

Abstract
Context:
Patient satisfaction is of increasing importance and recognized as an important indicator for quality of care. It is influenced by the patients, physicians and practice's characteristics. The literature on diabetes has increasingly focused on the quality of care and its measurement. The relationship between the quality of diabetes care and patient satisfaction is poorly understood and it requires further elaboration.
Aims:
The aim of this study is to Identify the underlying factors influencing patient's satisfaction with the diabetes care, to assess whether comprehensive diabetes management that provided in diabetic clinic improves satisfaction and glycemic control.
Settings and Design:
Cross-sectional study Family Medicine and Diabetic Clinics at King Abdul-Aziz Medical City.
Materials and Methods:
A total of 230 type two diabetic patients attending their follow-up were requested to fill the questionnaire. The questionnaire identified patients, doctors and practice related factors.
Statistical Analysis Used:
SPSS 16 with appropriate statistical test.
Results:
The response rate was 85%. Mean hemoglobin A1c (HbA1c) level was 0.087 ± 0.020. Around half of the patients were having high satisfaction rate of (>60%). Doctor's communication ranked the highest satisfaction level among other factors. However, no association between satisfaction with other patient's characteristics and HbA1c.
Conclusions:
Physicians play a major role in promoting higher level of satisfaction by good communication with their patients. More efforts are needed to improve certain aspects of diabetic care such as: Patient's education and periodic physical examination. Although the present study did not show any association between satisfaction and important outcome like HbA1c, more studies are needed to explore such complex relationship. To obtain more significant results a bigger sample size might be needed.
Keywords: Hemoglobin A1c, patient's satisfaction, primary care type II diabetes
Introduction
Patient satisfaction is of increasing importance and widely recognized as an important indicator of quality of the medical care. There was no homogeneous definition of patient satisfaction, since satisfaction concerns different aspects of care or settings, as well as care given by various professions.[1] Thus the interpretation of patients' satisfaction as an overall score is often difficult, but comparisons over defined dimensions of care being more appropriate.[2]
Many of studies have focused on main components including patients', physicians' and practices' characteristics, which influenced patients' ratings of satisfactions.[3] However, previous studies have not identified those factors that are most important. Moreover, in recent years, the characteristics of the external environment have been also considered as additional factors influencing individual evaluation.[4,5]
Improving the quality-of-care for patients with chronic conditions like diabetes mellitus became an important focus of the health-care system and policy.[6] The focus on diabetes mellitus was increasing because it became a major public health problem. In general, studies showed that number of adults having diabetes will be more than double between 2000 and 2030, with most increase occurring in Asia.[7] In Saudi Arabia, a recent study showed that the overall prevalence of diabetes mellitus is 30%.[8] The literature on diabetes mellitus has increasingly focused on the quality of diabetes care and its measurement. The quality-of-care is a multidimensional concept with a combination of access, effectiveness of clinical care and interpersonal care.[9] In the last years, health systems changed the way of thinking and delivering care i.e., patient became the center of the overall care process and new organizational models were applied in order to provide patient-centered services.[10]
Furthermore, the quality of diabetes care is widely sub-optimal and most of the interventions depend on active involvement and participation of patients. Thus working through patient satisfaction may be an important way of improving diabetes care.[11] Some studies have highlighted that satisfaction strongly increases when care is provided in accordance with the clinical standard procedures.[12]
Different psychosocial and behavioral hypotheses have been proposed to explain the association between patients' satisfaction and medical outcomes. Taken depression as an example, it was independently associated with satisfaction and quality-of-life, but not diabetes control.[13] Empirical findings typically suggest a positive relationship between health outcomes and satisfaction with care. Alternative theory suggested that patient satisfaction may be both a consequence and a determinant of health status.[14]
In Saudi Arabia, there was a paucity of reliable and valid satisfaction measures for specific population. Most of the studies investigated factors correlated with patients' satisfaction with primary care services.[11,15] Up to our knowledge, there were no published studies that investigated the relationship between the components of patient satisfaction and health status.
We performed this study because we felt that despite many studies looked into satisfaction and quality improvement; patients' views on the quality of their care had rarely been investigated and therefore needed further elaboration.
The objectives of this study were
To identify the underlying factors affecting patient satisfaction with the diabetes care.
