

Abstract
Background:
Lack of evidence in literature to show low vision care enhances the reading performance in children with Multiple Disabilities and Visual Impairment (MDVI).
Aim:
To evaluate the effectiveness of Low Vision Care intervention on the reading performance of children with MDVI.
Materials and Methods:
Three subjects who were diagnosed to have cerebral palsy and visual impairment, studying in a special school were recruited for the study. All of them underwent detailed eye examination and low vision care evaluation at a tertiary eye care hospital. A single subject multiple baseline (study) design was adopted and the study period was 16 weeks. The reading performance (reading speed, reading accuracy, reading fluency) was evaluated during the baseline phase and the intervention phase. The median of all the reading parameters for each week was noted. The trend of the reading performance was graphically represented in both the phases.
Results:
Reading speed increased by 37 Word per minute, 37 Letters per minute and 5 letters per minute for the subject 1, 2 and 3 respectively after the intervention. Reading accuracy was 84%, 91% and 86.4% at the end of the baseline period and 98.7%, 98.4% and 99% at the end of 16 weeks for subject 1, 2 and 3 respectively. Average reading fluency score was 8.3, 7.1 and 5.5 in the baseline period and 10.2, 10.2 and 8.7 in the intervention period.
Conclusion:
This study shows evidence of noticeable improvement in reading performance of children with MDVI using a novel study design.
Keywords: Low vision care, multiple disabilities and visual impairment, reading performance
The reading development of children with visual impairment (VI) lags behind that of children with normal vision.[1] Studies, have documented that sensory impairments, particularly VI, occur more frequently (50-70%) among children with developmental disabilities than in the general population.[2,3,4,5] This is because many of the underlying causes of brain damage and injury such as prematurity and birth asphyxia, are known to affect the visual system.[6]
Literature has stated that “there has been increasing recognition that children with multiple disabilities and visual impairment (MDVI) constitute a distinct group with a unique set of educational needs”.[7] Reduced visual input has been proved to be the crucial factor that hinders the reading performance of children with low vision.[1] Poorer reading performance of children with low vision is mostly a matter of slower reading speed.[1]
Although there seems to be an observed agreement that children with MDVI are poorer readers and spellers than sighted children, there is no adequate evidence in literature on clinical and functional improvement through low vision care intervention among these children. An exception is the study on the usage of low vision devices among this group by McLinden et al.[7] This study attempts to look at the impact of low vision care intervention on the reading progress of children with MDVI as measured by reading speed, accuracy percentage and fluency.
Materials and Methods
Single Subject multiple baseline study design[8] was adopted to study the impact of low vision care intervention (independent variable) on the reading performance (dependent variable) of MDVI children. Three children with cerebral palsy and visual impairment, as diagnosed by neurologist who were studying in a special school in Chennai were recruited. The inclusion criteria used were,(i) children aged 05-16 years (ii) multiple disabled with visual impairment (Royal National Institute for Blindness defines MDVI in children as whose disabilities, physical, sensory, mental or behavioural, are severe in themselves and in combination with their diminished vision, to interfere with normal development or education). (iii) Best corrected visual acuity < 6/18 for distance, (iv) difficulty in reading their respective grade text book font (v) verbally able to answer questions and able to read out aloud (vi) stable general health as reported by their parents for the past 1 year. Children with the following characteristics were excluded: (i) Previous history of low vision care (ii) parental permission not received. Health record maintained by the schools were scrutinised by one of the authors and the special educators dealing with the special children were approached for reading performance of the recruited students.
The parents of the children gave written consent for their child to participate in the study. The study adhered to the Tenets of Helsinki and was carried out as per the guidelines of the Institutional Review Board of Vision Research Foundation.
