

Abstract
WE EXAMINED THE PREVALENCE OF DIETING and negative eating attitudes among 2279 females (aged 10–14 years) in southern Ontario. Self-report questionnaires revealed that 29.3% of the girls were currently trying to lose weight and 10.5% had scores greater than the clinical threshold for disordered eating (Children's version of the Eating Attitudes Test [ChEAT] score ≥ 20). Those with elevated ChEAT scores were more likely than those with lower scores to be engaged in dieting and other extreme weight control methods.
A Canadian study published in 2001 reported that 23% of adolescent females were dieting to lose weight.1 Outside of Canada, a high prevalence of dieting has also been reported among preadolescent females.2 Dieting has been identified as a risk factor for eating disorders3,4 and the associated chronic health problems.5 A recent longitudinal study involving 14 972 males and females between the ages of 9 and 14 years revealed that dieting to control weight was not only ineffective but actually led to weight gain.6 The weight gain appeared to result from a cycle of restrictive dieting followed by bouts of overeating or binge eating. If the trend toward girls dieting at a younger age is also found in Canada, additional risk factor research will be required to foster the development of age-appropriate prevention programs.
Given the evidence that dieting in children is being reported at earlier ages,2,7,8 the present cross-sectional study was designed to assess the prevalence of dieting and negative eating attitudes and behaviours among girls aged 10 to 14 years in southern Ontario.
Between 1993 and 2003, 2279 pre- and early adolescent girls (mean age 11.8 years, standard deviation [SD] 0.9) were recruited from 42 schools in southern Ontario (grades 6–8). Ethics approval was obtained from hospital and local school boards; parental consent and student oral assent were also obtained. Participants completed the Children's version of the Eating Attitudes Test (ChEAT) to assess eating attitudes and behaviours. In addition to the ChEAT, participants were asked to report on pubertal status, weight and height for calculation of body mass index (BMI) (kg/m2) and whether they were currently trying to lose weight.
A majority of the subjects were Canadian-born (78.3%) and reported English as their first language (75.1%). Nearly half of the total sample (46.4%) reported that they had had their first menses. The mean BMI for the total sample was 18.8 (SD 5.4). About 78.4% of the girls fell within the recommended BMI range for their age group, with 14.4% below and 7.2% above the range for their age.9 Participants' weight perceptions ranged from 31.3% of the total sample feeling “too fat,” to 58.9% feeling “just right” and 9.8% feeling “too thin.” Although some concern has been raised over the validity of using self-reported height and weight in young females, it is felt that the impact of potential over- or underestimating is likely minimal given recent studies that have shown that selfreports are reliable means of classifying weight status in adolescents.10,11
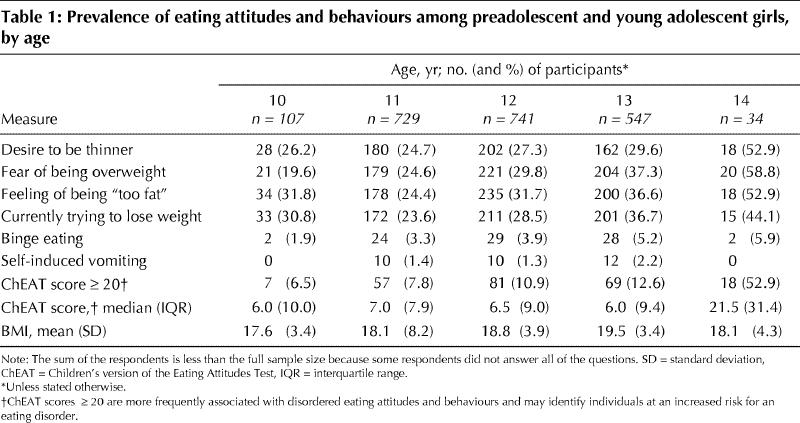
The mean ChEAT score for the entire sample was 9.3 (SD 9.0), with 10.5% reporting ChEAT scores above the clinical threshold score of 20. ChEAT scores of 20 or more have been associated with more disturbed eating attitudes and behaviours and an increased vulnerability toward development of an eating disorder.12 A total of 29.3% answered Yes to the question “Are you currently trying to lose weight?” Binge eating and self-induced vomiting occurred regularly in only 3.9% and 1.5% of the overall sample respectively.
Using a one-way analysis of variance controlling for BMI, a significant main effect of age on total ChEAT scores was found (F [4,1677] 30.43, p < 0.001) (Table 1). Posthoc multiple comparisons, using Bonferroni corrections, showed that 14-year-old girls had significantly higher scores than all other age groups (p < 0.001). Similar age differences were found on the ChEAT subscales (dieting, bulimia, food preoccupation and oral control) (p < 0.001).
Table 1
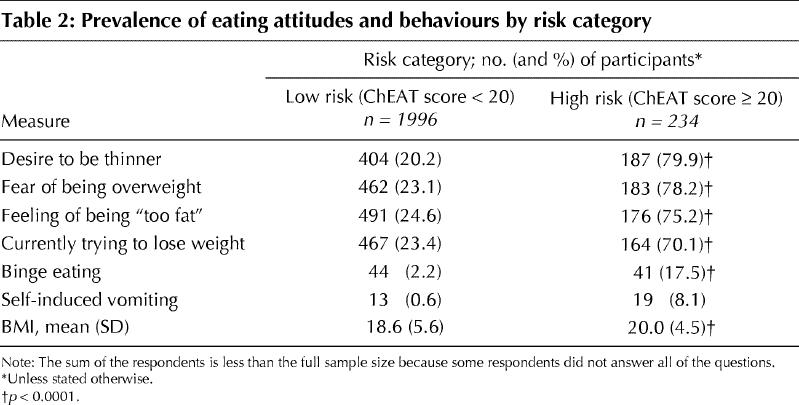
Eating and weight loss behaviours among girls with normal and elevated ChEAT scores are compared in Table 2. The girls with scores of 20 or higher were significantly more likely to be trying to lose weight and engaging in other extreme weight control methods and attitudes (e.g., vomiting, binge eating). The high-risk group had significantly higher BMI scores, an association reported elsewhere with older females.1 However, the majority of the present sample (92.7%) were within, or below, the normal weight range for their age and height.
