

Abstract
Objective
To analyse the epidemiology of measles in China and determine the progress made towards the national elimination of the disease.
Methods
We analysed measles surveillance data – on the age, sex, residence and vaccination status of each case and the corresponding outcome, dates of onset and report and laboratory results – collected between January 2005 and October 2013.
Findings
Between 2005 and October 2013, 596 391 measles cases and 368 measles-related deaths were reported in China. Annual incidence, in cases per 100 000 population, decreased from 9.95 in 2008 to 0.46 in 2012 but then rose to more than 1.96 in 2013. The number of provinces that reported an annual incidence of less than one case per million population increased from one in 2009 to 15 in 2012 but fell back to one in 2013. Median case age decreased from 83 months in 2005 to 14 months in 2012 and 11 months in January to October 2013. Between 2008 and 2012, the incidence of measles in all age groups, including those not targeted for vaccination, decreased by at least 93.6%. However, resurgence started in late 2012 and continued into 2013. Of the cases reported in January to October 2013, 40% were aged 8 months to 6 years.
Conclusion
Although there is evidence of progress towards the elimination of measles from China, resurgence in 2013 indicated that many children were still not being vaccinated on time. Routine immunization must be strengthened and the remaining immunity gaps need to be identified and filled.
Résumé
Objectif
Analyser l'épidémiologie de la rougeole en Chine et déterminer les progrès réalisés sur la voie de l'élimination nationale de la maladie.
Méthodes
Nous avons analysé les données de surveillance de la rougeole – concernant l'âge, le sexe, le lieu de résidence et le statut vaccinal de chaque cas et les résultats correspondants, les dates de l'apparition et de signalement de la maladie, et les résultats de laboratoire –collectées entre janvier 2005 et octobre 2013
Résultats
Entre 2005 et octobre 2013, 596 391 cas de rougeole et 368 décès liés à la rougeole ont été signalés en Chine. L'incidence annuelle exprimée en cas pour 100 000 habitants a diminué de 9,95 en 2008 à 0,46 en 2012, mais a ensuite augmenté à plus de 1,96 en 2013. Le nombre de provinces ayant signalé une incidence annuelle inférieure à un cas pour un million d'habitants a augmenté de 1 en 2009 à 15 en 2012, mais est retombé à 1 en 2013. L'âge médian des cas a diminué de 83 mois en 2005 à 14 mois en 2012 et à 11 mois pendant la période allant de janvier à octobre 2013. Entre 2008 et 2012, l'incidence de la rougeole dans tous les groupes d'âge, y compris ceux qui ne sont pas ciblés pour la vaccination, a diminué d'au moins 93,6%. Cependant, la résurgence a commencé à la fin de l'année 2012 et s'est poursuivie en 2013. Parmi les cas signalés de janvier à octobre 2013, 40% étaient âgés de 8 mois à 6 ans.
Conclusion
Bien qu'il y ait des preuves de progrès vers l'objectif d'élimination de la rougeole en Chine, la résurgence de 2013 indique que de nombreux enfants n'étaient toujours pas vaccinés à temps. La vaccination de routine doit être renforcée et les lacunes immunitaires restantes doivent être identifiées et comblées.
Resumen
Objetivo
Analizar la epidemiología del sarampión en China y determinar el progreso hecho hacia la erradicación nacional de la enfermedad.
Métodos
Hemos analizado los datos de vigilancia del sarampión recogidos entre enero de 2005 y octubre de 2013 en base a la edad, el sexo, la residencia y el estado de vacunación de cada caso y el resultado correspondiente, las fechas de inicio de la enfermedad y de su comunicación, y los resultados de laboratorio.
Resultados
Entre 2005 y octubre de 2013, se registraron 596 391 casos de sarampión y 368 muertes relacionadas con el sarampión en China. La incidencia anual, en casos por 100 000 habitantes, descendió del 9,95 en 2008 al 0,46 en 2012, pero volvió a aumentar en el 2013 hasta más del 1,96. El número de provincias que informó acerca de una incidencia anual de menos de un caso por millón de habitantes aumentó de una en 2009 a 15 en 2012, pero volvió a caer a una en 2013. La edad media de los casos disminuyó de 83 a 14 meses en 2012, y a 11 meses de enero a octubre de 2013. Entre 2008 y 2012, la incidencia del sarampión en todos los grupos de edad, incluidos los que no estaban incluidos en la vacunación, se redujo en al menos un 93,6 %. Sin embargo, un resurgimiento comenzó a finales de 2012 y continuó en 2013. De los casos comunicados de enero a octubre de 2013, el 40 % tenía entre 8 meses y 6 años.
Conclusión
Aunque hay pruebas de los progresos hacia la erradicación del sarampión en China, el resurgimiento en el año 2013 mostró que todavía hay muchos niños que no reciben la vacuna a tiempo. Es necesario reforzar la vacunación sistemática e identificar y completar las lagunas restantes en la inmunización.
ملخص
الغرض
تحليل وبائيات الحصبة في الصين وتحديد التقدم المحرز تجاه القضاء على الحصبة على الصعيد الوطني.
