greater active participation of learners have proven to be equally or more effective than the traditional lecture format.15,16,17,19
Finishing the lecture
At the end of the lecture handouts are distributed (some instructors do this at the beginning, although this is generally not recommended because it may distract the students).8,50,56 If possible, handouts should be documents that students may use later on the job (such as conceptual maps, algorithms, tables), instead of a printout of the slides. However, a reduced version of these can be useful for students to take notes.2
It is also important to evaluate the lecture, not only through student satisfaction surveys but also ideally by peer reviews,1,52,66 and then consider what needs to be changed in the future.2,50,62,67
CONCLUSION
Lectures are one of the most frequently used methods for teaching medical knowledge. Adult learning principles that emphasize the relevance and usefulness of the contents, include active and reflective strategies and connect to experience and previous knowledge should be considered to create a meaningful whole. Additionally, instructional design principles for the planning, preparation and delivery of lectures can transform the lecture into a useful, effective, significant and memorable learning experience.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Brown G, Manogue M. AMEE Medical Education Guide No. 22: Refreshing lecturing: A guide for lecturers. Med Teach. 2001;23:231–44. doi: 10.1080/01421590120043000. [DOI] [PubMed] [Google Scholar]
- 2.Brown G, Edmunds S. Lectures. In: Dent JA, Harden RM, editors. A Practical Guide for Medical Teachers. 3rd ed. Elsevier; 2009. pp. 73–9. [Google Scholar]
- 3.Davis M, Forrest K. Oxford: Wiley-Blackwell and BMJ Books; 2008. How to teach Continuing Medical Education; pp. 41–59. [Google Scholar]
- 4.Bullock I, Davis M, Lockey A, Mackway-Jones K, editors. Pocket Guide to Teaching for Medical Instructors. 2nd ed. Blackwell and BMJ Books; 2008. Advanced Life Support Group and Resuscitation Council (UK) [Google Scholar]
- 5.Bligh DA. San Francisco (CA): Jossey-Bass; 2000. What's the use of lectures? [Google Scholar]
- 6.Clark RC. American Society for Training and Development; 2010. Evidence-based training methods: A guide for training professionals. [Google Scholar]
- 7.Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance. JAMA. 1995;274:700–5. doi: 10.1001/jama.274.9.700. [DOI] [PubMed] [Google Scholar]
- 8.Davis DA, Thomson MA, Oxman AD, Haynes RB. Evidence for the effectiveness of CME: A review of 50 randomized controlled trials. JAMA. 1992;268:1111–6. [PubMed] [Google Scholar]
- 9.Warner S, Williams DE, Lukman R, Powell CC, 2nd, Kundinger K. Classroom lectures do not influence family practice residents’ learning. Acad Med. 1998;73:347–8. doi: 10.1097/00001888-199803000-00029. [DOI] [PubMed] [Google Scholar]
- 10.Stuart J, Rutherford RJ. Medical student concentration during lectures. Lancet. 1978;2:514–6. doi: 10.1016/s0140-6736(78)92233-x. [DOI] [PubMed] [Google Scholar]
- 11.Stahl SM, Davis RL. New York (NY): Cambridge University Press; 2011. Best Practices in Medical Teaching. [Google Scholar]
- 12.Chaudhury SR. The Lecture. In: Buskist W, Groccia JE, editors. Evidence-Based Teaching. San Francisco (CA): Jossey-Bass, Wiley; 2011. [Google Scholar]
- 13.Mayer RE, Stull A, DeLeeuw K, Almeroth K, Bimber B, Chun D, et al. Clickers in the classroom: Fostering learning with questioning methods in large lecture classes. Contemp Educ Psychol. 2009;34:51–7. [Google Scholar]
- 14.Mazur group. Peer Instruction. [Last cited 2013 Oct 15]. Available from: http://mazur.harvard.edu/research/detailspage.php?rowid=8 .