To assess whether comprehensive diabetes management provided in a specialized clinic (diabetic clinic) improve satisfaction and control of type II diabetic patients.
Subjects and Methods
Study design
This cross-sectional study was conducted by using a self-administered questionnaire that measured patients' satisfaction.
Setting and participants
It was carried out in Iskan primary care center at King Abdul-Aziz Medical City (KAMC), Riyadh. This practice consisted of family medicine and primary care clinics providing primary care services for around 50,000 patients, where diabetics accounted for around 8-10%. It involved patients from diffuse social and economic background, but it mainly served National Guard employees and their families who are residing in adjacent location. It also holds a diabetic clinic, which provides comprehensive diabetes care running by family physicians 3 times a week. Patient satisfaction is compared between family medicine clinic and diabetic clinic in the same practice in order to fulfill our objectives.
Target population
Study population is type two diabetic patients who were following in Iskan clinics at KAMC. Non-probability sampling of patients who were attending their follow-up from 20th May to 15th October 2008 was included provided that they had at least one hemoglobin A1c (HbA1c) reading within the last 3 months.
Sample size
It was calculated based on the following formula:[16]
Sample size n = [DEFF * Np (1 − p)]/[(d2/Z21− α/2* (N − 1) + p * (1 − p)]
where population size 50,000, prevalence 23% and design effect 1.
A sample size of 244 patients is required at 5% significance and 95% confidence interval.
Tool
An Arabic language self-administered questionnaire was used in this cross-sectional study. It measured domains of patients' satisfaction. HbA1c level collected from patients' medical records.
Measurements of patient satisfaction
Based on the literature review various instruments have been proposed to measure patients' satisfaction in primary care. The General Practice Assessment Survey is useful and valid instrument for assessing several important dimensions of primary care.[17] Furthermore, some studies used it to measure diabetic patients' satisfaction.[14,18] Currently, it is modified to Global Physical Activity Questionnaire, which has been developed at the National Primary Care Research and Development Center at The University of Manchester for the year 2003.[19]
We constructed our own questionnaire based on selected items from several validated questionnaires such as Diabetes Treatment Satisfaction Questionnaire, General Practice Assessment Survey and Diabetes Clinic Satisfaction Questionnaire DCSQ[20,21,22] Furthermore, we developed new questions based on the published literature concerning diabetic patient's satisfaction; these items were translated into Arabic.
The cover page of the questionnaire contained instructions for the staff (assistant/nurse) as well as a brief introduction for patient.
The questionnaire consisted of four sections as listed below with the following main variables:
-
Patient's related factors
- Patient's socio-demographic.
- Co-morbid illnesses.
- Health status.
- Duration and treatment of diabetes.
-
Practice related factors
- Access.
- Continuity of the care.
- Waiting time.
- Appointment system (follow up).
-
Doctor's related factors
- Technical aspect of the care.
- Communication skills.
- Referral and coordination.
-
Satisfaction with following aspects of diabetes care
- Treatment including medication and life-style modification.
- Patient education.
- Consultation time.
- Foot care.
-
Overall level of satisfaction
Level of satisfaction concerning diabetes care was defined using a five-point likert scale: “Strongly dissatisfied,” “dissatisfied,” “neither satisfied nor dissatisfied,” “satisfied” and “very satisfied” which correspond to five, four, three, two and one point respectively. While satisfaction items about doctors and practice are scored using a sex-point likert scale: “Very poor,” “poor” “fair,” “good,” “very good” and “excellent.”
Measurement of diabetes control
It is well-known that HbA1c level has been used to monitor both the treatment and the long-term metabolic control in diabetes. It is also routinely measured in general practice and therefore is available in medical records. Moreover, plenty of studies looked at the association between level of patients' satisfaction and HbA1c. Thus, we chose HbA1c as a measure for diabetic control.[23,24,25] despite recent systematic review showed no evidence for the effectiveness of point of care testing for HbA1c in the management of diabetes.[26]
Data collection and analysis
Data were collected from patients attending their diabetes follow-up in either family medicine or diabetic clinics over a 6-months period. Subjects were identified from patient list for each consultant running either of the clinics for a particular day. Unit assistant/nurse were asked to identify patients who were having HbA1c measurement within the last 3 months through checking the lab result first or by asking particular patient if he/she did any lab works recently. If so, they were asked to fill out specific information in the questionnaire (medical record number and HbA1c level) then forward it to patient to be completed during waiting time. In case of illiterate patients the survey was administered by Arabic speaking people who were either trained unit assistants or author.