الطريقة
أجرينا تحليلاً لبيانات ترصد الحصبة – حول العمر والجنس ومحل الإقامة وحالة التطعيم لكل حالة والنتيجة المقابلة، وتواريخ البدء والتقرير ونتائج المختبر – التي تم جمعها بين كانون الثاني/يناير 2005 وتشرين الأول/أكتوبر 2013.
النتائج
بين عام 2005 وتشرين الأول/أكتوبر 2013، تم الإبلاغ عن 596391 حالة حصبة و368 حالة وفاة ناجمة عن الحصبة في الصين. وانخفض معدل الحدوث السنوي، في الحالات لكل 100000 نسمة، من 9.95 في عام 2008 إلى 0.46 في عام 2012 ولكنه ارتفع بعد ذلك إلى أكثر من 1.96 في عام 2013. وزاد عدد المقاطعات التي أبلغت عن حدوث سنوي لأقل من حالة واحدة لكل مليون نسمة من حالة واحدة في عام 2009 إلى 15 في عام 2012، ولكنه انخفض مرة أخرى إلى حالة واحدة في عام 2013. وانخفض العمر المتوسط للحالة من 83 شهرا في عام 2005 إلى 14 شهرا في عام 2012 و11 شهراً في كانون الثاني/يناير 2005 إلى تشرين الأول/أكتوبر 2013. وبين عامي 2008 و2012، انخفض حدوث الحصبة في جميع الفئات العمرية، بما في ذلك تلك التي لم يستهدفها التطعيم، بنسبة 93.6 ٪ على الأقل. ومع ذلك، بدأت عودة الظهور في أواخر عام 2012 واستمر حتى عام 2013. ومن بين الحالات التي تم الإبلاغ عنها في كانون الثاني/يناير حتي تشرين الأول/أكتوبر 2013، كانت نسبة 40 ٪ في عمر 8 أشهر إلى 6 سنوات.
الاستنتاج
على الرغم من وجود أدلة على إحراز تقدم نحو القضاء على الحصبة من الصين، إلا أن عودة الظهور في عام 2013 أشارت إلى أنه لا يزال هناك العديد من الأطفال الذين لا يجري تطعيمهم في الوقت المحدد. ويجب تعزيز التمنيع الروتيني، كما يتعين تحديد ثغرات المناعة المتبقية وسدها.
摘要
目的
分析中国麻疹流行病学,确定全国消除麻疹所取得的进展。
方法
我们分析了2005年1月和2013年10月之间收集的麻疹监测数据,这些数据包括每个病例的年龄、性别、居住地、疫苗接种状态和相应结局、发生和报告日期以及实验室结果。
结果
2005年至2013年10月,中国报告了596391个麻疹病例和368例与麻疹相关的死亡。每十万人口的年发病率从2008年的9.95降低到2012年的0.46,但在其后的2013年上升到1.96以上。报告年发病率少于每百万人口1个病例的省份从2009年的1个增加到2012年的15个,但是在2013年回落到1个。病例年龄中值从2005年的83个月降低到2012年的14个月和2013年1月到10月的11个月。在2008年至2012年之间,所有年龄组(包括非疫苗接种目标人群)麻疹的发病率减少了至少93.6%。但是,在2012年末开始回升,并在2013年继续了这种趋势。在2013年1月到10月报告的病例中,40%病人年龄为8个月到6岁。
结论
虽然,有证据表明中国消除麻疹取得了进展,2013年的反弹显示有的地区很多孩子仍没有及时接种疫苗。必须加强常规疫苗接种,并需要识别和填补余下的免疫空白。
Резюме
Цель
Проанализировать эпидемиологию кори в Китае и оценить результаты элиминации данной болезни в национальном масштабе.
Методы
Были проанализированы данные эпиднадзора за корью (включающие возраст, пол, место проживания, статус вакцинации в каждом случае и соответствующий результат, даты проявления и сообщения о заболевании, а также лабораторные результаты), собранные в период с января 2005 по октябрь 2013 гг.
Результаты
В период с 2005 по октябрь 2013 гг. в Китае было зарегистрировано 596 391 случаев заболевания корью и 368 смертельных исходов. Ежегодная заболеваемость, измеряемая в количестве случаев на 100 000 населения, снизилась с 9,95 случаев в 2008 году до 0,46 в 2012 году, но затем превысила 1,96 случаев в 2013 году. Число провинций, сообщивших о годовой заболеваемости менее одного случая на миллион населения, увеличилось с одной в 2009 году до пятнадцати в 2012 году, но вновь уменьшилось до одной в 2013 году. Средний возраст заболевших уменьшился с 83 месяцев в 2005 году до 14 месяцев в 2012 году и до 11 месяцев в период с января по октябрь 2013 года. В 2008-2012 гг. заболеваемость корью во всех возрастных группах, включая группы, не предназначенные для вакцинации, снизилась как минимум на 93,6%. Тем не менее, в конце 2012 года наблюдался рост заболеваемости, который продолжился в 2013 году. Из числа случаев, зарегистрированных в январе-октябре 2013 года, 40% заболевших были в возрасте от 8 месяцев до 6 лет.