All the children underwent detailed eye examination in the tertiary eye care hospital. The examination included detailed medical and ocular history, the best corrected visual acuity assessment for distance and near, refraction, accommodative responses, contrast sensitivity testing, color vision testing, visual field assessment, ocular motility testing, cover test, pupillary assessment, slit lamp biomicroscopy and detailed fundus examination. The cause for the visual impairment was documented by an ophthalmologist.
Using exact agreement method, inter-observer agreement between the researcher and the professional working with special children was calculated. This was done to ensure that the researcher assessed the subjects reading performances correctly. Agreement was calculated using the formula: Agreement Frequency/(Agreement Frequency + Disagreement Frequency) × 100 = ___%, the researcher had to demonstrate at least 80% inter-observer agreement with the professional during the training sessions when practicing with each subject before proceeding to the study.
The study had two phases, namely baseline phase and intervention phase. In both the phase reading performance (reading speed, reading accuracy and reading fluency) were measured. At the end of the baseline phase, each child underwent detailed low vision care examination to arrive at the appropriate low vision devices for the near reading performance. In order to differentiate between improvement in reading performance due to practice and maturity from low vision care, staggering the implementation time of the intervention among three subjects was done. [Fig. 1]. Therefore, the baseline period for the first subject was four weeks, for the second subject 8 weeks and for the third subject 12 weeks. The intervention phase for the first, second and third subjects were 12, 8 and 4 weeks.
Figure 1.
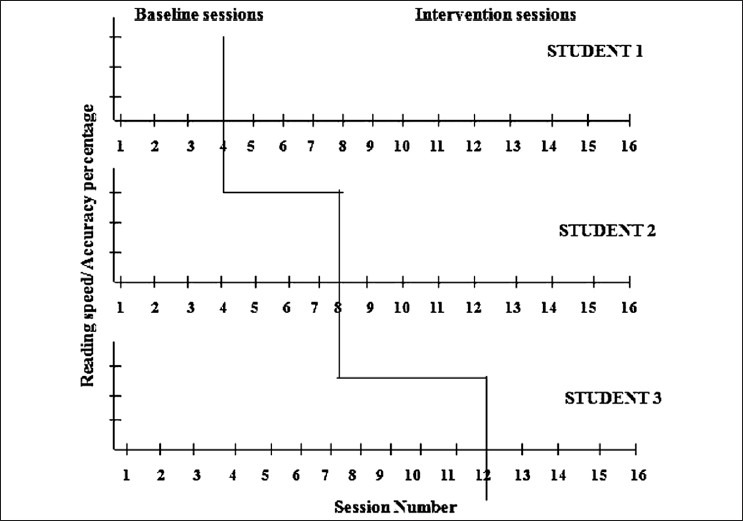
Experimental design of the study
Reading speed was calculated using the formula: Words/letters read/minute. Reading accuracy was calculated using the formula:
Total number of words/letters – number of errors × 100
Total number of words/letters
A word or letter was scored as an error each time when it was omitted, mispronounced or substituted.
Reading Fluency is an indicator that the reader is actively constructing the meaning of a passage as they read.[9] The reading fluency score was assessed using multidimensional fluency rating scale. The multidimensional fluency rating scale has seven items (enthusiasm and volume, smoothness, pace, confidence, stress, clarity, and pronunciation). The rating scale was presented to four reading experts, who rated the reading fluency of each subject individually by listening to the recordings. Out of 16 sessions of recording, 8 sessions (baseline 4, intervention 4) were rated. The total score for each item was calculated as the sum of the rating scores of 4 individuals. Hence, on a fluency scale of 1-4 for each item, the minimum score would be 4 and the maximum score would be 16.
The reading materials used were short passages for measuring reading performance and the words in each passage were different for each subject. Each passage consisted of words with continuous text. These reading passages were selected from their respective grade text books and presented in font size similar to their presenting near visual acuity when tested with the Bailey-Lovie word reading chart. The passages taken were from the lessons still not taught to them to avoid influence of familiarity of the text on reading performance.