The questionnaire was discussed with him/her in order to reach consensus of asking/explaining particular question in case if patient did not understand such question.
A pilot study was carried out.
SPSS software (release 16, SPSS Inc., Chicago, U.S) was used for data entry and analysis. We used appropriate statistical test to identify the association of overall satisfaction with HbA1c level as well as other selected characteristics.
Results
A total of 230 questionnaires were distributed among patients following with family medicine and diabetic clinics. Only 195 were completed giving a response rate of ~85%.
Patient's socio-demographics
Data from 195 diabetic patients from both diabetic and family medicine clinics were analyzed. 101 (51.8%) patients were following with family medicine clinic and 94 (48.2%) were from diabetic clinic. Their ages ranged from 30 to 70 years with a mean age of 53 years. Majority of them (41.5%) aged 45-60 years. There were more females (56.9%) then males (43.1%). Majority of the population were married (80%) and illiterate (47.7%) [Table 1]. Around 86.7% were having co-morbid illnesses with dyslipidemia and hypertension being the highest among other diseases. Nearly, 38% of them were having diabetes for more than 10 years. Around half of the patients were treated with oral hypoglycemic agents. Only few patients stated that they were on diet and exercise along with medication. The mean HbA1c was 0.087 [Figure 1].
Table 1.
Socio-demographic characteristics of diabetic patients attending FM and diabetic clinics
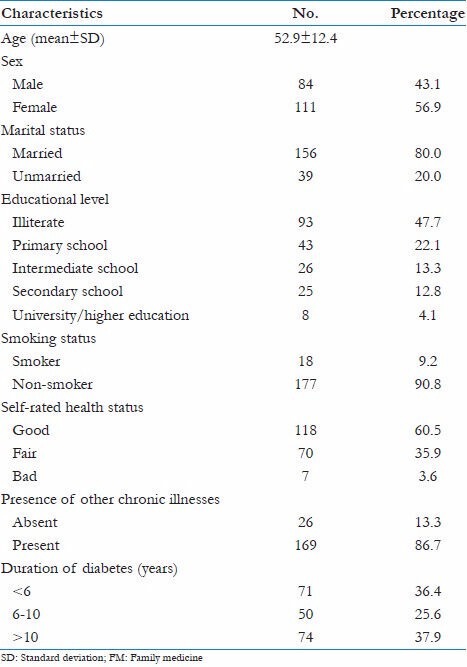
Figure 1.
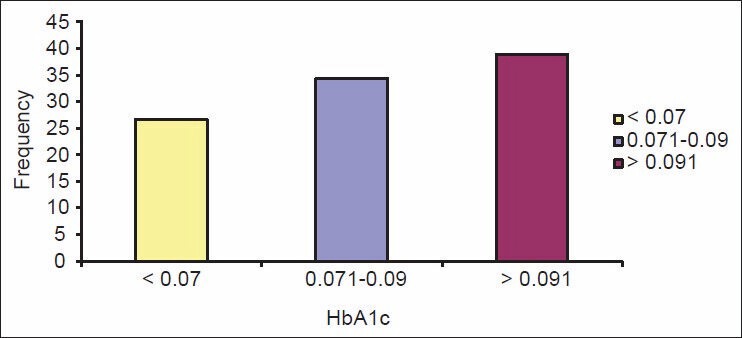
Frequency of hemoglobin A1c among diabetic patients
Practice's related factors
Nearly, 53% of patients considered the appointment system excellent. Whereas, 45% considered it good and few of them (2%) rated it as poor. When it comes to telephone access, around 55% were not able to judge on this facility mainly because they did not try it before [Table 2]. Half of the sample was visiting the practice 3-4 times/year. 22% had to wait for less than 10 min for the consultation to begun. 33% had average waiting time (11-20) minutes. Around 58% rated their waiting time as good, 24.6% considered their waiting time as excellent and 17.4% stated that it is poor.
Table 2.