Вывод
Несмотря на имеющиеся доказательства элиминации кори в Китае, рост заболеваемости в 2013 году показал, что многие дети не проходят своевременную вакцинацию. Необходимо усилить меры по плановой иммунизации, а также определить и устранить оставшиеся пробелы в формировании иммунитета.
Introduction
Measles is a highly infectious disease that causes enormous morbidity and mortality among children in many parts of the world. For example, it has been estimated that measles and its complications led to the deaths of more than 164 000 children in 20081 and about 139 300 children in 2010.2
The availability of safe and effective vaccines makes the global elimination of measles possible, at least in theory. By 2011, the Region of the Americas of the World Health Organization (WHO) had sustained measles elimination status for more than a decade. Four of WHO’s other regions have adopted measles elimination targets, while the South-East Asia Region has set itself the task of greatly reducing its measles-related mortality – to less than 5% of the estimated value for the year 2000 – by 2015.3,4
In 2005, the Regional Committee for WHO’s Western Pacific Region resolved to attempt to eliminate measles from the Western Pacific Region by 2012.5 In setting this target, the Committee defined measles elimination as the absence of endemic measles transmission in a defined geographical area for at least 12 months, in the presence of a well performing surveillance system.6
China has a mainland population of more than 1.3 billion and an area of 9.6 million km2 and is the largest country in WHO’s Western Pacific Region. Despite substantial efforts to eliminate measles from China in recent years, measles virus continues to circulate and cause significant morbidity in the country and China accounts for a large proportion of the measles cases reported in the Western Pacific Region.7,8 The elimination of measles in China is therefore critical to achieving the goal of regional measles elimination.
In 1978, China established the national Expanded Programme on Immunization and began to implement a standard schedule for routine immunization that included a dose of measles vaccine administered at 8 months of age. A second routine dose of measles vaccine, at 7 years of age, was recommended in 1986. The 1997 national plan of action for accelerated measles control called for measles vaccine coverage of at least 90%. The recommended age for a child to receive a second dose of measles vaccine was lowered to between 18 and 24 months in 2005.9 The mean annual measles incidence reported in China, in cases per 100 000 population, was 572.0 between 1960 and 1969, 355.3 between 1970 and 1979, 52.9 between 1980 and 1989, and 7.6 between 1990 and 1999,10 and it has remained below 10 since 2000.
In 2006, China endorsed the 2006–2012 national action plan for measles elimination. Subsequently, the country followed a comprehensive strategy for measles elimination, which included immunization, measles surveillance and infection control. Estimated coverage with the first dose of a vaccine containing measles virus increased from 80.4% in 2000 to 91.1% in 2009, while coverage with the second dose of such a vaccine increased from less than 80% before 2005 to 84.3% in 2009.6 Between 2003 and 2009, 27 of the 31 mainland provinces of China conducted unsynchronized province-wide supplementary immunization activities against measles, with 185.7 million children targeted.6 In September 2010, China conducted synchronized nationwide supplementary immunization activities against measles. These nationwide activities, which ignored vaccination status, achieved a reported coverage of 97.52%.11
A national case-based system of measles surveillance with laboratory support has been operational in China since 2009. Over the intervening years, the performance indicators for this system have steadily improved.12 In 2011, the percentage of suspected measles cases investigated within 48 hours of reporting (93.30%), the percentage of suspected measles cases providing an adequate serum specimen (90.37%) and the percentage of serum specimens with laboratory results reported within 7 days of specimen collection (93.85%) exceeded the corresponding target values of 80% for each indicator.13
Programmes for the elimination of measles need to be monitored through the analysis of surveillance data and performance indicators. We report an epidemiological description of data collected in China’s national case-based system of measles surveillance since 2005, and discuss the implications of our findings and the next steps needed for the elimination of measles from China.
Methods
Although measles has been a notifiable disease in China since the 1950s, for many years only aggregate data on measles incidence were submitted to the country’s national level. The National Measles Surveillance Guidelines that were issued in 1998 recommended that case-based measles surveillance be conducted in two selected provinces – Beijing and Shanghai. When the Guidelines were updated, in 2003, it was recommended that such surveillance should be expanded to cover 18 provinces. In 2005, China began to implement a National Notifiable Disease Reporting System that permitted surveillance data to flow from hospitals and county-level Centres for Disease Control to the national Centre for Disease Control and Prevention, through a web-based computerized reporting system. The system collected information on the age, sex, location of residence, date of onset and occupation of each suspected measles case.7,9 It was not until 2009 that the Ministry of Health asked that all of China’s provinces conduct case-based measles surveillance. In this surveillance, a suspected case of measles was defined as any person with fever and rash and one or more of the following symptoms: cough, coryza and conjunctivitis. Also in 2009, the Ministry of Health asked that the vaccination status and laboratory test results of each suspected measles case and the results of any corresponding outbreak investigation be added to the information routinely collected by the National Notifiable Disease Reporting System. In the routine examination of a suspected measles case in China, a serum specimen is collected, sent to a measles laboratory and tested for measles-specific IgM in a commercial enzyme-linked immunosorbent assay. Specimens for the isolation of measles virus may also be collected and all of the resulting viral isolates are sent to the National Measles Laboratory for genotyping.14
For this report, the case-based measles surveillance data reported to the national Centre for Disease Control and Prevention between January 2005 and October 2013 were analysed. In line with China’s current national measles surveillance guideline,15 which was updated in 2009 – i.e. before WHO determined that measles cases in the Western Pacific Region can no longer be confirmed on clinical grounds alone – in this paper the term “measles case” refers to a case confirmed by laboratory testing, epidemiological linkage or clinical criteria. These criteria include (i) fever, (ii) a maculopapular rash and (iii) cough, coryza or conjunctivitis. Case numbers were counted by date of onset and incidences – expressed as the number of cases per 100 000 or million population – were calculated using population denominators provided by China’s National Bureau of Statistics.
