

Abstract
Objective:
Families' perceptions, beliefs, and attitudes about malaria causation, symptom identification, treatment of malaria, and prevention are often overlooked in malaria control efforts. This study was conducted to understand these issues, which can be an important step towards developing strategies, aimed at controlling malaria.
Materials and Methods:
A community based descriptive cross-sectional study in four villages: Danwarai, Gehuru, Jiga, and Kashin Zama of Aliero local government area in Kebbi Sate, in northern Nigeria. Two hundred household were randomly selected and interviewed using standardized questionnaire.
Results:
Knowledge of the role of mosquitoes in malaria transmission (11.8%) and cause of malaria (9.6%) was observed to be low among the study population. Comprehensive knowledge about malaria prevention measures was high (90%), but not reflecting in their practice (16%). They have good knowledge of mosquito behavior (breeding areas (64.5%), resting places (70%) and biting time (81%)). Seeking hospital care for a febrile child was a good practice (68.5%) observed. Attitudes regarding the best antimalarial therapy was limited (56.7%) to chloroquine.
Conclusions:
Misconceptions about malaria transmission and its cause still exist. Knowledge about preventive measures does not necessarily translate into improvement in practices. There is a need for targeted educational programs to increase the communities' efforts to develop desirable attitude and practices regarding malaria and their participation for malaria control.
Keywords: Attitudes, knowledge, malaria, practices, rural-Aliero
Introduction
Malaria is unique among diseases because its roots lie so deep within human communities.[1] Malaria beliefs and practices are often related to culture, and can influence the effectiveness of control strategies;[2] thus, local knowledge and practice related to malaria is important for the implementation of culturally appropriate, sustainable, and effective interventions.[3]
Globally, an estimated half of world populations are at risk of malaria. Malaria is endemic in Africa with an estimated 80% of cases and 90% of deaths of the global burden occurring there, especially amongst children and pregnant women. Together, the Democratic Republic of the Congo and Nigeria account for over 40% of the estimated total of malaria deaths globally.[4] Malaria is a major public health problem in Nigeria with an estimated 100 million malaria cases and over 300,000 deaths per year. It accounts for 60% of outpatient visits, 30% of hospitalizations among children under 5 years of age, and 11% maternal mortality.[5]
Twelve years after the first Abuja declaration, Nigeria failed to halve the malaria burden in 2010. In the next 2 years leading up to the Millennium Development Goals' (MDG) deadline, Nigeria is still recording high prevalence (98.4%) of malaria,[6] hence it is doubtful if Nigeria could halt by 2015 and begin to reverse the incidence of malaria.
The failure to consider community's knowledge, attitude, and practice (KAP) about malaria has contributed to the inability of programs to achieve sustainable control.[7] People's behavior may increase malaria risk, but to change such behavior is not easy. Indeed, there are many reasons why particular behaviors exist and they often are tied to considerable benefits in areas quite distinct from health. Thus, it is not usually the case that “these people don't know any better”, but rather that their native logic and rationality make sense within the realities and limitations of their local circumstances.[1]
Families are the primary context within which most health problems and illnesses occur and have a powerful influence on health. Most health belief and behavior are developed and maintained within the family.[8] Community perceptions, beliefs, and attitudes about malaria causation, symptom identification, treatment of malaria, and prevention influence efforts to address malaria and are often overlooked in control efforts[9] and it vary from community to community and among individual households.[10] Considering these issues it can be an important step towards developing strategies aimed at controlling the malaria.[11] Understanding who already knows about malaria and malaria prevention, who has adopted malaria prevention and mosquito avoidance practices, and who is at risk of malaria infection is a necessary precursor to identifying and targeting vulnerable populations and ensuring successful implementation and sustainability of malaria control efforts.[12]
There is paucity of data on KAP studies on malaria in northwestern Nigeria. Studies on KAP[10,13] have demonstrated that, direct interaction with community plays an important role in circumventing malaria spread. Healthcare provider like family physician can focus both on traditional physician-patient model and complement it with population based medicine for primary prevention of malaria as domiciliary care and primary prevention are defining characteristics of family medicine. So, in order to create a synergy between primary care physician and community efforts and governmental/nongovernmental organized malaria control interventions in north Nigeria in particular, there is an urgent need to determine the people's knowledge, attitude, and practice of malaria and its control.