Table 2
Although previous studies examined adolescent girls,1 our study suggests that unhealthy dieting behaviours are reported in girls as young as 10 years of age (Table 1). The potential negative health outcomes associated with dieting and disordered eating stress the need for primary prevention efforts to begin at the elementary school level. Our findings highlight an opportunity for prevention strategies for girls during the preadolescent phase that will avert future disordered eating behaviours. It is logical that any such program would be distinct from those aimed at older adolescent girls, for whom strategies for prevention and normalization of existing disordered behaviours are necessary.13,14,15
Formal training of educators and public health practitioners in the prevention of disordered eating in adolescent girls has begun in Ontario (G.M., unpublished data, 2003) Although this is an essential first step, it is imperative that primary care physicians also help to disseminate these prevention messages more widely.
Footnotes
This article has been peer reviewed.
Contributors: As lead investigator, Gail McVey headed the development of the project, collected the data and drafted the manuscript. Stacey Tweed and Elizabeth Blackmore contributed substantially to the conception and design of the study, interpretation and analysis of the data and revision of the manuscript. All authors approved the final version of the manuscript.
Competing interests: None declared.
Correspondence to: Gail McVey, Community Health Systems Resource Group, The Hospital for Sick Children, 555 University Ave., Toronto ON M5G 1X8; fax 416 813-7258; gail.mcvey@sickkids.ca; or the Outreach Program for Eating Disorders, tel 800 463-1856
References
- 1.Jones JM, Bennett S, Olmsted MP, Lawson ML, Rodin G. Disordered eating attitudes and behaviours in teenaged girls: a school-based study. CMAJ 2001; 165(5):547-52. [PMC free article] [PubMed]
- 2.Ricciardelli LA, McCabe MP. Children's body image concerns and eating disturbance: a review of the literature. Clin Psychol Rev 2001:21(3):325-44. [DOI] [PubMed]
- 3.Marchi M, Cohen P. Early childhood eating behaviours and adolescent eating disorders. J Am Acad Child Adolesc Psychiatry 1990;29:112-7. [DOI] [PubMed]
- 4.Patton GC, Johnson-Sabine E, Wood K, Mann AH, Wakeling A. Abnormal eating attitudes in London schoolgirls — a prospective epidemiological study: outcome at twelve month follow-up. Psychol Med 1990;20:383-94. [DOI] [PubMed]
- 5.Fisher M, Golden NH, Katzman DK, Kreipe RE, Rees J, Schebendach J, et al. Eating disorders in adolescents: a background paper. J Adolesc Health 1995;16(6):420-37. [DOI] [PubMed]
- 6.Field AE, Austin SB, Taylor CB, Malspeis S, Rosner B, Rockett HR, et al. Relation between dieting and weight change among preadolescents and adolescents. Pediatrics 2003;112(4):900-6. [DOI] [PubMed]
- 7.Hill AJ, Oliver S, Rogers PJ. Eating in the adult world: the rise of dieting in childhood and adolescence. Brit J Clin Psychol 1992;31:95-105. [DOI] [PubMed]
- 8.Maloney MJ, McGuire JB, Daniels SR, Specker B. Dieting behavior and eating attitudes in children. Pediatrics 1989;84:482-9. [PubMed]
- 9.Hammer LD, Kraemer HC, Wilson DM, Ritter PL, Dornbusch SM. Standardized percentile curves of body-mass index for children and adolescents. Am J Dis Child 1991;145:259-63. [DOI] [PubMed]
- 10.Goodman E, Hinden B, Khandelwal S. Accuracy of teen and parental reports of obesity and body mass index. Pediatrics 2000;106:52-8. [DOI] [PubMed]
- 11.Strauss RS. Comparison of measured and self-reported weight and height in a cross-sectional sample of young adolescents. Int J Obes Relat Metab Disord 1999;23:904-8. [DOI] [PubMed]
- 12.Maloney MJ, McGuire JB, Daniels SR. Reliability testing of a children's version of the Eating Attitude Test. J Am Acad Child Adolesc Psychiatry 1988;27: 541-3. [DOI] [PubMed]
- 13.McVey GL, Pepler D, Davis R, Flett GL, Abdolell M. Risk and protective factors associated with disordered eating during early adolescence. J Early Adolesc 2002;22(1):75-95.
- 14.McVey GL, Lieberman M, Voorberg N, Wardrope D, Blackmore E. School based peer support groups: a new approach to the prevention of disordered eating. Eat Disord J Treat Prev 2003;11(8):169-86. [DOI] [PubMed]
- 15.McVey GL, Davis R, Tweed S, Shaw BF. Evaluation of a school based program designed to improve body image satisfaction, global self-esteem, and eating attitudes and behaviours: a replication study. Int J Eat Disord. In press. [DOI] [PubMed]