Results
Between January 2005 and December 2012, 569 948 measles cases – including 344 measles-related deaths – were recorded in China. Overall, 59.9% of these cases were in males. Annual numbers of cases over the same period ranged from 6183 in 2012 to 131 441 in 2008 – representing annual incidences of 0.46 and 9.95 cases per 100 000 population, respectively. Only 40.2% of the measles cases reported in this period were laboratory confirmed but the percentage of cases that were laboratory confirmed increased from 28.7% in 2005 to 98.3% in 2012 (Fig. 1, Table 1).
Fig. 1.
Monthly numbers of measles cases, January 2005–October 2013, China
a The clinical criteria for case confirmation are (i) fever, (ii) a maculopapular rash and (iii) cough, coryza or conjunctivitis.
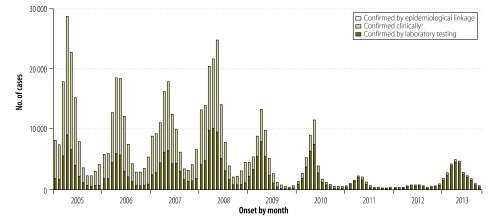
Table 1. Measles cases, January 2005–October 2013, China.
| Variable | Year |
||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013a | |
| Measles incidence (per 100 000 population) | 9.47 | 7.62 | 8.29 | 9.95 | 3.95 | 2.86 | 0.74 | 0.46 | 1.96 |
| No. of measles cases | 123 136 | 99 602 | 109 023 | 131 441 | 52 461 | 38 159 | 9 943 | 6 183 | 26 443 |
| Laboratory confirmation, % of cases | 28.7 | 29.8 | 37.2 | 39.9 | 56.2 | 69.7 | 90.0 | 98.3 | 96.3 |
| Male sex, % of cases | 58 | 59 | 60 | 60 | 61 | 61 | 61 | 59 | 60 |
| No. of measles-related deaths | 56 | 35 | 67 | 103 | 37 | 27 | 10 | 9 | 24 |
| Measles-related mortality, deaths per million population) | 0.042 | 0.027 | 0.05 | 0.077 | 0.029 | 0.02 | 0.007 | 0.006 | 0.02 |
| No. of measles outbreaks reportedb | – | – | – | – | 322 | 311 | 63 | 11 | 91 |
| No. of measles cases in outbreaks | – | – | – | – | 2 205 | 1 994 | 237 | 28 | 368 |
| Median no. of cases per outbreak (range) | – | – | – | – | 3 (2–203) | 3 (2–88) | 2 (2–15) | 2 (2–5) | 2 (2–29) |
| Median duration of outbreak, days (range) | – | – | – | – | 8 (1–114) | 8 (1–163) | 7 (1–56) | 4 (1–13) | 8 (1–44) |
ND, no data.
a The data shown for 2013 refer only to the first 10 months of the year.
b In China, a measles outbreak is defined as the occurrence, within a 10-day period, of either at least two confirmed cases in a village, district, school or similar unit, or at least five confirmed cases in a township.
Although 707 measles outbreaks were recorded between 2009 and 2012, the number, size and duration of such outbreaks decreased annually over this period. The number of measles cases reported in the first 10 months of 2013 – 26 443 – was three times the number reported in the whole of 2012 (Table 1).
Measles showed a similar seasonality in each year between 2005 and 2009, with peaks in incidence in April and May and troughs in August to October (Fig. 1). The troughs in incidence in 2010, 2011 and 2012 were relatively prolonged, from August to December. In 2012 there was no evidence of a peak in April and May, but incidence towards the end of the year was relatively high (Fig. 1). The numbers of cases occurring in November 2012 (556) and December 2012 (897) were 288% and 216% higher, respectively, than the corresponding values in 2011. In 2013 there was, once again, a seasonal peak in April and May (Fig. 1).
Between 2005 and 2008, measles was endemic throughout the country. Over this four-year period, no province had an annual incidence of less than one case per million population and more than 86% of China’s counties reported at least one measles case each year. Only one province (Ningxia) reported an annual incidence of at least 100 cases per million population in 2009 but the number of such provinces rose to four (Beijing, Hebei, Heilongjiang and Tianjin) in 2010 before falling back to one (Tibet) in 2011 and none in 2012. In contrast, one province in 2009 (Hainan), three in 2010 (Fujian, Guangxi and Hainan), four in 2011 (Guangxi, Hainan, Jiangxi and Jilin) and 15 in 2012 reported measles incidences below one case per million population. The percentage of China’s counties that reported at least one measles case in the year decreased from 90.7% in 2008 to 36.4% in 2012. In the first 10 months of 2013, no provinces reported a measles incidence of at least 100 cases per million population but only one province (Heilongjiang) reported less than one measles case per million.
