

Abstract
Objective
The purpose of this paper is to assess whether smokers adjust their beliefs in a pattern that is consistent with Cognitive Dissonance Theory. This is accomplished by examining the longitudinal pattern of belief change among smokers as their smoking behaviours change.
Methods
A telephone survey was conducted of nationally representative samples of adult smokers from Canada, the USA, the UK and Australia from the International Tobacco Control Four Country Survey. Smokers were followed across three waves (October 2002 to December 2004), during which they were asked to report on their smoking-related beliefs and their quitting behaviour.
Findings
Smokers with no history of quitting across the three waves exhibited the highest levels of rationalisations for smoking. When smokers quit smoking, they reported having fewer rationalisations for smoking compared with when they had previously been smoking. However, among those who attempted to quit but then relapsed, there was once again a renewed tendency to rationalise their smoking. This rebound in the use of rationalisations was higher for functional beliefs than for risk-minimising beliefs, as predicted by social psychological theory.
Conclusions
Smokers are motivated to rationalise their behaviour through the endorsement of more positive beliefs about smoking, and these beliefs change systematically with changes in smoking status. More work is needed to determine if this cognitive dissonance-reducing function has an inhibiting effect on any subsequent intentions to quit.
Most smokers will agree that smoking poses a serious health risk,1 yet many continue to smoke. How do smokers deal with the knowledge that they are doing something they know may kill them? Leon Festinger’s classic Cognitive Dissonance Theory provides a framework for understanding the discrepancy between the knowledge that smoking is harmful and the behaviour of continuing to smoke. According to Cognitive Dissonance Theory, when people engage in behaviour that is inconsistent with their beliefs, they experience an unpleasant psychological tension, known as dissonance, which they are motivated to reduce.2 Festinger suggested that dissonance reduction will follow the path of least resistance. He explained that when a change in behaviour is difficult to achieve, such as quitting smoking, a change in attitudes occurs instead. Given the difficulty of quitting smoking,3 the theory would predict that smokers are more likely to adjust their beliefs to justify their behaviour than they are to change their smoking behaviour.4
Indeed, there is social psychological research that is consistent with the view that smokers engage in belief generation that helps to justify their smoking. For instance, smokers commonly endorse beliefs that help to enhance the functional features of the dissonant behaviour (eg, rationalising that smoking reduces stress and increases concentration)5–7 or minimise the negative features of the undesirable consequences (eg, underestimating the health risks of smoking).8–17 However, these studies only demonstrate that smokers, compared with non-smokers, endorse more pro-smoking beliefs or perceive fewer risks associated with smoking. Given that smoking has long been the poster child of Cognitive Dissonance Theory2 it is surprising how little research there is that specifically examines the mean levels of belief change among smokers. In one of the earliest papers on dissonance reduction among smokers in 1968, the authors understood the importance of looking at the pattern of belief change among smokers as their behaviour changed across time.18 However, due to the difficulty in recruiting and retaining a large enough sample of smokers whose behaviour changed over time, the authors resorted to cross-sectional comparisons of the beliefs of smokers, non-smokers and ex-smokers at the baseline wave. Since then, no other study that we know of has successfully been able to report on the longitudinal pattern of smokers’ beliefs as they change their behaviour. Most studies have been correlational in nature and have relied mainly on cross-sectional data.9,18–22 These studies thus cannot provide compelling evidence that smokers’ endorsement of such beliefs is a function of the dissonance-reducing motivations theorised by Festinger. A more faithful rendering of Cognitive Dissonance Theory demands that the mean levels of beliefs be examined across time among the same individuals, with each smoker acting as his or her own control.
One reason why smokers may be motivated to reduce their dissonance is because the resulting cognitive consistency has the psychological benefit of promoting mental health and maintaining a positive self-view.23,24 However, an unintended consequence of endorsing more pro-smoking beliefs is that smokers may also unknowingly be reducing their psychological need to change their behaviour.10 Indeed, multiple cross-sectional studies have found that higher endorsements of pro-smoking beliefs are associated with lower quit intentions among smokers.9,10,25 More recently, two longitudinal studies revealed that rationalisations that act to either highlight the functional beliefs of smoking or minimise the risks associated with smoking are also negatively related to subsequent quit attempts.8,26 Festinger alluded to the possibility that dissonance may be a powerful motivator to quit smoking, but as these results seem to suggest, smokers may be able to circumvent their dissonance by changing their attitudes.
Yet, despite commonly using a dissonance framework to explain their findings, few studies provide convincing evidence that smokers’ belief endorsements are driven by dissonance-reducing motivations. To do so would require either an experimental study27 or an examination of the longitudinal pattern of belief change as a function of behaviour. As Oakes and colleagues discuss,10 it is important to establish whether the beliefs that smokers endorse are merely convenient defenses that are discarded when the cognitive dissonance is resolved by quitting or whether those beliefs are more enduring and accurate representations of the smoker’s perceptions about smoking. If smokers do adjust their beliefs at the service of dissonance-reducing motivations, we would expect to observe a change in beliefs among the same individuals across time as their behaviour changes. Importantly, a change in beliefs would occur only after a change in behaviour has occurred. If, however, beliefs represent more stable individual differences, we would not expect beliefs to shift as an individual changes his or her behaviour.
