

Abstract
Metabolic syndrome (MetS) has been redefined by a new criterion in Japan, in which waist circumference cut‐off points, that is 85 cm for men and 90 cm for women, are used; however, objections are rising against this criterion. The present study examined the criterion for waist circumference to predict the accumulation of the components of MetS. In the present study, we used data for 5972 Japanese people who received annual health examinations, and 621 men (16.3%) and 51 women (2.4%) were diagnosed as having MetS. A cut‐off point as a predictor for two or more components of MetS was evaluated by the sensitivity/specificity and a receiver operating characteristic analysis. The optimal point of waist circumference was estimated as being approximately 84 cm for men and 80 cm for women. We therefore recommend revising the cut‐off value for the criterion of MetS in women according to our results and studies from other investigators. (J Diabetes Invest, doi: 10.1111/j.2040‐1124.2010.00020.x, 2010)
Keywords: Metabolic syndrome, Waist circumference, Cut‐off point
Introduction
Metabolic syndrome (MetS), which is defined by multiple risk factors, including central obesity, high blood pressure, dyslipidemia, and high fasting blood glucose; and persons with MetS have an elevated risk of developing cardiovascular disease (CVD), which is correlated with all‐cause mortality1. Because the morbidity and mortality of CVD is rapidly increasing worldwide2, establishing appropriate screening for MetS is essential to prevent the initiation and progression of CVD.
To date, internationally recognized definitions of MetS have been released, namely the criteria of the World Health Organization (WHO)3, the National Cholesterol Education Program’s Adult Treatment Panel III (NCEP‐ATP III)4, and the International Diabetes Federation (IDF)5. In Japan, a criterion for MetS has been defined as the presence of central obesity (85 cm for men and 90 cm for women) plus any two of the following three factors; (i) dyslipidemia; (ii) high blood pressure; and (iii) impaired fasting glucose6. In contrast, the IDF recommended cut‐off levels of 90 cm for men and 80 cm for women for central obesity in Asian individuals5. There has been controversy as to which of these cut‐off points of waist circumference is better for diagnosing central obesity in Japanese men and women. The aim of the present article is to re‐evaluate the waist circumference for detecting the risk factor accumulation of MetS in Japanese subjects.
Subjects and Methods
The total number of participants in the present study was 5972 (3811 men and 2161 women), aged 20–79 years, who received annual health examinations at Okayama Red Cross General Hospital with informed consent. We measured waist circumference at the umbilical level. MetS was defined among men and women as waist circumferences in excess of 85 cm and 90 cm6, respectively, in addition to having two or more of the following components: (i) dyslipidemia: triglycerides ≥ 150 mg/dL and/or HDL cholesterol <40 mg/dL; (ii) high blood pressure: blood pressure ≥ 130/85 mmHg; and (iii) impaired fasting glucose: fasting plasma glucose ≥ 110 mg/dL6. If an individual was receiving drug therapy for hypertriglyceridemia, low HDL cholesterol, high blood pressure or diabetes mellitus, each item was recorded as a positive finding regardless of the data. To identify the optimal cut‐off point of waist circumference as a predictor of the presence of at least two components comprising the MetS, we carried out receiver operating characteristic (ROC) analysis. The statistical software spss for Windows (version 8.0; SPSS, Chicago, IL, USA) was used for the analysis.
Results
The mean age of the study subjects was 49.9 ± 10.1 years for men and 48.6 ± 9.4 years for women. Among the 5972 Japanese subjects, 1744 men (45.8%) had a waist circumference in excess of 85 cm and 216 women (10.0%) had a waist circumference exceeding 90 cm. In addition, the prevalence of MetS according to the Japanese diagnostic criteria was 621 (16.3%) for men and 51 (2.4%) for women.