The mean and median ages of the measles cases reported between 2005 and 2012 were 125 and 52 months (interquartile range, IQR: 11–227), respectively. The median age of a case decreased from 83 months (IQR: 13–227) in 2005 to 14 months (IQR: 8–252) in 2012 and just 11 months in January to October 2013. In each year that we investigated, the age group showing the highest incidence of measles was either that of children younger than 8 months – that is, those who were too young to receive a first dose of measles-virus-containing vaccine – or children aged 8 to 23 months – that is, those who were eligible for one or both scheduled doses of measles-virus-containing vaccine. The annual incidence of measles in each age group has gradually decreased since 2008. Compared with the values for 2008, for example, the annual incidences recorded in 2012 were 93.6%, 93.6%, 96.7%, 98.6%, 96.1% and 93.9% lower among those aged less than 8 months, 8 to 23 months, 2 to 6 years, 7 to 14 years, 15 to 34 years and more than 34 years, respectively. Between 2005 and 2012, the percentage of the year’s measles cases that occurred in infants aged less than 8 months increased from 11.3% to 24.5% and the percentage of the year’s measles cases that occurred in children aged 8 to 23 months increased from 19.4% to 33.9%. There were corresponding decreases in the percentages of the year’s measles cases recorded among children aged 2 to 6 and 7 to 14 years, which fell from 21.4% to 11.9% and from 17.4% to just 2.4%, respectively. The percentage of the cases reported in the first 10 months of 2013 that occurred in infants aged less than 8 months was greater than the corresponding value for the whole of 2012 (31% versus 21%; Fig. 2).
Fig. 2.
Yearly numbers of measles cases divided by age group, 2005–2013, China
Note: The data shown for 2013 refer only to the first 10 months of the year.

The annual number of measles-related deaths ranged from 9 in 2012 to 103 in 2008 (Table 1). There were many more such deaths in the first 10 months of 2013 (n = 24) than in the whole of 2012 (n = 9). Of the measles-related deaths that occurred in January to October 2013, 13 (54.2%), 8 (33.3%) and 3 (12.5%) were among children aged less than 8 months, 8 to 23 months and 24 to 82 months, respectively.
Of the 123 159 measles cases that were reported with residence information between January 2009 and October 2013, only 9.4% had a record of migrating no more than 3 months before they developed a rash but 47.8% were living in a county in which they had not been born when their rash developed. The percentage of measles cases with known place of residence that were living in a county in which they had not been born when their rash developed increased steadily, from 36.8% in 2009 to 57.7% for the first 10 months of 2013. Paediatric cases of measles were more likely to have vaccination records than the adult cases (Table 2). Overall, 31 159 cases aged 8 to 23 months were reported between January 2009 and December 2012. Just over half (53%) of these cases were unvaccinated. The corresponding proportion for the first 10 months of 2013 was relatively large (72%). Similarly, the proportion of cases aged 2 to 6 years that were unvaccinated was twice as high for the first 10 months of 2013 as for the period from 2009 to 2012 (Table 2).
Table 2. Vaccination histories of measles cases, January 2009–October 2013, China.
| Month of onset | Age group | Vaccination status, no. (%) |
|||||
|---|---|---|---|---|---|---|---|
| No dose of MCV | One dose of MCV | Two or more doses of MCV | Unknown | Total | |||
| Jan 2009–Dec 2012 | < 8 months | 21 972 (100) | 0 | 0 | 0 | 21 972 | |
| 8–23 months | 16 607 (53) | 7 649 (25) | 613 (2) | 6 290 (20) | 31 159 | ||
| 2–6 years | 3 931 (26) | 3 248 (21) | 2 998 (20) | 4 975 (33) | 15 152 | ||
| 7–14 years | 1 121 (17) | 1 093 (16) | 1 430 (21) | 3 148 (46) | 6 792 | ||
| ≥ 15 years | 7 398 (24) | 1379 (4) | 653 (2) | 22 241 (70) | 31 671 | ||
| All | 47 673 (45) | 13 585 (13) | 5 706 (55) | 39 782 (37) | 106 746 | ||
| Jan–Oct 2013 | < 8 months | 8 148 (100) | 0 | 0 | 0 | 8 148 | |
| 8–23 months | 5 629 (72) | 1 354 (17) | 100 (1) | 741 (10) | 7 824 | ||
| 2–6 years | 1440 (53) | 347 (13) | 438 (16) | 509 (18) | 2 734 | ||
| 7–14 years | 171 (28) | 77 (13) | 147 (24) | 211 (35) | 606 | ||
| ≥ 15 years | 1 436 (20) | 275 (4) | 80 (1) | 5 340 (75) | 7 131 | ||
| All | 16 555 (63) | 2 081 (8) | 768 (3) | 7 039 (26) | 26 443 | ||
MCV, measles-virus-containing vaccine.
Between 2009 and 2012, genotype information was reported via the measles surveillance system for just 1324 (1.2%) of the measles cases recorded over the same period. Of the genotyped isolates, 1300 (98.2%) were genotype H1, one was D4, one was D8, one was D11 and 15 were D9.