In a recent longitudinal study of smokers, Borland et al8 noticed that the pattern of risk-minimising beliefs was relatively stable across time and thus concluded that the ‘stable beliefs’ hypothesis was supported over the ‘convenient-defense’ hypothesis. However, their analysis was aggregated across individuals (mostly continuing smokers) whose behaviour may or may not have changed during the course of the study. They did not specifically examine the pattern of beliefs among individuals whose behaviour changed over the course of the study (eg, those who quit smoking). Using essentially the same data set as Borland et al8 and Yong and Borland26, we extend their results by examining how functional-enhancing and risk-minimising beliefs wax and wane over time among three groups of individuals: smokers who continue smoking, smokers who quit and smokers who quit and relapse. In addition, whereas both papers by Yong and Borland26 and Borland et al8 examined the relation of beliefs at one wave to predict cessation in the next wave, we examine the rise and fall of pro-smoking beliefs among the same cohort of individuals across three waves. It is essential to examine the pattern of beliefs separately for each of these groups across multiple waves in order to find any evidence for, or against, Cognitive Dissonance Theory.
Presuming that smokers do change their beliefs in a pattern that is consistent with Cognitive Dissonance Theory, it is also important to understand the magnitude of change in a way that is meaningful. That is, do smokers make subtle or drastic adjustments to their beliefs as their behaviour changes? According to Dissonance Theory, a larger magnitude of belief change is an indication of greater dissonance. In addition, comparing the magnitude of belief change across a variety of commonly used rationalisations may shed light on which beliefs are most likely to be used by smokers in the service of dissonance reduction. To date, no study has attempted to capture the scale of change in beliefs that is associated with a change in behaviour.
OBJECTIVES
The purpose of this paper is to assess whether smokers adjust their beliefs in a pattern that is consistent with Cognitive Dissonance Theory. In addition, our analyses will determine the magnitude of belief change among smokers as their behaviour shifts. Finally, we will attempt to explore the direction of the relation between beliefs and behaviour. Does a change in beliefs follow a change in behaviour, or vice versa? To answer these questions, we examine the longitudinal patterns of belief change among smokers who quit, with specific comparisons of those who maintained their quit status (successful quitters) versus those who relapsed (failed quitters). A longitudinal examination of how smokers’ beliefs change as their behaviour changes would provide strong evidence for the long-held view that smokers endorse more positive beliefs of smoking in an attempt to minimise their cognitive dissonance. From a dissonance perspective, we would expect that successful quitters would endorse pro-smoking beliefs less once they are no longer smoking.10 In addition, we would expect a rebound effect among failed quitters, with these individuals again endorsing more pro-smoking beliefs once they relapse to smoking (even if they had previously endorsed more negative beliefs during the time they had quit).
Furthermore, although Festinger2 suggested that dissonance reduction will follow the path of least resistance, few studies have tested this hypothesis beyond the conjecture that beliefs are changed ahead of behaviours. In this paper, we test this hypothesis by comparing the magnitude of belief change among various forms of rationalisations commonly used for smoking. If dissonance reduction does follow the path of least resistance, we would expect to see some rationalisations being endorsed more than others. As Kunda28 suggested, there are reality constraints on the beliefs that we are able to hold. In the case of smoking, not all rationalisations are equally likely to be used in reducing dissonance. Because of the multitude of anti-smoking messages about the harms of smoking, risk-minimising beliefs such as ‘the medical evidence that smoking is harmful is exaggerated’ should not be used as freely as a way to justify one’s smoking; the reality of the harms would constrain the use of such rationalisations. In contrast, functional beliefs such as ‘smoking helps me concentrate better’ and ‘smoking is an important part of my life’ are less subject to empirical scrutiny and counterargument. Therefore, relative to risk-minimising beliefs (which are constrained by the reality of the harmfulness of smoking), functional beliefs are expected to be more strongly endorsed by continuing smokers, drop off to a greater extent during a quit episode and rebound to a greater degree among quitters who relapse.
METHODS
The International Tobacco Control Policy Four Country Survey (ITC-4) is a longitudinal study conducted annually among a cohort of adult smokers from Canada, the USA, the UK and Australia (see Fong et al29 and Thompson et al30 for a detailed explanation of the conceptual model and methods of the ITC Project). The present analysis was conducted on the first three waves of the ITC-4: wave 1 (W1) was conducted in October to December 2002, wave 2 (W2) was conducted in May to September 2003 and wave 3 (W3) was conducted in August to December 2004. In addition, a replication of the analyses was conducted using data from a parallel set of waves (wave 2 to wave 4), with wave 4 (W4) conducted from October 2005 to January 2006.
Procedure
The ITC-4 cohort was constructed from probability sampling methods, with telephone numbers selected at random from the population of each country within strata defined by geographic region and community size. Eligible households were identified by asking a household informant the number of adult smokers. The Next Birthday Method was used to randomly select the respondent in households with multiple smokers.31 The surveys were conducted using computer-assisted telephone interviewing software. A full description of the ITC-4 methodology, sample profile and survey rates, including comparisons with national benchmarks, is available online (http://www.itcproject.org).
Sample
Eligible respondents (n=3005) were smokers at W1 (n=10 148) who met the below inclusion criteria at W2 (n=6682) and W3 (n=3005). The replication sample consisted of those smokers at W2 (n=8115) who had valid data at W3 (n=5408) and W4 (n=2493). Recent quitters (<1 month) at W2 (n=185) were excluded, as were smokers at W2 who were quit at W3 (n=600). This allowed us to define three groups: (1) continuing smokers who were daily smokers at W1 and who continued to smoke through W2 and W3, without any intermediate failed attempts between waves; (2) successful quitters who were daily smokers at W1, had quit for at least 30 days at W2 and who had remained quit at W3 and (3) failed quitters who were daily smokers at W1, had quit for at least 30 days at W2 but had relapsed back to smoking at W3 (see table 1).
