

Abstract
Many patients undergoing coronary angiography because of chest pain syndromes, believed to be indicative of obstructive atherosclerosis of the epicardial coronary arteries, are found to have normal angiograms. In the past two decades, a number of studies have reported that abnormalities in the function and structure of the coronary microcirculation may occur in patients without obstructive atherosclerosis, but with risk factors or with myocardial diseases as well as in patients with obstructive atherosclerosis; furthermore, coronary microvascular dysfunction (CMD) can be iatrogenic. In some instances, CMD represents an epiphenomenon, whereas in others it is an important marker of risk or may even contribute to the pathogenesis of cardiovascular and myocardial diseases, thus becoming a therapeutic target. This review article provides an update on the clinical relevance of CMD in different clinical settings and also the implications for therapy.
Keywords: Acute coronary syndromes, Coronary microvascular dysfunction, Myocardial diseases, Coronary microvascular obstruction, Stable angina
Introduction
Many patients undergo coronary angiography because of chest pain syndromes believed to be indicative of coronary artery disease (CAD). A significant proportion of such patients, however, are found to have normal-appearing coronary arteries. Several published series have reported that up to 40% of patients undergoing coronary angiography fall into this category.1
In 1985, Cannon and Epstein2 introduced the term ‘microvascular angina’ (MVA) for this patient population, in view of what appeared to be heightened sensitivity of the coronary microcirculation to vasoconstrictor stimuli associated with a limited microvascular vasodilator capacity. They proposed that dysfunction of small intramural prearteriolar coronary arteries might be the pathogenetic cause of this syndrome.3 Although there was an initial attempt to group all these patients into one category, it was soon realized that they represent a spectrum from both the pathophysiological and clinical viewpoint.
In the past 20 years, a large number of studies using both invasive and non-invasive techniques for the assessment of coronary physiology have produced a large wealth of data leading to a better understanding of coronary microvascular dysfunction (CMD) and microvascular ischaemia. Specifically, studies using positron emission tomography (PET) have permitted to establish the normal range of absolute myocardial blood flow (MBF, mL/min/g) and of coronary flow reserve (CFR, the ratio of MBF during near maximal coronary vasodilatation to baseline MBF) in healthy volunteers of different age and gender.4 The availability of normal values of MBF and CFR has allowed the investigation of coronary physiology in subjects at an increased risk of CAD and also in different categories of patients with symptoms and signs, suggestive of myocardial ischaemia despite normal coronary angiograms5 (Figure 1). Of note, chest pain syndromes with normal angiography represent a wider category including, among others, MVA.
Figure 1.

In addition to the ‘classic mechanisms’ (i.e. atherosclerotic disease and vasospastic disease) that lead to myocardial ischaemia, coronary microvascular dysfunction (CMD) has recently emerged as a ‘third’ potential mechanism of myocardial ischaemia. As in the case of the other two mechanisms, coronary microvascular dysfunction (alone or in combination with the other two) can lead to transient myocardial ischaemia as in patients with coronary artery disease (CAD) or cardiomyopathy (CMP) or to severe acute ischaemia as observed in Takotsubo syndrome. CFR, coronary flow reserve.
In 2007, Camici and Crea6 reviewed this subject and proposed original clinical and pathogenetic classifications of CMD. Accordingly, CMD was classified into four main types on the basis of the clinical setting in which it occurs: (i) CMD in the absence of myocardial diseases and obstructive CAD, (ii) CMD in myocardial diseases, (iii) CMD in obstructive CAD, and (iv) iatrogenic CMD. Furthermore, they proposed that several pathogenetic mechanisms can contribute to CMD and their importance varies in different clinical settings, although many of them may coexist in the same condition (Table 1). The molecular pathways of CMD and, in particular of, endothelial and smooth muscle dysfunction have extensively been reviewed in previous articles.7,8
Table 1.
Classification of coronary microvascular dysfunction
| Clinical setting | Main pathogenetic mechanisms | |
|---|---|---|
| Type 1: in the absence of myocardial diseases and obstructive CAD | Risk factors Microvascular angina |
Endothelial dysfunction SMC dysfunction Vascular remodelling |
| Type 2: in myocardial diseases | Hypertrophic cardiomyopathy Dilated cardiomyopathy Anderson-Fabry's disease Amyloidosis Myocarditis Aortic stenosis |
Vascular remodelling SMC dysfunction Extramural compression Luminal obstruction |
| Type 3: in obstructive CAD | Stable angina Acute coronary syndrome |
Endothelial dysfunction SMC dysfunction Luminal obstruction |
| Type 4: iatrogenic | PCI Coronary artery grafting |
Luminal obstruction Autonomic dysfunction |
CAD, coronary artery diseases; SMC, smooth muscle cells; PCI, percutaneous coronary intervention.
The aim of this article was to provide an update on CMD based on the more recent literature published on this subject.
Coronary microvascular dysfunction in patients without myocardial diseases and obstructive atherosclerosis
Risk factors
A large body of evidence supports the role of traditional risk factors with endothelial-dependent dysfunction and the adverse prognosis associated with this finding. In addition, reports indicate that abnormal non-endothelium-dependent microvascular dilatation appears to be involved in functional and structural alterations that lead to impaired CFR with aging,9 hypertension,10,11 diabetes,12,13 dyslipidaemia,14,15 and insulin resistance.16 In most of these reports, the vasodilator stimulus was adenosine, which increases blood flow mostly by non-endothelial-dependent mechanisms via receptors on microvascular smooth muscle cells that modulate intracellular calcium.17
Diabetes
It is associated with CMD not only in the heart but also in other organs such as the eye, kidney, and brain, so deserves specific mention. Chronic hyperglycaemia is associated with significantly reduced endothelial-dependent and endothelial-independent coronary vasodilator function.18 Further evidence implicates insulin resistance or hyperinsulinaemia,19 and interventions aiming at improving insulin sensitivity have been shown to improve endothelial function and decrease myocardial ischaemia in patients with no obstructive atherosclerosis.20 However, other studies demonstrate that hyperinsulinaemia or insulin resistance are not associated when other confounding factors are excluded.21
Chronic inflammation
It is a relatively novel risk factor of increasing importance. High levels of C-reactive protein, as a marker of low-grade chronic inflammation, have been found associated with increased frequency of ischaemic episodes, detected by ambulatory electrocardiogram (ECG) in patients with MVA,22 suggesting a role for inflammation in the modulation of coronary microvascular responses in these patients.
Accordingly, a high prevalence of CMD has recently been described in patients with systemic lupus erythematosus and rheumatoid arthritis,23,24 characterized by an inverse correlation between CFR and C-reactive protein concentrations, thus confirming that chronic inflammation may contribute to microvascular abnormalities.25
Other risk factors
Overall, risk factors were associated with CMD, but accounted for <20% of the observed variability in the WISE study.26 Therefore other, as yet unidentified, factors must primarily account for non-endothelial-dependent CMD. Promising candidates include, but are not limited to, disorders of nitric oxide metabolism, dysregulation of numerous mediators including inflammatory cytokines, oestrogen, or adrenergic receptors, and alterations in the expression or production of local vasoactive substances such as angiotensin II and endothelin.27
Microvascular angina
As noted above, up to 40% of patients with signs and symptoms of ischaemia undergoing coronary angiography do not have obstructive atherosclerosis.1,28 Following exclusion of non-coronary causes of chest pain, the presence of coronary vascular dysfunction, ischaemia on stress testing, and chest pain persisting at 1 year of follow-up identify a subgroup at higher risk for adverse clinical outcomes.29 Estimates from the WISE database show that there are at least 3–4 million patients in the USA alone with signs and symptoms of ischaemia despite no evidence of obstructive atherosclerosis,30,31 with associated poor quality of life, psychological distress, and health-care costs that approximate those of patients with obstructive CAD. These contemporary data indicate that we should use the terms ‘coronary microvascular dysfunction’ and ‘microvascular angina’ for these patients rather than ‘angina with normal coronary arteries’. An illustrated model of CMD in the absence of obstructive atherosclerosis is shown in Figure 2.
Figure 2.

Scheme of the potential causes and consequences of coronary microvascular dysfunction. HC, hypertrophic cardiomyopathy.
While prior studies failed to demonstrate CMD and myocardial ischaemia in this population,32 contemporary studies using sensitive measures of ischaemia have documented that the majority of patients with angina and ST segment depression during exercise stress test exhibit regional myocardial underperfusion33 and signs of ischaemia.34,35 Accordingly, pathophysiological studies have documented frequent coronary endothelial and non-endothelial coronary dysfunction in patients with signs and symptoms of ischaemia despite the lack of obstructive atherosclerosis,36 consistent with CMD. In 1991, Maseri et al. proposed that the abnormality may not involve all coronary microvessels of a major coronary branch uniformly, but may be distributed in the myocardium in a scattered manner. This distribution of perfusion abnormalities can provide a plausible explanation for the difficulties in obtaining objective evidence of myocardial ischaemia in most MVA patients when standard diagnostic methods are used. Indeed, a sparse distribution of myocardial ischaemia, although sufficient to produce ECG changes and also myocardial perfusion scintigraphic defects, may not result in detectable contractile abnormalities because of the normal function of the surrounding myocardial tissue. Similarly, the release into the coronary sinus of ischaemic metabolites by the sparse myocardial ischaemic foci can go undetected because of their dilution in the larger flow from normal myocardial areas.37
Patients with MVA have been considered ‘low risk’.38 Although this issue remains controversial, invasive angiographic data demonstrate that this group includes a spectrum of patients, more frequently women, at higher risk of adverse cardiac events.39 The WISE study at 5.4-year follow-up demonstrated adverse events including cardiac death (53% being sudden cardiac death), stroke, and new onset heart failure rather than myocardial infarction, in particular in women with reduced CFR assessed by adenosine.40 Recent studies based on invasive or non-invasive coronary angiography have confirmed the observation of a relatively higher prevalence in women, and extended previous findings showing a higher mortality, although they included patients with angina and normal coronary arteries without systematic exclusion of patients with non-coronary causes of chest pain.41
While the relationship between CMD and epicardial atherosclerosis is not fully understood, it has been proposed that it is a single disease process, where response to intimal atherosclerotic injury may vary related to sex differences in vascular remodelling and vascular reactivity, thereby preferentially impacting women.42,43
Stable microvascular angina
Chest pain presentation is often reported by clinicians to differ in women with ‘normal’ angiograms. Although data from the WISE study indicate that typical vs. atypical angina does not discriminate between obstructive and non-obstructive coronary disease in a population of women undergoing coronary angiography,44 there is often a variable threshold of physical activity that provokes angina in MVA, low heart rate activities such as mental arousal, or palpitation are more common triggers than in patients with obstructive atherosclerosis. Furthermore, in MVA, chest pain typically persists for several minutes after interrupting efforts and/or shows poor or slow response to short-acting nitrates.45 Another feature which helps in the differential diagnosis is the response of ECG exercise stress testing to sublingual nitrates. Indeed, while the results of the test typically improve after sublingual nitrates in patients with obstructive atherosclerosis, they remain unchanged or may even worsen in patients with MVA.46
Chest pain persisting for many years after angiography in women with apparently ‘normal’ coronaries is associated with future development of coronary atherosclerosis and an adverse prognosis.47
Reduction of CFR assessed non-invasively using PET,48 cardiac magnetic resonance (CMR),49 or transthoracic Doppler echocardiography50 can be useful for diagnosis. Furthermore, angina and ST segment depression in the absence of regional wall motion abnormalities during adenosine or dipyridamole echo-stress represent a distinctive feature of MVA.51 Perfusion imaging studies have documented that about half of patients with chest pain have reduced CFR in the absence of obstructive CAD.52 Resolution of chest pain spontaneously or with drugs is associated with improvement of microvascular function.53
Currently, invasive coronary vasomotor testing remains the gold standard for the diagnosis of CMD, has a described risk/benefit safety record,28,54 and is associated to a worse outcome.55 Diffuse coronary artery spasm pronounced in the distal epicardial coronary arteries and probably extending into the microvasculature may be provoked by intracoronary injection of acetylcholine in a substantial proportion of patients with MVA. Acetylcholine, in solution in 37°C physiological saline (concentration adjusted to obtain 5 mL of solution volume for each quantity of acetylcholine), should be injected in sequential doses (20, 50, and 100 μg into the left coronary artery and 20 and 50 μg) over a period of 20 s. Doses of acetylcholine should be given at 5-min intervals. Coronary angiography should be performed 1 min after the start of each injection. Angiography should be performed immediately in the event of an ischaemic change on the ECG or chest pain. Nitrates should always be administered at the end of the tests or after documentation of distal spasm.56
Unstable microvascular angina
‘Normal’ coronary angiograms, defined as luminal narrowing <50%, are reported relatively frequently in patients with acute coronary syndrome (ACS), including 10–25% of women when compared with 6–10% of men.57 Ongoing investigation is addressing the paradox whereby women have less obstructive CAD and less severe myocardial infarctions, yet worsening clinical outcomes. The higher mortality compared with men has been attributed to advanced age, co-morbidity,58 and underutilization of guideline care among women;59 yet, the largest mortality gap is seen in younger women with a number of studies demonstrating persistent sex differences despite covariate adjustment.60
Takotsubo syndrome
Coronary microvascular dysfunction may be involved in apical ballooning syndrome, also known as stress-induced or Takotsubo syndrome. By definition, patients with Takotsubo syndrome do not have obstructive CAD, yet they demonstrate abnormal myocardial perfusion,61 abnormal CFR measured by echocardiography,62 and abnormal PET imaging, consistent with an inverse perfusion/metabolism mismatch.63 Myocardial perfusion, contractility, and left ventricular function improve markedly with the administration of intravenous adenosine in patients with Takotsubo syndrome, but not in those with acute myocardial infarction,64 while patients with a history of Takotsubo syndrome demonstrate cold pressure test-induced wall motion abnormalities.65 Furthermore, a long-term follow-up study demonstrated reduced endothelial-dependent response to acute mental stress in patients with a history of Takotsubo syndrome.66 Taken together, these observations suggest that the syndrome is caused by intense microvascular constriction with subclinical CMD persisting over time, perhaps facilitated by endothelial dysfunction.