Audio recording was done when the children were reading to reassess the observations made by the author and a digital timer was used to time all of the readings.
Each session was administered 3 days a week in order to measure and monitor their levels of reading speed, accuracy and fluency. At the end, time taken for the completion of the passage and the subject's number of words/letters read, errors made were noted on the data collection score sheet along with day and session number individually. Then reading speed and accuracy percentage were calculated. Dependent variables were recorded for each passage on all the three days and the median score was plotted for each session.
Data analysis
Graphing the single-subject data provided a compact, visual account of the effectiveness of the low vision care intervention approach in reading activities. The graphs were presented to illustrate the number of words/letters read per minute, and the accuracy percentage for each session for each baseline and intervention session readings for each subject. Graphs were drawn with sessions on X-axis and speed, accuracy percentage and fluency score individually on Y-axis. Each subject's data was shown individually. Data for single case designs were analysed in accordance with level, trend, slope and overlap.
Results
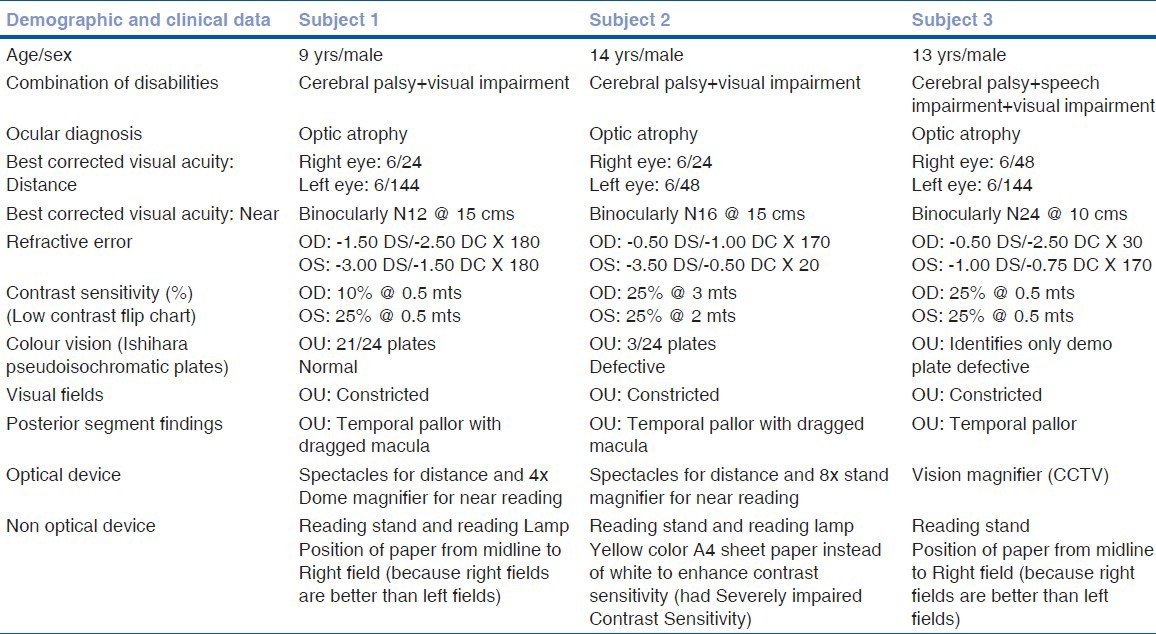
The demographic and clinical details of the three subjects are presented in Table 1. Inter-observer agreement measures were collected before the baseline phase of the study. Average inter-observer agreement for all the subjects was 93.67% (range 86-98%).
Table 1.
Clinical data of the three subjects
The trend of reading performance (dependent variable) over the baseline period and with intervention was explained for each subject individually to understand the impact of Low vision intervention on each subject.