Table 1.
Distribution of cohort by quitting status at each of three waves
| Quitting status | W1 | W2 | W3 | W1 to W3 sample, n (%) | W2 to W4 sample, n (%) |
|---|---|---|---|---|---|
| Continuing smokers | Smoking | Smoking and no quit attempt since previous wave | Smoking and no quit attempt since previous wave | 2730 (90.8) | 2186 (87.7) |
| Successful quitters | Smoking | Quit at time of survey for at least 30 days | Remained quit from time of previous wave | 170 (5.7) | 221 (8.9) |
| Failed quitters | Smoking | Quit at time of survey for at least 30 days | Relapsed back to smoking at time of survey | 105 (3.5) | 86 (3.4) |
| Total | 3005 | 2493 |
Measures
The ITC-4 Survey was standardised across the four countries: respondents in each country were asked the same questions, with only minor variations for colloquial speech. Table 2 presents demographic information and sample characteristics for each of the three groups.
Table 2.
Characteristics of International Tobacco Four Country Survey sample by country (n=4048)
| Canada | USA | UK | Australia | |
|---|---|---|---|---|
| Sex | ||||
| Female | 55.1% | 58.3% | 56.6% | 53.2% |
| Male | 44.9% | 41.7% | 43.4% | 46.8% |
| Age, years | ||||
| 18–24 | 12.6% | 11.9% | 6.3% | 14.5% |
| 25–39 | 31.8% | 38.8% | 29.6% | 35.7% |
| 40–54 | 35.8% | 36.7% | 35.7% | 35.5% |
| 55+ | 19.9% | 24.5% | 28.3% | 14.3% |
| Education | ||||
| High school diploma or lower | 45.0% | 41.2% | 64.5% | 66.6% |
| Technical, trade school, community college or some university | 41.4% | 44.9% | 23.0% | 20.5% |
| University degree or higher | 13.6% | 13.8% | 12.5% | 12.9% |
| Income | ||||
| Under $30 000/under £15 000 (UK) | 31.1% | 38.1% | 32.8% | 29.5% |
| $30 000–$59 999/£15 001–£30 000 | 38.1% | 37.8% | 36.8% | 35.7% |
| $60 000 and over/£30 001 and over | 30.8% | 24.1% | 30.5% | 34.8% |
| Ethnicity | ||||
| White/English only | 88.7% | 79.4% | 95.1% | 87.2% |
| Other/mixed | 11.3% | 20.6% | 4.9% | 12.8% |
| Mean cigarettes per day (SD) | 16.0 (9.65) | 17.7 (11.5) | 16.6 (9.7) | 18.0 (12.4) |
| Mean time to first cigarette (min) (SD) | 72.2 (140.8) | 71.9 (142.2) | 73.6 (141.8) | 83.7 (154.7) |
Measures of quitting and definitions of quitting outcome.
Standard measures of smoking behaviour and quit history were included in the ITC-4. Quitting behaviour was assessed by asking smokers: “Have you made any attempts to stop smoking since we last talked with you?” to which participants answered yes/no. Quit attempt was defined as any quit attempt made between waves that lasted for at least 30 days. To assess quitting success, those who reported an attempt were also asked whether they were now back smoking or still quit.
Measures of rationalisations
Measures for smoking beliefs were designed to capture a range of positive functional beliefs and risk-minimising beliefs, which we will generally refer to as rationalisations. These items have been used in several waves of the ITC Surveys and in other studies as measures of dissonance-reducing beliefs.9,10 Table 3 lists the nine items that were used to measure the functional and risk-minimising beliefs among smokers. Response options for these questions ranged from ‘1, strongly disagree’ to ‘5, strongly agree’. Factor analysis with oblique rotation revealed the presence of two components that mapped very well onto the theorised forms of rationalisations: functional beliefs and risk-minimising beliefs, corresponding to the two earlier papers that used some of these data.8,26 Table 3 reports the item–total correlations and Cronbach αs for each item in the functional beliefs and risk-minimising beliefs components at each of the three waves. One of the functional belief items (“Smoking makes it easier for you to socialize”) demonstrated relatively low item–total correlations, so it was dropped from all subsequent analyses. The functional beliefs and risk-minimising beliefs scales were significantly, although weakly, correlated with each other at W1 (r=0.29, p<0.001), W2 (r=0.31, p<0.001) and W3 (r=0.34, p<0.001).
Table 3.
Measures of rationalisations and item reliability
| Item–total correlations
|
|||||
|---|---|---|---|---|---|
| W1 | W2 | W3 | |||
| Functional beliefs | 1 | You enjoy smoking too much to give it up | 0.32 | 0.34 | 0.38 |
| 2 | Smoking calms you down when you are stressed or upset | 0.31 | 0.33 | 0.36 | |
| 3 | Smoking helps you concentrate better | 0.44 | 0.44 | 0.43 | |
| 4 | Smoking is an important part of your life | 0.38 | 0.44 | 0.45 | |
| 5 | Smoking makes it easier for you to socialize | 0.24 | 0.26 | 0.21 | |
| Functional beliefs: Cronbach’s α− | 0.58 | 0.61 | 0.61 | ||
| Risk-minimising beliefs | 6 | You have the kind of genetic makeup that allows you to smoke without it giving you health problems | 0.42 | 0.42 | 0.45 |
| 7 | The medical evidence that smoking is harmful is exaggerated | 0.46 | 0.50 | 0.51 | |
| 8 | You’ve got to die of something, so why not enjoy yourself and smoke | 0.52 | 0.56 | 0.55 | |
| 9 | Smoking is no more risky than lots of other things that people do | 0.47 | 0.53 | 0.50 | |
| Risk-minimising beliefs: Cronbach α | 0.68 | 0.72 | 0.71 | ||
The new reliability coefficients for the functional beliefs scale (with item 5 removed) are 0.59, 0.62 and 0.62 for W1, W2 and W3, respectively.
