

Abstract
Introduction:
This study was conducted to analyze the reliability of clinical diagnosis in ACL tear injuries.
Material and methods:
All patients attending our clinic with knee pain from 2009 to 2013 underwent systematic and thorough clinical assessment. From one hundred and three patients with knee problems in 73 were arhroscopicaly diagnosed ACL tears. All these patients underwent therapeutic arthroscopic knee surgery. The clinical diagnosis was confirmed during this procedure. The accuracy, sensitivity and specificity were calculated based on these arthroscopic findings.
Results:
The accuracy of clinical diagnosis in our study was 82.5% for ACL tears. Our study revealed high sensitivity and specificity and almost high accuracy for ACL injuries of knee joint in comparison to arthroscopy. MRI is an appropriate screening tool for therapeutic arthroscopy, making diagnostic arthroscopy unnecessary in most patients.
Conclusion:
Magnetic resonance imaging is accurate and non invasive modality for the assessment of ligamentous injuries. It can be used as a first line investigation in patients with soft tissue trauma to knee.
Keywords: MRI, arthroscopy, ACL, knee
1. INTRODUCTION
The knee joint is a common site of injury, mainly due to trauma, repetitive activities and sports activities (1).
Disruption of the anterior crucial ligament (ACL), a major stabilizer of the knee, leads to loss of stability of the knee and potentially significant dysfunction, although the ACL is the most frequently torn ligament of the knee; the ACL tear has remained clinically elusive. Additionally, ruptures near ligaments’ insertion may be missed and magnetic resonance imaging (MRI) examination reveals an intact ACL. The accuracy, sensitivity and specificity values for knee lesions vary widely in literature (2).
The clinical relevance of MRI, however, is determined in one way by its value in the selection of patients for or exclusion of patients from treatment with therapeutic arthroscopy. This overall assessment of the entire joint, also called composite diagnosis (3), is more relevant than the accurate diagnosis of all specific lesions of the various anatomic structures.
Determination of the clinical relevance of MRI can be affected by selection bias. Selection criteria for arthroscopy, results of which are used as the reference standard, play a role in most studies and potentially have a major influence on the interpretation of MRI results. MRI has a better soft tissue contrast and multi planar slice capability which has revolutionized and has become the ideal modality for imaging complex anatomy of the knee joint (4).
Advanced modality in the management of internal derangement of knee joint is arthroscopy, which can be used in its dual mode, either as diagnostic and/or as therapeutic tool. Arthroscopy offers direct visualization of all interarticular structures with high diagnostic accuracy, the possibility to examine the stability of the knee under anesthesia and the possibility to perform a therapeutic procedure in the same session (5).
In this study ACL tears were clinically diagnosed by positive Anterior Drawer Test and positive Lachman test. Arthroscopy was used to assess the reliability of clinical diagnosis.
2. PATIENTS AND METHODS
In our study we involved 103 patients with history of knee injuries who were admitted in the Clinic of Traumatology, Clinical Center-Majka Tereza, Skopje. MRI of the knee joint was done before the admission and some of them before the clinical examination.
Patients were subjected to physical examination involved assessing Anterior Drawer Test and positive Lachman test. The major difference between these is the degree of knee flexion (90 degrees in the drawer sign and 20-30 degrees in Lachman). All clinically diagnosed patients underwent diagnostic and therapeutic knee arthroscopy to assess the accuracy of clinical diagnosis after required investigations and consent in the Clinic of Traumatology, Clinical Center-Majka Tereza, Skopje during the years 2009 and 2013.
However some patients who had been referred from outside or taken treatment and MRI being done prior to admission in our hospital are considered with same MRI report and not subjected to fresh MRI investigation.
Images of magnetic resonance were performed with 1.0-T system (Phillips Medical Systems) at Institute of Radiology in Skopje.
The standardized MR imaging protocol consisted of sagittal, coronal and axial sequences, in section thickness of 3-5 mm. ACL was considered normal when it appeared as a band of fibers of low to intermediate signal intensity on both sagittal and coronal dual images. The ACL was considered to be partially torn when there was abnormal signal intensity within the ligament or when otherwise intact fibers appeared wavy on sagittal or coronal dual images. The ACL was considered to be completely torn if there was disruption of all fibers or if it was not discernible at all on MRI. For statistical analysis, we considered normal as one group and complete tears and partially torn ligaments as another group.