Practice related factors evaluation's scale
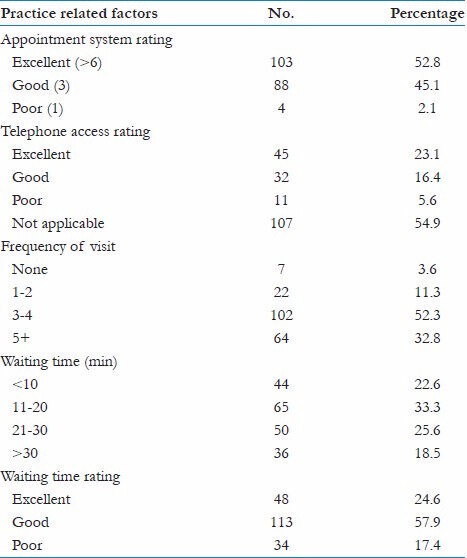
Majority of patients (84.6%) were following with a specific family physician in which 80% of them stated that they were always seen by their usual doctor, 16.4% sometimes and only 3.6% were rarely seen by the same physician.
Doctor's related factors
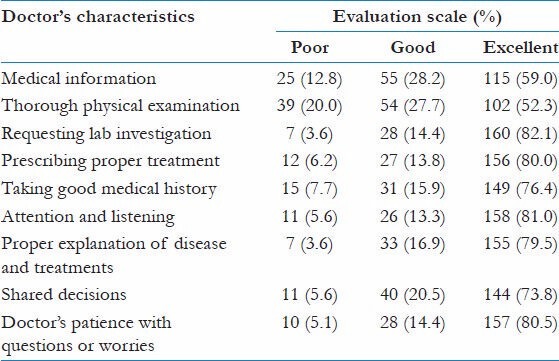
The questions aimed to assess mainly the clinical competence and communication skills of the physician [Table 3]. Majority of the patients rated their physician's skills as excellent in all aspects except for medical information and through physical examination. Upon questioning patients whether they recommended their physicians to other family members or friends: 75% answered yes, 21% were not sure and 4% they won't recommend their usual doctors.
Table 3.
Doctor's clinical competence and communication evaluation's scale
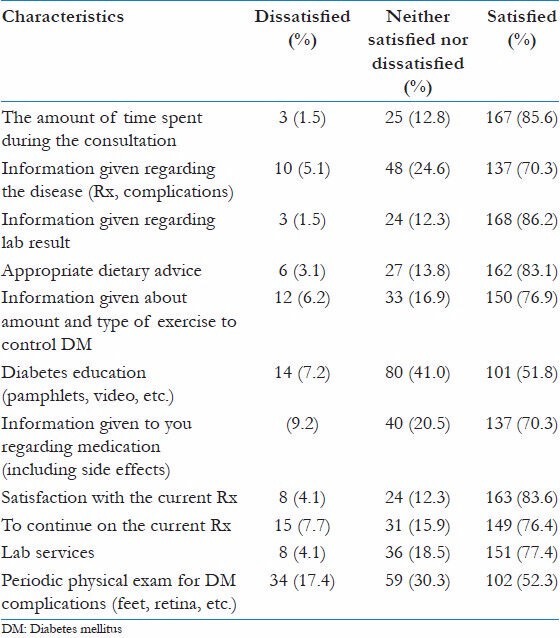
Satisfaction with diabetes care
Majority of patients (>70%) were satisfied with most of the items. Among the satisfied group, 86.2% were satisfied with the information given about their lab results. On the other hand, only half of them were satisfied about diabetes education and the periodic physical examination namely retinal and feet exam [Table 4].
Table 4.
The diabetic care evaluation scale
Overall patient's satisfaction
From the previous variables, we calculated the overall satisfaction rate, which was demonstrated in Figure 2. In this study, we investigated the outcome of diabetic care as represented by HbA1c level. The mean HbA1c level was 0.087 ± 0.020.
Figure 2.
