

Abstract
Continuing professional development (CPD) involves not only educational activities to enhance medical competence in medical knowledge and skills, but also in management, team building, professionalism, interpersonal communication, technology, teaching, and accountability. This paper aims at reviewing best practices to promote effective CPD. Principles and guidelines, as already defined by some professional societies and world organizations, are emphasized as core actions to best enhance an effective lifelong learning after residency. The personal learning plan (PLP) is discussed as the core of a well-structured CPD and we describe how it should be created. Fundamental CPD principles and how they are integrated in the framework of every physician's professional life will be described. The value of systematic and comprehensive CPD documentation and assessment is emphasized. Accreditation requirements and professional relationships with commercial sponsors are discussed.
Keywords: Accreditation, Appraisal, Continuing Professional Development Clinical Audit, Continuing Medical Education, Personal Learning Plan, Portfolio, Revalidation
INTRODUCTION
The first reported continuing medical education (CME) course took place in 1935; however, only in the 1960s did CME start to be discussed as a coherent body of literature.1 This paper reviews best practices of effective continuing professional development (CPD). CPD's complexity, relevance, guidelines, and principles and managing a CPD program will be discussed. The four-step CPD cycle is discussed in the context of three professional behaviors for which doctors and CPD providers have specific roles and needs.
DEFINITION
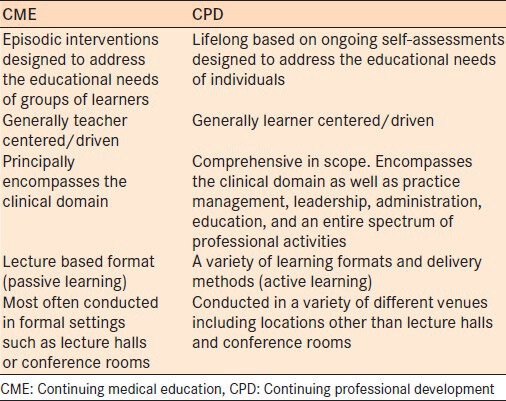
CME's concept generally refers to expanding medical knowledge, skills, and attitudes.2 CPD incorporates and exceeds this concept by acknowledging a wide range of competencies needed to practice high quality medicine, including medical, managerial, ethical, social, and personal skills [Table 1].3,4,5 Grounded on the well-developed tradition of lifelong learning in medical profession, CPD integrates every physician's ethical responsibility and increases job satisfaction.6,7,8
Table 1.
CME and CPD contrasts
A variety of CPD definitions have been given:
“A continuing process, outside formal undergraduate and postgraduate training, that allows individual doctors to maintain and improve standards of medical practice through the development of knowledge, skills, attitudes, and behavior. CPD should also support specific changes in practice.”9
“The wide-ranging competencies beyond clinical update, research and scientific writing, multidisciplinary context of patient care, ethical practice, communication, management and behavioral skills, team building, information technology, audit, and appropriate attitudinal change to ensure improved patient outcomes and satisfaction.”10
“A range of learning activities through which health professionals maintain and develop throughout their careers to ensure that they retain their capacity to practice safely, effectively, and legally within their evolving scope of practice.”11
Each definition shares the broader perspective of CPD, that it:
Is self-driven and individually tailored according to needs assessment
Considers the doctor's complex working environment as a “…multidisciplinary context of patient care”.10 Four broad groups are summarized in the Basel Declaration of European Union of Medical Specialists (UEMS): The individual/society; healthcare professionals; health employers; and healthcare fund raisers12
Is an ongoing learning process building on initial education to ensure competence regarding current and future work duties
Goes beyond the traditional designation for doctor's CME after residency training, a narrower concept, usually only including medical knowledge and skill
Expands content from clinical to holistic topics such as interpersonal communication skills, ethics, practice management, professionalism, and extends learning venues from the classical conference room to practice settings13,14
-
Embraces new educational domains set by professional societies:
- The Royal College of Physicians and Surgeons of Canada's seven key benchmark competencies (CanMeds): Medical expert/clinical, collaborator/manager, health advocate, scholar, professional, decision maker, and communicator15
- The Medical Council of New Zealand's domains for recertification and CPD: Medical care, communication, collaboration and management, scholarship, and professionalism16
- The American Board of Medical Specialities evaluation domains: Bedside manner, medical knowledge, interpersonal and communication skills, professionalism, system-based practical clinical work, learning, and development efforts17
- The United Kingdom's General Medical Council's domains: Knowledge, skills and performance; safety and quality; communication, partnership and teamwork; and maintaining trust18
- The Royal Australian New Zealand College of Ophthalmology's framework learning categories: Clinical expertise, risk management and clinical governance, and professional values19
Is a “self-evaluation model reporting form” necessarily including an evaluation component10
Should produce behavioral change in medical practice so that healthcare improvement is achieved and measurable13
Involves legal aspects such as avoiding lawsuits and practicing under compulsory relicensure1
Promotes the physician's accountability.20
RELEVANCE
Emphasis on CPD has been growing due to several factors:
Physicians are leading longer professional lives
Globally increasing mobility of both patients and healthcare professionals21,22
Accelerated proliferation of new knowledge, new technology, and techniques
Society's increased expectations of the medical profession
Public healthcare systems concerns
Complex healthcare working environments where doctors are constantly challenged to develop and master multidisciplinary teamwork among peers, allied healthcare personnel, employers, regulators, and healthcare systems authorities
Increasing requirements of CPD activities’ measure of performance.