- 15.Fagen AP, Crouch CH, Mazur E. Peer Instruction: Results from a range of classrooms. Phys Teach. 2002;40:206–9. [Google Scholar]
- 16.Udovic D, Morris D, Dickman A, Postlethwait J, Wetherwax P. Workshop Biology: Demonstrating the effectiveness of active learning in an introductory Biology course. Bioscience. 2002;52:272–81. [Google Scholar]
- 17.Knight JK, Wood WB. Teaching more by lecturing less. Cell Biol Educ. 2005;4:298–310. doi: 10.1187/05-06-0082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Johnson SA, Romanello ML. Generational diversity. Teaching and learning approaches. Nurs Educ. 2005;30:212–6. doi: 10.1097/00006223-200509000-00009. [DOI] [PubMed] [Google Scholar]
- 19.Beichner RJ, Saul JM, Abbott DS, Morse JJ, Deardorff DL, Allain RJ, et al. The Student-Centered Activities for Large Enrollment Undergraduate Programs (SCALE-UP) Project. In: Redish E, Cooney P, editors. Reserach-Based Reform of University Physics. College Park (MD): American Association of Physics Teachers; 2007. [Last cited 2013 Oct 16]. pp. 1–42. Available from: http://www.per-central.org/document/ServeFile.cfm?ID=4517andDocID=183 . [Google Scholar]
- 20.Mangold K. Educating a new generation. Teaching baby boomer faculty about Millennial students. Nurs Educ. 2007;32:21–3. doi: 10.1097/00006223-200701000-00007. [DOI] [PubMed] [Google Scholar]
- 21.Gibson SE. Intergenerational communication in the classroom: Recommendations for successful teacher-student relationships. Nurs Educ Perspect. 2009;30:37–9. [PubMed] [Google Scholar]
- 22.Paterson T. General considerations in providing critical care education. Crit Care Nurs Q. 2010;33:67–74. doi: 10.1097/CNQ.0b013e3181c8dfa8. [DOI] [PubMed] [Google Scholar]
- 23.Bransford JD, Brown AL, Cocking RR, editors. How people learn. Brain, mind, experience and school. Expanded edition. Washington, D.C: National Academy Press; 2000. Committee on Developments in the Science of Learning. [Google Scholar]
- 24.Clark RC, Mayer RE. San Francisco (CA): Pfeiffer; 2003. e-learning and the science of instruction. [Google Scholar]
- 25.Clark R, Nguyen F, Sweller J. San Francisco (CA): Pfeiffer; 2006. Efficiency in learning. Evidence-based Guidelines to Manage Cognitive Load. [Google Scholar]
- 26.Cook MP. Visual representations in Science education: The influence of prior knowledge and cognitive load theory on instructional design principles. Sci Educ. 2006;90:1073–91. [Google Scholar]
- 27.Reynolds G. Berkeley (CA): New Riders; 2010. Presentation Zen design. Simple design principles and techniques to enhance your presentations. [Google Scholar]
- 28.Duarte N. Sebastopol (CA): O’Reilly; 2011. Slide: ology. The art and science of creating great presentations. [Google Scholar]
- 29.Taylor DC, Hamdy H. Adult learning theories: Implications for learning and teaching in medical education: AMEE Guide No. 83. [Last cited 2013 Oct 14];Med Teach. 2013 35:e1561–72. doi: 10.3109/0142159X.2013.828153. Available from: http://informahealthcare.com/doi/pdf/10.3109/0142159X.2013.828153 . [DOI] [PubMed] [Google Scholar]