Analysis
SPSS (V.17.0) was used for all statistical analyses. Because there were no significant interactions by country, analyses include data collapsed across the four countries. The rise and fall in beliefs between subsequent waves for each of the smoking status groups were assessed by conducting paired samples t-tests. To examine the pattern of rationalisations, we conducted a 3 (group: continuing smokers, successful quitters and failed quitters) ×3 (time: W1, W2 and W3) mixed factorial analysis of variance on our measures of rationalisations, and the relevant simple effects were examined. Effect sizes for mean differences across waves were computed by calculating Cohen’s D (d).32,33 In addition, to examine whether the pattern of dissonance-reducing rationalisations was the same for both functional beliefs and risk-minimising beliefs, we conducted a 3 (group: continuing smokers, successful quitters and failed quitters) ×3 (time: W1, W2 and W3) ×2 (rationalisation type: functional beliefs vs risk-minimising beliefs) mixed analysis of variance.
RESULTS
Rationalisations and smoking behaviour—evidence for dissonance reduction
In accordance with Cognitive Dissonance Theory, which predicts that smokers will adjust their beliefs to better match their current behaviour, we found that each of the ration-alisation components followed the predicted pattern of dissonance reduction. Figures 1 and 2 show the longitudinal patterns of justifications for each of the functional beliefs and the risk-minimising beliefs components, respectively, across the three groups.
Figure 1.
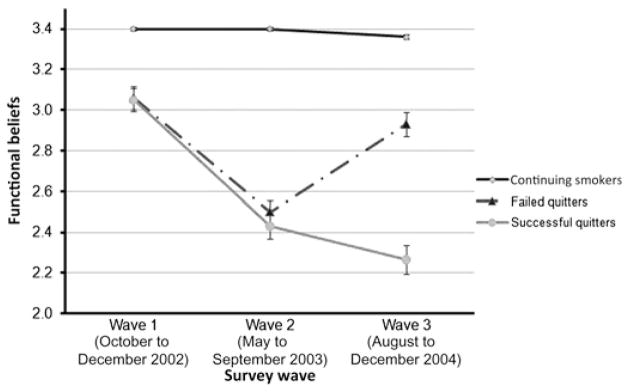
Longitudinal pattern for functional beliefs among continuing smokers, successful quitters and failed quitters.
Figure 2.
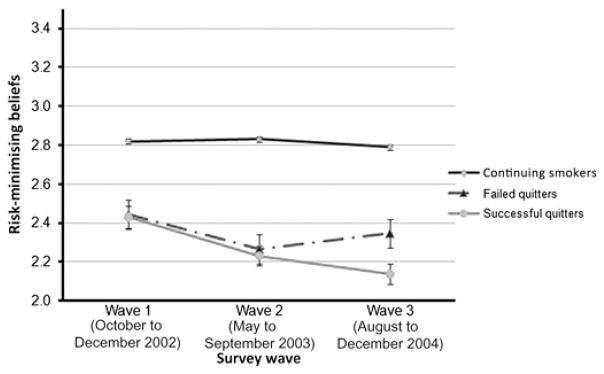
Longitudinal pattern for risk-minimising beliefs among continuing smokers, successful quitters and failed quitters.
Patterns of rationalisations
Functional beliefs
Our analyses revealed that continuing smokers endorsed higher levels of functional beliefs at all three waves (all ps<0.001) relative to successful quitters and failed quitters (see table 4 for means). In addition, there was no significant change in continuing smokers’ endorsements of functional beliefs from W1 to W2 (Mdiff=0.00, t <1) and only a small change from W2 to W3 (Mdiff=−0.04, t(2727)=4.03, p<0.001, d=0.07), which reached significance due to the large sample size of this group.32 By contrast, successful quitters and failed quitters did not differ in their endorsement of functional beliefs at W1 (F<1). At W2, when both groups had quit smoking, successful quitters and failed quitters demonstrated a large reduction in their endorsements of functional beliefs compared with levels previously held at W1 (Mdiff=−0.62, t(168)=9.66, p<0.001, d=0.75 and Mdiff=−0.56, t(104)=8.60, p<0.001, d=0.84, respectively). Again at W2, these two groups did not differ in their functional beliefs (F<1). At W3, however, whereas successful quitters demonstrated a continued, but small, reduction in those beliefs (Mdiff=−0.17, t(168)=2.99, p<0.01, d=0.23), failed quitters’ scores showed a large increase in functional beliefs from W2 (Mdiff=0.43, t(104)= −6.39, p<0.001, d=0.63), which reached levels that were similar to W1 (Mdiff=−0.13, t(104)=2.01, p=0.05, d=0.19)—their level prior to having made a serious quit attempt. See figure 1 for the longitudinal pattern of functional beliefs.
Table 4.
