

Abstract
Context:
In recent years, there has been a marked change in life-style of South Asian countries caused by economic growth, affluence, urbanization and dietary westernization. Few studies on the prevalence of obesity, hypertension and diabetes in the Indian population have been reported. However, there has been scarce literature on the study of prevalence of type 2 diabetes mellitus (DM) and Hypertension in overweight and obese people in India with criteria suggested by World Health Organization (WHO) for Asians. Information on such public health issues would provide evidence based data to develop guidelines and policies on this subject.
Aim:
The aim of this article is to determine the prevalence of hypertension and type 2 DM in overweight and obese people.
Setting and Design:
A cross-sectional study consisted of people selected from the out-patient department and indoors of a large defense hospital in a semi urban area of Assam.
Materials and Methods:
Patients with overweight and obesity, reporting for consultation and medical examination were taken into the study. The data collected was analyzed using the criteria for overweight, obesity, diabetes and hypertension defined by WHO, Joint National Committee VII and International Diabetes Federation, American Diabetes Association. A descriptive statistical analysis has been carried out in the study.
Results:
A total of 300 people were the subject population of this study. Among the subject population, there were 97 overweight and 203 obese. The 56 subjects were found to be diabetic. The prevalence of type 2 DM in overweight subjects was 15.5% and in obese was 20.2% and overall was 18.7%. Prevalence of hypertension in the overweight population was 8.2% and in obese was 22.2% and overall found to be 17.7%.
Conclusions:
The prevalence of type 2 DM, hypertension in the obese group of the study population were found to be 20.2%, 22.2% and in the overweight population were 15.5% and 8.2%, respectively. This indicates that the prevalence of type 2 DM and hypertension increases with increasing weight of the individuals. The prevalence of type 2 DM and hypertension were relatively higher compared with other studies in India and abroad.
Keywords: Hypertension, obesity, overweight, type 2 diabetes mellitus
Introduction
During the last decade, the medical community has established that obesity due to over-nutrition and reduced physical activity has become not only the most prevalent nutritional disorder of the developed world, but an alarming threat to public health world-wide. Before 20th century, despite the warnings of physicians such as Galen and Hippocrates, many cultures have harbored the false belief that obesity was a sign of health. However, robust medical evidence has dispelled this and revealed in detail how obese individuals are prone to the plethora of diseases.[1]
The global epidemic of overweight and obesity – “globesity” - is rapidly becoming a major public health problem in many parts of the world.[2] World Health Organization (WHO) in its latest projections indicate that globally in 2008 approximately 1.5 billion adults (age 20+) were overweight and at least 500 million adults were obese. WHO further projects that by 2015, at least 2.3 billion adults will be overweight and more than 700 million will be obese. Overweight and obesity are associated with an increased risk of developing hypertension and diabetes.[3,4,5,6,7] The prevalence of these chronic disorders has been reported to be increasing in India. Overweight and obesity have been found to have an impact in the clinical profile of diabetes and hypertension in various studies. In India, there is a rising burden of chronic diseases such as hypertension and diabetes mellitus (DM). India has the largest number of diabetics in the world with a 3.8% in rural and 11.8% in urban adults. The prevalence of hypertension has been reported to range between 12% and 17% among rural and 20-40% in urban adults.[8]
There are many studies about the prevalence of hypertension and type 2 DM in India and abroad, but there are no such studies in overweight and obese individuals with latest Asia specific criteria for obesity. This study will provide more information on the subject. A better understanding of the close linkage of obesity with hypertension and diabetes may help in prevention and treatment of obesity and may lead to reductions in cardiovascular and renal risk.
Materials and Methods
This cross-sectional study consisted of total 300 overweight and obese people selected from the outpatient departments (OPDs) and indoor wards of a large Defense Service Hospital in Assam during April 2009 to March 2011.
Design of the study
This study was based on the cross-sectional study design. The subjects who took part in the study were selected on the basis of criteria for overweight and obesity as suggested for Asians by WHO expert consultation on body mass index (BMI) in Asian populations.[9,10]
Inclusion criteria
Age > 18 years of age.
Weight > 20% of ideal weight or BMI > 23 kg/m2 or waist > 90 cm in men and > 80 cm in women.
Exclusion criteria
People who did not volunteer to participate in the study.
Criteria for overweight and obesity
Any one of the following criteria[9,10]
Weight > 20% of ideal bodyweight is overweight and > 30% is obese.
BMI > 23-24.9 is overweight and > 25 is obese.
Waist circumference: Men > 90 cm, women > 80 cm.
Diagnosis of DM
Diabetes was diagnosed if: (a) Fasting plasma glucose ≥ 126 mg/dL (7.0 mmol/L) or (b) 2 h plasma glucose ≥ 200 mg/dL (11.1 mmol/L) during an oral glucose tolerance test using a glucose load of equivalent to 75 g anhydrous glucose in water or (c) Symptoms of diabetes plus random plasma glucose ≥ 200 mg/dL (11.1 mmol/L). Repeat test was carried out to confirm the diagnosis of DM.[11]
Diagnosis of hypertension
The diagnosis of Hypertension was made on the basis of Joint National Committee VII (JNC VII) criteria.[12] Blood pressure record was performed in two sittings after 2 min interval and blood pressure ≥ 140/90 mm of Hg was taken as hypertension.