- 30.Arogundade RA. Adult learning principles for effective teaching in Radiology programmes: A review of the literature. West Afr J Med. 2011;30:3–10. doi: 10.4314/wajm.v30i1.69876. [DOI] [PubMed] [Google Scholar]
- 31.Schön DA. 1st ed. San Francisco (CA): Jossey-Bass; 1987. Educating the reflective practitioner; pp. 3–22. [Google Scholar]
- 32.Ericsson KA, Krampe RT, Tesch-Römer C. The role of deliberate practice in the acquisition of expert performance. Psychol Rev. 1993;100:363–406. [Google Scholar]
- 33.Ericsson KA. Deliberate practice and the acquisition and maintenance of expert performance in Medicine and related domains. Acad Med. 2004;79:S70–81. doi: 10.1097/00001888-200410001-00022. [DOI] [PubMed] [Google Scholar]
- 34.Stagnaro-Green A. Applying adult learning principles to medical education in the United States. Med Teach. 2004;26:79–85. doi: 10.1080/01421590310001642957. [DOI] [PubMed] [Google Scholar]
- 35.Knowles MS, Holton RA, 3rd, Swanson RA. 7th ed. Burlington (MA): Elsevier; 2011. The Adult Learner; pp. 64–69. (183-203). [Google Scholar]
- 36.Roberts TV, Gustavs J, Mack HG. Becoming an expert: A review of adult learning theory and implications for Vocational Training in Ophthalmology. Clin Experiment Ophthalmol. 2012;40:519–26. doi: 10.1111/j.1442-9071.2011.02716.x. [DOI] [PubMed] [Google Scholar]
- 37.Norman GR, Schmidt HG. The psychological basis of problem-based learning: A review of the evidence. Acad Med. 1992;67:557–65. doi: 10.1097/00001888-199209000-00002. [DOI] [PubMed] [Google Scholar]
- 38.Bonwell CC, Eison JA. Washington DC: Jossey-Bass; 1991. Active Learning: Creating Excitement in the Classroom (J-B ASHE Higher Education Report Series AEHE) pp. 1–4. [Google Scholar]
- 39.Hake RR. Interactive-engagement versus traditional methods: A six-thousand-student survey of mechanics test data for introductory physics course. Am J Phys. 1998;66:64–74. [Google Scholar]
- 40.Prince M. Does active learning work? A review of the research. J Eng Educ. 2004;93:223–31. [Google Scholar]
- 41.Michael J. Where's the evidence that active learning works? Adv Physiol Educ. 2006;30:159–67. doi: 10.1152/advan.00053.2006. [DOI] [PubMed] [Google Scholar]
- 42.Frohna AZ, Hamstra SJ, Mullan PB, Gruppen LD. Teaching medical education principles and methods to faculty using an active learning approach: The University of Michigan Medical Education Scholars Program. Acad Med. 2006;81:975–8. doi: 10.1097/01.ACM.0000242573.71314.74. [DOI] [PubMed] [Google Scholar]
- 43.Barkley EF. 1st ed. San Francisco (CA): Jossey-Bass; 2010. Student engagement techniques. A handbook for college faculty. [Google Scholar]
- 44.Hoellwarth C, Moelter MJ. The implications of a robust curriculum in introductory mechanics. Am J Phys. 2011;79:540–5. [Google Scholar]
- 45.President's Council of Advisors on Science and Technology. Engage to Excel: Producing one million additional college graduates with degrees in Science, Technology, Engineering and Mathematics. 2012. [Last cited 2013 Oct 10]. Available from http://www.whitehouse.gov/sites/default/files/microsites/ostp/pcast-engage-to-excel-final_feb.pdf .