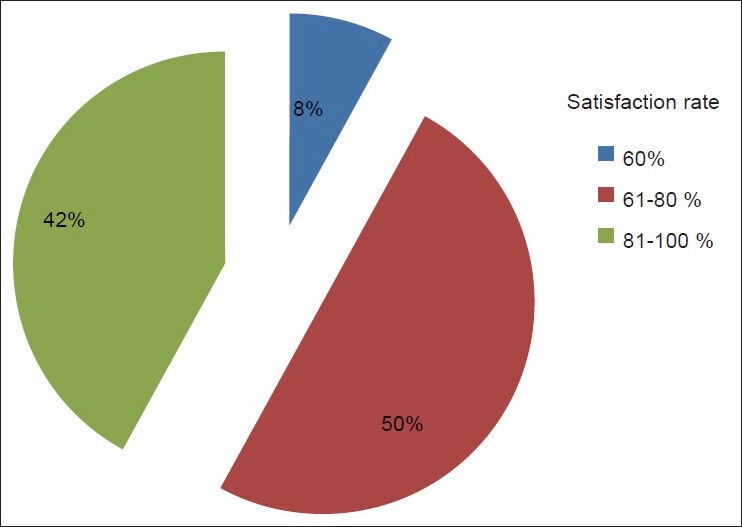
Overall patient satisfaction rate
There was no relationship between overall satisfaction and other factors such as age, sex and marital status, level of education, health status and duration of diabetes. However, overall satisfaction and clinic showed a significant association (P < 0.05). When it comes to HbA1c and overall satisfaction, analysis of regression did not show any association.
Discussion
We conducted this study to identify the underlying factors influencing diabetic patients satisfaction and to determine whether there is an association between satisfaction of diabetic patients and HbA1c as a measure of control. 220 questionnaires were collected, 25 were excluded due to missing data and duplication. Response rate 88.6% was reasonable or even higher than the response rate achieved in a similar study.[27]
Looking at patient's characteristics we observed that here were more females (56.9%) then males (43.1%). A reason which might explain this result is the fact that numbers of females are more than males in our community. Furthermore, patients who took part in this study were volunteers who agreed to be interviewed by the investigator or her assistant. Large proportions were either illiterate (47.7%) or had received average education i.e. primary and intermediate level (35.4%). Thus majority of patients were interviewed by the researcher while few of them were able to fill the questionnaires.
Nearly, 86% of patients had chronic illnesses; most of them were having more than two diseases. dyslipidemia and hypertension were the most frequent. This result had many implications as it might affect the level of satisfaction. It has been found that patients with two or more chronic illnesses reported more problems with getting the information they needed, problems with medications, difficulty obtaining answers to questions and lack of time with clinicians.[28]
Such patients reported more hassles with the health care system than those with a single chronic illness, but when communication and coordination of care increased, the patients' perception of hassle decreased and satisfaction improved.[29] In our study, we did not look for this association.
HbA1c was between 0.057 and 0.165 with mean level 0.087 ± 0.020. Only 26.7% controlled i.e. their HbA1c < 0.07%. This variation in HbA1c can be explained by multiple factors. It might be due to the natural history of disease with expected deterioration of blood glucose control. In fact 63.6% were having diabetes for more than 6 years, 38% out of them having it for more than 10 years.
Some studies had shown variation in diabetes care quality and outcome at level of patient, physician and clinic.[30] One study found that more than 95% of variance in HbA1c values was attributable to the patient level. Patient age and intensification of pharmacotherapy were related to favorable change in HbA1c.[25] In other hand, health-care professionals do not have to fear negative effects of an intensified treatment on self-rated health status, treatment satisfaction and distress.[31]
Access is considered one of the pillars of primary care. Patients were slightly more satisfied with access to family medicine (FM) clinic compared with diabetic clinic with statistical significant (P < 0.05). However, both clinic were accessible and ranked moderate satisfaction rate (65.3% and 70%) this finding was consistent with previous studies.[32] When it comes to follow up frequency, majority of patient were satisfied with follow up system. The satisfaction with 6-monthly follow-up was high.[33]
Continuity has been regarded as a crucial component of quality of care. Continuity ranked higher satisfaction level in both diabetic and FM clinics (79.8% and 80.7%) (P > 0.05).
But unlike other studies, which showed significant correlation with overall satisfaction.[32] Diabetes care can be coordinated across providers, but multidisciplinary care teams should be alert to potential coordination challenges and possible solutions including longitudinal care planning with structured communications at key points in care.