Genotype was also reported for more than 1600 (about 6.2%) of the measles cases recorded in the first 10 months of 2013. Of the genotyped isolates made in 2013, 96% were H1, 2% were D9 and 2% were D8.
Discussion
In 2006, China committed to eliminate measles and implemented strategies to interrupt the indigenous transmission of measles virus. Our analysis of measles epidemiology from 2005 to 2012 showed a steady decrease in the annual incidence of measles in China. However, there was a resurgence of measles in 2013, with a seasonal peak in April and May of that year. It therefore appears that more effort will be needed to eliminate indigenous transmission of measles virus in China.
The national incidence of measles in China decreased substantially – from 100 cases per million population in 2008 to 4.6 cases per million in 2012 – before rebounding to 19.6 per million in just the first 10 months of 2013. Similarly, although 15 of China’s 31 mainland provinces reported annual incidences of measles below one case per million population in 2012, only one province reported such a low incidence in the first 10 months of 2013. By 2011, surveillance for measles in China at the national level was meeting most of WHO’s quality criteria.16
Since 2008, most of the progress made in the elimination of measles in China has been achieved through the concerted efforts of the national Expanded Programme on Immunization, often in collaboration with the country’s educational system. The policies followed for measles immunization in China have been similar to those used in countries that have successfully eliminated measles. For example, China has implemented a two-dose policy of measles vaccination for more than 25 years using effective measles vaccines. High coverage has been achieved with both measles vaccine doses. Since 2009, for example, the first dose of measles-virus-containing vaccine has reached more than 90% of the target population. China also conducted province-level supplemental immunization activities with a measles vaccine between 2003 and 2009. In 2010, it conducted a very large, nationwide campaign of supplemental immunization activities against measles in which more than 100 million children were vaccinated in a three-week period. China has also used checks on children entering schools and kindergartens to help to ensure that school-age children are – or have been – vaccinated against measles.
Before the implementation of the 2006 measles action plan – as well as in the action plan’s early years – several of China’s provinces conducted supplemental immunization activities that were designed to stop the transmission of measles virus among children aged 8 months to 14 years – that is, the age group with the highest incidence of measles. There were two such provinces (Guizhou and Xinjiang) in 2004,17,18 two (Ningxia and Zhejiang) in 2005,19 four (Hainan, Jilin, Qinghai and Tibet) in 2006 and three (Hebei, Shaanxi and four prefectures of Sichuan) in 2007.20 In the years following these activities, dramatic decreases in the reported incidence of measles cases were recorded in each of these provinces. However, these province-level activities appeared to have little impact on measles incidence at the national level. In 2008, for example, the national incidence of measles was higher than at any other time in the past 15 years. Although a coordinated nationwide campaign of measles vaccination was considered, such a campaign was prevented by limitations in the vaccine supply and programme capacity and provinces were left to organize their own activities using a variety of vaccination strategies.21 However, after a fairly large “catch-up” campaign of supplemental immunization activities that covered 19 provinces in 2008 and 2009,22 there was a clear need for a nationwide campaign. The 2010 nationwide campaign – again based on supplemental immunization activities – seems to have been largely successful, since it was soon followed by relatively low measles incidences. Encouragingly, the decreases seen in measles incidence were not restricted to vaccine-targeted children but were also recorded among infants who were too young to vaccinate and adults who were also not targeted in the campaign.
Additional efforts needed
The resurgence of measles in 2013 occurred primarily among young, unvaccinated children, including infants who were too young to have been vaccinated and children of pre-school age who had missed one or both of their scheduled vaccinations. Despite the use of strong policies and programmes for measles vaccination, the H1 measles genotype continues to circulate in almost all of China’s provinces. The H1 genotype is the only indigenous measles genotype in China. Since there is no non-human reservoir for measles, the circulation of this genotype represents person-to-person transmission that has persisted in China for at least 20 years.23
The elimination of measles in China will require all of the remaining immunity gaps to be identified and filled – to the point that transmission of measles virus can no longer be sustained. If immunity gaps are to be identified and adequately filled, case investigation and outbreak analysis and response may all need to be improved. Measles virus is so highly transmissible that it is able to travel along chains of transmission even among relatively well vaccinated populations and infect groups of susceptible individuals – especially unvaccinated young children.24 The resurgence of measles seen among young unvaccinated Chinese children in 2013 indicates a weakness in routine immunization that allows some children to miss one or both of their scheduled doses of measles vaccine. Such weakness must be eliminated if a further resurgence in the next few years is to be avoided and measles is ever to be eliminated in China.
The knowledge that the routine programme of measles vaccination has weaknesses is important. Surveillance and outbreak analysis can provide information about who is acquiring measles and about the immunity gaps in target populations. Additional studies are needed to identify why, in the routine programme, not all of the eligible children are being vaccinated in a timely manner. Are children missing immunization opportunities at health-care encounters? Are children who have recently relocated not been identified and enrolled in an immunization clinic in a timely manner? Research on health services and health-care seeking may be useful in identifying the reasons that some children are missing measles vaccinations. Such studies have been found useful in countries that have already eliminated measles by strengthening routine immunization25 and could well be beneficial in China.26 Records-based surveys of vaccine coverage may also help to identify any gaps in population immunity and the main risk factors for failure to be vaccinated.27
In China, huge numbers of individuals are currently migrating from rural areas to towns and cities, largely in search of employment. Children who have moved county since birth – including those of individuals who have relocated in this fashion – are less likely to be fully vaccinated than local children.28–31 Improvements in the identification and location of children who are new to an area may permit marked improvements in vaccine coverage.