Coronary microvascular dysfunction in myocardial diseases
Hypertrophic cardiomyopathy
Myocardial ischaemia, due to severe CMD, is an established pathophysiological feature in hypertrophic cardiomyopathy (HCM) and may be associated with important disease-related complications that impact clinical outcome.67 Marked structural abnormalities of the small intramural coronary arteries, including medial hypertrophy, intimal hyperplasia, and decreased luminal size, are considered the most relevant substrate producing CMD and myocardial ischaemia in HCM.6 Patients with HCM and demonstrable sarcomere myofilament mutations are characterized by more severe CMD and increased prevalence of myocardial fibrosis, compared with genotype-negative individuals.68
There is now evidence that late gadolinium enhancement (LGE), as visualized by CMR, is representative of myocardial fibrosis in HCM.69 The majority of patients demonstrate areas of LGE, and the incidence of fibrosis was found to increase significantly across quartiles of end-diastolic wall thickness.70 These findings suggest that CMD over time may lead to recurrent ischaemia and myocyte death, thus acting as a localizer of replacement fibrosis71 (Figure 3). This has important clinical implications for long-term outcome in HCM patients; indeed, in one-third of the patients, the clinical course is progressive and disabling, leading to chronic limiting symptoms and complications such as atrial fibrillation and stroke, and ultimately causing heart failure-related death.72 In this subgroup, consistent evidence points to CMD as a critical determinant of clinical progression and adverse outcome.
Figure 3.

Proposed cascade of events in hypertrophic cardiomyopathy, from abnormal coronary arteriolar remodelling leading to myocardial ischaemia, fibrosis and adverse left ventricular remodelling, and heart failure.
Accordingly, a recent meta-analysis in over 1000 HCM patients has shown that LGE significantly correlates, at an average follow-up of >3 years, with the development of heart failure and with all-cause and cardiac mortality, with a trend towards significance also for the prediction of sudden death.73 Based on these studies, extensive LGE at CMR is now considered among the features that indicate an increased risk of sudden death in HCM, together with the classical predictors including a family history of sudden death, unexplained syncope, LV wall thickness of >30 mm, recurrent episodes of non-sustained ventricular tachycardia during ambulatory ECG monitoring, and hypotensive response or attenuated increase in blood pressure during exercise.74
Dilated cardiomyopathy
It has previously been assumed that myocardial ischaemia does not play a role in the pathogenesis of DCM, because a pre-requisite for the diagnosis of idiopathic DCM is the absence of significant epicardial CAD.75 Yet, subsequent studies have not only shown that MBF abnormalities occur even in the early stages of the disease, but also that myocardial ischaemia attributable to CMD may have an independent role in the progression of the disease.76 Although MBF abnormalities were initially attributed to extravascular mechanisms as the result of left ventricle (LV) dysfunction, structural abnormalities of the vessels and reduced capillary density, in conjunction with the abnormal endothelial function that is frequently observed in these patients, can contribute to decreased hyperaemic MBF.77
As in patients with HCM, the degree of CMD has been shown to be an independent predictor of cardiac events and is associated with an increased risk of sudden death and further progression of heart failure.78 Of note, early data suggest that LGE, reflecting the presence of fibrotic areas possibly secondary to CMD, may have a relevant prognostic value in dilated cardiomyopathy, although this hypothesis needs confirmation in larger studies.79
Myocarditis
Recent studies have shown that parvovirus B19 and human herpesvirus 6 are the most common pathogens of viral myocarditis,80 and that the clinical presentation of patients with myocarditis can be related to the type of virus present in the myocardium.81 Patients with myocardial parvovirus B19 infection, indeed, seem to mainly present with chest pain, whereas those with myocardial herpesvirus 6 infection or combined parvovirus B19/herpesvirus 6 infection seem to mainly show symptoms of heart failure. It is known that endothelial cells represent specific targets in parvovirus B19-associated myocarditis probably through blood group P antigen.82 Thus, a causal relationship between parvovirus B19-related myocardial inflammation and/or infection of vascular endothelial cells and CMD can be suspected. In addition, myocardial inflammation in response to viral infection was found to be associated with increased endothelial expression of human leucocyte antigen system and adhesion molecules, and to be correlated with systemic endothelial dysfunction. Taken together, these findings suggest that symptoms of chest pain in patients with parvovirus B19-associated myocarditis without significant CAD may be caused by intense coronary vasoconstriction, as a result of myocarditis-induced coronary endothelial dysfunction and/or direct infection of endothelial cells and/or smooth muscle cells. Severe vasoconstriction/spasm of microcirculation might contribute to explain ST-segment elevation in some patients, which can result from sufficiently diffuse subepicardial or transmural myocardial ischaemia.83,84
Aortic stenosis
Angina episodes are reported by about half of the patients with a severe degree of aortic stenosis, and this occurs despite the evidence of normal epicardial coronary arteries at angiography.85 Of note, the appearance of angina greatly increases the risk of sudden death, when compared with that of asymptomatic patients.86
Coronary flow reserve is reduced in aortic stenosis87 due to a combination of mechanisms, including: (i) reduced time of diastolic coronary filling; (ii) increased LV diastolic filling pressure and intramyocardial pressure during diastole, both contributing to impairment of perfusion selectively in the subendocardium;88 (iii) reduced capillary density;89 (iv) a low coronary perfusion pressure when compared with intra-cavitary pressure; and (v) increased intramyocardial systolic pressure and delay in myocardial relaxation at the end of systole, which further reduces time of coronary filling and perfusion.
Post-mortem studies have confirmed capillary rarefaction in aortic stenosis while, in contrast with hypertension and HCM, they failed to find additional structural alterations, which can cause CMD like medial hypertrophy or perivascular fibrosis.90
Recent studies in patients with aortic stenosis, based on the measurement of MBF by PET, have shed new light on the mechanisms of CMD. Resting total left ventricular MBF has been found to increase proportionally with left ventricular mass. As this occurs in spite of vascular rarefaction, it is likely that the increase in resting MBF is mainly sustained through metabolic vasodilatation in response to the increased myocardial oxygen demand. This is responsible for a partial exhaustion of the autoregulatory capacity of the coronary microcirculation and, therefore, contributes to limit CFR. These studies have also confirmed the experimental observation that subendocardial perfusion is severely reduced and have shown that the reduction of CFR is strictly related to aortic valve area, to haemodynamic load on the left ventricle, and to the reduced diastolic perfusion time rather than to the increase in left ventricular mass.91
Infiltrative diseases
The role of CMD in infiltrative cardiac diseases is discussed in Supplementary material online.
Coronary microvascular dysfunction in obstructive atherosclerosis
Stable coronary artery disease
Several lines of evidence suggest that the direct relationship between chronic obstructive coronary atherosclerosis and angina may represent an overly simplified view. Indeed, many patients with angina and evidence of myocardial ischaemia do not have detectable coronary atherosclerosis at angiography, as highlighted in the section on MVA. Conversely, a number of patients with severe coronary atherosclerotic obstructions do not experience angina. Accordingly, in a recent study, about half of the consecutive patients with an ACS as first manifestation of CAD undergoing coronary angiography exhibited a multivessel disease.92 This observation strongly suggests that pre-existing obstructive CAD had been silent probably because preserved microvascular function and, more importantly, adequate collateral development prevented angina and ischaemia in spite of obstructive CAD.
The ‘plaque-centric’ hypothesis can also be called into question when the impact of therapeutic strategies based on the removal of coronary atherosclerotic obstructions is considered. Most reports agree that, on a background of medical therapy, revascularization improves symptoms, but in many patients angina recurs after 2–3 years while myocardial infarction and death are not prevented, as clearly shown in a recent comprehensive meta-analysis.93
These observations certainly do not deny the usefulness of revascularization in patients with ACS, when coronary revascularization is needed to prevent an impending catastrophe, but they do raise questions about whether revascularization should continue to be regarded as the ultimate treatment for obstructive atherosclerosis in stable patients. Thus, in patients with stable angina who do not have a large area at risk of myocardial ischaemia, the main goal of treatment remains global risk factor control and anti-anginal treatment possibly targeting both large epicardial coronary arteries and coronary microcirculation.
Acute coronary syndromes
The temporal association between events occurring in large epicardial vessels (plaque erosion or fissure associated with thrombus formation) and in the microcirculation (paradoxical vasoconstriction) does not allow to establish what is the causal relation between these two events. It is widely believed that epicardial events precede and cause microvascular events. A more extreme view is that, at least in a proportion of patients, a primary CMD might play a causal role in determining thrombus formation in epicardial coronary arteries. Several lines of evidence support this working hypothesis which has recently been proposed by Lerman et al.94
In the setting of ST elevation myocardial infarction (STEMI), a specific pathophysiological condition is represented by CMD, which occurs after successful recanalization of the infarct-related artery. Prompt referral for mechanical reperfusion by urgent primary percutaneous coronary intervention (PCI) represents the pivotal step in the current management of STEMI.95 Yet, in a sizable proportion of patients, primary PCI achieves epicardial coronary artery recanalization, but not myocardial reperfusion, a condition known as ‘no-reflow’ and currently more commonly defined as microvascular obstruction (MVO).96
In 1993, at the climax of the thrombolytic era, Lincoff and Topol97 wrote a provocative editorial wondering whether reperfusion was just an illusion. At that time, they estimated that only ‘25% or less’ of patients treated by thrombolysis had an optimal reperfusion, defined as a rapid, complete, and sustained coronary recanalization with adequate myocardial tissue perfusion. What is this figure after 15 years at the climax of primary PCI era? A reasonable estimate of the proportion of patients who get optimal myocardial reperfusion, among those without cardiogenic shock undergoing primary PCI, is ∼35%.98,99
A series of consistent data have clearly shown that MVO has a strong negative impact on outcome, negating the potential benefit of primary PCI.100,101
In man, MVO is caused by the variable combination of four pathogenetic mechanisms: (i) distal atherothrombotic embolization; (ii) ischaemic injury; (iii) reperfusion injury; and (iv) individual susceptibility of coronary microcirculation to injury.
The notion that the susceptibility of coronary microcirculation to injury varies in different patients is supported by the observation that in man, MVO is occasionally observed during elective percutaneous coronary procedures,102 while it can be absent following primary PCI carried out several hours after coronary occlusion. Predisposition may be acquired and/or genetic. In particular, diabetes has been associated with impaired microvascular reperfusion after primary PCI, and hypercholesterolaemia in animal models aggravates reperfusion injury by enhancing endothelial oxidative stress.103,104 Of note, ischaemic pre-conditioning appears to have a beneficial effect on microvascular function.105 With regard to genetic predisposition, the 1976T>C polymorphism of the adenosine 2A receptors gene was suspected to be associated with a higher prevalence of MVO, but this working hypothesis has never been proved.
Iatrogenic coronary microvascular dysfunction
Percutaneous interventions
The clinical relevance of distal embolization following PCI and resulting in CMD is considerable. In a recent comprehensive meta-analysis, Testa et al. have assessed the occurrence and prognostic impact of troponin (Tn) elevation in patients with normal baseline levels undergoing PCI. Tn elevation after PCI occurred in about one-third of patients. At 18-month follow-up, peri-procedural Tn elevation was associated with a 50% increased risk of subsequent major cardiovascular events, a two-fold increased risk of death, a three-fold increased risk of myocardial infarction, and a 50% increased risk of re-PCI.106
It is only possible to speculate as to why peri-procedural myocardial necrosis marker elevations influence long-term mortality. One potential mechanism may be related to the myocardial damage per se, which might lead to increased mortality as a result of electrical instability or of persistent myocardial ischaemia associated with CMD. Alternatively, raised necrosis marker levels after PCI may signal a more active atherosclerotic process associated with an adverse prognosis due to a higher risk of cardiovascular events.