Nearly, 78% were referred to other specialties. Only 42.8% were seen by diabetic educator within a year. This might explain why diabetic education scored less satisfaction among other aspects of care. Patient education has been considered to be necessary for self-management.[1] Diabetes care can be coordinated across providers, but multidisciplinary care teams should be alert to potential coordination challenges and possible solutions including longitudinal care planning with structured communications at key points in care.[34]
Several studies have looked at patients' assessment of their physician's technical skills and the effect on satisfaction, but the findings were contradictory.[35] Communication skills ranked the highest satisfaction level among other aspect of care in both diabetic and FM clinics (86.4% and 90%) respectively. Thus, physicians can promote higher rates of satisfaction by improving the way of interaction with patients by all means with doctor-patient communication being the most important factor.[35]
All of the previously mentioned factors were contributing to the moderate and high overall satisfaction. Half of the patients had a satisfaction score of 61-80%. It was proposed that when patients were asked about satisfaction with their care, they reviewed their experiences and compared them with expectations. Experience that exceed expectations lead to satisfied patient.[36] Keeping in mind the fact that patients in general are usually positive in evaluating their general practice services and reluctant to express low satisfaction.
The relationship between the quality of diabetes care and patient satisfaction is complex and poorly understood. When it comes to HbA1c and overall satisfaction, statistical test did not show any correlation. Unlike other studies, which proved this association.[19] However, overall satisfaction and family medicine clinic showed a significant association (P < 0.05), i.e. patients attending family medicine clinic tend to be more satisfied than those patients following in diabetic clinic. Although one observational study showed no positive effect of diabetes mini-clinics another have found benefits such as better glycemic control.[37]
Recommendation
Primary care professionals involved in diabetes care may improve satisfaction by using a more patient-centered approach.
Special attention should be given for some diabetic care measures such as: Risk factor control, patient education and periodic feet/eye examination.
The clinic visits for diabetic patient should be structured proactively with concrete guidelines to optimize their care.
Patient's waiting time should be also evaluated and ideally reduced or used as an opportunity for patient education.
Bringing diabetic patients into special primary care sessions designed to meet their clinical, educational and psychosocial needs might be an effective way of improving their care and therefore improve satisfaction.
Limitations of the study
This study was carried out on the National Guard population, who shared similar background and socio-economic status. Thus results cannot be generalized.
Since most of the patients were interviewed by researcher and her assistant. We expected some patients to be reluctant in expressing low satisfaction in some of the aspects. However, at the same time, this interview assured that all questions were interpreted and understood at the same manner.
The association between the outcome of diabetes care and patient satisfaction cannot be confirmed because the study was cross-sectional.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Hornsten A, Lundman B, Selstam EK, Sandstrom H. Patient satisfaction with diabetes care. J Adv Nurs. 2005;51:609–17. doi: 10.1111/j.1365-2648.2005.03546.x. [DOI] [PubMed] [Google Scholar]
- 2.Kersnik J. An evaluation of patient satisfaction with family practice care in Slovenia. Int J Qual Health Care. 2000;12:143–7. doi: 10.1093/intqhc/12.2.143. [DOI] [PubMed] [Google Scholar]
- 3.Lubeck DP, Litwin MS, Henning JM, Mathias SD, Bloor L, Carroll PR. An instrument to measure patient satisfaction with healthcare in an observational database: Results of a validation study using data from CaPSURE. Am J Manag Care. 2000;6:70–6. [PubMed] [Google Scholar]