We investigated the sensitivity and specificity of waist circumference in predicting the association with two or more metabolic risk factors; that is dyslipidemia, high blood pressure and impaired fasting glucose. In men, the sensitivity and specificity of the waist circumference criterion, that is 85 cm, were 64.2% and 60.2%, respectively. However, in women, the sensitivity and specificity of waist circumference criterion, that is 90 cm, were found to be 29.3% and 91.5%, respectively. A cut‐off point as a predictor for two or more components of MetS was evaluated by sensitivity/specificity curves, as well as a ROC curve. The optimal point yielding the maximal sensitivity plus specificity for predicting two or more risk factors was estimated to be approximately 84 cm (sensitivity: 66.3%, specificity: 59.4%) of waist circumference for men and 80 cm (sensitivity: 69.0%, specificity: 65.4%) for women (Figure 1). Based on these findings, 1966 men (51.6%) and 718 women (33.2%) had a waist circumference exceeding 84 cm and 80 cm, respectively. In addition, 675 men (17.7%) and 119 women (5.5%) were diagnosed as having MetS by using 84 cm for men and 80 cm for women as the waist circumference criterion.
Figure 1.
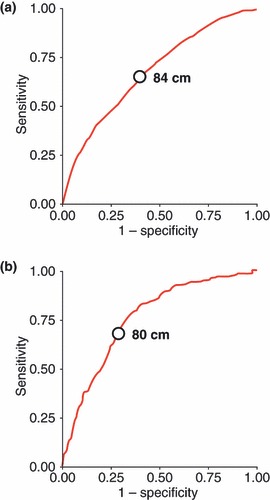
Receiver operating characteristic (ROC) curve of waist circumference for detecting two or more risk factors of the metabolic syndrome in (a) men and (b) women. ○, Cut‐off waist circumference yielding the maximal sensitivity plus specificity for predicting the presence of multiple risk factors.
Discussion
The IDF has used a waist circumference cut‐off value of 90 cm for men and 80 cm for women as its diagnostic criteria of MetS for Asians5. In contrast, the waist circumference cut‐off value for Japanese was 85 cm for men and 90 cm for women, which correspond to 100 cm2 of intraperitoneal visceral fat in a cross‐section at the height of the navel as shown by computed tomography (CT) both for men and women6. To address this controversial point, we re‐evaluated the cut‐off points of waist circumference for the diagnosis of MetS using ROC analysis. We proposed that the optimal cut‐off points are 84 cm for men and 80 cm for women for predicting the clustering of the components of MetS. In men, the criterion of waist circumference deduced from the present study was matched to that of the criterion of MetS in Japan. However, in women, the cut‐off value of waist circumference in the present study was lower than that of the criterion.
The first report that estimated the waist circumference cut‐off value for diagnosis of MetS in Japan was a study of 3574 employees of a telephone company and their family members (2947 men and 627 women). It estimated the optimal cut‐off value for the intraperitoneal visceral fat area at the height of the navel, as determined by CT, to be 100 cm2 for men and 65 cm2 for women. Based on these findings, the corresponding cut‐off value for waist circumference is 86 cm for men and 77 cm for women7. Hara et al. also calculated the optimal cut‐off point of waist circumference among 692 healthy subjects (408 men and 284 women). and the value of 85 cm for men and 78 cm for women yielded the maximal sensitivity plus specificity for predicting the presence of multiple risk factors8. Other studies also reported that the optimal cut‐off point for men ranges from approximately 85 to 90 cm; however, in women it ranges from 77 to 83 cm, approximately 80 cm overall (Table 1)9–15.