For subject 1, the trend changed from stable to slightly therapeutic (improving reading performance) during the baseline period while it sloped down (counter therapeutic), immediate to intervention, after which it recovered and continuously showed a rising slope (therapeutic) exceeding the baseline level until the end of 16 weeks of the study period, [Fig. 2]. Subject 1's reading speed was between 65 and 72 words per minute during his baseline period. It increased to 109 words per minute at the end of 16 weeks.
Figure 2.
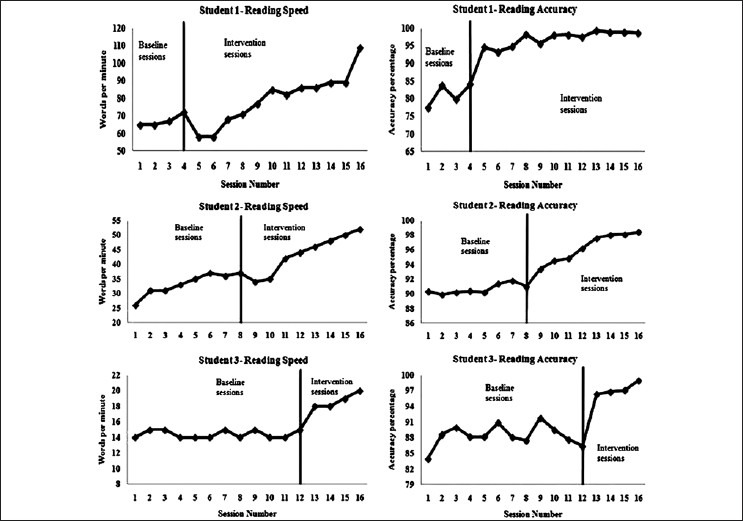
Reading speed and accuracy percentage of all the subjects over 16 sessions
For subject 2, the trend was therapeutic till 6th week and got stabilized; following intervention, it also showed negative sloping (counter therapeutic) for two weeks and the slope was rising (therapeutic) till 16 weeks time [Fig. 2]. Subject 2's reading speed was between 26 and 37 letters per minute during his baseline period which increased to 52 letters per minute over 16 sessions.
For subject 3, the baseline data was stable and no therapeutic effect was noticed. Following intervention the trend was clearly higher than the baseline level [Fig. 2]. Subject 3's reading speed was between 14 and 15 letters per minute during his baseline period. It increased to 20 letters per minute over 16 sessions.
Unlike reading speed, reading accuracy showed no significant variation in the baseline period in any of the participants. However, in the intervention phase, steep slope (therapeutic effect) was noticed which establishes the effect of low vision intervention over the reading speed [Fig. 2].
Subject 1's accuracy percentage for reading prior to intervention was between 77.5% and 84.1%. His reading accuracy climbed to 98.7% at the end of 16th week with intervention.
Subject 2's accuracy percentage for reading prior to intervention was between 90.3% and 91.0%. His reading accuracy climbed to 98.4% after 8 sessions of intervention.
Subject 3's accuracy percentage for reading prior to intervention was between 84.0% and 86.4%. His reading accuracy climbed to 99.0% after 4 sessions of intervention.
Reading fluency score of Subject 1, was 8.3 and 10.2, Subject 2, 7.1 and 10.2 and Subject 3, 5.5 and 8.7 as given by the reading experts for all the seven items (expression and volume, smoothness, pace, confidence, stress, clarity and pronunciation) on fluency scale for baseline and intervention sessions respectively.
Discussion
The results of the present study indicate that the use of low vision devices can increase the reading speed, and improve reading accuracy and fluency. However, the role of special educational approach, the motivation of the parents, teachers and the children involved, study environment and the focused care of the special educators and the parents cannot be underestimated. Studies have documented that children with low vision with or without additional disabilities are poorer readers and spellers than sighted children.[10,11] A study on reading performance in children with low vision indicated that a large majority of children with low vision can achieve reading rates that are close to those of age-matched children with normal vision when appropriate magnification was provided; and found that the reading abilities of children using low vision devices with regular print continued to increase with higher grades, whereas the reading abilities of subjects relying on large print reached a plateau.[12]
Each of the three subjects in the present study read more words/letters per minute during intervention than during baseline phase. The reason for the difference in the impact of intervention in subject 3 can perhaps be attributed to his auditory learning dependency before being recruited for thisstudy resulting in the minimum increase in the reading speed.