Sample size
A total of 300 personnel were taken into the study.
Protocol
People were enrolled in the study when they reported to hospital OPD. An informed consent was obtained from the people after explaining the study procedures in detail. During the process of their medical assessment at our hospital, relevant history and measurements were taken, questionnaire filled as per study proforma and relevant investigations were asked for. Relevant investigations were carried out to diagnose diabetes and associated abnormalities. The data were collected and results were analyzed.
The following parameters were recorded
Personal details, which included name, age, sex, address, trade and occupation.
History of any relevant previous illness such as diabetes, hypertension.
Anthropometry – Height, weight, waist circumference, hip circumference. BMI and waist: Hip ratio was calculated from the parameters measured.
Resting heart rate.
Resting blood pressure in the right arm – Sitting position.
Electrocardiography – Resting if indicated.
Biochemical investigations.
Blood sugar profile assessment, which includes fasting (8 h of fasting) blood sugar, 2 h post-prandial blood sugar or glucose tolerance test if indicated. Repeat test for confirmation of diagnosis of DM.
Lipid profile (8 h of fasting) including total cholesterol, triglycerides, low density lipoprotein, high density lipoprotein and very low density lipoprotein.
Serum uric acid if indicated.
Ultrasonography Abdomen if indicated.
Statistical analysis
Descriptive statistical analysis has been carried out in the present study and results on categorical measurements are presented in a number (%). Chi-square test has been used to find the significance of study parameters on categorical scale between two or more groups.[13,14,15,16]
Statistical software
The statistical software statistical product and service solutions (SPSS 15.0) was used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables, etc.
Results
A total of 300 people were the subject population of this study, out of which 217 (72.3%) were males and 83 (27.7%) females.
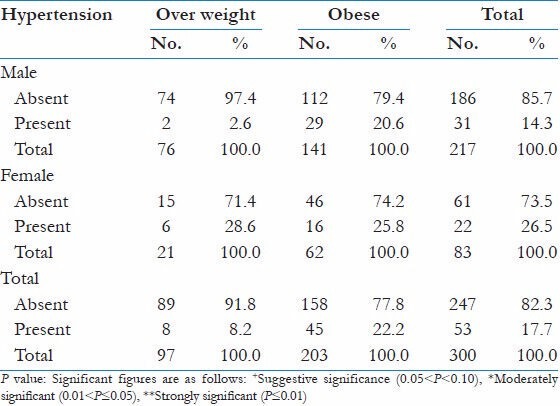
Prevalence of hypertension in the overweight population were 8 (8.2%) and in the obese population were 45 (22.2%) and overall 53 (17.7%) as shown in Table 1. The overall prevalence of hypertension was 17.7% with 22.2% in the obese group was more significantly associated with χ2 = 8.740; P < 0.001**.
Table 1.
Prevalence of hypertension
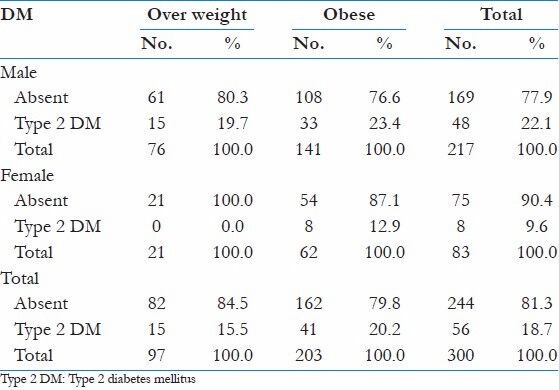
Prevalence of type 2 DM in overweight subjects were 15 (15.5%) and in the obese population were 41 (20.2%) and overall 56 (18.7%). The overall prevalence of type 2 DM was more positively associated with obese groups with 20.2% compared with 15.5% in overweight with χ2 = 0.969; P = 0.325 as shown in Table 2.
Table 2.
Prevalence of type 2 DM based on blood sugar level
Discussion
This study was a cross-sectional study of a select population that presented to a tertiary care armed forces hospital. A total of 300 people were the subject population of this study, out of which 217 (72.3%) were males and 83 (27.7%) females. More males were part of the study because more males reported as the study was conducted in an armed forces hospital. Prevalence of hypertension varies across the globe, in part reflecting the age and ethnicity of the populations studied. Population studies have documented variable prevalence rate of hypertension in different populations. The criteria for diagnosing hypertension in this study were as per JNC VII.[12]
In this study, prevalence of hypertension in the overweight population was 8.2% and in an obese population were 22.2% and overall 17.7%. Prevalence in developing countries seems to be similar to that European or other developed countries ranging from 10% to 20% among adults.[17] Amongst the recent study, the Chennai urban Rural Epidemiological Study (CURES – part I 2003) conducted by Mohan from Madras Diabetic Research Foundation, which covered 50,000 subjects revealed that 23% of the survey population had hypertension.[18] Study of Mani from Chennai performed in a Hamlet of the rural population covering 21,062 subjects detected hypertension in 5.26%.[19] The prevalence of hypertension was relatively high compared with other studies due to overweight and obese study population. The prevalence was detected to increase with increasing weight.