Finally, there is evidence that, in patients with stable CAD and exercise inducible ischaemia undergoing elective PCI, CFR does not recover immediately after the procedure despite successful recanalization, suggesting persistent functional CMD as elegantly demonstrated by Uren et al.107 by PET.
Surgical interventions
Surgical trauma and cardiopulmonary bypass contribute to a systemic inflammatory response, measurable by circulating cytokines, which promotes CMD.108,109 This can be the result of many factors, including contact of blood with the bypass circuit, myocardial ischaemia during bypass, aortic cross clamping, and reperfusion injury. Perioperative myocardial infarction results in further elevation of inflammatory markers.110,111 Spyrou et al. measured MBF and CFR in patients undergoing coronary artery bypass grafting (CABG) using PET. They found that hyperaemic MBF and CFR improved progressively over the 6 months following CABG, suggesting persistent CMD that recovers slowly after surgery.112
One study using LGE at CMR imaging and TnI measurement found that about one-third of the patients undergoing CABG had new myocardial infarction demonstrated by CMR, and that a cut-off of TnI of 5 µg/L (upper normal limit of 0.6 µg/L) at 1 h had 67% sensitivity and 79% specificity for detecting the new infarction. In this study, the predictive value of creatin kinase-myocardial band (CK-MB) for the diagnosis of myocardial infarction was lower than that of TnI: using a cut-off of CK-MB of 25 µg/L (upper normal limit of 4.8 µg/L) at 1 h had 44% sensitivity and 89% specificity for detecting the new infarction.113 Substantial biomarker elevations after CABG have been shown to have significant prognostic implications.114
The fact that different mechanisms of injury following PCI and CABG have similar prognostic implications suggests that patient prognosis is eventually driven by the extent of necrosis regardless of the mechanisms responsible for its occurrence.
The prognostic impact of myocardial damage following CABG, assessed by enzyme elevation, is clinically relevant. Indeed, post-procedural enzyme elevation is a potentially important surrogate endpoint for clinical trials. Also of significance is the potential use of these enzyme elevations as a measure of procedure quality, including the comparison of different centres and even of individual operators. Important in this regard will be standardizing the post-procedure time when enzyme levels should be determined. Future effort should be directed to achieving a better understanding of the mechanisms that contribute to procedural myocardial necrosis, particularly those that are under the control of the operator and thus potentially amenable to easy correction.
Treatment of coronary microvascular dysfunction
Coronary microvascular dysfunction in the absence of myocardial diseases and obstructive coronary artery disease
Neglia et al. using PET demonstrated that hyperaemic MBF and CFR were significantly improved in patients with hypertension and left ventricular hypertrophy following treatment with perindopril and indapamide for 6 months, suggesting reverse remodelling of intramural arterioles. The latter hypothesis has been confirmed in an ancillary study in spontaneously hypertensive rats, where the same drugs improved coronary flow and histology provided evidence of significant reverse remodelling of coronary arterioles.115
In patients with MVA, a first important line of treatment is represented by life style modification such as smoking cessation and weight-loss, which are known to improve endothelial dysfunction and CMD, and should therefore be strongly encouraged.116 Notably, the proven benefit of exercise training in this population117 suggests that adrenergic modulation may play an important role. Furthermore, statins and angiotensin converting enzyme (ACE) inhibitors, in hypertensive patients, which improve endothelial dysfunction, should represent a first line of treatment in patients with MVA.118,119
Much of the evidence of treatment in patients with CMD, however, has focused on improvement in symptoms. Many anti-ischaemic therapies have been evaluated including data that calcium antagonists do not improve CFR and show inconsistent effects on symptoms,120 while beta-blockers are effective for improving chest pain symptoms.121 No controlled studies are available on the effects of long-acting nitrates on health status outcomes, while the efficacy of sublingual nitrates seems less consistent than in patients with obstructive CAD.122
A small trial in women with CMD demonstrated angina improvement measured by the Seattle Angina Questionnaire on ranolazine compared with placebo as well as trends towards improvement in myocardial perfusion abnormalities by CMR imaging.123 In a more recent study, ranolazine improved both angina status and exercise stress test results in patients with MVA, when compared with ivabradine or placebo.124
The beneficial effects of xanthines in MVA can be related to two different mechanisms.125,126 First, xanthines inhibit the arteriolar dilator effects of adenosine, through antagonism of vascular A2 receptors on smooth muscle cells thus favouring CBF redistribution towards myocardial areas with CMD.127 Secondly, xanthines might exhibit an ‘analgesic’ effect, as they antagonize the stimulation of cardiac nerve pain fibres by adenosine, which is a major mediator of ischaemic pain.128 Nicorandil, a nitrate and adenosine triphosphate sensitive potassium channel agonist, has been shown to improve peak exercise capacity, but failed to significantly improve exercise-induced ST changes.129
Alpha antagonists, such as doxazosin block alpha-mediated vasoconstriction, have not been shown to improve angina, exercise duration, or ischaemia by ECG.130 The rho-kinase inhibitor, fasudil, has been shown to prevent acetylcholine-induced ischaemia in these patients.131
Other therapies have been evaluated in women without obstructive CAD. Imipramine improves symptoms in patients with abnormal cardiac pain perception and normal coronary angiograms; possibly through a visceral analgesic effect. Imipramine also has anticholinergic and alpha antagonist effects demonstrated in both the coronary and peripheral circulation.132 Menopausal hormone therapy may improve emotional well being in postmenopausal women with angina and ‘normal’ angiograms; yet, there is no symptom benefit for these patients.133
Finally, more demanding forms of treatment are spinal cord stimulation134 and enhanced external counterpulsation.135
Figure 4 summarizes the proposed treatment algorithm for patients with MVA. All patients should receive optimal risk factor control. If symptoms are not well controlled, addition of traditional and non-traditional anti-ischaemic drugs is recommended. In patients in who enhanced pain perception is suspected drugs which modulate pain perception are indicated. Interventions like spinal cord stimulation, enhanced external counterpulsation, and cognitive behavioural therapy should be reserved to patients with refractory symptoms, which seriously limit life quality.
Figure 4.
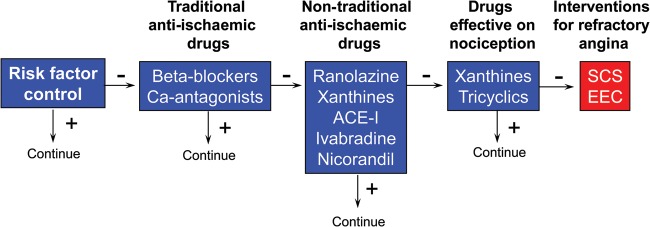
Treatment algorithm for patients with microvascular angina. SCS, spinal cord stimulation; EEC, enhanced external counterpulsation.
Developing strategies to provide effective prevention and treatment of CMD and angina is urgently needed. Appropriately powered, randomized, outcome trials testing management strategies have not been conducted in the ‘at-risk’ population. Existing guidelines focus on symptom management and current clinical practice on ‘reassurance’. This appears to be insufficient because ischaemia-related symptoms frequently recur and these patients incur in relatively large health-care costs, in addition to the major adverse cardiac events. Large-scale, practical, outcome trials testing the efficacy of currently available traditional anti-atherothrombotic and anti-ischaemic therapy, as well as novel therapies in this population, are warranted.
Coronary microvascular dysfunction in myocardial diseases
Although CMD has been demonstrated and might play a pathogenetic role in most myocardial diseases, studies specifically assessing the effect of therapy on CMD are largely lacking.
In HCM, alcohol septal ablation seems to improve CFR and septal endocardial-to-epicardial MBF,136,137 while verapamil, disopyramide, and ACE inhibitors fail to improve myocardial perfusion.138–141
In patients with dilated cardiomyopathy, beta-blockers142,143 but not calcium antagonists or ACE inhibitors144 seem to have beneficial effects on CMD, likely as a result of improved haemodynamics. Of note, favourable effects on CMD have recently been reported by treatment with allopurinol.145
While CMD can be present and play an important role in the clinical presentation of acute myocarditis, no study has hitherto assessed the effects of any form of intervention on CMD in these patients. Thus, consequences of treatment and their clinical implications remain undefined.
As discussed above, a short diastolic time plays a significant role in causing reduction of CFR and angina in patients with aortic stenosis. Thus, drugs that increase diastolic time, like beta-blockers, might help in delaying the ominous onset of myocardial ischaemia and angina in these patients. As an alternative, in case of contraindication or intolerance to beta-blockers, ivabradine, known to selectively reduce heart rate but not blood pressure, might be of help in this setting. These considerations, however, are purely speculative, as clinical studies about the effects of these drugs on coronary microvascular perfusion and on angina and clinical outcome are lacking and should therefore be investigated in prospective randomized trials.
The treatment of infiltrative cardiac diseases is discussed in Supplementary material online.
Coronary microvascular dysfunction in obstructive coronary artery disease
Therapeutic interventions able to promote collateral growth may have an impact on outcome and also on symptoms in patients with refractory angina, i.e. those who are judged not to be candidates for revascularization procedures.
Several forms of therapy have been proposed to promote angiogenesis and collateral circulation,146 but their role still waits to be definitely clarified.
Gene therapy initially appeared as the most valid approach to stimulate and enhance microcirculation and collateral growth in refractory angina, but controlled randomized studies have on the whole been disappointing with no or negligible benefit on symptoms and myocardial ischaemia, when compared with control groups.147 More recently, attempts to promote collateral circulation in patients with refractory angina have been based on the intramyocardial administration of progenitor vascular cells.148 The early clinical results, although promising, do not allow to establish firm conclusions about the efficacy of these form of therapy, which needs to be addressed in larger studies.
In the setting of ACS, an important, largely unmet therapeutic need is the prevention of MVO after primary PCI. Distal embolization of thrombus and debris material has been suggested to play a major role. Accordingly, two small randomized studies149,150 found a beneficial effect of manual thrombus aspiration vs. the standard procedure on surrogate endpoints of myocardial reperfusion. Then, in a medium-sized trial, patients undergoing primary PCI were randomized to thrombus aspiration or standard treatment; thrombus aspiration was associated with a significant reduction of major cardiac events (death/re-infarction) at 12 months.151,152 This study, however, was characterized by an unusually high rate of deaths in the control group. Furthermore, in a recent study, thrombus aspiration failed to reduce mortality at 30 days.153
With regard to pharmacological therapy, intracoronary adenosine administration appears to be the most promising approach. Accordingly, a recent medium-sized controlled randomized trial found that a high dose of intracoronary adenosine, but not nitroprusside, given immediately after thrombus aspiration in patients treated with abciximab, was associated with a lower rate of MVO when compared with placebo; the trial was not powered, however, to assess the effects on clinical endpoints.154
Finally, an attractive form of treatment is ischaemic conditioning, which is known to increase resistance of myocardial cells to ischaemic injury.155 In particular, ischaemic post-conditioning156,157 and remote pre-conditioning158 have been found to improve MVO.
Furthermore, in small pilot studies, cyclosporine159,160 and atrial natriuretic peptide,161 which activate the molecular pathway triggering ischaemic pre-conditioning, have been shown to reduce infarct size. However, these promising early findings need to be confirmed in larger studies with clinical endpoints.
Figure 5 summarizes a therapeutic algorithm for the prevention of MVO.
Figure 5.

Prevention more than treatment has a central role in the management of microvascular angina. It starts before infarction pain occurs by targeting risk factors and by avoiding the blockage of ischaemic pre-conditioning. After the onset of infarction pain and before hospital arrival, the reduction in ischaemic time, an early administration of IIb/IIIa inhibitors, and remote ischaemic pre-conditioning have an important role. In the catheterization laboratory, the use of thrombus aspiration, high doses of intracoronary adenosine, and ischaemic post-conditioning are good opportunities to prevent microvascular obstruction (MVO). No drugs have been shown to reverse established microvascular obstruction (from Ref.110). IC, intracoronary; IPC, ischaemic pre-conditioning.
Iatrogenic coronary microvascular dysfunction
The treatment of iatrogenic CMD is discussed in Supplementary material online.
Conflict of interest: none declared.
Future perspectives
The large body of evidence on the role of CMD in cardiovascular diseases and summarized in the current review indicates that an assessment of coronary microcirculation is frequently needed for optimal patient management. Although, in some instances, CMD represents an epiphenomenon, more frequently, it is an important marker of risk thus providing useful information in risk stratification, as it is the case in hypertrophic and dilated cardiomyopathy or may even contribute to the pathogenesis of cardiovascular and myocardial diseases, thus becoming a therapeutic target as it is the case in patients with stable angina or MVO after primary PCI. The clinical implications of the four types of CMD discussed in this review are summarized in Table 2.