Materials and Methods
Study area
The study was carried out in the four villages Danwarai, Gehuru, Jiga, and Kashin Zama of Aliero Local Government Area. Aliero is approximately located at latitudes 4°23'S and 12°26'40“N and longitudes 3°6'W and 4°27'35“E. It was created in 1996, with a total land mass of 412.25 km2[14] and has a total population of 67,078.[15]
Study design and data collection
The study was a community based cross-sectional study. A structured questionnaire was used for interview. The questionnaire was administered to 200 randomly selected households in July and August 2012. Only one adult was interviewed per household. The interviewees were the heads of households. In their absence, a responsible adult above 18 years, chosen by the family was interviewed. The questionnaire was prepared in English language but translated and communicated in local languages when necessary.
Ethical clearance
The study was approved by Kebbi State University of Science and Technology. The objectives of the study were explained to community leaders and local government executives before the permission was granted. Full verbal explanation of the study was given to members of selected households and consent was obtained before inclusion as participants. Respondents were given the right to refuse to take part in the study as well as to withdraw any time during the interview. Privacy and confidentiality were maintained throughout the study.
Data analysis
The data were entered into a Microsoft Excel - Worksheet and analyzed using Epi Info, version 3.5.3. Descriptive statistics were carried out to measure relative frequencies, percentages, averages, and relative frequencies of the variables.
Results
Sociodemographic characteristics of the study population
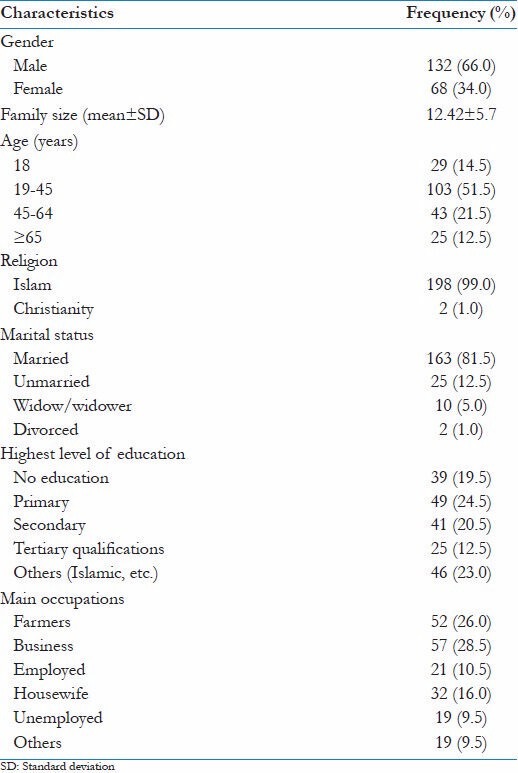
A total of 200 households' heads were interviewed, 36 from Danwarai, 80 from Gehuru, 39 from Jiga, and 45 from Kashin Zama. There were 68 (34.0%) females and 132 (66.0%) males. Islam was the predominant religion with 198 (99.0%) respondents and Christianity with only two (1.0%) respondents. The sociodemographic and household characteristics of the study population are presented in Table 1.
Table 1.
Sociodemographic characteristics of the study population
Knowledge of malaria, its transmission, cause, and symptom
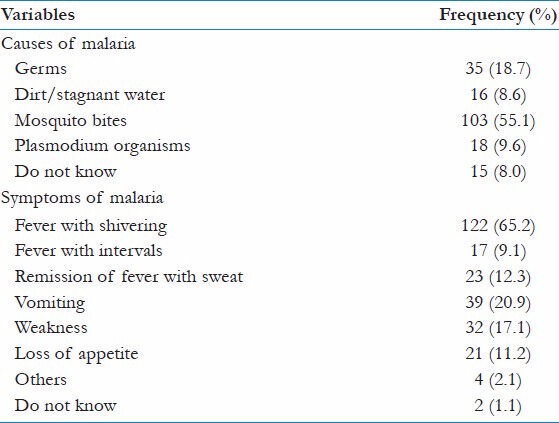
When asked, “Have you heard of malaria?”; 187 respondents (93.5%) stated yes and 13 (6.5%) stated no. Of the ‘yes’ group, 80 (42.8%) knew malaria because they suffered it. Only 22 (11.8%) respondent correctly stated that mosquitoes which has bitten a malaria patient, was the mode of transmission, while most 139 (74.3%) reported by bites of any mosquito. Plasmodium organism as the main cause of malaria was correctly identified by only 18 (9.6%). Majority of them, 103 (55.1%) reported mosquito bite as cause of malaria. The most commonly mentioned symptom was fever with shivering by 122 respondents (65.2%) [Tables 2 and 3].