Despite the increased emphasis on CPD, a variety of barriers must be overcome:
Physician's work overload and less time allocated to learn
Underfunding
Improperly defined commercial sponsorships
Noncompliance with best practices to design, develop, implement, and evaluate CPD educational interventions
Biased education and conflicts of interest with sponsors
Lack of clear definition of responsible parties and their specific roles in CPD
Effective assessment of CPD activities to gauge cost-effectiveness
Coordination of all stakeholders
Demonstration of the doctor's CPD to society.23
PRINCIPLES
Given the increased emphasis and barriers described above, it is obvious that CPD must change to be a systematic process that is credible and transparent to the community.1,13 Though medical school and residency training have long been formally regulated, only recently has CPD garnered such attention.24 Additionally, there is wide variability in the approach to CPD globally.25 Despite this, the UEMS promotes free movement of European medical specialists, while trying to ensure healthcare's high quality.26 Therefore in Europe, CPD programs’ harmonization among countries would enhance medical care.21 An effective CPD scheme should have three quality components:24,27,28
Professional improvement that ensures personal learning related to the populations’ changing needs and developing healthcare service
Effective learning interventions should be designed upon clear, attainable, and measurable learning outcomes and offer relevant and evidence-based content to the physician's clinical practice
It must be accountable, transparent, amenable to regulation, and useful for assuring quality in the process of relicensure.
Furthermore, it is essential that skillful CPD management is clearly articulated based on the various CPD stakeholders’ needs.1
Additionally, there must be way for the physician to monitor and report CPD activities.29 Many schemes and recommendations exist as to how best to award credit to CPD programs. These schemes typically have the following key components, which can coexist to a certain extent:
Credit based, where one credit is usually awarded for each hour of educational time spent. A minimum should be achieved over a defined time period30
Document based, where an organized flow of documents help to demonstrate and assess CPD.1
As examples of good CPD practices we suggest the guidelines to administer and manage a CPD program compiled by the International Council of Ophthalmology (ICO). Additionally, the ICO has suggested that ophthalmology societies’ CPD committees should take responsibility for CPD activities. Committees should be responsible for designing, implementing, and evaluating a CPD program according to specific criteria.13
PARTICIPANT PERSPECTIVE
The personal learning plan
Personally designed, CPD reflects adult learning principles of autonomy, self-direction, goal orientation, and practice-based learning.27 PLPs document accomplished educational events, behavior changes in practice, and how career aspirations were enhanced.
The ICO has suggested a question template13 to guide doctors willing to build a PLP as part of their professional development. It is a three-stage stepwise procedure:
Development of the PLP, in which doctors are required to reflect on their learning professional needs
Completion of activities, in which doctors choose activities to meet their professional needs, and
Submission of a report, for which doctors must reflect and write about the effectiveness of their learning.
CPD's practice can be conceptually organized around three fundamental questions: What will I learn? How will I learn? and How well have I learned? These three questions can be thought of in terms of the CPD cycle: (1) Identify what to learn; (2) plan how to learn; (3) learn; and (4) follow-up14 [Figure 1].
Figure 1.
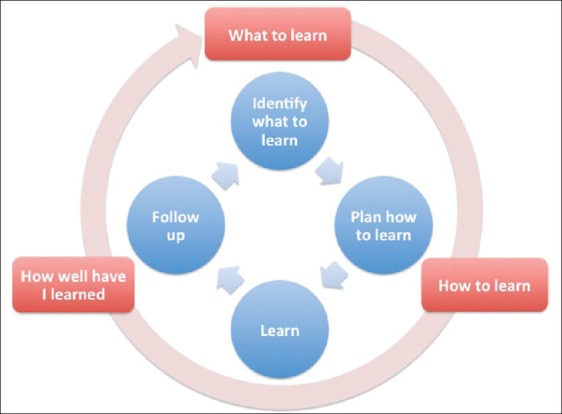
The continuing professional development cycle steps (in blue) and the triggering questions to professional behaviors in practice (in orange)
What will I learn?