In 2013, most of the resurgence seen in measles cases was the result of the susceptibility of unvaccinated or incompletely vaccinated children – as has been the experience in some other countries.32,33 In some of China’s provinces, however, 2013 saw an increasing incidence of measles among adults. Although most adults in China are immune to measles, few have records of their vaccination status. The resulting general inability to distinguish immune adults from the non-immune without testing each individual makes campaigns of adult vaccination against measles difficult or inefficient.
In conclusion, although substantial progress was made in China between 2005 and 2012 towards the elimination of measles, there was a resurgence of the disease – mostly among young, unvaccinated children – in 2013. This resurgence started only two years after a nationwide campaign based on supplementary immunization activities and occurred primarily among children who became age-eligible for measles vaccination after that campaign. The strengthening of routine immunization programmes, so that measles vaccine can be administered on time to virtually all age-eligible children, is a challenge that will have to be met in order for China to eliminate measles.
Acknowledgements
We thank the staff of each province-, prefecture- and county-level Center for Disease Control and Prevention. We are also grateful to Peter Strebel and Walter A Orenstein for their valuable comments. Three of the authors (CM, LH and YZ) contributed equally to this article.
Competing interests:
None declared.
References
- 1.World Health Organization Global reductions in measles mortality 2000–2008 and the risk of measles resurgence. Wkly Epidemiol Rec. 2009;84:509–16. [PubMed] [Google Scholar]
- 2.Simons E, Ferrari M, Fricks J, Wannemuehler K, Anand A, Burton A, et al. Assessment of the 2010 global measles mortality reduction goal: results from a model of surveillance data. Lancet. 2012;379:2173–8. doi: 10.1016/S0140-6736(12)60522-4. [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization Progress in global control and regional elimination of measles, 2000–2011. Wkly Epidemiol Rec. 2013;88:29–36. [PubMed] [Google Scholar]
- 4.Measles elimination by 2020 [Internet]. New Delhi: World Health Organization Regional Office for South-East Asia; 2013. Available from: http://www.searo.who.int/mediacentre/releases/2013/pr1565/en/index.html [accessed 9 January 2014].
- 5.World Health Organization Monitoring progress towards measles elimination. Wkly Epidemiol Rec. 2010;85:490–4. [PubMed] [Google Scholar]
- 6.Guidelines on verification of measles elimination in the Western Pacific Region Manila: World Health Organization, Western Pacific Region; 2013. Available from: http://www.wpro.who.int/immunization/documents/measles_elimination_verification_guidelines_2013/en/index.html [accessed 9 January 2014].
- 7.World Health Organization Progress towards the 2012 measles elimination goal in WHO’s Western Pacific Region, 1990–2008. Wkly Epidemiol Rec. 2009;84:271–9. [PubMed] [Google Scholar]
- 8.Li J, Lu L, Pang X, Sun M, Ma R, Liu D, et al. A 60-year review on the changing epidemiology of measles in capital Beijing, China, 1951–2011. BMC Public Health. 2013;13:986. doi: 10.1186/1471-2458-13-986. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ma C, An Z, Hao L, Cairns KL, Zhang Y, Ma J, et al. Progress toward measles elimination in the People’s Republic of China, 2000–2009. J Infect Dis. 2011;204(Suppl 1):S447–54. doi: 10.1093/infdis/jir103. [DOI] [PubMed] [Google Scholar]
- 10.Lixia W, Guang Z, Lee LA, Zhiwei Y, Jingjin Y, Jun Z, et al. Progress in accelerated measles control in the People’s Republic of China, 1991–2000. J Infect Dis. 2003;187(Suppl 1):S252–7. doi: 10.1086/368045. [DOI] [PubMed] [Google Scholar]
- 11.Ma C, Hao L, Ma J, Zhang Y, Cao L, Liang X, et al. Measles epidemiological characteristics and progress of measles elimination in China, 2010. Chin J Vaccin Immun. 2011;17:242–5. Chinese. [Google Scholar]
- 12.Ma C, Hao L, An Z, Ma J, Zhang Y, Xu W, et al. Establishment and performance of measles surveillance system in the People’s Republic of China. Chin J Vaccin Immun. 2010;16:297–306. Chinese. [Google Scholar]
- 13.Ma C, Su Q, Hao L, Zhang Y, Xu W, Luo H. Performance of measles surveillance system in the People's Republic of China, 2011. Chin J Vaccin Immun. 2012;18:481–4. Chinese. [Google Scholar]
- 14.Xu W, Zhu Z, Jiang X, Zhang Y, Cui A, Mao N, et al. Establishment and running status of measles laboratory network in China. Chin J Vaccin Immun. 2006;12:1–6. Chinese. [Google Scholar]
- 15.National measles surveillance guideline Beijing: Chinese Ministry of Health; 2009. Available from: http://www.moh.gov.cn/jkj/s3581/200902/9ea8e400444c45b0a48e3e55d929c9b5.shtml [accessed 2 February 2014]. Chinese.