- 4.Stubbe JH, Brouwer W, Delnoij DM. Patients' experiences with quality of hospital care: The consumer quality index cataract questionnaire. BMC Ophthalmol. 2007;7:14. doi: 10.1186/1471-2415-7-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kollen BJ, Groenier KH, Berendsen AJ. Patients' experiences with continuum of care across hospitals. A multilevel analysis of consumer quality index continuum of care. Patient Educ Couns. 2011;83:269–72. doi: 10.1016/j.pec.2010.04.035. [DOI] [PubMed] [Google Scholar]
- 6.Gulliford MC, Naithani S, Morgan M. Continuity of care and intermediate outcomes of type 2 diabetes mellitus. Fam Pract. 2007;24:245–51. doi: 10.1093/fampra/cmm014. [DOI] [PubMed] [Google Scholar]
- 7.Herman WH, Zimmet P. Type 2 diabetes: An epidemic requiring global attention and urgent action. Diabetes Care. 2012;35:943–4. doi: 10.2337/dc12-0298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Alqurashi KA, Aljabri KS, Bokhari SA. Prevalence of diabetes mellitus in a Saudi community. Ann Saudi Med. 2011;31:19–23. doi: 10.4103/0256-4947.75773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maddigan SL, Majumdar SR, Guirguis LM, Lewanczuk RZ, Lee TK, Toth EL, et al. Improvements in patient-reported outcomes associated with an intervention to enhance quality of care for rural patients with type 2 diabetes: Results of a controlled trial. Diabetes Care. 2004;27:1306–12. doi: 10.2337/diacare.27.6.1306. [DOI] [PubMed] [Google Scholar]
- 10.Cornwell J, Goodrich J. Exploring how to enable compassionate care in hospital to improve patient experience. Nurs Times. 2009;105:15. [PubMed] [Google Scholar]
- 11.Narayan KM, Gregg EW, Fagot-Campagna A, Gary TL, Saaddine JB, Parker C, et al. Relationship between quality of diabetes care and patient satisfaction. J Natl Med Assoc. 2003;95:64–70. [PMC free article] [PubMed] [Google Scholar]
- 12.Lantz PM, Janz NK, Fagerlin A, Schwartz K, Liu L, Lakhani I, et al. Satisfaction with surgery outcomes and the decision process in a population-based sample of women with breast cancer. Health Serv Res. 2005;40:745–67. doi: 10.1111/j.1475-6773.2005.00383.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Katerndahl D, Calmbach WL, Becho J. Effect of comorbid depression on outcomes in diabetes and its relationship to quality of care and patient adherence: A statewide primary care ambulatory research and resources consortium study. Prim Care Companion CNS Disord. 2012;14 doi: 10.4088/PCC.11m01269. PCC.11m01269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Alazri MH, Neal RD. The association between satisfaction with services provided in primary care and outcomes in Type 2 diabetes mellitus. Diabet Med. 2003;20:486–90. doi: 10.1046/j.1464-5491.2003.00957.x. [DOI] [PubMed] [Google Scholar]
- 15.Saeed AA, Mohammed BA, Magzoub ME, Al-Doghaither AH. Satisfaction and correlates of patients' satisfaction with physicians' services in primary health care centers. Saudi Med J. 2001;22:262–7. [PubMed] [Google Scholar]
- 16.Dean AG, Sullivan KM, Soe MM. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version. [Last accessed 02 Mar 2014]. www.OpenEpi.com . updated 2013/04/06.
- 17.Ramsay J, Campbell JL, Schroter S, Green J, Roland M. The general practice assessment survey (GPAS): Tests of data quality and measurement properties. Fam Pract. 2000;17:372–9. doi: 10.1093/fampra/17.5.372. [DOI] [PubMed] [Google Scholar]
- 18.Campbell SM, Hann M, Hacker J, Burns C, Oliver D, Thapar A, et al. Identifying predictors of high quality care in English general practice: Observational study. BMJ. 2001;323:784–7. doi: 10.1136/bmj.323.7316.784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.GPAQ-A patient questionnaire for general practice. University of Cambridge and University of Manchester; [Last updated 25 July 2013]. Available from: http://www.medicine.manchester.ac.uk/primarycare/npcrdc archive/GPAQ_a_patient_questionnaire_for_general_practice_.htm . [Google Scholar]
- 20.Rutter CL, Jones C, Dhatariya KK, James J, Irvine L, Wilson EC, et al. Determining in-patient diabetes treatment satisfaction in the UK - The DIPSat study. Diabet Med. 2013;30:731–8. doi: 10.1111/dme.12095. [DOI] [PubMed] [Google Scholar]