A learning need is a gap between current personal competencies/population health status and the desired state. 14 Well-designed educational interventions fill these gaps and remove barriers to change in behavior. Perceived needs may be identified during an appraisal; whereas, unperceived needs may demand direct knowledge testing.1,14 Learning gaps may be identified during direct patient care, in interactions with the clinical team and department, in nonclinical activities (readings, scientific conferences), in quality management and risk assessment (audits, patient satisfaction surveys), in specific needs assessment (self-assessments and revalidation), and in peer review.1
Clinical audit
A clinical audit is a systematic staged cycle of review of one's own patients’ charts and surgical outcomes.31 Audit criteria must be best practice evidence-based and clearly presented before the audit takes place. Recommendations from clinical practice guidelines may be useful to develop criteria and standards. Criteria are explicit statements defining what the outcomes of care will measure. Standards are the threshold of expected compliance for each criterion. Data is collected and results compared to criteria and standards. Change should be implemented by formulating recommendations. Clinical audits are an important component of medical professional accountability and can serve as a method of determining gaps in knowledge.32,33,34,35
How will I learn?
Following a gap's identification, a learning activity should be planned and undertaken–CPD cycle steps 2 and 3 [Figure 1].1,14 Sometimes an educational event is undertaken by doctors not for the sake of advancing factual learning, but for boosting their confidence on a particular topic or skill.1 CPD activities should be chosen according to the type of the identified need whether it be knowledge and skills updating, competency assurance, or performance demonstration in practice.14
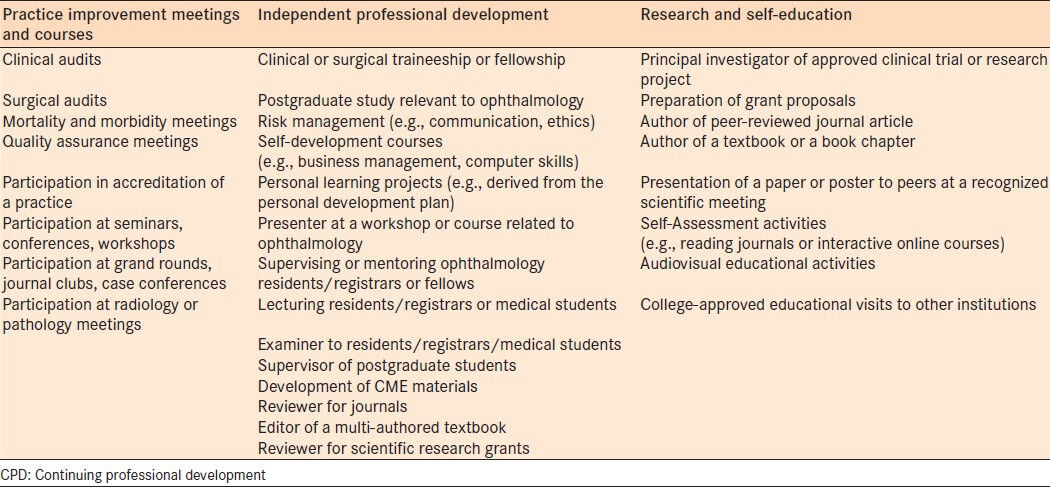
CPD activities can assume a variety of formats characterized as practice improvement, independent professional development, or research/self education. Table 2 presents several examples of educational events according to this categorization.13
Table 2.
CPD activities
A portfolio is a record of what its creator has to offer in terms of range, quality of knowledge, and level of skill attainment.36,37 An e-portfolio documents the individual's professional progression as a web-based collection of artifacts: Reflections, resources, demonstrations, accomplishments, and time periods. e-portfolios encourage exchange of ideas and feedback between owner and those entitled to interact with it, thus offering meaningful learning experiences.38,39
How well have I learned?
Assessment closes the CPD cycle and involves two components:1
Reinforcement or finding opportunities in clinical practice to apply new knowledge and skills
Dissemination of new learning to colleagues at practice settings (e.g., rounds, clinical meetings, and unplanned moments during clinical practice).