Table 1. Reports on optimal cutoff point of waist circumference for the diagnosis of metabolic syndrome in Japan.
| Author (reference number) | No. subjects | Cut‐off point for men (cm) | Cut‐off point for women (cm) |
|---|---|---|---|
| Miyawaki T et al.7 | 3574 | 86 | 77 |
| Hara K et al.8 | 692 | 85 | 78 |
| Miyatake N et al.9 | 3185 | 85 | 80 |
| Nishimura R et al.10 | 2113 | 85 | 81 |
| Eguchi M et al.11 | 420 | 83 | 78 |
| Narisawa S et al.12 | 12,725 | 87 | 83 |
| Oka R et al.13 | 1870 | 89 | 82 |
| Sato A et al.14 | 395 | 87 | 80 |
| Doi Y et al.15 | 2452 | 90 | 80 |
| Present study | 5972 | 84 | 80 |
The cut‐off points of waist circumference for MetS suggested by the NCEP‐ATP III (102 cm for men and 88 cm for women) are accepted in Western countries and there are no studies that consider whether the optimal cut‐off value should be revised. In contrast, several studies that were carried out in Asian countries show that the cut‐off values should be lower than those of the NCEP‐ATP III (Table 2)16–21. Although the cut‐off values are defined by the IDF for Asian populations as 90 cm for men and 80 cm for women, several studies from Korea18,20,21 and China19 suggest that the optimal cut‐off points are different from those of the IDF. Taking these findings together with those of the studies from Japan (Table 1) and Asian countries (Table 2), ethnic differences are likely to exist between populations across Asia, and the criteria for defining MetS in Japan needs to be revised.
Table 2. Reports on optimal cut‐off point of waist circumference for the diagnosis of metabolic syndrome in Asian countries.
The present study has potential limitations. First, the subjects enrolled in our study chose to undergo annual health examinations; they were therefore more health‐conscious than average, which might have caused some bias in the current study. Second, the cross‐sectional study design makes it difficult to infer causality between waist circumference and metabolic risk factors. Finally, it is still controversial whether or not the waist circumference cut‐off values of MetS are significant predictors of cardiovascular events. McNeil et al. assessed the association between MetS, using the NCEP III definition, and CVD with an 11‐year follow‐up period, and they reported that waist circumference is not a significant predictor for CVD22. Therefore, our findings are not fully applicable to clinical and public health practice settings. Further studies are needed to prospectively relate the accumulation of visceral fat to the presence of risk factors of CVD.
In conclusion, although follow‐up studies are required to prove the feasibility of the definition of MetS to predict the development of CVD, the cut‐off value of waist circumference as a criterion for MetS in Japan should be 80 cm for women based on the present results and a review of the literature.
Acknowledgment
This study was supported in part by Grants‐in‐Aid for Young Scientists (B), the Ministry of Education, Culture, Sports, Science and Technology, Japan to Dr Ogawa (21790813). No potential conflicts of interest relevant to this study were reported.
References
- 1.Lakka HM, Laaksonen DE, Lakka TA, et al. The metabolic syndrome and total and cardiovascular disease mortality in middle‐aged men. JAMA 2002; 288: 2709–2716 [DOI] [PubMed] [Google Scholar]
- 2.Eckel RH, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet 2005; 365: 1415–1428 [DOI] [PubMed] [Google Scholar]
- 3.World Health Organization . Definition, Diagnosis and Classification of Diabetes and its Complications: Report of a WHO Consultation. WHO, Geneva, 1999. [Google Scholar]
- 4.Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III) . Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP). JAMA 2001; 285: 2486–2497 [DOI] [PubMed] [Google Scholar]