Table 2.
Knowledge of malaria and its transmission
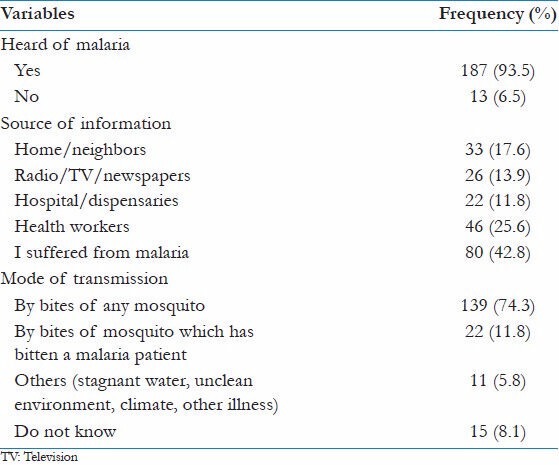
Table 3.
Knowledge of malaria causes and symptoms
Knowledge of preventive measures
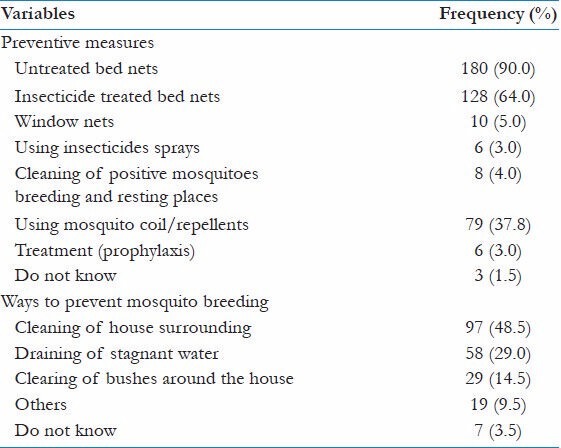
About 180 (90.0%) of the respondents reported any bed nets as the most common known protective method against malaria, while 128 (64.0%) respondent had knowledge of insecticide treated bed net (ITNs). Second most common known preventive measure was use of mosquito coils by 79 (37.8%) respondent. The knowledge of ways to prevent mosquito breeding, by cleaning of house surroundings was reported by 97 (48.5%) and draining of stagnant water by 58 (29.0%) [Table 4].
Table 4.
Knowledge of malaria preventive measures
Knowledge of mosquito behavior
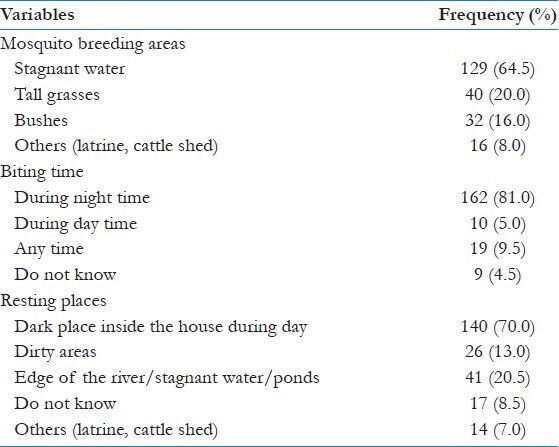
Stagnant water was reported as mosquito breeding area by most, 129 (64.5%) respondent. Knowledge about mosquito biting time was relatively high, almost all 162 (81.0%) knew that night time is the biting time of mosquito. Majority of respondents 140 (70.0%) identified the indoor dark resting place during day as the resting places of mosquitoes [Table 5].
Table 5.