In this study, prevalence of type 2 DM in overweight subjects were 15.5% and in the obese population were 20.2% and overall 18.7%. CURES – Part I 2003 conducted by Mohan from Madras Diabetic Research Foundation which covered 50,000 subjects revealed that 16% of the subject above the age of 20 years were affected by diabetes.[18] Study of Mani from Chennai done in a Hamlet of the rural population covering 21,062 subjects detected diabetes in 3.64%.[19] The prevalence rates found in this study differs from other similar studies conducted. The prevalence rates were relatively high because of overweight and obese study population. The prevalence was found more in obese than overweight group that indicates that prevalence increases with increasing weight.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Haslam D. Obesity: A medical history. Obes Rev. 2007;8(Suppl 1):31–6. doi: 10.1111/j.1467-789X.2007.00314.x. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i. [PubMed] [Google Scholar]
- 3.Brown CD, Higgins M, Donato KA, Rohde FC, Garrison R, Obarzanek E, et al. Body mass index and the prevalence of hypertension and dyslipidemia. Obes Res. 2000;8:605–19. doi: 10.1038/oby.2000.79. [DOI] [PubMed] [Google Scholar]
- 4.Gregg EW, Cheng YJ, Cadwell BL, Imperatore G, Williams DE, Flegal KM, et al. Secular trends in cardiovascular disease risk factors according to body mass index in US adults. JAMA. 2005;293:1868–74. doi: 10.1001/jama.293.15.1868. [DOI] [PubMed] [Google Scholar]
- 5.Huang Z, Willett WC, Manson JE, Rosner B, Stampfer MJ, Speizer FE, et al. Body weight, weight change, and risk for hypertension in women. Ann Intern Med. 1998;128:81–8. doi: 10.7326/0003-4819-128-2-199801150-00001. [DOI] [PubMed] [Google Scholar]
- 6.Wannamethee SG, Shaper AG. Weight change and duration of overweight and obesity in the incidence of type 2 diabetes. Diabetes Care. 1999;22:1266–72. doi: 10.2337/diacare.22.8.1266. [DOI] [PubMed] [Google Scholar]
- 7.Gelber RP, Gaziano JM, Manson JE, Buring JE, Sesso HD. A prospective study of body mass index and the risk of developing hypertension in men. Am J Hypertens. 2007;20:370–7. doi: 10.1016/j.amjhyper.2006.10.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reddy KS, Shah B, Varghese C, Ramadoss A. Chronic diseases 3. Lancet. 2005;366:1746–51. doi: 10.1016/S0140-6736(05)67343-6. [DOI] [PubMed] [Google Scholar]
- 9.World Health Organization/International Association for the Study of Obesity/International Obesity Takforce. The Asia-Pacific perspective: Redefining Obesity and its treatment. Available from: http://www.idi.org.au/obesityreport.htm .
- 10.WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363:157–63. doi: 10.1016/S0140-6736(03)15268-3. [DOI] [PubMed] [Google Scholar]
- 11.Part 1: Diagnosis and Classification of Diabetes Mellitus. Geneva: Department of Non Communicable Diseases Surveillance, WHO; 1999. World Health Organisation. Definition, diagnosis and classification of diabetes mellitus and its complications. [Google Scholar]
- 12.Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jr, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: The JNC 7 report. JAMA. 2003;289:2560–72. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- 13.Rosner B. Fundamentals of Biostatistics. 5th ed. Duxbury: 2000. pp. 80–240. [Google Scholar]
- 14.Riffenburg RH. Statistics in Medicine. 2nd ed. Waltham, Massachussetts, United States of America: Academic Press; 2005. pp. 85–125. [Google Scholar]
- 15.Rao PS, Richard J. A Manual for Students in Health Sciences. New Delhi: Prentice Hall of India; 2000. An introduction to biostatistics; pp. 86–160. [Google Scholar]
- 16.Eng J. Sample size estimation: How many individuals should be studied? Radiology. 2003;227:309–13. doi: 10.1148/radiol.2272012051. [DOI] [PubMed] [Google Scholar]
- 17.Park K. Park's Textbook of Preventive and Social Medicine. 20th ed. Jabalpur (India): M/s Banarsidas Bhanot Publishers; 2005. Hypertension; p. 325. [Google Scholar]
- 18.Mohan V. Prevalence of diabetes and hypertension in South Indian population - The Chennai urban rural epidemiology study (CURES) Asian J Diabetol. 2003;5:29–3. [Google Scholar]
- 19.Mani MK. Prevention of chronic renal failure at the community level. Kidney Int Suppl. 2003;83:S86–9. doi: 10.1046/j.1523-1755.63.s83.17.x. [DOI] [PubMed] [Google Scholar]