Table 2.
Diagnosis, prognostic value, and treatment of coronary microvascular dysfunction in different clinical settings
| Type of CMD | Specific diseases | Diagnosis | Impact on outcome | Treatment |
|---|---|---|---|---|
| Type 1 | RF MVA |
TTDE TTDE, CMR |
Unknown* Documented |
RF control RF control, see Figure 4 |
| Type 2 | HCM COCM PVB9 Myocarditis AFD Amyloidosis AS |
CMR, PET CMR, PET A-Ch CMR, PET CMR, PET CMR, PET |
Documented Unknown Unknown Unknown Unknown Unknown |
Alcohol septal ablation? Allopurinol Unknown Beta-galactosidase? Unknown Beta-blockers, Ivabradine? |
| Type 3 | Stable angina MVO after pPCI |
Angina after PCI BG, STR, CMR |
Unknown Documented |
Angiogenesis See Figure 5 |
| Type 4 | PCI CABG |
Tn raise Tn raise |
Documented Documented |
Statins, alpha-blockers? Statins |
A-ch, acetylcholine test; AFD, Anderson-Fabry's disease; AS, aortic stenosis; BG, blush grade; CABG, coronary aortic bypass graft; CMD, coronary microvascular dysfunction; CMR, cardiac magnetic resonance; COCM, congestive cardiomyopathy; HCM, hypertrophic cardiomyopathy; MVA, microvascular angina; MVO, microvascular obstruction; PET: positron emission tomography; pPCI, primary percutaneous coronary intervention; PVB, Parvovirus B9; RF, risk factors; STR, ST segment resolution; Tn, troponin; TTDE, transthoracic Doppler echocardiography.
It is unknown the incremental prognostic value of coronary microvascular dysfunction in addition to that conveyed by risk factors
Supplementary material
Supplementary material is available at European Heart Journal online.
Funding
This work was supported by contracts from the National Heart, Lung and Blood Institutes (nos N01-HV-68161, N01-HV-68162, N01-HV-68163, and N01-HV-68164), grants (U0164829, U01 HL649141, U01 HL649241, T32HL69751, R01 HL090957, and 1R03AG032631) from the NIH, GCRC grant (MO1-RR00425) from the NIH, the National Center for Advancing Translational Sciences (grant UL1TR000124), and grants from the Gustavus and Louis Pfeiffer Research Foundation, Danville, NJ, The Women's Guild of Cedars-Sinai Medical Center, Los Angeles, CA, The Ladies Hospital Aid Society of Western Pennsylvania, Pittsburgh, PA, and QMED, Inc., Laurence Harbor, NJ, the Edythe L. Broad Women's Heart Research Fellowship, Cedars-Sinai Medical Center, Los Angeles, CA, the Barbra Streisand Women's Cardiovascular Research and Education Program, Cedars-Sinai Medical Center, Los Angeles and The Society for Women's Health Research (SWHR), Washington, DC.
Supplementary Material
References
- 1.Patel MR, Peterson ED, Dai D, Brennan JM, Redberg RF, Anderson HV, Brindis RG, Douglas PS. Low diagnostic yield of elective coronary angiography. N Engl J Med. 2010;362:886–895. doi: 10.1056/NEJMoa0907272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Cannon RO, Epstein SE. ‘Microvascular angina’ as a cause of chest pain with angiographically normal coronary arteries. Am J Cardiol. 1988;61:1338–1343. doi: 10.1016/0002-9149(88)91180-0. [DOI] [PubMed] [Google Scholar]
- 3.Epstein SE, Cannon RO. Site of increased resistance to coronary flow in patients with angina pectoris and normal epicardial coronary arteries. J Am Coll Cardiol. 1986;8:459–461. doi: 10.1016/s0735-1097(86)80067-5. [DOI] [PubMed] [Google Scholar]
- 4.Chareonthaitawee P, Kaufmann P, Rimoldi O, Camici PG. Heterogeneity of resting and hyperemic myocardial blood flow in healthy humans. Cardiovasc Res. 2001;50:151–161. doi: 10.1016/s0008-6363(01)00202-4. [DOI] [PubMed] [Google Scholar]
- 5.Camici PG, Rimoldi OE. The clinical value of myocardial blood flow measurement. J Nucl Med. 2009;50:1076–1087. doi: 10.2967/jnumed.108.054478. [DOI] [PubMed] [Google Scholar]
- 6.Camici PG, Crea F. Coronary microvascular dysfunction. N Engl J Med. 2007;356:830–840. doi: 10.1056/NEJMra061889. [DOI] [PubMed] [Google Scholar]
- 7.Förstermann U, Sessa WC. Nitric oxide synthases: regulation and function. Eur Heart J. 2012;33:829–837. doi: 10.1093/eurheartj/ehr304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Satoh K, Fukumoto Y, Shimokawa H. Rho-kinase: important new therapeutic target in cardiovascular diseases. Am J Physiol Heart Circ Physiol. 2011;301:H287–H296. doi: 10.1152/ajpheart.00327.2011. [DOI] [PubMed] [Google Scholar]
- 9.Moreau P, d'Uscio LV, Luscher TF. Structure and reactivity of small arteries in aging. Cardiovasc Res. 1998;37:247–253. doi: 10.1016/s0008-6363(97)00225-3. [DOI] [PubMed] [Google Scholar]
- 10.Antony I, Nitenberg A, Foult JM, Aptecar E. Coronary vasodilator reserve in untreated and treated hypertensive patients with and without left ventricular hypertrophy. J Am Coll Cardiol. 1993;22:514–520. doi: 10.1016/0735-1097(93)90058-9. [DOI] [PubMed] [Google Scholar]
- 11.Rizzoni D, Palombo C, Porteri E, Muiesan ML, Kozakova M, La Canna G, Nardi M, Guelfi D, Salvetti M, Morizzo C, Vittone F, Rosei EA. Relationships between coronary flow vasodilator capacity and small artery remodelling in hypertensive patients. J Hypertens. 2003;21:625–631. doi: 10.1097/00004872-200303000-00030. [DOI] [PubMed] [Google Scholar]
- 12.Nahser PJ, Jr, Brown RE, Oskarsson H, Winniford MD, Rossen JD. Maximal coronary flow reserve and metabolic coronary vasodilation in patients with diabetes mellitus. Circulation. 1995;91:635–640. doi: 10.1161/01.cir.91.3.635. [DOI] [PubMed] [Google Scholar]
- 13.Nitenberg A, Valensi P, Sachs R, Dali M, Aptecar E, Attali JR. Impairment of coronary vascular reserve and ach-induced coronary vasodilation in diabetic patients with angiographically normal coronary arteries and normal left ventricular systolic function. Diabetes. 1993;42:1017–1025. doi: 10.2337/diab.42.7.1017. [DOI] [PubMed] [Google Scholar]
- 14.Dayanikli F, Grambow D, Muzik O, Mosca L, Rubenfire M, Schwaiger M. Early detection of abnormal coronary flow reserve in asymptomatic men at high risk for coronary artery disease using positron emission tomography. Circulation. 1994;90:808–817. doi: 10.1161/01.cir.90.2.808. [DOI] [PubMed] [Google Scholar]
- 15.Kaufmann PA, Gnecchi-Ruscone T, Schafers KP, Luscher TF, Camici PG. Low density lipoprotein cholesterol and coronary microvascular dysfunction in hypercholesterolemia. J Am Coll Cardiol. 2000;36:103–109. doi: 10.1016/s0735-1097(00)00697-5. [DOI] [PubMed] [Google Scholar]
- 16.Dagres N, Saller B, Haude M, Husing J, von Birgelen C, Schmermund A, Sack S, Baumgart D, Mann K, Erbel R. Insulin sensitivity and coronary vasoreactivity: Insulin sensitivity relates to adenosine-stimulated coronary flow response in human subjects. Clin Endocrinol (Oxf) 2004;61:724–731. doi: 10.1111/j.1365-2265.2004.02156.x. [DOI] [PubMed] [Google Scholar]
- 17.Tune JD, Gorman MW, Feigl EO. Matching coronary blood flow to myocardial oxygen consumption. J Appl Physiol. 2004;97:404–415. doi: 10.1152/japplphysiol.01345.2003. [DOI] [PubMed] [Google Scholar]
- 18.Di Carli MF, Janisse J, Grunberger G, Ager J. Role of chronic hyperglycemia in the pathogenesis of coronary microvascular dysfunction in diabetes. J Am Coll Cardiol. 2003;41:1387–1393. doi: 10.1016/s0735-1097(03)00166-9. [DOI] [PubMed] [Google Scholar]
- 19.Reaven GM. Role of insulin resistance in human disease (syndrome X): an expanded definition. Annu Rev Med. 1993;44:121–131. doi: 10.1146/annurev.me.44.020193.001005. [DOI] [PubMed] [Google Scholar]
- 20.Jadhav S, Ferrell W, Greer IA, Petrie JR, Cobbe SM, Sattar N. Effects of metformin on microvascular function and exercise tolerance in women with angina and normal coronary arteries: a randomized, double-blind, placebo-controlled study. J Am Coll Cardiol. 2006;48:956–963. doi: 10.1016/j.jacc.2006.04.088. [DOI] [PubMed] [Google Scholar]
- 21.Cavallo Perin P, Pacini G, Giunti S, Comune M, Conte MR, Cassader M, Pagano G. Microvascular angina (cardiological syndrome X) per se is not associated with hyperinsulinaemia or insulin resistance. Eur J Clin Invest. 2000;30:481–486. doi: 10.1046/j.1365-2362.2000.00651.x. [DOI] [PubMed] [Google Scholar]
- 22.Cosin-Sales J, Pizzi C, Brown S, Kaski JC. C-reactive protein, clinical presentation, and ischaemic activity in patients with chest pain and normal coronary angiograms. J Am Coll Cardiol. 2003;41:1468–1474. doi: 10.1016/s0735-1097(03)00243-2. [DOI] [PubMed] [Google Scholar]
- 23.Ishimori ML, Martin R, Berman DS, Goykhman P, Shaw LJ, Shufelt C, Slomka PJ, Thomson LE, Schapira J, Yang Y, Wallace DJ, Weisman MH, Bairey Merz CN. Myocardial ischemia in the absence of obstructive coronary artery disease in systemic lupus erythematosus. JACC Cardiovasc Imaging. 2011;4:27–33. doi: 10.1016/j.jcmg.2010.09.019. [DOI] [PubMed] [Google Scholar]
- 24.Recio-Mayoral A, Rimoldi OE, Camici PG, Kaski JC. Inflammation and microvascular dysfunction in cardiac syndrome X patients without conventional risk factors for coronary artery disease. JACC Cardiovasc Imaging. 2013;6:660–667. doi: 10.1016/j.jcmg.2012.12.011. [DOI] [PubMed] [Google Scholar]
- 25.Tondi P, Santoliquido A, Di Giorgio A, Sestito A, Sgueglia GA, Flore R, Careri G, Pinnacchio G, Lanza GA, Crea F. Endothelial dysfunction as assessed by flow-mediated dilation in patients with cardiac syndrome X: role of inflammation. Eur Rev Med Pharmacol Sci. 2011;15:1074–1077. [PubMed] [Google Scholar]
- 26.Wessel TR, Arant CB, McGorray SP, Sharaf BL, Reis SE, Kerensky RA, von Mering GO, Smith KM, Pauly DF, Handberg EM, Mankad S, Olson MB, Johnson BD, Merz CN, Sopko G, Pepine CJ. Coronary microvascular reactivity is only partially predicted by atherosclerosis risk factors or coronary artery disease in women evaluated for suspected ischemia: results from the NHLBI women's ischemia syndrome evaluation (WISE) Clin Cardiol. 2007;30:69–74. doi: 10.1002/clc.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cox ID, Botker HE, Bagger JP, Sonne HS, Kristensen BO, Kaski JC. Elevated endothelin concentrations are associated with reduced coronary vasomotor responses in patients with chest pain and normal coronary arteriograms. J Am Coll Cardiol. 1999;34:455–460. doi: 10.1016/s0735-1097(99)00224-7. [DOI] [PubMed] [Google Scholar]
- 28.Ong P, Athanasiadis A, Borgulya G, Mahrholdt H, Kaski JC, Sechtem U. High prevalence of a pathological response to acetylcholine testing in patients with stable angina pectoris and unobstructed coronary arteries. The ACOVA Study (Abnormal COronary VAsomotion in patients with stable angina and unobstructed coronary arteries) J Am Coll Cardiol. 2023;59:655–662. doi: 10.1016/j.jacc.2011.11.015. [DOI] [PubMed] [Google Scholar]