Means and SDs for functional and risk-minimising beliefs at each wave by smoking status
| Quitting status | W1 | W2 | W3 |
|---|---|---|---|
| Functional beliefs, mean (SD) | |||
| Continuing smokers | 3.40 (0.01)a | 3.40 (0.01)a | 3.36 (0.01)b |
| Successful quitters | 3.05 (0.06)c | 2.43 (0.06)d | 2.27 (0.07)e |
| Failed quitters | 3.06 (0.06)c | 2.50 (0.05)d | 2.93 (0.06)c |
| Risk-minimising beliefs, mean (SD) | |||
| Continuing smokers | 2.82 (0.01)f | 2.83 (0.01)f | 2.79 (0.01)g |
| Successful quitters | 2.43 (0.06)h | 2.23 (0.05)i | 2.13 (0.05)j |
| Failed quitters | 2.44 (0.07)h | 2.26 (0.07)i | 2.35 (0.07)hi |
Higher means indicate a greater endorsement of functional or risk-minimising beliefs (5-point scales). For each type of belief, elements with a common single subscript letter represent non-significantly different means, p<0.05, as determined by relevant simple effects tests.
All other elements within each belief type are significantly different from each other.
Risk-minimising beliefs
Similar to the results obtained for functional beliefs, our analyses revealed that continuing smokers demonstrated higher levels of risk-minimising beliefs at all three waves (all ps<0.001) relative to successful and failed quitters (see table 4 for means). There was no significant change in continuing smokers’ endorsements of risk-minimising beliefs from W1 to W2 (Mdiff=0.01, t<1) and only a small change from W2 to W3 (Mdiff=−0.04, t(2726)=7.20, p<0.001, d=0.01), which again was due to the large sample size of this group. In contrast, although successful quitters and failed quitters did not differ in their endorsement of risk-minimising beliefs at W1 (F<1) or at W2 (F<1), both groups demonstrated a small reduction in their risk-minimising beliefs from W1 to W2 (Mdiff=−0.20, t(168)= 3.55, p<0.001, d=0.28 and Mdiff=−0.18, t(103)=2.53, p<0.01, d=0.25, respectively). At W3, successful quitters demonstrated a marginally significant reduction in those beliefs (Mdiff=−0.09, t(168)=1.85, p=0.06, d=0.14), whereas failed quitters tended to increase risk-minimising beliefs back to levels not significantly different from W1 levels (Mdiff=0.08, t(104)=1.66, p=0.10, d=0.12). However, this increase from W2 to W3 for failed quitters did not reach significance (t(103)=1.23, p=0.22). See figure 2 for the longitudinal pattern of risk-minimising beliefs.
Differences between types of rationalisations
We also found a significant three-way interaction between time, group and type of rationalisation F(4, 8072)=12.94, p<0.001). Functional beliefs changed more in the successful quitter and failed quitter groups than did risk-minimising beliefs. After confirming that the relevant two-way interaction between group and type of rationalisation was significant F(2, 4036)= 3.35, p<0.05), the simple effects revealed that all three groups endorsed risk-minimising beliefs significantly less than functional beliefs at each of the three waves, all Fs>6.81, ps<0.01. In addition, successful and failed quitters reduced their risk-minimising beliefs less than their functional beliefs from W1 to W2 (Fs>9.53, ps<0.01). Between W2 and W3, failed quitters showed a smaller increase in their risk-minimising beliefs than they did their functional beliefs F(1, 8072)=11.05, p<0.001). However, successful quitters failed to show a significant difference in how much they decreased endorsements of functional and risk-minimising beliefs (F<1) between W2 and W3.
Direction of effects
Among individuals whose behaviour changes across the three waves of this study (ie, failed and successful quitters), we conducted a binary logistic regression to test the direction of the relation between beliefs and behaviour—that is whether a change in behaviour leads to a change in beliefs or whether a change in beliefs leads to a change in behaviour. If attitudes precede behaviour, then we would expect that our measures of beliefs would be predictive of subsequent behaviour. However, neither functional beliefs (OR=0.84, 95% CI (0.58 to 1.21), p=0.34) nor risk-minimising beliefs (OR=0.93, 95% CI (0.66 to 1 32), p=0.69) at W2 were predictive of whether an individual would remain quit or regress back to smoking at W3. Thus, because we were not able to predict behaviour at W3 with beliefs at W2, behaviour change is likely to result in attitude change rather than vice versa.
Replication of findings
In order to validate our findings, we conducted the same series of analyses for both functional and risk-minimising beliefs using data from W2 to W4 of the ITC-4. Among our three groups, this rise and fall of rationalisation endorsements were replicated for the functional beliefs component and replicated almost entirely for the risk-minimising component, with only three differences emerging.
First, successful quitters failed to show a continued decrease in risk-minimising beliefs from W3 to W4 (F<1). Second, and consistent with our hypothesis, the rebound in risk-minimising beliefs among failed quitters from W3 (M=2.34) to W4 (M=2.56) was highly significant (F (1,85)=9.82, p<0.01), unlike the trend in the previous data set. Importantly, these levels were not different from W2 levels (M=2.50), t<1, demonstrating that, once they were smoking again at W4, failed quitters were endorsing those risk-minimising beliefs just as strongly as they had before they had made a quit attempt at W2.
Third, compared with functional beliefs, we found that risk-minimising beliefs were endorsed less across all three waves (all Fs>6.66, ps<0.01) for each of the three groups, except among successful quitters at W3, which failed to reach significance (F=1.83, p=0.17).