The reading speed graphs of subject 1 and subject 2 showed an immediate drop in speed after intervention for a period of 2 weeks. Later, both demonstrated a steady progress in reading speed. In case of subject 3, no drop in reading speed was observed but rather steady progress was demonstrated. This may be because subject 1 and 2 received dome magnifier and stand magnifier which require good handling skills while reading whereas subject 3 received an electronic device (CCTV) which does not require much handling.
The results indicate that low vision care intervention can increase levels of reading speed in children with MDVI. Though the amount of increase varied among subjects, all subjects demonstrated an improvement in levels of words/letters read both during and after intervention. The present study results provided similar evidence as seen in existing literature.[1]
With low vision care intervention there was an increased reading rate in all the three subjects in the present study. However, they did not reach the age-appropriate reading rate as reported by Lovie-Kitchin et al.[12] Several factors, including the presence of VI from birth or at early age and consequent delayed opportunity for formal education, might explain the reason for slow reading ability in this group.
Poorer reading performance of children with low vision is mostly a matter of a slower reading speed and accuracy. They are both slower and less accurate readers than sighted children.[1] Study by Douglas et al.[13] indicates that children with low vision, matched on reading comprehension and speed but accuracy appeared to show subtle differences in their reading processes when compared to normally sighted readers. The baseline sessions results of the present study also supports that children with low vision with additional disabilities are less accurate readers. There may be two explanations for this, which may well coexist. First, it might be expected that a child who has reduced visual input finds it difficult to see the print may be more prone to “guessing” a semantically appropriate word. Secondly, low vision readers may mistakenly identify words that look similar to one another in terms of their orthographic pattern.
The intervention sessions results of the present study indicate that the use of low vision devices can also increase the reading accuracy along with reading speed in children with multiple disabilities. The reading accuracy graphs showed no drop in accuracy after low vision care intervention. This may be because low vision devices help the children to see the image of the word/letter “more clearly” thereby reducing “guessing” and “confusion” of the word/letter.
Subjects had an overall improvement in reading accuracy from baseline to intervention sessions. This suggest low vision care intervention can increase accuracy from “frustration level” to “independent level”[9] and explains that subjects were able to read the assessment text or other text of similar difficulty without assistance.
It is documented in educational literature that reading fluency plays an important role in the decoding, comprehension, and motivation of readers.[9] To our knowledge there is no prior research indicating that improved visual input constraints can increase levels of subject oral reading fluency. The results of the present study indicate that the low vision care intervention can increase reading fluency when rated by the prosodic quality (expression and volume, smoothness, pace, confidence, stress, clarity and pronunciation) on a scale from 1 to 4.
Scores from the reading experts indicates that the three subjects made good progress in the reading fluency along with speed and accuracy after intervention. The results of the three subjects clearly indicated that the low vision care intervention can increase levels of oral reading fluency especially in the areas of confidence, clarity, stress and pace with the increase in reading speed and accuracy. The amount of increase varied among subjects, but all subjects demonstrated an improvement in levels of oral reading fluency during intervention.
The findings of the present study also reinforce the evidence by McLinden et al.[7] showing effective use of devices by children with multiple disabilities despite physical aspects of the child's function. The two subjects in the present study were prescribed optical devices, and the third subject was prescribed an electronic device. Optical devices included stand and a dome magnifier, and both require a good hand-eye co-ordination and handling skills compared to the electronic device.