Portfolios as portable collection of artifacts can also be valuable assessment tools amenable to appraisal discussions, peer-review, and revalidation.39 Within their regulator function, societies and colleges are encouraged to establish CPD guidelines and provide their members a PLP and a clinical audit template to include in their personal portfolio. This material can be available online and should ideally include the designation and description of the chosen learning activity, planned date to undertake the activity and completion date, CPD points awarded, personal reflection about learning goals fulfillment, effective learning achieved, and its impact in practice.13 Medical teaching organizations are increasingly adopting their own e-portfolio systems such as the free user-friendly online portfolio of the British Medical Journal.40
PROVIDER PERSPECTIVE
Methods and tools
CME has traditionally been concerned with disseminating information, but CPD has shifted the emphasis to demonstrating change in behavior in clinical practice.1,14 Adults participate in educational events when motivated by the identification of a specific learning need and a pragmatic desire to apply knowledge and skills gained.27,41 Unplanned learning that occurs in daily workplace cannot be disregarded and is usually reinforced and disseminated.1 CPD providers must design educational interventions to meet identified gaps considering the participants prior knowledge. Learning objectives must be designed from the learner's perspective and clearly map the content in terms of expected outcomes. Well-written learning objectives will suggest the best CPD delivery method and format concerning the educational event's goal: Knowledge updating, competency development, or performance demonstration. Consideration of the size and the type of the audience (e.g., generalists versus subspecialists) may also dictate appropriate methods.
Regardless of the selected delivery method or format, interactive practice-based learning formats are the most successful.14,42,43 Incorporating at least 25% of interactivity into a learning intervention; such as a lecture by ensuring time and opportunity for questions and discussion, shifts the educational focus from passive teaching to active learning.44
Time and space boundless and web-based CPD events are now being widely used in medical education incorporating even remote communities. If tutor-led and interactivity opportunities are provided, passive learning situations will be avoided. Social media (social networks, wikis, blogs, virtual worlds, and simulations) is being increasingly considered by educators/organizations for its potential in medical education. The medical community is changing from having conservative and reluctant stand on this issue to embracing and leveraging these tools into formal education. Online tools improve research efficiency and social media enhances professional networking.45,46,47,48
Accreditation
CPD must be amenable to external evaluation to become transparent, demonstrable, and accountable.1,13,14 If consistently planned, undertaken, and recorded; CPD can be assessed. Ideally always as a self-assessment including regular discussions with peers or a formal examination. More than a process to meet accreditation requirements or to be credit awarded, assessment should be envisioned as a higher value to bring effectiveness to learning.49 A set of international standards was defined by World Federation of Medical Education to work as a global tool for quality assurance and development of CPD.24
Measuring CPD activities’ effectiveness is crucial and should start during the CPD program, but ultimately to include effects on population health status. These assessments can be used to justify cost effectiveness of educational events’ outcomes.10 CPD program's assessment should provide information on whether:
Target audience needs were addressed
Learning objectives were met
Participants were engaged
Behavior changes were achieved.
Based on business and industry widespread Kirkpatrick's evaluation model, Dixon has defined four CME levels of evaluation that should match teaching strategies and learning event outcomes:
Perception and satisfaction
Competencies
Professional performance
Healthcare outcome.50
Two more levels were later added:
Participation related to an educational event's attendance
Return of investment related to cost-effectiveness.14
There are a variety of ways to perform the evaluation. Clinical audits suit patient outcomes assessment; whereas, CPD credit accumulation, learning portfolios, criterion reference methods, computer diaries, peer review, and chart audits can be used for performance evaluation. Grant describes an exhaustive list of different assessment methods according to the evaluation object.1 Davis contrasts a list of assessment tools to factors affecting their choice as cost, validity, reliability, acceptability, and feedback opportunity.14
Several professional societies and world organizations and colleges51,52,53,54,55,56,57,58,59,60 provide accreditation guidelines including:
Online standard documentation templates and application forms, available in a transparent and practical presentation for all interested
-
Accreditation criteria for providers including:
- Goals and learning objectives clearly built on an identified learning gap
- Content/format delivery in accordance with the goal of the educational event
- Assessment type in accordance with the preestablished learning objectives
- Assessment type and results shared with the participants
- Assessment results made available for future CPD program improvement
- Clear guidelines to avoid commercial sponsorship conflict.
The growth of e-learning CPD has led to accreditation criteria for this format. The European Accreditation Council of Continuing Medical Education (EACCME) has established criteria to ensure e-learning interventions’ accreditation.61 The same goal was pursued by the e-CPD Task Force of the Royal College.62 These criteria add items specific to e-learning such as:
Confirm privacy and confidentiality of the learner
State revision of content and expiry date
Content must be evidence based
Follow adult learning principles such as problem-based learning, reflective learning, and task-based learning
Content delivery must comply with multimedia principles
Should have engaging strategies promoting interaction and meaningful learning
Provide feedback of learning.