Knowledge of mosquito behavior
Attitudes and practices against malaria and its control
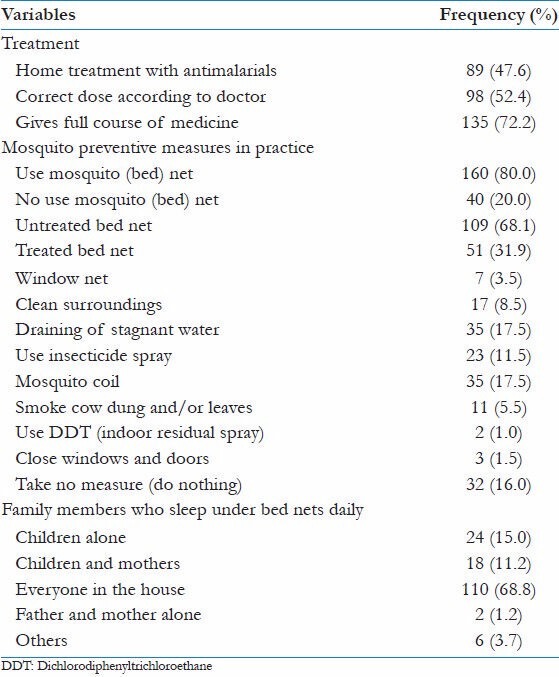
When asked what they would do if their child had fever, most caregivers 137 (68.5%) reported that they would go to a hospital. The most important factor was condition of child when deciding to seek formal care for child with fever, reported by 104 (52.0%) followed by perceived cost by 77 (38.5%) respondent. Attitude regarding the best antimalarial therapy was limited to chloroquine, reported by most of them, 106 (56.7%). About 160 (80.0%) of the respondents reported to own any bed nets as the most common protective method against malaria in practice, while 40 (20.0%) reported not using the mosquito net. Those who reported using bed nets only 51 (31.9%) reported using ITNs and 109 (68.1%) reported using untreated nets. Second most common preventive measure in practice was mosquito coil reported by 35 (17.5%). Although 32 (16.0%) reported using no preventive measures, about 110 (68.8%) reported that everyone in their family was sleeping under bed nets [Tables 6 and 7]. In practice, 89 (47.6%) respondents reported home treatment with antimalarial.
Table 6.
Attitudes against malaria and its control
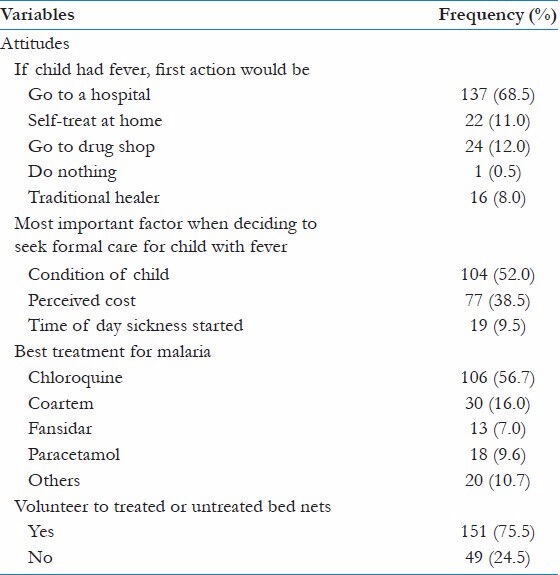
Table 7.
Practices against malaria and its control
Discussion
KAP of malaria and its control were observed to be low among the study population. This result is in agreement with previous findings of other similar studies[9,12,13,16] and in contrast to other similar studies.[17,18,19] Majority of respondents reported to have ever heard about malaria. This was consistent with other studies[13,16,19] that shows almost all the respondents have heard about malaria. The main source of information was from individuals' experiences with malaria as reported earlier in a study in Nigeria,[20] followed by health centers; consistent with another Nigerian study.[21] There was gaps in knowledge by 8.1% of the respondents stating that they did not know the mode of transmission and more than half (74.3%) of the study participants mentioned bites of any mosquito as a mode of malaria transmission. Only a small proportion of respondents correctly mentioned about malaria transmission and its cause. Thus, the knowledge level of respondents about the mode of malaria transmission was very low when compared to the findings in previous studies reported across Africa.[2,6,11,19,22,23] This may be attributable to low level of education in the rural community. Knowledge of mosquito behavior is important to take appropriate malaria preventive actions and it was relatively high among participants of the present study.