In normal practice with multiple-baseline designs the intervention is implemented after stability has been demonstrated in baseline. In our study, we predetermined the baseline period. This was done due to time constraints of the subjects. For subject 1, the trend abruptly changed from stable to slightly therapeutic during the baseline to counter therapeutic after intervention which then recovered and exceeded baseline performance. This difference in level could indicate that control had been established to claim the impact of intervention on the reading speed. To confirm our findings, probably in future, intervention can be planned after achieving stability in the baseline. A longitudinal study to confirm the present evidence of positive impact of low vision care intervention on reading performance among MDVI subjects with a larger sample size needs to be planned.
In conclusion, this study shows evidence that low vision care intervention had a noticeable impact in improving reading performance of the three subjects with MDVI based on reading speed, accuracy and reading fluency results.
Footnotes
Source of Support: Vision research foundation, Chennai A
Conflict of Interest: None declared.
References
- 1.Gompel M, Janssen NM, Van Bon WH, Schreuder R. Visual Input and Orthographic Knowledge in Word Reading of Children with Low Vision. J Vis Impair Blind. 2003;97:273–84. [Google Scholar]
- 2.Mervis CA, Boyle CA, Yeargin- Allsopp M. Prevalence and selected characteristics of childhood vision impairment. Dev Med Child Neurol. 2002;44:538–41. doi: 10.1017/s0012162201002523. [DOI] [PubMed] [Google Scholar]
- 3.Nordmark E, Hagglund G, Lagergren J. Cerebral palsy in southern Sweden Prevalence and clinical features. Acta Paediatr. 2001;11:1271–6. doi: 10.1080/080352501317130317. [DOI] [PubMed] [Google Scholar]
- 4.Jacob N, Prabhakar A. Montréal, Canada: Proceedings of the ICEVI 9th International Conference on Low Vision 2008 July 7-11; 2008. Counting on Sight. Visual impairments among children with developmental disabilities. [Google Scholar]
- 5.Britto T, Poongothai, Mamta, Dijik KV, Jesudasan N. Children with multiple disabilities and low vision: Identification, assessment and training through low vision services in South India. Int Congr Ser. 2005;1282:42–6. [Google Scholar]
- 6.Dowdeswell HJ, Slater AM, Broomhall J, Tripp J. Visual deficits in children born at less than 32 weeks gestation with and without major ocular pathology and cerebral damage. Br J Ophthalmol. 1995;79:447–52. doi: 10.1136/bjo.79.5.447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.McLinden M, Douglas G, McCall S, Arter C. Developing Effective Practice in the Use of LVAs by Children who have Multiple Disabilities and Visual Impairment in the United Kingdom. Vis Impair Res. 2001;4:91–106. [Google Scholar]
- 8.Center DB, Leach RA. The multiple baseline across subjects design: Proposed use in research. J Manipulative Physio Ther. 1984;7:231–6. [PubMed] [Google Scholar]
- 9.Zutell J, Rasinski TV. Training teachers to attend to their subjects’ oral reading fluency. Theory Pract. 1991;30:211–7. [Google Scholar]
- 10.Gompel M, Van Bon WH, Schreuder R, Andriaansen J JM. Reading and Spelling Competence of Dutch Children with Low Vision. J Vis Impair Blind. 2002;96:435–47. [Google Scholar]
- 11.Arter C, Mason H. Spelling for the visually impaired child. Br J Vis Impair. 1994;12:18–21. [Google Scholar]
- 12.Lovie-Kitchin JE, Bevan JD, Hein B. Reading performance in children with low vision. Clin Exp Optom. 2001;84:148–54. doi: 10.1111/j.1444-0938.2001.tb04958.x. [DOI] [PubMed] [Google Scholar]
- 13.Douglas G, Grimley M, McLinden M, Watson L. Reading errors made by children with low vision. Ophthalmic Physiol Opt. 2004;24:319–22. doi: 10.1111/j.1475-1313.2004.00204.x. [DOI] [PubMed] [Google Scholar]