Sponsor relationships
Minimizing potential conflict of interest from sponsors is imperative. To gain approval for industry sponsorship the CPD provider should make an application to the ophthalmology society's CME committee and follow criteria.63,64 The Canadian Medical Association Policy indicates that: “Organizations providing financial support to accredited CPD events cannot have any role or influence over any aspect of the CPD planning process. Physician's organizations that receive ‘educational grants’ should provide a statement of account to each sponsoring organization for how funding was allocated or spent”.65 The Royal College Approval of Accredited Group Activities Application Form contains items related to fiscal matters and requires a declaration of conflict of interest. A letter should be sent to the sponsor(s) indicating that funds will be received as an educational grant.66 Speakers may verbally disclose any conflicts of interest or provide written documentation in the event's brochure.
In General, CPD providers should be made solely responsible for designing, implementing, and assessing the educational intervention. The sponsorship and its terms must be communicated to the local/national professional society/healthcare authority. Content should be unbiased, commercial sponsorship acknowledged, and speakers’ conflict of interest disclosed.
CPD sponsorship guidelines should enforce the physician's understanding that they must:
Keep their primary obligation to their patients and duties to society
Ensure an unbiased participation in collaborative efforts between their interaction and pharmaceutical companies (health supplies, research, and education)
Avoid/manage situations with conflict of interest
Promote clear physician-developed guidelines for interaction of physician-industry.
CONCLUSIONS
CME is a lifelong learning process pursued by doctors from medical school until retirement, and has traditionally been viewed in terms of knowledge updating.
CPD demands professional skills that extend beyond medical knowledge such as management, education and training, information technology, audit, communication, and team building. There is great variability in how CPD is being conducted globally. We believe that whether a legal obligation or an unregulated voluntary option, all physicians should undertake some form of CPD. Coordination and harmonization of CPD management will bring efficiency to the process and overcome barriers discussed.
Though customization is needed according to local needs, there are universal guidelines and principles to develop and maintain CPD complying to best practices. Societies and colleges should accept responsibility for both CME and CPD of doctors, establish effective CPD schemes and develop strategies to meet the needs of doctors, the populations they serve, and the organizations where they work.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Grant J. 2nd ed. London: New York Radcliffe Publishing; 2012. The good CPD guide. A practical guide to managed continuing professional development in medicine. [DOI] [PubMed] [Google Scholar]
- 2.What is CME? UEMS page. [Last accessed 2013 Nov 02]. Available from: http://www.uems.net/index.php?id=63 .
- 3.What is CPD? UEMS page. [last accessed 2013 Nov 02]. Available from: http://www.uems.net/index.php?id=64 .
- 4.Chan KW. Contrasting CME and CPD. Medical education: From continuing medical education to continuing professional development. Asia Pac Fam Med. 2002:88–90. [Google Scholar]
- 5.Linos D. The American Model in CME: Lessons to Learn. [Last accessed 2013 Nov 02]. Available from: http://www.aemh.org/pdf/Linos.pdf .
- 6.Brussels: UEMS; 2001. [Last accessed 2013 Nov 02]. Union Européene des Médecins Spécialistes. Basel Declaration – UEMS Policy on Continuing Professional Development. Available from: www.uems.net/http://admin.uems.net/uploadedfiles/35.pdf . [Google Scholar]
- 7.Hojat M, Kowitt B, Doria C, Gonnella JS. Career satisfaction and professional accomplishments. Med Educ. 2010;44:969–76. doi: 10.1111/j.1365-2923.2010.03735.x. [DOI] [PubMed] [Google Scholar]
- 8.Veloski JJ, Hojat M. Measuring specific elements of professionalism: Empathy, teamwork, and lifelong learning. In: Stern DT, editor. Measuring Medical Professionalism. 1 ed. Chapter 7. New York: Oxford University Press; 2006. [Google Scholar]
- 9.Academy of Royal Medical Colleges., Ten Principles for CPD. 1999. [Last accessed 2012 Nov 02]. Available from: http://www.rcgp.org.uk/revalidation-and-cpd/~/media/Files/Revalidation-and-CPD/ACADEMY-GUIDANCE-CPD-HEADINGS.ashx .
- 10.World Health Organization; 2010. [Last accessed 2013 Nov 02]. Regional Guidelines for Continuing Medical Education (CME)/Continuing Professional Development (CPD) Activities. Available from: https://www.wbginvestmentclimate.org/toolkits/health-in-africa-policy-toolkit/upload/WHO-CME-Requirements.pdf . [Google Scholar]
- 11.Continuing professional development and your registration. Health and care professions council. Information for registrands. [Last accessed 2013 Nov 02]. Available from: http://www.hpc-uk.org/assets/documents/10001314CPD_and_your_registration.pdf .