DISCUSSION
Our findings provide a pattern of belief change that is consistent with the existence of dissonance-reducing motivations among smokers: rationalisations are highest among smokers when they are smoking and lowest when they have quit, but importantly these rationalisations return to original levels, or close to original levels, when a quit attempt fails. Importantly, changes in beliefs seem to follow changes in behaviour. This pattern suggests that rationalisations are indeed invoked in the service of the motivation to reduce dissonance and that smokers are able to reduce their dissonance by modifying their beliefs in ways that help to rationalise their continued smoking.
In addition, the finding that different types of rationalisations are used by smokers highlights the view that different modes of dissonance reduction can serve as functional alternatives. Our results revealed that the magnitude of belief change that accompanies a change in smoking behaviour can be quite large. However, as we predicted, the magnitude of belief change is greater for functional beliefs than for risk-minimising beliefs. The larger changes in functional beliefs suggest that smokers may be less likely to encounter resistance when attempting to enhance the functional beliefs about smoking as a means of dissonance reduction because these beliefs are not as easy to challenge. It is difficult to counterargue if a smoker says that smoking increases concentration or is too enjoyable to give up. The greater degree of shifting in the functional beliefs—those beliefs that are less constrained by factual counterarguments—is consistent with Festinger’s conjecture that dissonance reduction will follow the path of least resistance. These findings are also consistent with our hypothesis that public education has reduced smokers’ capacity to shift risk-minimising beliefs to be more supportive of smoking. We might expect smokers to experience less dissonance and hence have less need for ration-alisations in countries where the knowledge of smoking harms is lower, such as in China.34 Therefore, it may be useful to target these beliefs more in public education programmes to further constrain smokers’ potential avenues of dissonance reduction through rationalisations.
We also note that we found no country interactions between the patterns of rationalisations in any of our analyses. This cross-country consistency is intriguing, signifying the possibility of a near-universal phenomenon among smokers. We are beginning to look for similarities beyond the four culturally similar countries in this study to determine the extent to which the phenomenon is culturally universal.35 Recent evidence from Thailand and Malaysia suggests that rationalisations are indeed important in the linkage to quit intentions in these countries.25 However, further work is needed to investigate potential cultural differences in dissonance-reducing motivations.
Implications
The powerful motivation to rationalise one’s behaviour has long been understood by the tobacco industry. Internal documents show that the tobacco industry and its front groups have heavily invested in public relations’ efforts precisely to provide smokers with a psychological crutch and self-rationale to continue to smoke.36,37 When given the choice to change their beliefs or change their behaviour as a means of reducing their dissonance, smokers are more likely to change their beliefs (through the endorsement of rationalisations) because it is easier than quitting.9
Interventions designed to promote and motivate quitting may therefore be more effective if there are explicit attempts to counteract these rationalisations. We suggest that if this route of dissonance reduction is cut-off, then the only other remaining way for smokers to reduce their dissonance is to change their behaviour. This view has been supported by several studies that have demonstrated a change in health behaviour when cognitive dissonance is aroused.38–42 However, although these dissonance-inspired interventions have successfully been applied to influence the performance of positive behaviours related to health, the environment and interpersonal relations, this research has yet to be applied to smoking behaviour. Thus, interventions that can specifically head off and counter some of the most common rationalisations may be of potential value in (1) making smokers aware of their use of rationalisations and (2) cutting out the routes of escape commonly used by smokers, which might indeed increase the motivation to actually quit.
Although the findings from our study provide preliminary support for the proposed interventions, we suggest that cessation campaigns might also benefit from targeting such rationalisations compared with simply trying to provide people with information about the health effects of smoking alone. In particular, our findings suggest that such interventions may benefit from focusing on smokers’ use of functional beliefs over the commonly targeted risk-related beliefs. Therapy and interventions could affect real change in the quit process by identifying those commonly held rationalisations and directly targeting them as barriers to successful quitting. Doing so might also be an effective strategy to inoculate people against relapse. Although many of the commonly used preventive strategies designed to ‘inoculate’ youth and young adults from drug and substance use already have some component of attitude change (such as the correction of inflated or erroneous beliefs),38 very few directly attempt to inform people of the effects that their own biased beliefs have on their behaviour.
Limitations
The main limitation of this study was that we could only consider a small sample of all possible rationalisations that smokers commonly employ, which explains the moderate reliability estimates we found for our two scales of functional and risk-minimising beliefs. A poor-fitting item was removed from the functional beliefs scale; however, the scale reliability estimates still remained slightly below the conventional acceptable level of 0.70 for this scale. Furthermore, the inter-survey interval was 12 months, and those who quit had been quit for different lengths of time. We therefore do not know how rapidly these beliefs change. Removing those quit for <1 month was done to ensure that the effect size was maximised. However, once we obtain enough cases of recent quitters, it will be of interest to study how rapidly dissonant beliefs change with changing smoking status.
Second, because we did not employ a controlled experimental design with random assignment to smoking status, we cannot conclusively rule out the possibility that a third spurious variable is causing the observed changes in attitudes over time. In addition, a longitudinal design does not enable us to make definitive conclusions regarding the direction of the causality between attitudes and behaviour that an experimental design would permit. Nonetheless, we were able to use the longitudinal design of this study to illustrate that the change in attitudes are likely the result of a change in behaviour, rather than the reverse. This study is therefore one of the strongest tests of cognitive dissonance among smokers to date.