- 29.Johnson BD, Shaw LJ, Pepine CJ, Reis SE, Kelsey SF, Sopko G, Rogers WJ, Mankad S, Sharaf BL, Bittner V, Bairey Merz CN. Persistent chest pain predicts cardiovascular events in women without obstructive coronary artery disease: results from the NIH-NHLBI-sponsored women's ischemia syndrome evaluation (WISE) study. Eur Heart J. 2006;27:1408–1415. doi: 10.1093/eurheartj/ehl040. [DOI] [PubMed] [Google Scholar]
- 30.Merz NB, Johnson BD, Kelsey PSF, Reis SE, Lewis JF, Reichek N, Rogers WJ, Pepine CF, Shaw LJ. Diagnostic, prognostic, and cost assessment of coronary artery disease in women. Am J Manag Care. 2001;7:959–965. [PubMed] [Google Scholar]
- 31.Shaw LJ, Bairey Merz CN, Pepine CJ, Reis SE, Bittner V, Kelsey SF, Olson M, Johnson BD, Mankad S, Sharaf BL, Rogers WJ, Wessel TR, Arant CB, Pohost GM, Lerman A, Quyyumi AA, Sopko G. Insights from the NHLBI-sponsored women's ischemia syndrome evaluation (WISE) study: part i: gender differences in traditional and novel risk factors, symptom evaluation, and gender-optimized diagnostic strategies. J Am Coll Cardiol. 2006;47:S4–S20. doi: 10.1016/j.jacc.2005.01.072. [DOI] [PubMed] [Google Scholar]
- 32.Cannon RO, Camici PG, Epstein SE. Pathophysiological dilemma of syndrome X. Circulation. 1992;85:883–892. doi: 10.1161/01.cir.85.3.883. [DOI] [PubMed] [Google Scholar]
- 33.Panting JR, Gatehouse PD, Yang GZ, Grothues F, Firmin DN, Collins P, Pennell DJ. Abnormal subendocardial perfusion in cardiac syndrome X detected by cardiovascular magnetic resonance imaging. N Engl J Med. 2002;346:1948–1953. doi: 10.1056/NEJMoa012369. [DOI] [PubMed] [Google Scholar]
- 34.Buchthal SD, den Hollander JA, Bairey Merz CN, Rogers WA, Pepine CJ, Reichek N, Reis S, Kelsey SF, Pohost GM. Metabolic evidence of myocardial ischemia by 31-P spectroscopy in women with chest pain but no significant coronary stenoses: pilot phase results from the NHLBI-sponsored WISE study. N Engl J Med. 2000;342:829–835. doi: 10.1056/NEJM200003233421201. [DOI] [PubMed] [Google Scholar]
- 35.Buffon A, Rigattieri S, Santini SA, Ramazzotti V, Crea F, Giardina B, Maseri A. Myocardial ischemia-reperfusion damage after pacing-induced tachycardia in patients with cardiac syndrome X. Am J Physiol Heart Circ Physiol. 2000;279:H2627–H2633. doi: 10.1152/ajpheart.2000.279.6.H2627. [DOI] [PubMed] [Google Scholar]
- 36.Bairey Merz CN, Shaw LJ, Reis SE, Bittner V, Kelsey SF, Olson M, Johnson BD, Pepine CJ, Mankad S, Sharaf BL, Rogers WJ, Pohost GM, Lerman A, Quyyumi AA, Sopko G. Insights from the NHLBI-sponsored women's ischemia syndrome evaluation (WISE) study: Part ii: Gender differences in presentation, diagnosis, and outcome with regard to gender-based pathophysiology of atherosclerosis and macrovascular and microvascular coronary disease. J Am Coll Cardiol. 2006;47:S21–S29. doi: 10.1016/j.jacc.2004.12.084. [DOI] [PubMed] [Google Scholar]
- 37.Maseri A, Crea F, Kaski JC, Crake T. Mechanisms of angina pectoris in syndrome X. J Am Coll Cardiol. 1991;17:499–506. doi: 10.1016/s0735-1097(10)80122-6. [DOI] [PubMed] [Google Scholar]
- 38.Lamendola P, Lanza GA, Spinelli A, Sgueglia GA, Di Monaco A, Barone L, Sestito A, Crea F. Long-term prognosis of patients with cardiac syndrome X. Int J Cardiol. 2010;140:197–199. doi: 10.1016/j.ijcard.2008.11.026. [DOI] [PubMed] [Google Scholar]
- 39.Gulati M, Cooper-DeHoff RM, McClure C, Johnson BD, Shaw LJ, Handberg EM, Zineh I, Kelsey SF, Arnsdorf MF, Black HR, Pepine CJ, Merz CN. Adverse cardiovascular outcomes in women with nonobstructive coronary artery disease: a report from the women's ischemia syndrome evaluation study and the St James women take heart project. Arch Intern Med. 2009;169:843–850. doi: 10.1001/archinternmed.2009.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Pepine CJ, Anderson RD, Sharaf BL, Reis SE, Smith KM, Handberg EM, Johnson BD, Sopko G, Bairey Merz CN. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia results from the national heart, lung and blood institute WISE (women's ischemia syndrome evaluation) study. J Am Coll Cardiol. 2010;55:2825–2832. doi: 10.1016/j.jacc.2010.01.054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Jespersen L, Hvelplund A, Abildstrom SZ, Pedersen F, Galatius S, Madsen JK, Jorgensen E, Kelbaek H, Prescott E. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33:734–744. doi: 10.1093/eurheartj/ehr331. [DOI] [PubMed] [Google Scholar]
- 42.Kaski JC. Overview of gender aspects of cardiac syndrome X. Cardiovasc Res. 2002;53:620–626. doi: 10.1016/s0008-6363(01)00460-6. [DOI] [PubMed] [Google Scholar]
- 43.Shaw LJ, Bugiardini R, Bairey Merz CN. Women and ischemic heart disease: evolving knowledge. J Am Coll Cardiol. 2009;54:1561–1575. doi: 10.1016/j.jacc.2009.04.098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gulati M, Shaw LJ, Bairey Merz CN. Myocardial ischemia in women: lessons from the NHLBI WISE study. Clin Cardiol. 2012;35:141–148. doi: 10.1002/clc.21966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Lanza GA. Cardiac syndrome X: a critical overview and future perspectives. Heart. 2007;93:159–166. doi: 10.1136/hrt.2005.067330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Lanza GA, Manzoli A, Bia E, Crea F, Maseri A. Acute effects of nitrates on exercise testing in patients with syndrome X. Clinical and pathophysiological implications. Circulation. 1994;90:2695–2700. doi: 10.1161/01.cir.90.6.2695. [DOI] [PubMed] [Google Scholar]
- 47.Bugiardini R, Manfrini O, Pizzi C, Fontana F, Morgagni G. Endothelial function predicts future development of coronary artery disease: a study of women with chest pain and normal coronary angiograms. Circulation. 2004;109:2518–2523. doi: 10.1161/01.CIR.0000128208.22378.E3. [DOI] [PubMed] [Google Scholar]
- 48.Marroquin OC, Holubkov R, Edmundowicz D, Rickens C, Pohost G, Buchthal S, Pepine CJ, Sopko G, Sembrat RC, Meltzer CC, Reis SE. Heterogeneity of microvascular dysfunction in women with chest pain not attributable to coronary artery disease: implications for clinical practice. Am Heart J. 2003;145:628–635. doi: 10.1067/mhj.2003.95. [DOI] [PubMed] [Google Scholar]
- 49.Lanza GA, Buffon A, Sestito A, Natale L, Sgueglia GA, Galiuto L, Infusino F, Mariani L, Centola A, Crea F. Relation between stress-induced myocardial perfusion defects on cardiovascular magnetic resonance and coronary microvascular dysfunction in patients with cardiac syndrome X. J Am Coll Cardiol. 2008;51:466–472. doi: 10.1016/j.jacc.2007.08.060. [DOI] [PubMed] [Google Scholar]
- 50.Sestito A, Lanza GA, Di Monaco A, Lamendola P, Careri G, Tarzia P, Pinnacchio G, Battipaglia I, Crea F. Relation between cardiovascular risk factors and coronary microvascular dysfunction in cardiac syndrome X. J Cardiovasc Med. 2011;12:322–327. doi: 10.2459/JCM.0b013e3283406479. [DOI] [PubMed] [Google Scholar]
- 51.Lanza GA, Crea F. Primary coronary microvascular dysfunction: clinical presentation, pathophysiology, and management. Circulation. 2010;121:2317–2325. doi: 10.1161/CIRCULATIONAHA.109.900191. [DOI] [PubMed] [Google Scholar]
- 52.Cavusoglu Y, Entok E, Timuralp B, Vardareli E, Kudaiberdieva G, Birdane A, Gorenek B, Unalir A, Goktekin O, Ata N. Regional distribution and extent of perfusion abnormalities, and the lung to heart uptake ratios during exercise thallium-201 SPECT imaging in patients with cardiac syndrome X. Can J Cardiol. 2005;21:57–62. [PubMed] [Google Scholar]
- 53.Pizzi C, Manfrini O, Fontana F, Bugiardini R. Angiotensin-converting enzyme inhibitors and 3-hydroxy-3-methylglutaryl coenzyme a reductase in cardiac syndrome X: role of superoxide dismutase activity. Circulation. 2004;109:53–58. doi: 10.1161/01.CIR.0000100722.34034.E4. [DOI] [PubMed] [Google Scholar]
- 54.Wei J, Mehta PK, Johnson BD, Samuels B, Kar S, Anderson RD, Azarbal B, Petersen J, Sharaf B, Handberg E, Shufelt C, Kothawade K, Sopko G, Lerman A, Shaw L, Kelsey SF, Pepine CJ, Merz CN. Safety of coronary reactivity testing in women with no obstructive coronary artery disease: results from the NHLBI-sponsored WISE (women's ischemia syndrome evaluation) study. JACC Cardiovasc Interv. 2012;5:646–653. doi: 10.1016/j.jcin.2012.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.von Mering GO, Arant CB, Wessel TR, McGorray SP, Bairey Merz CN, Sharaf BL, Smith KM, Olson MB, Johnson BD, Sopko G, Handberg E, Pepine CJ, Kerensky RA. Abnormal coronary vasomotion as a prognostic indicator of cardiovascular events in women: results from the national heart, lung, and blood institute-sponsored women's ischemia syndrome evaluation (WISE) Circulation. 2004;109:722–725. doi: 10.1161/01.CIR.0000115525.92645.16. [DOI] [PubMed] [Google Scholar]
- 56.JCS Joint Working Group. Guidelines for diagnosis and treatment of patients with vasospastic angina (coronary spastic angina) (JCS 2008) Circ J. 2010;74:1745–1762. doi: 10.1253/circj.cj-10-74-0802. [DOI] [PubMed] [Google Scholar]
- 57.Bugiardini R, Bairey Merz CN. Angina with ‘normal’ coronary arteries: a changing philosophy. JAMA. 2005;293:477–484. doi: 10.1001/jama.293.4.477. [DOI] [PubMed] [Google Scholar]
- 58.Humphries KH, Pu A, Gao M, Carere RG, Pilote L. Angina with ‘normal’ coronary arteries: sex differences in outcomes. Am Heart J. 2008;155:375–381. doi: 10.1016/j.ahj.2007.10.019. [DOI] [PubMed] [Google Scholar]
- 59.Blomkalns AL, Chen AY, Hochman JS, Peterson ED, Trynosky K, Diercks DB, Brogan GX, Jr, Boden WE, Roe MT, Ohman EM, Gibler WB, Newby LK. Gender disparities in the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: large-scale observations from the crusade (can rapid risk stratification of unstable angina patients suppress adverse outcomes with early implementation of the American College of Cardiology/American Heart Association Guidelines) national quality improvement initiative. J Am Coll Cardiol. 2005;45:832–837. doi: 10.1016/j.jacc.2004.11.055. [DOI] [PubMed] [Google Scholar]