- 12.Basel Declaration. UEMS Policy on Continuing Professional Development. 2001. [Last accessed 2013 Nov 02]. Available from: http://www.uems.net/fileadmin/user_upload/uems_documents/old_website_documents/35.pdf .
- 13.Zagorski Z, Tso MOM. Klin Monatsbl Augenheilkd. Suppl 7. Vol. 223. New York: Georg Thieme Verlag, KG Stuttgart; 2006. [Last accessed 2013 Nov 02]. Principles and Guidelines of a Curriculum for Continuing Medical Education in Ophthalmology. Presented by International Task Force on Continuing Medical Education (CME) in Ophthalmology. On Behalf of The International Council of Ophthalmology (ICO) p. S3±S23. Vol. 223. S1–S23/2006. Available from: http://www.icoph.org/resources/33/Principles-and-Guidelines-of-a-Curriculum-for-Continuing-Medical-Education-in-Ophthalmology.html . [Google Scholar]
- 14.Davis D, Barnes BE, Fox R. 1ed. Chicago: American Medical Association (AMA), AMA Press; 2003. The continuing professional development of physicians. from research to practice. [Google Scholar]
- 15.CanMeds Framework-Royall College. 2005. [Last accessed 2013 Nov 02]. Available from: http://www.ub.edu/medicina_unitateducaciomedica/documentos/CanMeds.pdf .
- 16.Medical Council of New Zeland. Home page. [Last accessed 2013 Nov 02]. Available from: http://www.mcnz.org.nz .
- 17.Maintenance of Certification Competencies. American Board of Medical Specialities. 2012. [Last accessed 2013 Nov 02]. Available from: http://www.abms.org .
- 18.General Medical Council. Regulating doctors, ensuring good medical practice. 2013. [Last accessed 2013 Nov 02]. Available from: http://www.gmc-uk.org/guidance/good_medical_practice.asp .
- 19.RANZCO CPD Program Handbook 2009-2011. [Last accessed 2013 Nov 02]. Available from: http://www.ranzco.edu/index.php/fellows/continuing-professional-development .
- 20.Thomson LG, Davis PM. Best medical practices in social accountability and continuing professional development: A survey and literature review. J Interprofessional Care. 2008;22:30–9. doi: 10.1080/13561820802013347. [DOI] [PubMed] [Google Scholar]
- 21.Bullock A, Bailey S, Cowpe J, Barnes E, Thomas H, Thomas R, et al. Continuing professional development systems and requirements for graduate dentists in the EU: Survey results from the DentCPD project. Eur J Dent Educ. 2013:17. doi: 10.1111/j.1600-0579.2012.00764.x. [DOI] [PubMed] [Google Scholar]
- 22.Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T, et al. Health professionals for a new century: Transforming education to strengthen health systems in an interdependent world. [Last accessed 2013 Nov 02];The Lancet. 2010 376:1923–58. doi: 10.1016/S0140-6736(10)61854-5. Available from: http://nrs.harvard.edu/urn-3:HUL.Inst Repos: 4626403 . [DOI] [PubMed] [Google Scholar]
- 23.Davis D, Parboosingh J. “Academic” CME and the social contract. Acad Med. 1993;68:329–32. doi: 10.1097/00001888-199305000-00003. [DOI] [PubMed] [Google Scholar]
- 24.World Federation for Medical Education (WFME). 2003. Continuing professional development of medical doctors: WFME global standards for quality improvement. [Last accessed 2013 Nov 02]. Available from: http://www.wfme.org/standards/cpd/doc_download/16-continuing-professional-development-cpd-ofmedicaldoctors--english .
- 25.General Medical Council: Continuing Professional Development. The international perspective July 2011. [Last accessed 2013 Nov 02]. Available from: http://www.gmcuk.org/CPD___The_International_Perspective_Jul_11.pdf_44810902.pdf .
- 26.UEMS. [Last accessed 2013 Nov 02]. Available from: http://www.uems.net .
- 27.Continuing Professional Development (CPD). A summary of the state of knowledge about physician training. Swedish Society of Medicine and the Swedish Medical Association joint working group. 2012. [Last accessed 2013 Nov 02]. English version 1. 2012. ISBN 978-91-979 706-1-7. Available from: http://www.sls.se/Global/cpd/cpd2012_english.pdf .