This study has demonstrated that respondent had a good knowledge about malaria signs and symptoms. Majority of the respondents mentioned fever (with shivering) as the most common symptom of malaria and is consistent with observations from other similar studies.[9,16,24,25,26] This high level of awareness of the clinical features of malaria might be due to increased access to mass media, health education by health workers, and self experience of malaria. Environmental vector control through elimination of the vector habitat at an early stage is an important primary preventive measure for malaria. In this study, the respondents had good knowledge on environmental preventive measures, consistent with other studies in Nigeria[18,20] and in Ethiopia;[19] but the knowledge does not necessarily translate into improved practice of preventive measures; an observation reflected in this study. This might be due to poor socioeconomic status and low level of formal education of the rural communities.
Knowledge on the use of bed net as a preventive measure against mosquito bite was high among the respondents (90%) in this study, but only 80% reported use of any bed nets (ITNs or non ITNs). The remaining 10% were aware of their effectiveness in prevention of malaria but could not afford them. Similar high level of knowledge on preventive use of bed net had been observed in other studies in Ethiopia[19,27] and in Malawi.[22] The awareness of ITNs was high among respondents, but only 31.9% of respondents were actually using it. The added advantage of treating bed nets with residual insecticides should be made known to the communities. Since the cost is reported a major reason for its low utilization in this study and in other study in Nigeria,[18] government should consider subsidizing mosquito nets to enable all families to invest in them.
Use of hospital for treatment was uniformly advocated, which is similar with a study in Ethiopia.[19] This might reflect issues of accessibility and quality in the health facilities. But in practice 47.6% of respondent reported giving home treatment, which is consistent with findings reported from other studies in Nigeria[26,28,29] and other countries.[30,31] The use of home treatment might be because most of them could not afford hospital and needed prompt treatment. The knowledge of proper administration of antimalarials was also limited as reported in other studies.[17,31] Thus, malaria control policies should recognize the role of home treatment in the management of malaria and provide trainings for the adequate use of antimalarial drugs. An encouraging finding of our study was that only 8% of respondent mentioned traditional healer as a choice of treatment, which was consistent with previous study in Nigeria.[32] Although local shops were not the popular treatment source in rural areas of Aliero, but sometimes they were the alternative to medical facilities. As a result, a significant portion of the population were receiving initial treatment for perceived malaria from local shops, whose knowledge and capacity for curative treatment is questionable[33] and should be considered when designing treatment and intervention programs. There is potential to improve malaria care by educating local shopkeepers on the symptoms, appropriate treatment, and dosages of antimalarial drugs. Such educational interventions have been shown to change malaria treatment seeking behavior in other malaria endemic areas.[34,35] In addition, ensuring that shopkeepers understand the proper drug regimen for treating an episode of malaria may help protect against the development of drug resistance by limiting overuse and underdosing.[36]
Misconceptions about malaria transmission still exist. Increasing the knowledge about malaria transmission and benefits of using available effective preventive and control measures by the individual households and the community could contribute much to the overall reduction of the malaria burden. Educational messages must be culturally sensitive and capitalize on the positive beliefs and behaviors that already exist in local communities. Likewise, programs that mobilizes communities can play a critical role in the adoption of preventive behaviors. An understanding of how these strategies reach the population together with the identification of the main determinants that influence protective behavior are required to monitor evaluate the progress of the malaria control efforts.
Perhaps solution of malaria control lies -in primary care physicians such as family physician or community health workers working in the rural communities. The result of this study will increase their current knowledge for health education and promotion on malaria at the first contact either in the health facilities or in the patient's family house upon home visit.
Acknowledgment
We wish to thank the villagers of Danwarai, Gehuru, Jiga, and Kashi Zama in Aliero Local Government community who participated in the study. I am grateful to their Chairman for his cooperation and logistic support during the study period.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Heggenhougen HK, Hackethal V, Vivek P. The behavioural and social aspects of malaria control: An introduction and annotated bibliography. World Health Organization on behalf of the Special Programme for Research and Training in Tropical Diseases. 2003 TDR/STR/SEB/VOL/031. [Google Scholar]
- 2.Adera TD. Beliefs and traditional treatment of malaria in Kishe settlement area, South West Ethiopia. Ethiop Med J. 2003;41:25–34. [PubMed] [Google Scholar]
- 3.Vijayakumar KN, Gunasekaran K, Sahu SS, Jambulingam P. Knowledge, attitude and practice on malaria: A study in a tribal belt of Orissa state, India with reference to use of long lasting treated mosquito nets. Acta Trop. 2009;112:137–42. doi: 10.1016/j.actatropica.2009.07.011. [DOI] [PubMed] [Google Scholar]
- 4.WHO. World Malaria Report 2012. Geneva: World Health Organization; 2012. p. xiii. [Google Scholar]
- 5.Nigeria Malaria Fact Sheet United States Embassy in Nigeria Economic Section, United States Embassy in Nigeria, Abuja, Nigeria. 2011. [Last accessed on 2013 Aug 07]. Available from: http://www.nigeria.usembassy.gov .