- 60.Vaccarino V, Badimon L, Corti R, de Wit C, Dorobantu M, Hall A, Koller A, Marzilli M, Pries A, Bugiardini R. Ischaemic heart disease in women: are there sex differences in pathophysiology and risk factors? Position paper from the working group on coronary pathophysiology and microcirculation of the European Society of Cardiology. Cardiovasc Res. 2011;90:9–17. doi: 10.1093/cvr/cvq394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Elesber A, Lerman A, Bybee KA, Murphy JG, Barsness G, Singh M, Rihal CS, Prasad A. Myocardial perfusion in apical ballooning syndrome correlate of myocardial injury. Am Heart J. 2006;152:469 e9–469e13. doi: 10.1016/j.ahj.2006.06.007. [DOI] [PubMed] [Google Scholar]
- 62.Rigo F, Sicari R, Citro R, Ossena G, Buja P, Picano E. Diffuse, marked, reversible impairment in coronary microcirculation in stress cardiomyopathy: a Doppler transthoracic echo study. Ann Med. 2009;41:462–470. doi: 10.1080/07853890903022793. [DOI] [PubMed] [Google Scholar]
- 63.Feola M, Rosso GL, Casasso F, Morena L, Biggi A, Chauvie S, Ribichini F, Uslenghi E. Reversible inverse mismatch in transient left ventricular apical ballooning: perfusion/metabolism positron emission tomography imaging. J Nucl Cardiol. 2006;13:587–590. doi: 10.1016/j.nuclcard.2006.05.004. [DOI] [PubMed] [Google Scholar]
- 64.Galiuto L, De Caterina AR, Porfidia A, Paraggio L, Barchetta S, Locorotondo G, Rebuzzi AG, Crea F. Reversible coronary microvascular dysfunction: a common pathogenetic mechanism in apical ballooning or Takotsubo syndrome. Eur Heart J. 2010;31:1319–1327. doi: 10.1093/eurheartj/ehq039. [DOI] [PubMed] [Google Scholar]
- 65.Barletta G, Del Pace S, Boddi M, Del Bene R, Salvadori C, Bellandi B, Coppo M, Saletti E, Gensini GF. Abnormal coronary reserve and left ventricular wall motion during cold pressor test in patients with previous left ventricular ballooning syndrome. Eur Heart J. 2009;30:3007–3014. doi: 10.1093/eurheartj/ehp325. [DOI] [PubMed] [Google Scholar]
- 66.Martin EA, Prasad A, Rihal CS, Lerman LO, Lerman A. Endothelial function and vascular response to mental stress are impaired in patients with apical ballooning syndrome. J Am Coll Cardiol. 2010;56:1840–1846. doi: 10.1016/j.jacc.2010.03.107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Cecchi F, Olivotto I, Gistri R, Lorenzoni R, Chiriatti G, Camici PG. Coronary microvascular dysfunction and prognosis in hypertrophic cardiomyopathy. N Engl J Med. 2003;349:1027–1035. doi: 10.1056/NEJMoa025050. [DOI] [PubMed] [Google Scholar]
- 68.Olivotto I, Girolami F, Sciagrá R, Ackerman MJ, Sotgia B, Bos JM, Nistri S, Sgalambro A, Grifoni C, Torricelli F, Camici PG, Cecchi F. Microvascular function is selectively impaired in patients with hypertrophic cardiomyopathy and sarcomere myofilament gene mutations. J Am Coll Cardiol. 2011;58:839–848. doi: 10.1016/j.jacc.2011.05.018. [DOI] [PubMed] [Google Scholar]
- 69.Kwon DH, Smedira NG, Rodriguez ER, Tan C, Setser R, Thamilarasan M, Lytle BW, Lever HM, Desai MY. Cardiac magnetic resonance detection of myocardial scarring in hypertrophic cardiomyopathy: correlation with histopathology and prevalence of ventricular tachycardia. J Am Coll Cardiol. 2009;54:242–249. doi: 10.1016/j.jacc.2009.04.026. [DOI] [PubMed] [Google Scholar]
- 70.Petersen SE, Jerosch-Herold M, Hudsmith LE, Robson MD, Francis JM, Doll HA, Selvanayagam JB, Neubauer S, Watkins H. Evidence for microvascular dysfunction in hypertrophic cardiomyopathy: new insights from multiparametric magnetic resonance imaging. Circulation. 2007;115:2418–2425. doi: 10.1161/CIRCULATIONAHA.106.657023. [DOI] [PubMed] [Google Scholar]
- 71.Maron MS, Olivotto I, Maron BJ, Prasad SK, Cecchi F, Udelson JE, Camici PG. The case for myocardial ischemia in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2009;54:866–875. doi: 10.1016/j.jacc.2009.04.072. [DOI] [PubMed] [Google Scholar]
- 72.Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA. 2002;287:1308–1320. doi: 10.1001/jama.287.10.1308. [DOI] [PubMed] [Google Scholar]
- 73.Green JJ, Berger JS, Kramer CM, Salerno M. Prognostic value of late gadolinium enhancement in clinical outcomes for hypertrophic cardiomyopathy. JACC Cardiovasc Imaging. 2012;5:370–377. doi: 10.1016/j.jcmg.2011.11.021. [DOI] [PubMed] [Google Scholar]
- 74.Maron BJ, McKenna WJ, Danielson GK, Kappenberger LJ, Kuhn HJ, Seidman CE, Shah PM, Spencer WH, III, Spirito P, Ten Cate FJ, Wigle ED ACC/ESC clinical expert consensus document on hypertrophic cardiomyopathy: a report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents and the European Society of Cardiology Committee for Practice Guidelines (Committee to Develop an Expert Consensus Document on Hypertrophic Cardiomyopathy) Eur Heart J. 2003;24:1965–1991. doi: 10.1016/s0195-668x(03)00479-2. [DOI] [PubMed] [Google Scholar]
- 75.Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, Moss AJ, Seidman C, Young JB. Contemporary definitions and classification of the cardiomyopathies. An American Heart Association scientific statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–1816. doi: 10.1161/CIRCULATIONAHA.106.174287. [DOI] [PubMed] [Google Scholar]
- 76.Neglia D, Parodi O, Gallopin M, Sambuceti G, Giorgetti A, Pratali L, Salvadori P, Michelassi C, Lunardi M, Pelosi G, Marzilli M, L'Abbate A. Myocardial blood flow response to pacing tachycardia and to dipyridamole infusion in patients with dilated cardiomyopathy without overt heart failure. A quantitative assessment by positron emission tomography. Circulation. 1995;92:796–804. doi: 10.1161/01.cir.92.4.796. [DOI] [PubMed] [Google Scholar]
- 77.Noue T, Sakai Y, Morooka S, Hayashi T, Takaianagi K, Yamanaka T, Kakoi H, Takabatake Y. Coronary flow reserve in patients with dilated cardiomyopathy. Am Heart J. 1993;125:93–98. doi: 10.1016/0002-8703(93)90061-d. [DOI] [PubMed] [Google Scholar]
- 78.Koutalas E, Kanoupakis E, Vardas P. Sudden cardiac death in non-ischaemic dilated cardiomyopathy: a critical appraisal of existing and potential risk stratification tools. Int J Cardiol. 2013;167:335–341. doi: 10.1016/j.ijcard.2012.07.014. [DOI] [PubMed] [Google Scholar]
- 79.Lehrke S, Lossnitzer D, Schöb M, Steen H, Merten C, Kemmling H, Pribe R, Ehlermann P, Zugck C, Korosoglou G, Giannitsis E, Katus HA. Use of cardiovascular magnetic resonance for risk stratification in chronic heart failure: prognostic value of late gadolinium enhancement in patients with non-ischaemic dilated cardiomyopathy. Heart. 2011;97:727–732. doi: 10.1136/hrt.2010.205542. [DOI] [PubMed] [Google Scholar]
- 80.Kandolf R. Virus etiology of inflammatory cardiomyopathy. Dtsch Med Wochenschr. 2004;129:2187–2192. doi: 10.1055/s-2004-831863. [DOI] [PubMed] [Google Scholar]
- 81.Mahrholdt H, Wagner A, Deluigi CC, Kispert E, Hager S, Meinhardt G, Vogelsberg H, Fritz P, Dippon J, Bock CT, Klingel K, Kandolf R, Sechtem U. Presentation, patterns of myocardial damage, and clinical course of viral myocarditis. Circulation. 2006;114:1581–1590. doi: 10.1161/CIRCULATIONAHA.105.606509. [DOI] [PubMed] [Google Scholar]
- 82.Brown KE, Anderson SM, Young NS. Erythrocyte P antigen: cellular receptor for B19 parvovirus. Science. 1993;262:114–117. doi: 10.1126/science.8211117. [DOI] [PubMed] [Google Scholar]
- 83.Kuhl U, Pauschinger M, Bock T, Klingel K, Schwimmbeck CP, Seeberg B, Krautwurm L, Poller W, Schultheiss HP, Kandolf R. Parvovirus B19 infection mimicking acute myocardial infarction. Circulation. 2003;108:945–950. doi: 10.1161/01.CIR.0000085168.02782.2C. [DOI] [PubMed] [Google Scholar]
- 84.Yilmaz A, Mahrholdt H, Athanasiadis A, Vogelsberg H, Meinhardt G, Voehringer M, Kispert EM, Deluigi C, Baccouche H, Spodarev E, Klingel K, Kandolf R, Sechtem U. Coronary vasospasm as the underlying cause for chest pain in patients with PVB19 myocarditis. Heart. 2008;94:1456–1463. doi: 10.1136/hrt.2007.131383. [DOI] [PubMed] [Google Scholar]
- 85.Gould KL, Carabello BA. Why angina in aortic stenosis with normal coronary arteriograms? Circulation. 2003;107:3121–3123. doi: 10.1161/01.CIR.0000074243.02378.80. [DOI] [PubMed] [Google Scholar]
- 86.Ross J, Jr, Braunwald E. Aortic stenosis. Circulation. 1968;38:61–67. doi: 10.1161/01.cir.38.1s5.v-61. [DOI] [PubMed] [Google Scholar]
- 87.Marcus ML, Doty DB, Hiratzka LF, Marcus ML. Decreased coronary reserve: a mechanism for angina pectoris in patients with aortic stenosis and normal coronary arteries. N Engl J Med. 1982;307:1362–1366. doi: 10.1056/NEJM198211253072202. [DOI] [PubMed] [Google Scholar]
- 88.Dunn RB, Griggs DM. Ventricular filling pressure as a determinant of coronary blood flow during ischemia. Am J Physiol Heart Circ Physiol. 1983;244:H429–H436. doi: 10.1152/ajpheart.1983.244.3.H429. [DOI] [PubMed] [Google Scholar]
- 89.Breisch EA, Houser SR, Carey RA, Spann JF, Bove AA. Myocardial blood flow and capillary density in chronic pressure overload of the feline left ventricle. Cardiovasc Res. 1980;14:469–475. doi: 10.1093/cvr/14.8.469. [DOI] [PubMed] [Google Scholar]
- 90.Schwartzkopff B, Frenzel H, Dieckerhoff J, Betz P, Flasshove M, Schulte HD, Mundhenke M, Motz W, Strauer BE. Morphometric investigation of human myocardium in arterial hypertension and valvular aortic stenosis. Eur Heart J. 1992;13(Suppl D):17–23. doi: 10.1093/eurheartj/13.suppl_d.17. [DOI] [PubMed] [Google Scholar]
- 91.Rajappan K, Rimoldi OE, Dutka DP, Ariff B, Pennell DJ, Sheridan DJ, Camici PG. Mechanisms of coronary microcirculatory dysfunction in patients with aortic stenosis and angiographically normal coronary arteries. Circulation. 2002;105:470–476. doi: 10.1161/hc0402.102931. [DOI] [PubMed] [Google Scholar]
- 92.Niccoli GP, Giubilato S, Di Vito L, Leo A, Cosentino N, Pitocco D, Marco V, Ghirlanda G, Prati F, Crea F. Severity of coronary atherosclerosis in patients with a first acute coronary event: a diabetes paradox. Eur Heart J. 2013;34:729–741. doi: 10.1093/eurheartj/ehs393. [DOI] [PubMed] [Google Scholar]
- 93.Stergiopoulos K, Brown DL. Initial coronary stent implantation with medical therapy vs medical therapy alone for stable coronary artery disease: meta-analysis of randomized controlled trials. Arch Intern Med. 2012;172:312–319. doi: 10.1001/archinternmed.2011.1484. [DOI] [PubMed] [Google Scholar]
- 94.Lerman A, Holmes DR, Herrmann J, Gersh BJ. Microcirculatory dysfunction in ST-elevation myocardial infarction: cause, consequence, or both? Eur Heart J. 2007;28:788–797. doi: 10.1093/eurheartj/ehl501. [DOI] [PubMed] [Google Scholar]
- 95.Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20. doi: 10.1016/S0140-6736(03)12113-7. [DOI] [PubMed] [Google Scholar]