- 28.Khan KS, Coomarasamy A. 2006. “A hierarchy of effective teaching and learning to acquire competence in evidence-based medicine”. BMC Med Educ. 2006;6:59. doi: 10.1186/1472-6920-6-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Grant J, Stanton F. Edinburgh: Association for the Study of Medical Education; 1999. ASME occasional publication. The effectiveness of continuing professional development: a report for the Chief Medical Officer's review of continuing professional development in practice. [Google Scholar]
- 30.Peck C, McCall M, McLaren B, Rotem T. Continuing medical education and continuing professional development: International comparisons. [Last accessed 2013 Nov 02];BMJ. 2000 320:432–5. doi: 10.1136/bmj.320.7232.432. Available from: http://www.bmj.com/content/320/7232/432.pdf%2Bhtml . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lokuarachchi SK. Clinical Audit. What is it and how to do it? [Last accessed 2013 Nov 02];Galle Medical Journal. 2006 Sep;11 Available from: http://www.sljol.info/index.php/GMJ/article/download/1122/1029 . [Google Scholar]
- 32.Clinical audit. Wikipedia, the free encyclopedia. [Last accessed 2013 Nov 02]. Available from: http://.en.wikipedia.org/wiki/Clinical_audit .
- 33.Clinical Audit Criteria and Guidance Working Group. Health Audit Criteria and Guidance. 2008. [Last accessed 2013 Nov 02]. Available from: http://www.hse.ie/eng/about/Who/qualityandpatientsafety/resourcesintelligence/Quality_and_Patient_Safety_Documents/guid.pdf .
- 34.Bullivan J, Corbet- Nolan A. Health Quality Improvement Partnership. [Last assessed 2013 Nov 02]. Available from: http://www.hqip.org.uk/assets/Guidance/HQIP-Clinical-Audit-Simple-Guide-online1.pdf .
- 35.Principles for Best Practice in Clinical Audit. NHS, National Institute for Clinical Excellence. 2002. [Last accessed 2013 Nov 02]. Available from: http://www.nice.org.uk/media/796/23/bestpracticeclinicalaudit.pdf .
- 36.Redman W. 1 ed. London: Kogan Page; 1994. Portfolios for Development: A Guide for Trainers and Managers. [Google Scholar]
- 37.du Boulay C. From CME to CPD: Getting better at getting better? Individual learning portfolios may bridge a gap between learning and accountability. BMJ. 2000:320. doi: 10.1136/bmj.320.7232.393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Lorenz G, Ittelson J. An Overview of E-Portfolios (eli3001 e portfolios EDUCASE) ELI Paper 1: 2005 July. 2005. [Last accessed 2013 Nov 02]. Available from: http://net.educause.edu/ir/library/pdf/eli3001.pdf .
- 39.Gómez SS, Ostos EM, Solano JM, Salado TF. An electronic portfolio for quantitative assessment of surgical skills in undergraduate medical education. [Last accessed 2013 Nov 2]. Available from: http://www.biomedcentral.com/1472-6920/13/65 . [DOI] [PMC free article] [PubMed]
- 40.BMJ. Portfolio. [Last accessed 2013 Nov 02]. Available from: http://portfolio.bmj.com/portfolio/login.html .
- 41.Masmanian PE. Continuing Professional Education and the physician as a learner. JAMA. 2002;288:1057–60. doi: 10.1001/jama.288.9.1057. [DOI] [PubMed] [Google Scholar]
- 42.Davis DA, Thomson MA, Oxman AD, Haynes RB. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA. 1995;274:700–5. doi: 10.1001/jama.274.9.700. [DOI] [PubMed] [Google Scholar]
- 43.Learning Formats and Techniques. A Glossary by Type of Learning. [Last accessed 2013 Nov 02]. Available from: http://www.arrowhead.lib.mn.us/renewal/formats.htm .
- 44.Kane GM. Interactive Learning in Continuing Professional Development: “At Least 25 Per Cent of Time”. [Last accessed 2013 Nov 02]. Available from: http://www.royalcollege.ca/portal/page/portal/rc/common/documents/cpd_accreditation/support/interactive_learning_cpd_e.html .
- 45.Boulos MN, Maramba I, Wheeler S. Wikis, blogs and podcasts: A new generation of Web-based tools for virtual collaborative clinical practice and education. [Last accessed 2013 Nov 02];BMC Med Educ. 2006 6:41. doi: 10.1186/1472-6920-6-41. Available from: http://www.biomedcentral.com/content/pdf/1472-6920-6-41.pdf . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Labuschagne MJ. The role of simulation training in ophthalmology. Cont Med Educ. 2013. [Last accessed 2013 Nov 02]. p. 31. Available from: www.cmej.org.za/index.php/cmej/rt/printerFriendly/2697/2898 .