- 5.Alberti KG, Zimmet P, Shaw J. Metabolic syndrome ‐‐ a new world‐wide definition. A Consensus Statement from the International Diabetes Federation. Diabet Med 2006; 23: 469–480 [DOI] [PubMed] [Google Scholar]
- 6.An examination committee for criterion of metabolic syndrome. Definition and criteria of metabolic syndrome. Nippon Naika Gakkai Zasshi (in Japanese) 2005; 94: 794–809 [PubMed] [Google Scholar]
- 7.Miyawaki T, Hirata M, Moriyama K, et al. Metabolic syndrome in Japanese diagnosed with visceral fat measurement by computed tomography. Proc Jpn Acad 2005; 81 (Ser. B): 471–479 [Google Scholar]
- 8.Hara K, Matsushita Y, Horikoshi M, et al. A proposal for the cutoff point of waist circumference for the diagnosis of metabolic syndrome in the Japanese population. Diabetes Care 2006; 29: 1123–1124 [DOI] [PubMed] [Google Scholar]
- 9.Miyatake N, Wada J, Matsumoto S, Nishikawa H, Makino H, Numata T. Re‐evaluation of waist circumference in metabolic syndrome: a comparison between Japanese men and women. Acta Med Okayama 2007; 61: 167–169 [DOI] [PubMed] [Google Scholar]
- 10.Nishimura R, Nakagami T, Tominaga M, Yoshiike N, Tajima N. Prevalence of metabolic syndrome and optimal waist circumference cut‐off values in Japan. Diabetes Res Clin Pract 2007; 78: 77–84 [DOI] [PubMed] [Google Scholar]
- 11.Eguchi M, Tsuchihashi K, Saitoh S, et al. Visceral obesity in Japanese patients with metabolic syndrome: reappraisal of diagnostic criteria by CT scan. Hypertens Res 2007; 30: 315–323 [DOI] [PubMed] [Google Scholar]
- 12.Narisawa S, Nakamura K, Kato K, Yamada K, Sasaki J, Yamamoto M. Appropriate waist circumference cutoff values for persons with multiple cardiovascular risk factors in Japan: a large cross‐sectional study. J Epidemiol 2008; 18: 37–42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Oka R, Kobayashi J, Yagi K, et al. Reassessment of the cutoff values of waist circumference and visceral fat area for identifying Japanese subjects at risk for the metabolic syndrome. Diabetes Res Clin Pract 2008; 79: 474–481 [DOI] [PubMed] [Google Scholar]
- 14.Sato A, Asayama K, Ohkubo T, et al. Optimal cutoff point of waist circumference and use of home blood pressure as a definition of metabolic syndrome: the Ohasama study. Am J Hypertens 2008; 21: 514–520 [DOI] [PubMed] [Google Scholar]
- 15.Doi Y, Ninomiya T, Hata J, et al. Proposed criteria for metabolic syndrome in Japanese based on prospective evidence: the Hisayama study. Stroke 2009; 40: 1187–1194 [DOI] [PubMed] [Google Scholar]
- 16.Tan CE, Ma S, Wai D, Chew SK, Tai ES. Can we apply the National Cholesterol Education Program Adult Treatment Panel definition of the metabolic syndrome to Asians? Diabetes Care 2004; 27: 1182–1186 [DOI] [PubMed] [Google Scholar]
- 17.Misra A, Wasir JS, Pandey RM. An evaluation of candidate definitions of the metabolic syndrome in adult Asian Indians. Diabetes Care 2005; 28: 398–403 [DOI] [PubMed] [Google Scholar]
- 18.Lee SY, Park HS, Kim DJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract 2007; 75: 72–80 [DOI] [PubMed] [Google Scholar]
- 19.Bao Y, Lu J, Wang C, et al. Optimal waist circumference cutoffs for abdominal obesity in Chinese. Atherosclerosis 2008; 201: 378–384 [DOI] [PubMed] [Google Scholar]
- 20.Kim HK, Kim CH, Park JY, Lee KU. Lower waist‐circumference cutoff point for the assessment of cardiometabolic risk in Koreans. Diabetes Res Clin Pract 2009; 85: 35–39 [DOI] [PubMed] [Google Scholar]
- 21.Baik I. Optimal cutoff points of waist circumference for the criteria of abdominal obesity: comparison with the criteria of the International Diabetes Federation. Circ J 2009; 73: 2068–2075 [DOI] [PubMed] [Google Scholar]
- 22.McNeill AM, Rosamond WD, Girman CJ, et al. The metabolic syndrome and 11‐year risk of incident cardiovascular disease in the atherosclerosis risk in communities study. Diabetes Care 2005; 28: 385–390 [DOI] [PubMed] [Google Scholar]