- 96.Rezkalla SH, Kloner RA. Coronary no-reflow phenomenon: from the experimental laboratory to the cardiac catheterization laboratory. Catheter Cardiovasc Interv. 2008;72:950–957. doi: 10.1002/ccd.21715. [DOI] [PubMed] [Google Scholar]
- 97.Lincoff AM, Topol EJ. Illusion of reperfusion. Does anyone achieve optimal reperfusion during acute myocardial infarction? Circulation. 1993;88:1361–1374. doi: 10.1161/01.cir.88.3.1361. [DOI] [PubMed] [Google Scholar]
- 98.Niccoli G, Burzotta F, Galiuto L, Crea F. Myocardial no-reflow in humans. J Am Coll Cardiol. 2009;54:281–292. doi: 10.1016/j.jacc.2009.03.054. [DOI] [PubMed] [Google Scholar]
- 99.Niccoli G, Kharbanda RK, Crea F, Banning AP. No-reflow: again prevention is better than treatment. Eur Heart J. 2010;31:2449–2555. doi: 10.1093/eurheartj/ehq299. [DOI] [PubMed] [Google Scholar]
- 100.Brosh D, Assali AR, Mager A, et al. Effect of no-reflow during primary percutaneous coronary intervention for acute myocardial infarction on six-month mortality. Am J Cardiol. 2007;99:442–445. doi: 10.1016/j.amjcard.2006.08.054. [DOI] [PubMed] [Google Scholar]
- 101.Bolognese L, Carrabba N, Parodi G, Santoro GM, Buonamici P, Cerisano G, Antoniucci D. Impact of microvascular dysfunction on left ventricular remodeling and long-term clinical outcome after primary coronary angioplasty for acute myocardial infarction. Circulation. 2004;109:1121–1126. doi: 10.1161/01.CIR.0000118496.44135.A7. [DOI] [PubMed] [Google Scholar]
- 102.Montalescot G, Ongen Z, Guindy R, Sousa A, Lu SZ, Pahlajani D, Pellois A, Vicaut E for the RIVIERA Investigators. Predictors of outcome in patients undergoing PCI. Results of the RIVIERA study. Int J Cardiol. 2008;129:379–387. doi: 10.1016/j.ijcard.2007.07.127. [DOI] [PubMed] [Google Scholar]
- 103.Collet JP, Montalescot G. The acute reperfusion management of STEMI in patients with impaired glucose tolerance and type 2 diabetes. Diabetes Vasc Dis Res. 2005;2:136–143. doi: 10.3132/dvdr.2005.021. [DOI] [PubMed] [Google Scholar]
- 104.Golino P, Maroko PR, Carew TE. The effect of acute hypercholesterolemia on myocardial infarct size and the no-reflow phenomenon during coronary occlusion-reperfusion. Circulation. 1987;75:292–298. doi: 10.1161/01.cir.75.1.292. [DOI] [PubMed] [Google Scholar]
- 105.Rezkalla SH, Kloner RA. Ischaemic preconditioning and preinfarction angina in the clinical arena. Nat Clin Pract Cardiovasc Med. 2004;1:96–102. doi: 10.1038/ncpcardio0047. [DOI] [PubMed] [Google Scholar]
- 106.Testa L, Van Gaal WJ, Biondi Zoccai GG, Agostoni P, Latini RA, Bedogni F, Porto I, Banning AP. Myocardial infarction after percutaneous coronary intervention: a meta-analysis of troponin elevation applying the new universal definition. QJM. 2009;102:369–378. doi: 10.1093/qjmed/hcp005. [DOI] [PubMed] [Google Scholar]
- 107.Uren NG, Crake T, Lefroy DC, de Silva R, Davies GJ, Maseri A. Delayed recovery of coronary resistive vessel function after coronary angioplasty. J Am Coll Cardiol. 1993;21:612–662. doi: 10.1016/0735-1097(93)90092-f. [DOI] [PubMed] [Google Scholar]
- 108.Gulielmos V, Menschikowski M, Dill H, Eller M, Thiele S, Tugtekin SM, Jaross W, Schueler S. Interleukin-1, interleukin-6 and myocardial enzyme response after coronary artery bypass grafting—a prospective randomized comparison of the conventional and three minimally invasive surgical techniques. Eur J Cardiothorac Surg. 2000;18:594–601. doi: 10.1016/s1010-7940(00)00553-4. [DOI] [PubMed] [Google Scholar]
- 109.Clive Landis R, Murkin JM, Stump DA, Baker RA, Arrowsmith JE, De Somer F, Dain SL, Dobkowski WB, Ellis JE, Falter F, Fischer G, Hammon JW, Jonas RA, Kramer RS, Likosky DS, Paget Milsom F, Poullis M, Verrier ED, Walley K, Westaby S. Consensus statement: minimal criteria for reporting the systemic inflammatory response to cardiopulmonary bypass. Heart Surg Forum. 2010;13:E116–E123. doi: 10.1532/HSF98.20101022. [DOI] [PubMed] [Google Scholar]
- 110.Ren G, Dewald O, Frangogiannis NG. Inflammatory mechanisms in myocardial infarction. Curr Drug Targets Inflamm Allergy. 2003;2:242–256. doi: 10.2174/1568010033484098. [DOI] [PubMed] [Google Scholar]
- 111.Frangogiannis NG, Smith CW, Entman ML. The inflammatory response in myocardial infarction. Cardiovasc Res. 2002;53:31–47. doi: 10.1016/s0008-6363(01)00434-5. [DOI] [PubMed] [Google Scholar]
- 112.Spyrou N, Khan MA, Rosen SD, Jagathesan R, Foale R, Davies W, Sogliani F, De Lisle Stanbridge R, Camici PG. Persistent but reversible coronary microvascular dysfunction after bypass grafting. Am J Physiol. 2000;279:H2634–H2640. doi: 10.1152/ajpheart.2000.279.6.H2634. [DOI] [PubMed] [Google Scholar]
- 113.Lim CC, Cuculi F, van Gaal WJ, Testa L, Arnold JR, Karamitsos T, Francis JM, Digby JE, Antoniades C, Kharbanda RK, Neubauer S, Westaby S, Banning AP. Early diagnosis of perioperative myocardial infarction after coronary bypass grafting: a study using biomarkers and cardiac magnetic resonance imaging. Ann Thorac Surg. 2011;92:2046–2053. doi: 10.1016/j.athoracsur.2011.05.019. [DOI] [PubMed] [Google Scholar]
- 114.Croal BL, Hillis GS, Gibson PH, Fazal MT, El-Shafei H, Gibson G, Jeffrey RR, Buchan KG, West D, Cuthbertson BH. Relationship between postoperative cardiac troponin I levels and outcome of cardiac surgery. Circulation. 2006;114:1468–1475. doi: 10.1161/CIRCULATIONAHA.105.602370. [DOI] [PubMed] [Google Scholar]
- 115.Neglia D, Fommei E, Varela-Carver A, Mancini M, Ghione S, Lombardi M, Pisani P, Parker H, d'Amati G, Donato L, Camici PG. Treatment of hypertension with perindopril plus indapamide leads to reverse coronary microvascular remodelling and improved blood flow. J Hypertens. 2011;29:364–372. doi: 10.1097/HJH.0b013e328340a08e. [DOI] [PubMed] [Google Scholar]
- 116.Lim TK, Choy AJ, Khan F, Belch JJ, Struthers AD, Lang CC. Therapeutic development in cardiac syndrome X: a need to target the underlying pathophysiology. Cardiovasc Ther. 2009;27:49–58. doi: 10.1111/j.1755-5922.2008.00070.x. [DOI] [PubMed] [Google Scholar]
- 117.Eriksson BE, Tyni-Lenne R, Svedenhag J, Hallin R, Jensen-Urstad K, Jensen-Urstad M, Bergman K, Selven C. Physical training in syndrome X: physical training counteracts deconditioning and pain in syndrome X. J Am Coll Cardiol. 2000;36:1619–1625. doi: 10.1016/s0735-1097(00)00931-1. [DOI] [PubMed] [Google Scholar]
- 118.Kayikcioglu M, Payzin S, Yavuzgil O, Kultursay H, Can LH, Soydan I. Benefits of statin treatment in cardiac syndrome-X. Eur Heart J. 2003;24:1999–2005. doi: 10.1016/s0195-668x(03)00478-0. [DOI] [PubMed] [Google Scholar]
- 119.Chen JW, Hsu NW, Wu TC, Lin SJ, Chang MS. Long-term angiotensin-converting enzyme inhibition reduces plasma asymmetric dimethylarginine and improves endothelial nitric oxide bioavailability and coronary microvascular function in patients with syndrome x. Am J Cardiol. 2002;90:974–982. doi: 10.1016/s0002-9149(02)02664-4. [DOI] [PubMed] [Google Scholar]
- 120.Sutsch G, Oechslin E, Mayer I, Hess OM. Effect of diltiazem on coronary flow reserve in patients with microvascular angina. Int J Cardiol. 1995;52:135–143. doi: 10.1016/0167-5273(95)02458-9. [DOI] [PubMed] [Google Scholar]
- 121.Lanza GA, Colonna G, Pasceri V, Maseri A. Atenolol versus amlodipine versus isosorbide-5-mononitrate on anginal symptoms in syndrome X. Am J Cardiol. 1999;84:854–856. doi: 10.1016/s0002-9149(99)00450-6. [DOI] [PubMed] [Google Scholar]
- 122.Kaski JC, Rosano GMC, Collins P, Nihoyannopoulos P, Maseri A, Poole-Wilson PA. Cardiac syndrome X: clinical characteristics and left ventricular function: long-term follow-up study. J Am Coll Cardiol. 1995;25:807–814. doi: 10.1016/0735-1097(94)00507-M. [DOI] [PubMed] [Google Scholar]
- 123.Mehta PK, Goykhman P, Thomson LE, Shufelt C, Wei J, Yang Y, Gill E, Minissian M, Shaw LJ, Slomka PJ, Slivka M, Berman DS, Bairey Merz CN. Ranolazine improves angina in women with evidence of myocardial ischemia but no obstructive coronary artery disease. JACC Cardiovasc Imaging. 2011;4:514–522. doi: 10.1016/j.jcmg.2011.03.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124.Villano A, Di Franco A, Nerla R, Sestito A, Tarzia P, Lamendola P, Di Monaco A, Sarullo FM, Lanza GA, Crea F. Effects of ivabradine and ranolazine in patients with microvascular angina pectoris. Am J Cardiol. 2013;112:8–13. doi: 10.1016/j.amjcard.2013.02.045. [DOI] [PubMed] [Google Scholar]
- 125.Emdin M, Picano E, Lattanzi F, L'Abbate A. Improved exercise capacity with acute aminophylline administration in patients with syndrome X. J Am Coll Cardiol. 1989;14:1450–1453. doi: 10.1016/0735-1097(89)90380-x. [DOI] [PubMed] [Google Scholar]
- 126.Elliott PM, Krzyzowska-Dickinson K, Calvino R, Hann C, Kaski JC. Effect of oral aminophylline in patients with angina and normal coronary arteriograms (syndrome X) Heart. 1997;77:523–526. doi: 10.1136/hrt.77.6.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Crea F, Gaspardone A, Araujo L, Da Silva R, Kaski JC, Davies G, Maseri A. Effects of aminophylline on cardiac function and regional myocardial perfusion: implications regarding its antiischaemic action. Am Heart J. 1994;127:817–824. doi: 10.1016/0002-8703(94)90548-7. [DOI] [PubMed] [Google Scholar]
- 128.Crea F, Pupita G, Galassi AR, el-Tamimi H, Kaski JC, Davies G, Maseri A. Role of adenosine in pathogenesis of anginal pain. Circulation. 1990;81:164–172. doi: 10.1161/01.cir.81.1.164. [DOI] [PubMed] [Google Scholar]
- 129.Chen JW, Lee WL, Hsu NW, Lin SJ, Ting CT, Wang SP, Chang MS. Effects of short-term treatment of nicorandil on exercise-induced myocardial ischemia and abnormal cardiac autonomic activity in microvascular angina. Am J Cardiol. 1997;80:32–38. doi: 10.1016/s0002-9149(97)00279-8. [DOI] [PubMed] [Google Scholar]
- 130.Botker HE, Sonne HS, Schmitz O, Nielsen TT. Effects of doxazosin on exercise-induced angina pectoris, ST-segment depression, and insulin sensitivity in patients with syndrome X. Am J Cardiol. 1998;82:1352–1356. doi: 10.1016/s0002-9149(98)00640-7. [DOI] [PubMed] [Google Scholar]
- 131.Mohri M, Shimokawa H, Hirakawa Y, Masumoto A, Takeshita A. Rho-kinase inhibition with intracoronary fasudil prevents myocardial ischemia in patients with coronary microvascular spasm. J Am Coll Cardiol. 2003;41:15–19. doi: 10.1016/s0735-1097(02)02632-3. [DOI] [PubMed] [Google Scholar]
- 132.Cannon RO, III, Quyyumi AA, Mincemoyer R, Stine AM, Gracely RH, Smith WB, Geraci MF, Black BC, Uhde TW, Waclawiw MA, Maher K, Benjamin SB. Imipramine in patients with chest pain despite normal coronary angiograms. N Engl J Med. 1994;330:1411–1417. doi: 10.1056/NEJM199405193302003. [DOI] [PubMed] [Google Scholar]