Taken together, the present findings suggest that smokers’ beliefs can change in the service of dissonance-reducing motivations. Furthermore, dissonance reduction seems to follow the path of least resistance, with the most malleable beliefs being changed to a greater extent. Finally, because the pattern of rationalisations was consistent across each of the four countries sampled, dissonance-reducing motivations might be a fundamental drive among smokers within Western countries.
What this paper adds.
Smokers have long been used as the primary example to illustrate people’s motivation to maintain cognitive consistency through the endorsement of beliefs that are in agreement with their behaviour. However, few studies have explicitly looked at whether smokers’ beliefs change across time as their behaviour changes. Consistent with Cognitive Dissonance Theory, the findings from the current longitudinal analysis demonstrate that smokers rationalise their smoking by changing their beliefs to better match their behaviour.
Acknowledgments
We would also like to acknowledge the other members of the ITC team, Mary E Thompson for her help with data analysis and Karina Schumann for her technical assistance and support. We would also like to express our appreciation for support from the Prevention Scientist Award from the Canadian Cancer Society Research Institute, granted to GTF.
Funding This research was funded by grants from the National Cancer Institute of the USA (R01 CA 100362), the Roswell Park Transdisciplinary Tobacco Use Research Center (P50 CA111236), Robert Wood Johnson Foundation (045734), Canadian Institutes of Health Research (57897 and 79551), National Health and Medical Research Council of Australia (265903 and 450110), Cancer Research UK (C312/A3726) and Canadian Tobacco Control Research Initiative (014578), with additional support from the Centre for Behavioural Research and Program Evaluation, National Cancer Institute of Canada/Canadian Cancer Society (now the Propel Centre for Population Health Impact at the University of Waterloo) and the Ontario Institute for Cancer Research. Additional funding to the first author was provided through a CIHR Frederick Banting and Charles Best Canada Graduate Scholarship.
Footnotes
Competing interests All authors are employed by academic institutions or cancer control charities and have no competing financial interests.
Patient consent Obtained.
Ethics approval The study protocol was cleared for ethics by the institutional review boards or research ethics boards in each of the countries: the University of Waterloo (Canada), Roswell Park Cancer Institute (USA), University of Illinois–Chicago (USA), University of Strathclyde (UK) and The Cancer Council Victoria (Australia).
Contributors OF proposed and performed the data analyses, the literature review, wrote most of the initial draft and coordinated input from other authors. GTF and MPZ helped with the design and analyses. They also provided input and edited the initial draft and subsequent drafts throughout this process. H-HY, KMC and RB each provided analytical suggestions, contributed to the content and edited the drafts of the manuscript.
Provenance and peer review Not commissioned; externally peer reviewed.
References
- 1.McCoy SB, Gibbons FX, Reis TJ, et al. Perceptions of smoking risk as a function of smoking status. J Behav Med. 1992;15:469–88. doi: 10.1007/BF00844942. [DOI] [PubMed] [Google Scholar]
- 2.Festinger L. A Theory of Cognitive Dissonance. Evanston, IL: Row, Peterson; 1957. [Google Scholar]
- 3.Hughes JR, Keely J, Naud S. Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction. 2004;99:29–38. doi: 10.1111/j.1360-0443.2004.00540.x. [DOI] [PubMed] [Google Scholar]
- 4.Festinger L, Carlsmith JM. Cognitive consequence of forced compliance. J Abnorm Soc Psychol. 1959;58:203–11. doi: 10.1037/h0041593. [DOI] [PubMed] [Google Scholar]
- 5.Croog SH, Richards NP. Health beliefs and smoking patterns in heart patients and their wives: a longitudinal study. Am J Public Health. 1977;67:921–30. doi: 10.2105/ajph.67.10.921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dillard AJ, Mccaul KD, Klein WMP. Unrealistic optimism in smokers: implications for smoking myth endorsement and self-protective motivation. J Health Commun. 2006;11(Suppl 1):93–102. doi: 10.1080/10810730600637343. [DOI] [PubMed] [Google Scholar]
- 7.Weinstein ND, Slovic P, Gibson G. Accuracy and optimism in smokers’ beliefs about quitting. Nicotine Tob Res. 2004;6(Suppl 3):S375–80. doi: 10.1080/14622200412331320789. [DOI] [PubMed] [Google Scholar]
- 8.Borland R, Yong HH, Balmford J, et al. Do risk-minimising beliefs about smoking inhibit quitting? Findings from the international tobacco control (ITC) four-country survey. Prev Med. 2009;49:219–23. doi: 10.1016/j.ypmed.2009.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chapman S, Wong WL, Smith W. Self-exempting beliefs about smoking and health: differences between smokers and ex-smokers. Am J Public Health. 1993;83:215–19. doi: 10.2105/ajph.83.2.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Oakes W, Chapman S, Borland R, et al. “Bulletproof skeptics in life’s jungle”: which self-exempting beliefs about smoking most predict lack of progression towards quitting? Prev Med. 2004;39:776–82. doi: 10.1016/j.ypmed.2004.03.001. [DOI] [PubMed] [Google Scholar]