- 47.Micieli R, Micieli JA. Twitter as a tool for ophthalmologists. Can J Ophthalmol. 2012;47:410–3. doi: 10.1016/j.jcjo.2012.05.005. [DOI] [PubMed] [Google Scholar]
- 48.Bik HM, Goldstein MC. Introduction to Social Media for Scientists. [Last accessed 2013 Nov 02];PLoS Biol. 2013 11:e1001535. doi: 10.1371/journal.pbio.1001535. Available from: http://www.plosbiology.org/article/info: doi/10.1371/journal.pbio.1001535 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.du Boulay C. From CME to CPD: Getting better at getting better? Individual learning portfolios may bridge a gap between learning and accountability. BMJ. 2000:320. doi: 10.1136/bmj.320.7232.393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Houlden R. Collier: Evaluation of continuing professional development group activities. [Last accessed 2013 Nov 02]. Available from: http://www.royalcollege.ca/portal/page/portal/rc/common/documents/cpd_accreditation/sa_small_groups_e.pdf .
- 51.Accreditation Council for Continuing Medical Education ACCME) [Last accessed 2013 Nov 02]. Available from: www.accme.org/cme.providers .
- 52.Australian Medical Council. [Last accessed 2013 Nov 2]. Available from: http://www.amc.org.au/index.php/ar .
- 53.American Medical Association (AMA) CME provider resources. [Last accessed 2013 Nov 02]. Available from: http://www.ama-assn.org/ama/pub/education-careers/continuing-medical-education.page .
- 54.Details for CPD Guidance Framework for Appraisers and Appraisees. Academy of Medical Royal Colleges. [Last accessed 2013 Nov 02]. Available from: http://www.aomrc.org.uk/publications/statements/doc_details/9555-cpd-guidance-framework-for-appraisersand-appraisees.html .
- 55.UK Royal College of Ophthalmologists. [Last accessed 2013 Nov 02]. Available from: http://www.rcophth.ac.uk/page.asp?section=108 .
- 56.Guidance for CPD Approval. November 2010. Royal College of Ophthalmologists. [Last accessed 2013 Nov 2]. Available from: http://www.rcophth.ac.uk/core/core_picker/download.asp?id=707 .
- 57.Mandatory Educational Requirements Options of the Maintenance of Certification program (MOC) by the Approval of Accredited Group Learning Activities. [Last accessed 2013 Nov 02]. Available from: http://www.royalcollege.ca/portal/page/portal/rc/public .
- 58.Royal Austral i an and New Zeal and College of Ophthalmologists (RANZCO) Resources for CPD providers. [Last accessed 2013 Nov 02]. Availble from: http://www.ranzco.edu/index.php/fellows/continuing-professional-development/resources-for-cpd-providers .
- 59.The European Accreditation Council for CME (EACCME) [Last accessed 2013 Nov 02]. Available from: http://www.uems.net/index.php?id=70 .
- 60.Guidelines for Continuing Professional Development. Canadian Ophthalmological Society. [Last accessed 2014 Nov 02]. Available from: http://www.cos-sco.ca/wp-content/uploads/2012/06/COS-CPD-guidelines-rev-08inika.pdf .
- 61.The Accreditation of e-Learning Materials by EACCME. [Last accessed 2013 Nov 02]. Available from: http://www.uems.net/fileadmin/user_upload/uems_documents/contentogram_doc_client_20120530/UEMS_2011_20.pdf .
- 62.Criteria for aproval of online CPD Events for Maintenance of Certification (MOC) [Last accessed 2013 Nov 02]. Available from: http://www.royalcollege. ca/portal/page/portal/rc/members/cpd/cpd_accreditation/group_learning/cpd_accreditation_toolkit/online_event_criteria .
- 63.Royal College of General Practicioners Accreditation. RCGP educational accredition a guide for applicants. [Last accessed 2013 Nov 02]. Available from: http://www.rcgp.org.uk/revalidation-and-cpd/rcgp-educational-accreditation/~/media/Files/Revalidation-and-CPD/Accreditation/02%20%20RCGP%20A%20guide%20for%20%20Applicants%201213%20Master%20Copy.ashx .
- 64.Continuing Medical Education (CME) Requirements. International Council of Ophthalmology. 2003. [Last accessed 2013 Nov 02]. Available from: http://www.icoph.org/dynamic/attachments/resources/icocmereq.pdf .
- 65.Canadian Medical Association (CMA) Policy: Physicians and the Pharmaceutical Industry-Giuidelines for physicians in interactions with industry. 2007. [Last accessed 2013 Nov 02]. Available from: http://policybase.cma.ca/dbtw-wpd/Policypdf/PD08-01.pdf .
- 66.The Royal College of Physicians and Surgeons of Canada. Declaration of Conflict of interest. 2005. [Last accessed 2013 Nov 02]. Available from: http://www.royalcollege.ca/portal/page/portal/rc/common/documents/cpd_accreditation/coi_disclosure_form_e.pdf .