- 21.Paddock LE, Veloski J, Chatterton ML, Gevirtz FO, Nash DB. Development and validation of a questionnaire to evaluate patient satisfaction with diabetes disease management. Diabetes Care. 2000;23:951–6. doi: 10.2337/diacare.23.7.951. [DOI] [PubMed] [Google Scholar]
- 22.Westaway MS, Rheeder P, Van Zyl DG, Seager JR. Interpersonal and organizational dimensions of patient satisfaction: The moderating effects of health status. Int J Qual Health Care. 2003;15:337–44. doi: 10.1093/intqhc/mzg042. [DOI] [PubMed] [Google Scholar]
- 23.Harris MI. Health care and health status and outcomes for patients with type 2 diabetes. Diabetes Care. 2000;23:754–8. doi: 10.2337/diacare.23.6.754. [DOI] [PubMed] [Google Scholar]
- 24.Redekop WK, Koopmanschap MA, Stolk RP, Rutten GE, Wolffenbuttel BH, Niessen LW. Health-related quality of life and treatment satisfaction in Dutch patients with type 2 diabetes. Diabetes Care. 2002;25:458–63. doi: 10.2337/diacare.25.3.458. [DOI] [PubMed] [Google Scholar]
- 25.O'Connor PJ, Rush WA, Davidson G, Louis TA, Solberg LI, Crain L, et al. Variation in quality of diabetes care at the levels of patient, physician, and clinic. Prev Chronic Dis. 2008;5:A15. [PMC free article] [PubMed] [Google Scholar]
- 26.Al-Ansary L, Farmer A, Hirst J, Roberts N, Glasziou P, Perera R, et al. Point-of-care testing for Hb A1c in the management of diabetes: A systematic review and metaanalysis. Clin Chem. 2011;57:568–76. doi: 10.1373/clinchem.2010.157586. [DOI] [PubMed] [Google Scholar]
- 27.Alazri MH, Neal RD, Heywood P, Leese B. Patients' experiences of continuity in the care of type 2 diabetes: A focus group study in primary care. Br J Gen Pract. 2006;56:488–95. [PMC free article] [PubMed] [Google Scholar]
- 28.Parchman ML, Pugh JA, Noël PH, Larme AC. Continuity of care, self-management behaviors, and glucose control in patients with type 2 diabetes. Med Care. 2002;40:137–44. doi: 10.1097/00005650-200202000-00008. [DOI] [PubMed] [Google Scholar]
- 29.Thiedke CC. What do we really know about patient satisfaction? Fam Pract Manag. 2007;14:33–6. [PubMed] [Google Scholar]
- 30.O'Connor PJ, Asche SE, Crain AL, Rush WA, Whitebird RR, Solberg LI, et al. Is patient readiness to change a predictor of improved glycemic control? Diabetes Care. 2004;27:2325–9. doi: 10.2337/diacare.27.10.2325. [DOI] [PubMed] [Google Scholar]
- 31.van den Donk M, Gorter KJ, Rutten GE. No negative effects of a multi-factorial, intensified treatment on self-reported health status, treatment satisfaction, and diabetes-related distress in screen-detected type 2 diabetes patients. The Addition-Netherlands study. Qual Life Res. 2010;19:509–13. doi: 10.1007/s11136-010-9604-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rao M, Clarke A, Sanderson C, Hammersley R. Patients' own assessments of quality of primary care compared with objective records based measures of technical quality of care: Cross sectional study. BMJ. 2006;333:19. doi: 10.1136/bmj.38874.499167.7C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Wermeling PR, Janssen J, Gorter KJ, Beulens JW, Rutten GE. Satisfaction of well-controlled type 2 diabetes patients with three-monthly and six-monthly monitoring. BMC Fam Pract. 2013;14:107. doi: 10.1186/1471-2296-14-107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.MacPhail LH, Neuwirth EB, Bellows J. Coordination of diabetes care in four delivery models using an electronic health record. Med Care. 2009;47:993–9. doi: 10.1097/MLR.0b013e31819e1ffe. [DOI] [PubMed] [Google Scholar]
- 35.Little P, Everitt H, Williamson I, Warner G, Moore M, Gould C, et al. Observational study of effect of patient centredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323:908–11. doi: 10.1136/bmj.323.7318.908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wolosin RJ. The voice of the patient: A national, representative study of satisfaction with family physicians. Qual Manag Health Care. 2005;14:155–64. [PubMed] [Google Scholar]
- 37.Wagner EH, Grothaus LC, Sandhu N, Galvin MS, McGregor M, Artz K, et al. Chronic care clinics for diabetes in primary care: A system-wide randomized trial. Diabetes Care. 2001;24:695–700. doi: 10.2337/diacare.24.4.695. [DOI] [PubMed] [Google Scholar]