- 133.Adamson DL, Webb CM, Collins P. Esterified estrogens combined with methyltestosterone improve emotional well-being in postmenopausal women with chest pain and normal coronary angiograms. Menopause. 2001;8:233–238. doi: 10.1097/00042192-200107000-00003. [DOI] [PubMed] [Google Scholar]
- 134.Sgueglia GA, Sestito A, Spinelli A, Cioni B, Infusino F, Papacci F, Bellocci F, Meglio M, Crea F, Lanza GA. Long-term follow-up of patients with cardiac syndrome X treated by spinal cord stimulation. Heart. 2007;93:591–597. doi: 10.1136/hrt.2006.102194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135.Kronhaus KD, Lawson WE. Enhanced external counterpulsation is an effective treatment for Syndrome X. Int J Cardiol. 2009;135:256–257. doi: 10.1016/j.ijcard.2008.03.022. [DOI] [PubMed] [Google Scholar]
- 136.Jaber WA, Yang EH, Nishimura RA, Sorajja P, Rihal CS, Elesber A, Eeckhout E, Lerman A. Immediate improvement in coronary flow reserve after alcohol septal ablation in patients with hypertrophic obstructive cardiomyopathy. Heart. 2009;95:564–569. doi: 10.1136/hrt.2008.148239. [DOI] [PubMed] [Google Scholar]
- 137.Soliman OI, Geleijnse ML, Michels M, Dijkmans PA, Nemes A, van Dalen BM, Vletter WB, Serruys PW, ten Cate FJ. Effect of successful alcohol septal ablation on microvascular function in patients with obstructive hypertrophic cardiomyopathy. Am J Cardiol. 2008;101:1321–1327. doi: 10.1016/j.amjcard.2007.12.032. [DOI] [PubMed] [Google Scholar]
- 138.Choudhury L, Elliott P, Rimoldi O, Ryan M, Lammertsma AA, Boyd H, McKenna WJ, Camici PG. Transmural myocardial blood flow distribution in hypertrophic cardiomyopathy and effect of treatment. Basic Res Cardiol. 1999;94:49–59. doi: 10.1007/s003950050126. [DOI] [PubMed] [Google Scholar]
- 139.Gistri R, Cecchi F, Choudhury L, Montereggi A, Sorace O, Salvadori PA, Camici PG. Effect of verapamil on absolute myocardial blood flow in hypertrophic cardiomyopathy. Am J Cardiol. 1994;74:363–368. doi: 10.1016/0002-9149(94)90404-9. [DOI] [PubMed] [Google Scholar]
- 140.Hongo M, Nakatsuka T, Takenaka H, Tanaka M, Watanabe N, Yazaki Y, Sekiguchi M. Effects of intravenous disopyramide on coronary hemodynamics and vasodilator reserve in hypertrophic obstructive cardiomyopathy. Cardiology. 1996;87:6–11. doi: 10.1159/000177052. [DOI] [PubMed] [Google Scholar]
- 141.Kyriakidis M, Triposkiadis F, Dernellis J, Androulakis AE, Mellas P, Kelepeshis GA, Gialafos JE. Effects of cardiac versus circulatory angiotensin-converting enzyme inhibition on left ventricular diastolic function and coronary blood flow in hypertrophic obstructive cardiomyopathy. Circulation. 1998;97:1342–1347. doi: 10.1161/01.cir.97.14.1342. [DOI] [PubMed] [Google Scholar]
- 142.Erdogan D, Gullu H, Caliskan M, Ciftci O, Baycan S, Yildirir A, Muderrisoglu H. Nebivolol improves coronary flow reserve in patients with idiopathic dilated cardiomyopathy. Heart. 2007;93:319–324. doi: 10.1136/hrt.2006.091751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Fan Y, Lin JH, Dong G, Zhu J, Yin F, Yang SS. The effect of carvedilol on coronary flow reserve in patients with dilated cardiomyopathy. Zhonghua Nei Ke Za Zhi. 2010;49:217–219. [PubMed] [Google Scholar]
- 144.Neglia D, Sambuceti G, Giorgetti A, Bartoli M, Salvadori P, Sorace O, Puccini G, L'Abbate A, Parodi O. Effects of long-term treatment with verapamil on left ventricular function and myocardial blood flow in patients with dilated cardiomyopathy without overt heart failure. J Cardiovasc Pharmacol. 2000;36:744–750. doi: 10.1097/00005344-200012000-00009. [DOI] [PubMed] [Google Scholar]
- 145.Erdogan D, Tayyar S, Uysal BA, Icli A, Karabacak M, Ozaydin M, Dogan A. Effects of allopurinol on coronary microvascular and left ventricular function in patients with idiopathic dilated cardiomyopathy. Can J Cardiol. 2012;28:721–727. doi: 10.1016/j.cjca.2012.04.005. [DOI] [PubMed] [Google Scholar]
- 146.Chilian WM, Penn MS, Pung YF, Dong F, Mayorga M, Ohanyan V, Logan S, Yin L. Coronary collateral growth—back to the future. J Mol Cell Cardiol. 2012;52:905–911. doi: 10.1016/j.yjmcc.2011.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 147.Henry TD, Grines CL, Watkins MW, Dib N, Barbeau G, Moreadith R, Andrasfay T, Engler RL. Effects of Ad5FGF-4 in patients with angina: an analysis of pooled data from the AGENT-3 and AGENT-4 trials. J Am Coll Cardiol. 2007;50:1038–1046. doi: 10.1016/j.jacc.2007.06.010. [DOI] [PubMed] [Google Scholar]
- 148.Losordo DW, Henry TD, Davidson C, Sup Lee J, Costa MA, Bass T, Mendelsohn F, Fortuin FD, Pepine CJ, Traverse JH, Amrani D, Ewenstein BM, Riedel N, Story K, Barker K, Povsic TJ, Harrington RA, Schatz RA ACT34-CMI Investigators. Intramyocardial, autologous CD34+ cell therapy for refractory angina. Circ Res. 2011;109:428–436. doi: 10.1161/CIRCRESAHA.111.245993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Burzotta F, Trani C, Romagnoli E, Mazzari MA, Rebuzzi AG, De Vita M, Garramone B, Giannico F, Niccoli G, Biondi-Zoccai GG, Schiavoni G, Mongiardo R, Crea F. Manual thrombus-aspiration improves myocardial reperfusion: the randomized evaluation of the effect of mechanical reduction of distal embolization by thrombus-aspiration in primary and rescue angioplasty (REMEDIA) trial. J Am Coll Cardiol. 2005;46:371–376. doi: 10.1016/j.jacc.2005.04.057. [DOI] [PubMed] [Google Scholar]
- 150.Silva-Orrego P, Colombo P, Bigi R, Gregori D, Delgado A, Salvade P, Oreglia J, Orrico P, de Biase A, Piccalò G, Bossi I, Klugmann S. Thrombus aspiration before primary angioplasty improves myocardial reperfusion in acute myocardial infarction: the DEAR-MI (Dethrombosis to Enhance Acute Reperfusion in Myocardial Infarction) study. J Am Coll Cardiol. 2006;48:1552–1559. doi: 10.1016/j.jacc.2006.03.068. [DOI] [PubMed] [Google Scholar]
- 151.Vlaar PJ, Svilaas T, van der Horst IC, Diercks GF, Fokkema ML, de Smet BJ, van den Heuvel AF, Anthonio RL, Jessurun GA, Tan ES, Suurmeijer AJ, Zijlstra F. Cardiac death and reinfarction after 1 year in the Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS): a 1-year follow-up study. Lancet. 2008;371:1915–1920. doi: 10.1016/S0140-6736(08)60833-8. [DOI] [PubMed] [Google Scholar]
- 152.Svilaas T, Vlaar PJ, van der Horst IC, Diercks GF, de Smet BJ, van den Heuvel AF, Anthonio RL, Jessurun GA, Tan ES, Suurmeijer AJ, Zijlstra F. Thrombus aspiration during primary percutaneous coronary intervention. N Engl J Med. 2008;358:557–567. doi: 10.1056/NEJMoa0706416. [DOI] [PubMed] [Google Scholar]
- 153.Fröbert O, Lagerqvist B, Olivecrona GK, Omerovic E, Gudnason T, Maeng M, Aasa M, Angerås O, Calais F, Danielewicz M, Erlinge D, Hellsten L, Jensen U, Johansson AC, Kåregren A, Nilsson J, Robertson L, Sandhall L, Sjögren I, Ostlund O, Harnek J, James SK. Thrombus aspiration during ST-segment elevation myocardial infarction. N Engl J Med. 2013;369:1587–1597. doi: 10.1056/NEJMoa1308789. [DOI] [PubMed] [Google Scholar]
- 154.Niccoli G, Rigattieri S, De Vita MR, Valgimigli M, Corvo P, Fabbiocchi F, Romagnoli E, De Caterina AR, La Torre G, Lo Schiavo P, Tarantino F, Ferrari R, Tomai F, Olivares P, Cosentino N, D'Amario D, Leone AM, Porto I, Burzotta F, Trani C, Crea F. Open-label, randomized, placebo controlled evaluation of intracoronary adenosine or nitroprusside after thrombus aspiration during primary percutaneous coronary intervention for the prevention of microvascular obstruction in acute myocardial infarction: the REOPEN-AMI study. JACC Cardiovasc Interv. 2013;6:580–589. doi: 10.1016/j.jcin.2013.02.009. [DOI] [PubMed] [Google Scholar]
- 155.Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a delay of lethal cell injury in ischaemic myocardium. Circulation. 1986;74:1124–1136. doi: 10.1161/01.cir.74.5.1124. [DOI] [PubMed] [Google Scholar]
- 156.Staat P, Rioufol G, Piot C, Cottin Y, Cung TT, L'Huillier I, Aupetit JF, Bonnefoy E, Finet G, André-Fouët X, Ovize M. Postconditioning the human heart. Circulation. 2005;112:2143–2148. doi: 10.1161/CIRCULATIONAHA.105.558122. [DOI] [PubMed] [Google Scholar]
- 157.Thibault H, Piot C, Staat P, Bontemps L, Sportouch C, Rioufol G, Cung TT, Bonnefoy E, Angoulvant D, Aupetit JF, Finet G, André-Fouët X, Macia JC, Raczka F, Rossi R, Itti R, Kirkorian G, Derumeaux G, Ovize M. Long term benefit of postconditioning. Circulation. 2008;117:1037–1044. doi: 10.1161/CIRCULATIONAHA.107.729780. [DOI] [PubMed] [Google Scholar]
- 158.Bøtker HE, Kharbanda R, Schmidt MR, Bøttcher M, Kaltoft AK, Terkelsen CJ, Munk K, Andersen NH, Hansen TM, Trautner S, Lassen JF, Christiansen EH, Krusell LR, Kristensen SD, Thuesen L, Nielsen SS, Rehling M, Sørensen HT, Redington AN, Nielsen TT. Remote ischaemic conditioning before hospital admission, as a complement to angioplasty, and effect on myocardial salvage in patients with acute myocardial infarction: a randomised trial. Lancet. 2010;375:727–734. doi: 10.1016/S0140-6736(09)62001-8. [DOI] [PubMed] [Google Scholar]
- 159.Piot C, Croisille P, Staat P, Thibault H, Rioufol G, Mewton N, Elbelghiti R, Cung TT, Bonnefoy E, Angoulvant D, Macia C, Raczka F, Sportouch C, Gahide G, Finet G, André-Fouët X, Revel D, Kirkorian G, Monassier JP, Derumeaux G, Ovize M. Effect of cyclosporine on reperfusion injury in acute myocardial infarction. N Engl J Med. 2008;359:473–481. doi: 10.1056/NEJMoa071142. [DOI] [PubMed] [Google Scholar]
- 160.Mewton N, Croisille P, Gahide G, Rioufol G, Bonnefoy E, Sanchez I, Cung TT, Sportouch C, Angoulvant D, Finet G, André-Fouët X, Derumeaux G, Piot C, Vernhet H, Revel D, Ovize M. Effect of cyclosporine on left ventricular remodeling after reperfused myocardial infarction. J Am Coll Cardiol. 2010;55:1200–1205. doi: 10.1016/j.jacc.2009.10.052. [DOI] [PubMed] [Google Scholar]
- 161.Kitakaze M, Asakura M, Kim J, Shintani Y, Asanuma H, Hamasaki T, Seguchi O, Myoishi M, Minamino T, Ohara T, Nagai Y, Nanto S, Watanabe K, Fukuzawa S, Hirayama A, Nakamura N, Kimura K, Fujii K, Ishihara M, Saito Y, Tomoike H, Kitamura S J-WIND investigators. Human atrial natriuretic peptide and nicorandil as adjuncts to reperfusion treatment for acute myocardial infarction (J-WIND): two randomised trials. Lancet. 2007;370:1483–1493. doi: 10.1016/S0140-6736(07)61634-1. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.