All arthroscopic procedures were performed in a standard manner by experienced arthroscopic surgeon who was blinded to the radiologist’s diagnosis, using an infero-lateral and medial portal. Operative findings were documented in the official patient’s document, which included the survey of the entire joint and anatomical structure, lesions involved with the presence or absence of tear, its location, status of the articular cartilage and others. The composite data was tabulated and studied for correlation with MRI findings and grouped into four categories:
True-positive -if the MRI diagnosis was confirmed by arthroscopic evaluation.
True-negative -when MRI negative for lesio and confirmed by arthroscopy.
False-positive -when MRI shows lesion b t the arthroscopy was negative
False-negative-result when arthroscopy was positive but the MRI showed negative finding
Statistical analysis
Statistical analysis was used to calculate the sensitivity, specificity, accuracy, positive predictive value (PPV) and the negative predictive value (NPV), in order to assess the reliability of the MRI results.
Categorical variables were summarized using frequency and were compared using the chi-square or McNemar test as appropriate. p-value of less than 0.05 was considered to be statistically significant.
3. Results
The study group of 103 patients consisted of 81 men (79%) and 22 women (21%). All underwent arthroscopic knee surgery. The average age was 29.7 years (range: 16–58 years). Maximum number of patients (n=34) who suffered knee injuries were in the age group of 21-30 years (Figure 1). The right knee was involved in 56 cases (54.4%) and the left knee in 47 (45.6%) (Figure 2).
Figure l.
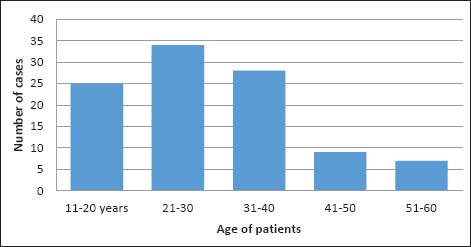
Age distribution of examinees
Figure 2.
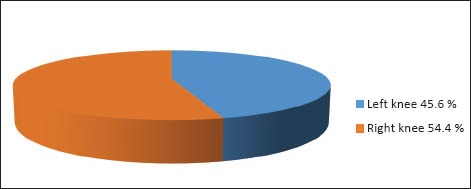
Side involved in examination
Table 1. show the methods and formulas used to calculate the reliability of clinical diagnosis. Clinical diagnostic test characteristics:
Table 1.
Formulas for calculation
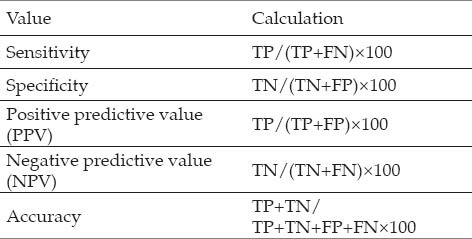
Sensitivity: how good the test is at detecting ACL teae
Specificity: how good the test is at identifying normal knee
Positive predictive value: how often a patient with a positive test has the ACL tear
Negative predictive value: how often a patient with a negative test does not have ACL tear
Accuracy: proportion of test which correetly identifies ACL injuries
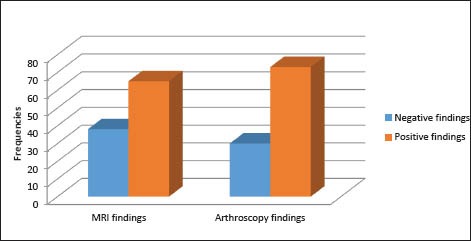
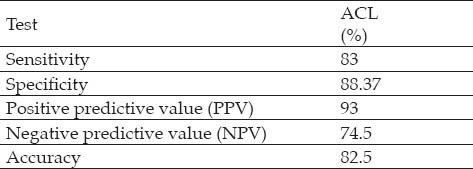
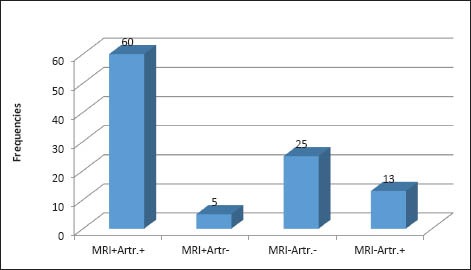
Comparison of the arthroscopic and MRI findings yielded the following results. MRI findings for the ACL yielded 60 true-positives (were confirmed on arthroscopy) and 25 true-negatives (without evidence of ACL) with 5 false positive (were miss interpreted to have ACL) and 13 false negative (were not diagnosed clinically) (Table 2; Figure 3), which resulted in 83% sensitivity, 88.37% specificity, 93% positive predictive value, 74.5% negative predictive value and 82.5% accuracy (Table 3).