- 6.Ako-Nai KA, Adesiyan M. Unusually High prevalence of malaria in a tertiary institution setting in South western Nigeria. Int J Med. 2012;7:121–9. [Google Scholar]
- 7.Tyagi P, Roy A, Malhotra MS. Knowledge, awareness and practices towards malaria in communities of Rural, semi-rural and bordering areas of east Delhi, India. J Vector Borne Dis. 2005;42:30–5. [PubMed] [Google Scholar]
- 8.Campbell TH, McDaniel SH, Cole-Kelly K. Family issues in Health care. In: Taylor RB, editor. Family Medicine Principles and Practices. 6th ed. New York: Springer-Verlag; 2002. p. 24. [Google Scholar]
- 9.Deressa W, Ali A, Enquoselassie F. Knowledge, attitude and practice about Malaria the mosquito and antimalarial drugs in a rural community. Ethiop J Health Dev. 2003;17:99–104. [Google Scholar]
- 10.Rodriguez AD, Penilla RP, Henry-Rodriguez M, Hemingway J, Francisco Betanzos A, Hernandez-Avilla JE. Knowledge and beliefs about malaria transmission and practices for vector control in Southern Mexico. Salud Púlica Méx. 2003;45:110–6. [PubMed] [Google Scholar]
- 11.Munguti KJ. Community perceptions and treatment seeking for malaria in Baringo District, Kenya: Implications for disease control. East Afri Med J. 1998;75:687–91. [PubMed] [Google Scholar]
- 12.Adongo PB, Kirkwood B, Kendall C. How local community knowledge about malaria affects insecticide treated net use in northern Ghana. Trop Med Int Health. 2005;10:366–78. doi: 10.1111/j.1365-3156.2005.01361.x. [DOI] [PubMed] [Google Scholar]
- 13.Mazigo HD, Obasy E, Mauka W, Manyiri P, Zinga M, Kweka EJ, et al. Knowledge, attitudes, and practices about malaria and its control in rural northwest Tanzania. Malar Res Treat. 2010;2010:794261. doi: 10.4061/2010/794261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Statistical Year Book. Kebbi State of Nigeria, Birnin Kebbi, Kebbi State. 2007 [Google Scholar]
- 15.Federal Republic of Nigeria Official Gazette, Abuja. 2009;96:B33. [Google Scholar]
- 16.Chovatiya SK, Gajera NB, Soni VC. People's perception on malaria: A case study in rural areas of Rajkot district, Gujarat-India. Health Sci Int J. 2013;2:1–5. [Google Scholar]
- 17.Adedotun AA, Morenikeji OA, Odaibo AB. Knowledge, attitudes and practices about malaria in an urban community in south-western Nigeria. J Vector Borne Dis. 2010;47:155–9. [PubMed] [Google Scholar]
- 18.Iriemenam NC, Dosunmu AO, Oyibo WA, Fagbenro-Beyioku AF. Knowledge, attitude, perception of malaria and evaluation of malaria parasitaemia among pregnant women attending antenatal care clinic in metropolitan Lagos, Nigeria. J Vector Borne Dis. 2011;48:12–7. [PubMed] [Google Scholar]
- 19.Abate A, Degarege A, Erko B. Community knowledge, attitude and practice about malaria in a low endemic setting of Shewa Robit Town, northeastern Ethiopia. BMC Public Health. 2013;13:312. doi: 10.1186/1471-2458-13-312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Olayemi IK, Omalu IC, Abolarinwa SO, Mustapha OM, Ayanwale VA, Mohammed AZ, et al. Knowledge of malaria and implications for control in an endemic urban area of north central Nigeria. Asian J Epidemiol. 2012;5:42–9. [Google Scholar]
- 21.Fatungase KO, Amoran OE, Fatugase OK. The impact of health education intervention on perception and treatment seeking behaviour about childhood infections among caregivers in rural communities in western Nigeria. Br J Med Med Res. 2013;3:1331–43. [Google Scholar]
- 22.Masangwi SJ, Grimason AM, Morse TD, Ferguson NS, Kazembe LN. Community knowledge variation, bed-net coverage and the role of a district healthcare system, and their implications for malaria control in southern Malawi. South Afr J Epidemiol Infect. 2012;27:116–25. [Google Scholar]