- 46.Kolb DA. 1st ed. Upper Saddle River (NJ): Prentice Hall; 1983. Experiential learning: Experience as the source of learning and development; pp. 20–38. [Google Scholar]
- 47.Duffy TM, Jonassen TH. Hillsdale (NJ): Lawrence Elbaum Associates; 1992. Constructivism and the technology of instruction: A conversation. [Google Scholar]
- 48.Schön DA. The reflective practitioners. How professionals think in action. Basic Books. 1983 [Google Scholar]
- 49.Trigwell K, Prosser M, Waterhouse F. Relations between teachers’ approaches to teaching and students’ approaches to teaching. High Educ. 1999;37:57–70. [Google Scholar]
- 50.Harden RM, Laidlaw SL. Elsevier, Churchill Livingstone; 2012. Essential skills for a medical teacher. An introduction to teaching and learning in medicine. [Google Scholar]
- 51.Harden RM, Crosby J. AMEE Guide No 20: The good teacher is more than a lecturer-the twelve roles of the teacher. Med Teach. 2000;22:334–47. [Google Scholar]
- 52.Cantillon P. Teaching large groups. BMJ. 2003;326:437–40. doi: 10.1136/bmj.326.7386.437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Herreid CF. Case Study Teaching. In: Buskist W, Groccia JE, editors. Evidence-Based Teaching. San Francisco (CA): Wiley, Jossey-Bass; 2011. [Google Scholar]
- 54.Copeland HL, Longworth DL, Hewson MG, Stoller JK. Successful lecturing. A prospective study to validate attributes of the effective medical lecture. J Gen Intern Med. 2000;15:366–71. doi: 10.1046/j.1525-1497.2000.06439.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Fyrenius A, Bergdahl B, Silén C. Lectures in problem-based learning-Why, when and how? An example of interactive lecturing that stimulates meaningful learning. Med Teach. 2005;27:61–5. doi: 10.1080/01421590400016365. [DOI] [PubMed] [Google Scholar]
- 56.Bowen JL. Educational strategies to promote clinical diagnostic reasoning. N Engl J Med. 2006;355:2217–25. doi: 10.1056/NEJMra054782. [DOI] [PubMed] [Google Scholar]
- 57.Smith MR. 1st ed. San Francisco (CA): Jossey-Bass; 2008. Conquering the content. A step-by-step guide to online course design; pp. 66–81. [Google Scholar]
- 58.Harden RM. Death by PowerPoint-the need for a ‘fidget index’. Med Teach. 2008;30:833–5. doi: 10.1080/01421590802307743. [DOI] [PubMed] [Google Scholar]
- 59.Clark RC. 3rd ed, 1st ed. San Francisco (CA): Pfeiffer; 2008. Developing technical training. A structured approach for developing classroom and computer-based instructional materials; pp. 55–180. [Google Scholar]
- 60.Ventura S, Onsman A. The use of popular movies during lectures to aid the teaching and learning of undergraduate pharmacology. Med Teach. 2009;31:662–4. doi: 10.1080/01421590802641489. [DOI] [PubMed] [Google Scholar]
- 61.Gülpinar MA, Yegen BC. Interactive lecturing for meaningful learning in large groups. Med Teach. 2005;27:590–4. doi: 10.1080/01421590500136139. [DOI] [PubMed] [Google Scholar]
- 62.Visioli S, Lodi G, Carrassi A, Zannini L. The role of observational research in improving faculty lecturing skills: A qualitative study in an Italian dental school. Med Teach. 2009;31:e362–9. doi: 10.1080/01421590902744860. [DOI] [PubMed] [Google Scholar]
- 63.Masikunis G, Panayiotidis A, Burke L. Changing the nature of lectures using a personal response system. Innov Educ Teach Int. 2009;46:199–212. [Google Scholar]
- 64.Nelson C, Hartling L, Campbell S, Oswald AE. The effects of audience response systems on learning outcomes in health professions education. A BEME systematic review: BEME Guide No. 21. Med Teach. 2012;34:e386–405. doi: 10.3109/0142159X.2012.680938. [DOI] [PubMed] [Google Scholar]
- 65.Mayorga Argañaraz EP, Bekerman JG, Palis AG. Rio de Janeiro, Brazil: Paper presented at: XXX Pan-American Congress of Ophthalmology; 2013. Aug 7-11, Using online seminars (webinars) to improve residents’ learning. [Google Scholar]
- 66.Siddiqui ZS, Jonas-Dwyer D, Carr SE. Twelve tips for peer observation of teaching. Med Teach. 2007;29:297–300. doi: 10.1080/01421590701291451. [DOI] [PubMed] [Google Scholar]
- 67.McLeod P, Steinert Y, Capek R, Chalk C, Brawer J, Ruhe V, et al. Peer review: An effective approach to cultivating lecturing virtuosity. Med Teach. 2013;35:e1046–51. doi: 10.3109/0142159X.2012.733460. [DOI] [PubMed] [Google Scholar]