Table 2.
MRI and Arthroscopy findings
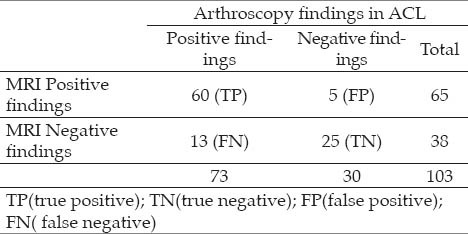
Figure 3.
MRI and Arthroscopy findings in ACL of the knee
Table 3.
ACL findings
McNemar test showed that x2=3.55, DF=1, p>0.05, i.e. There are no statistical differences in distribution of frequencies in positive and negative patients with MRI and arthroscopy or perceived difference is not statistically significant (Figure 4).
Figure 4.
MRI and Arthroscopy finding in ACL of the knee with McNemar
4. DISCUSSION
The purposeof ihis study was to assess the reliaCtltty ot clfnical diagnostc tnACL tearinjurirs. In the study we evaluated 103 patients with history of knee injuries who were admitted at Clinic of Traumatology in Skopje.
The age group ranging from 16 to 58 years. The youngest male patient was aged 16 years and the oldest female was 58 years. This showed that there was a tendency of males being injured and getting operated at the earlier age. A study done by Avcu et al. (6) showed males are most likely to suffer knee injuries since they are active in sports and the right knee was more frequently injured than left.
Rubin et al. (7) reported 93% sensitivity for diagnosing isolated ACL tears. Similarly several prospective studies have shown a sensitivity of 92-100% and specificity of 93-100% for the MR imaging diagnosis of ACL tears (8).
We obtained 83% sensitivity and 88.37% specificity of MRI with respect to fair correlation with arthroscopy in diagnosing ACL tears. Identification of ACL tears in our study was presented with 82.5% accuracy of MRI, ranged in “very good” (80-90%) interpretation group. The results of this study is in accordance to the literature which suggests an accuracy of 80 to 94 % for the crucial ligament tears (9). PPV of MRI is 93% NPV of MRI is 74.5%
Meta-analysis by Oei and colleagues (10) combined 29 studies from 1991 to 2000 that evaluated the validity of MRI with respect to miniscule and crucial ligament disorders of the knee. The pooled sensitivity of medial and lateral menisci was 93% and 79% while pooled specificities were 88% and 95% respectively. For ACL and PCL tear, pooled sensitivities and specificities were 94%, 91% and 94%, 99% respectively.
There is no doubt that the radiologist’s experience and training are very important factors in interpretation of MRI. At the same time, reliable statistical data of the diagnostic value of the MRI are also related to the independent base of reference. Regarding knee MRI, in most of the studies and in our study as well, the base of reference is arthroscopy (11, 12). This presupposes that arthroscopy is 100% accurate allows for the diagnosis of every possible knee pathology. This is not always the case (13). Arthroscopy is a technically demanding procedure and the results are varying according to surgeon’s experience, especially in difficult cases.
MRI is the most helpful diagnostic technique. The reported accuracy for detecting tears of the ACL has ranged from 70-100%. (14). Because the ACL crosses the knee joint at a slightly oblique angle, the complete ligament rarely is captured in its entirety by a single MRI scan in the true sagittal plane.
Arthroscopy should be considered a diagnostic aid used in conjunctions with a good history, complete physical examination and appropriate radiographs. It should serve as an adjuvant to, not as a replacement for, a thorough clinical evaluation. With increased proficiency in examination of extremities and more accurate adjuvant tests, including MRI, we rarely perform simple “diagnostic arthroscopy.” Surgical alternatives are discussed thoroughly with the patient before the procedure, and the definitive surgical procedure is performed at the time of an arthroscopic examination.
5. CONCLUSION
Our study revealed high sensitivity and specificity and almost high accuracy for ACL injuries of knee joint in comparison to arthroscopy. Findings of this small scale study of our population are consistent with larger studies in this field. So we have sufficient evidence to conclude that MRI is highly accurate in the diagnosis of ACL. MRI is an appropriate screening tool for therapeutic arthroscopy, making diagnostic arthroscopy unnecessary in most patients.