- 23.Amron OE. Impact of health education intervention on malaria prevention practices among nursing mothers in rural communities in Nigeria. Niger Med J. 2013;54:115–22. doi: 10.4103/0300-1652.110046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Joshi AB, Banjara MR. Malaria related knowledge, practices and behaviour of people in Nepal. J Vector Borne Dis. 2008;45:44–50. [PubMed] [Google Scholar]
- 25.Hanafi-Bojd AA, Vatandoost H, Oshaghi MA, Eshraghian MR, Haghdoost AA, Abedi F, et al. Knowledge, attitudes and practices regarding malaria control in an endemic area of southern Iran. Southeast Asian J Trop Med Public Health. 2011;42:491–501. [PubMed] [Google Scholar]
- 26.Okwa OO, Bello BA, Olundegun SA. Social aspects of malaria among students in two tertiary institutions in Lagos, Nigeria. Sierra Leone J Biomed Res. 2011;3:97–103. [Google Scholar]
- 27.Kaliyaperumal K, Yesuf D. Knowledge, attitudes and practices of local inhabitants about insecticide treated nets (ITNs) for malaria control in an endemic area of Ethiopia. East Afr J Public Health. 2009;6:205–10. doi: 10.4314/eajph.v6i2.51776. [DOI] [PubMed] [Google Scholar]
- 28.Fatungase KO, Amoran OE, Alausa KO. The effect of health education intervention on the home management of malaria among the caregivers of children aged under 5 years in Ogun State, Nigeria. Eur J Med Res. 2012;17:11. doi: 10.1186/2047-783X-17-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Okwa OO, Soremekun BM, Adeseko O, Raheem AM. Artisans and traders' knowledge, attitude and practices of malaria in selected areas of Lagos, Nigeria. Glo Adv Res J Med Sci. 2012;1:68–74. [Google Scholar]
- 30.Simsek Z, Kurcer MA. Malaria: Knowledge and behaviour in an endemic rural area of Turkey. Public Health. 2005;119:202–8. doi: 10.1016/j.puhe.2004.03.011. [DOI] [PubMed] [Google Scholar]
- 31.Nsagha DS, Njunda AL, Kamga HL, Nsagha SM, Assob JC, Wiysonge CS, et al. Knowledge and practices relating to malaria in a semi-urban area of Cameroon: Choices and sources of antimalarials, self-treatment and resistance. PAMJ. 2011;9:8. doi: 10.4314/pamj.v9i1.71180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Jombo GT, Mbaawuaga EM, Denen AP, Alao OO, Peters EJ, Dauda MA, et al. Choices of drugs for self-treatment of malaria among adult women in a Nigerian city: Implications for the success of the ongoing ‘roll back’ malaria programme. J Microbiol Antimicrob. 2010;2:57–63. [Google Scholar]
- 33.Ahmed SM, Hossain MA. Knowledge and practice of unqualified and semi-qualified allopathic providers in rural Bangladesh: Implications for the HRH problem. Health Policy. 2007;84:332–43. doi: 10.1016/j.healthpol.2007.05.011. [DOI] [PubMed] [Google Scholar]
- 34.Tavrow P, Shabahang J, Makama S. Vendor-to-vendor education to improve malaria treatment by private drug outlets in Bungoma District, Kenya. Malar J. 2003;2:10. doi: 10.1186/1475-2875-2-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Alvarado BE, Gomez E, Serra M, Carvajal R, Carrasquilla G. Evaluation of an educational strategy on malaria in rural areas of the Colombian Pacific Coast. Biomedica. 2006;26:342–52. [PubMed] [Google Scholar]
- 36.Abuya TO, Mutemi W, Karisa B, Ochola SA, Fegan G, Marsh V. Use of over-the-counter malaria medicines in children and adults in three districts in Kenya: Implications for private medicine retailer interventions. Malar J. 2007;6:57. doi: 10.1186/1475-2875-6-57. [DOI] [PMC free article] [PubMed] [Google Scholar]