- 16.Measles elimination field guide [Internet]. Geneva: World Health Organization; 2013. Available from: http://www.wpro.who.int/immunization/documents/measles_elimination_field_guide_2013.pdf [accessed 9 January 2014].
- 17.Zuo S, Lian X, Yin D, You X, Guo B, Tong Y, et al. Measles Mass Campaign experience and effect evaluation of Guizhou province, 2003-2004. Chin J Vaccin Immun. 2006;12:7–12. Chinese. [Google Scholar]
- 18.Yu X, Liu Q, Guan J, Ma H, Re Y, Xu X, et al. Evaluation of measles mass campaign of Xinjiang Uygur Automous Region in 2004. Chin J Vaccin Immun. 2006;12:373–5. Chinese. [Google Scholar]
- 19.Zhou L, Rui J, Fu Y, Li H, Li S, Lu W, et al. Evaluation measles mass campaign of NingXia Hui Autonomous Region in 2005. Chin J Pest Control 200723820–2.Chinese [Google Scholar]
- 20.Ma C, Luo H, An Z, Zhang P, Wen N, Xia W, et al. Analysis on epidemiological characteristics and measures of measles control in China during 2006-2007. Chin J Vaccin Immun. 2008;14:208–13. Chinese. [Google Scholar]
- 21.Liang X, Yin D, Li L, Wang L, Zuo S, Wen N, et al. Requirement of measles vaccine of the elimination of measles in China during period of 2006-2012. Chin J Vaccin Immun. 2005;11:398–401. Chinese. [Google Scholar]
- 22.Hao L, Ma C, Ma J, An Z, Luo H, Liang X. Analysis on epidemiological characteristics of measles in China from 2008-2009. Chin J Vaccin Immun. 2010;16:293–6. Chinese. [Google Scholar]
- 23.Zhang Y, Xu S, Wang H, Zhu Z, Ji Y, Liu C, et al. Single endemic genotype of measles virus continuously circulating in China for at least 16 years. PLoS One. 2012;7:e34401. doi: 10.1371/journal.pone.0034401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Domínguez A, Torner N, Barrabeig I, Rovira A, Rius C, Cayla J, et al. Working Group for the Study of the Measles Outbreak in Catalonia Large outbreak of measles in a community with high vaccination coverage: implications for the vaccination schedule. Clin Infect Dis. 2008;47:1143–9. doi: 10.1086/592258. [DOI] [PubMed] [Google Scholar]
- 25.Orenstein WA. The role of measles elimination in development of a national immunization program. Pediatr Infect Dis J. 2006;25:1093–101. doi: 10.1097/01.inf.0000246840.13477.28. [DOI] [PubMed] [Google Scholar]
- 26.Gao J, Chen E, Wang Z, Shen J, He H, Ma H, et al. Epidemic of measles following the nationwide mass immunization campaign. BMC Infect Dis. 2013;13:139. doi: 10.1186/1471-2334-13-139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hinman AR, Orenstein WA, Papania MJ. Evolution of measles elimination strategies in the United States. J Infect Dis. 2004;189(Suppl 1):S17–22. doi: 10.1086/377694. [DOI] [PubMed] [Google Scholar]
- 28.Hu Y, Li Q, Luo S, Lou L, Qi X, Xie S. Timeliness vaccination of measles containing vaccine and barriers to vaccination among migrant children in East China. PLoS One. 2013;8:e73264. doi: 10.1371/journal.pone.0073264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hu Y, Li Q, Chen E, Chen Y, Qi X. Determinants of childhood immunization uptake among socio-economically disadvantaged migrants in East China. Int J Environ Res Public Health. 2013;10:2845–56. doi: 10.3390/ijerph10072845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hu X, Xiao S, Chen B, Sa Z. Gaps in the 2010 measles SIA coverage among migrant children in Beijing: evidence from a parental survey. Vaccine. 2012;30:5721–5. doi: 10.1016/j.vaccine.2012.07.007. [DOI] [PubMed] [Google Scholar]
- 31.Sun M, Ma R, Zeng Y, Luo F, Zhang J, Hou W. Immunization status and risk factors of migrant children in densely populated areas of Beijing, China. Vaccine. 2010;28:1264–74. doi: 10.1016/j.vaccine.2009.11.015. [DOI] [PubMed] [Google Scholar]
- 32.Muscat M, Bang H, Wohlfahrt J, Glismann S, Mølbak K, EUVAC.NET Group Measles in Europe: an epidemiological assessment. Lancet. 2009;373:383–9. doi: 10.1016/S0140-6736(08)61849-8. [DOI] [PubMed] [Google Scholar]
- 33.Delaporte E, Wyler Lazarevic CA, Iten A, Sudre P. Large measles outbreak in Geneva, Switzerland, January to August 2011: descriptive epidemiology and demonstration of quarantine effectiveness. Euro Surveill. 2013;18:18. [PubMed] [Google Scholar]