Magnetic resonance imaging is accurate and non invasive modality for the assessment of ligamentous injuries. It can be used as a first line investigation in patients with soft tissue trauma to knee.
Footnotes
CONFLICT OF INTEREST: NONE DECLARED.
REFERENCES
- 1.Kaplan PA, Walker CW, Kilcoyne RF, Brown DE, Tusek D, Dussault RG. Occult fractures patterns of the knee associated with ACL tears. Assessment with MR imaging. Radiology. 1992;183:835–838. doi: 10.1148/radiology.183.3.1584943. [DOI] [PubMed] [Google Scholar]
- 2.Crawford R, Walley G, Bridgman S, Maffulli N. Magnetic resonance imaging versus arthroscopy in the diagnosis of knee pathology, concentrating on meniscal lesions and ACL tears: a systematic review. Br Med Bull. 2007;84:5–23. doi: 10.1093/bmb/ldm022. [DOI] [PubMed] [Google Scholar]
- 3.Bui-mansfield LT, Youngberg RA, Warme W, Pitcher JD, Nguyen PLL. Potential cost savings of MR imaging obtained before arthroscopy of the knee: evaluation of 50 consecutive patients. AJR. 1997;168:913–918. doi: 10.2214/ajr.168.4.9124139. [DOI] [PubMed] [Google Scholar]
- 4.Kean DM, Worthington BS, Preston BJ. Nuclear MRI of knee: examples of normal anatomy and pathology. Br J Radiol. 1983;56:355–361. doi: 10.1259/0007-1285-56-666-355. [DOI] [PubMed] [Google Scholar]
- 5.Mink JH, Levy T, Crues JV. Tears of the anterior cruciate ligament and menisci of the knee: MR imaging evaluation. Radiology. 1988;167(3):769–774. doi: 10.1148/radiology.167.3.3363138. [DOI] [PubMed] [Google Scholar]
- 6.S.E.I, et al. Knee joint examination by MRI: the correlation of pathology, age and sex. N Am J Med Sci. 2010;2(4):202–204. doi: 10.4297/najms.2010.2202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Rubin DA, Kettering JM, Towers JD, Britton CA. MR imaging of the knee having isolated and combined ligament injuries. AJR. 1998;170:1207–1213. doi: 10.2214/ajr.170.5.9574586. [DOI] [PubMed] [Google Scholar]
- 8.Lee K, Seigel MJ, Lau DM, Hildebolt CF, Matava MJ. ACL tears-MR imaging based diagnosis in pediatric population. Radiology. 1999;213(3):697–704. doi: 10.1148/radiology.213.3.r99dc26697. [DOI] [PubMed] [Google Scholar]
- 9.Tung GA, Davis LM, Wiggins ME, Fadale PD. Tears of the anterior cruciate ligament: Primary and secondary signs at MR imaging. Radiology. 1993;188:661–667. doi: 10.1148/radiology.188.3.8351329. [DOI] [PubMed] [Google Scholar]
- 10.Oei EH, Nikken JJ, Verstijnen AC, Ginai AZ, Myriam Hunink MG. MR Imaging of the Menisci and Cruciate Ligaments: A Systematic Review. Radiology. 2003;226:837–848. doi: 10.1148/radiol.2263011892. [DOI] [PubMed] [Google Scholar]
- 11.Esmaili Jah AA, Keyhani S, Zarei R, Moghaddam AK. Accuracy of MRI in comparison with clinical and arthroscopic findings in ligamentous and meniscal injuries of the knee. Acta Orthop Belg. 2005;71(2):189–196. [PubMed] [Google Scholar]
- 12.Navali AM, Bazavar M, Mohseni MA, Safari B, Tabrizi A. Arthroscopic evaluation of the accuracy of clinical examination versus MRI in diagnosing meniscus tears and cruciate ligament ruptures. Arch Iran Med. 2013;16(4):229–232. [PubMed] [Google Scholar]
- 13.Khanda G, Akhtar W, Ahsan H, Ahmad N. Assessment of menisci and ligamentous injuries of the knee on magnetic resonance imaging: correlation with arthroscopy. J Pak Medical Association. 2008;58(10):537–540. [PubMed] [Google Scholar]
- 14.Leiden: University of Leiden; 2010. Knee joint examinations by magnetic resonance imaging: The correlation of pathology, age, and sex. In: Patrice Vincken. MRI of the Knee Cost-Effective Use. [dissertation] [DOI] [PMC free article] [PubMed] [Google Scholar]