- 11.Weinstein ND. Accuracy of smokers’ risk perceptions. Nicotine Tob Res. 1999;1 (Suppl 1):S123–30. doi: 10.1080/14622299050011721. [DOI] [PubMed] [Google Scholar]
- 12.Weinstein ND. Unrealistic optimism about sucseptibility to health problems: conclusions from a community wide sample. J Behav Med. 1986;10:481–500. doi: 10.1007/BF00846146. [DOI] [PubMed] [Google Scholar]
- 13.Weinstein ND, Marcus SE, Moser RP. Smokers’ unrealistic optimism about their risk. Tob Control. 2005;14:55–9. doi: 10.1136/tc.2004.008375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Myers M, Iscoe C, Jennings C, et al. Federal Trade Commission staff report on the cigarette advertising investigation. Bureau of Consumer Division; 1981. [accessed 1 Sep 2011]. Updated 1982 March 15. http://tobaccodocuments.org/lor/03607752-7763.html. [Google Scholar]
- 15.Udow A. Memo to Newman F: FTC Staff Report on Cigarette Advertising: Supports of Statements on “Consumer Knowledge” [online] Philip Morris; 1981. [accessed 1 Sep 2011]. Bates No. 1005141237. http://legacy.library.ucsf.edu/tid/oxc54e00/pdf. [Google Scholar]
- 16.Simon L, Greenberg J, Brehm J. Trivialization: the forgotten mode of dissonance reduction. J Pers Soc Psychol. 1995;68:247–60. [Google Scholar]
- 17.Fishbein M. Consumer Beliefs and Behavior with Respect to Cigarette Smoking: A Critical Analysis of the Public Literature. Urbana (IL): University of Illinois (US); 1977. Report No: 50379.01. [Google Scholar]
- 18.Johnson RE. Smoking and the reduction of cognitive dissonance. J Pers Soc Psychol. 1968;9:260–5. doi: 10.1037/h0025901. [DOI] [PubMed] [Google Scholar]
- 19.Willaing I, Jørgensen T, Iverse L. How does individual smoking behaviour among hospital staff influence their knowledge of the health consequences of smoking? Scand J Public Healt. 2003;31:149–55. doi: 10.1080/14034940210164876. [DOI] [PubMed] [Google Scholar]
- 20.Clark E, McCann TV, Rowe K, et al. Cognitive dissonance and undergraduate nursing students’ knowledge of, and attitudes about, smoking. J Adv Nurs. 2004;46:586–94. doi: 10.1111/j.1365-2648.2004.03049.x. [DOI] [PubMed] [Google Scholar]
- 21.McMaster C, Lee C. Cognitive dissonance in tobacco smokers. Addict Behav. 1991;16:349–53. doi: 10.1016/0306-4603(91)90028-g. [DOI] [PubMed] [Google Scholar]
- 22.McCann TV, Clark E, Rowe K. Undergraduate nursing students’ attitudes towards smoking health promotion. Nurs Health Sci. 2005;7:164–73. doi: 10.1111/j.1442-2018.2005.00228.x. [DOI] [PubMed] [Google Scholar]
- 23.Steele CM. The Psychology of self-affirmation: sustaining the integrity of the self. In: Berkowitz L, editor. Adv Exp Soc Psychol. Vol. 21. New York: Academic Press; 1988. pp. 261–302. [Google Scholar]
- 24.Taylor SE, Brown JD. Illusion and well-being: a social psychological perspective on mental health. Psychol Bull. 1988;103:193–210. [PubMed] [Google Scholar]
- 25.Lee WB, Fong GT, Zanna MP, et al. Regret and rationalisation among smokers in Thailand and Malaysia: findings from the International Tobacco Control Southeast Asia Survey. Health Psychol. 2009;28:457–64. doi: 10.1037/a0014669. [DOI] [PubMed] [Google Scholar]
- 26.Yong HH, Borland R. Functional beliefs about smoking and quitting activity among adult smokers in four countries: findings from the International Tobacco Control Four-Country Survey. Health Psychol. 2008;27(Suppl 3):S216–23. doi: 10.1037/0278-6133.27.3(suppl.).s216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Zanna MP, Cooper J. Dissonance and the pill: an attribution approach to studying the arousal properties of dissonance. J Pers Soc Psychol. 1974;29:703–9. doi: 10.1037/h0036651. [DOI] [PubMed] [Google Scholar]
- 28.Kunda Z. The case for motivated reasoning. Psychol Bull. 1990;108:480–98. doi: 10.1037/0033-2909.108.3.480. [DOI] [PubMed] [Google Scholar]
- 29.Fong GT, Cummings KM, Borland R, et al. The conceptual framework of the International Tobacco Control (ITC) Policy Evaluation Project. Tob Control. 2006;15(Suppl 3):iii3–11. doi: 10.1136/tc.2005.015438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Thompson ME, Fong GT, Hammond D, et al. The methodology of the international tobacco control four-country survey. Tob Control. 2006;15(Suppl 3):iii12–18. doi: 10.1136/tc.2005.013870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Salmon CT, Nichols JS. The next-birthday method of respondent selection. Public Opin Q. 1983;47:270–6. [Google Scholar]
- 32.Cohen J. A power primer. Psychol Bull. 1992;112:155–9. doi: 10.1037//0033-2909.112.1.155. [DOI] [PubMed] [Google Scholar]
- 33.Morris SB, DeShon RP. Combining effect size estimates in meta-analysis with repeated measures and independent-groups designs. Psychol Methods. 2002;7:105–25. doi: 10.1037/1082-989x.7.1.105. [DOI] [PubMed] [Google Scholar]
- 34.Yang J, Hammond D, Driezen P, et al. Health knowledge and perception of risks among Chinese smokers and non-smokers: findings from the Wave 1 ITC China Survey. Tob Control. 2010;19(Suppl 2):i18–23. doi: 10.1136/tc.2009.029710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Fiske AP, Kitayama S, Markus HR, et al. The cultural matrix of social psychology. In: Gilbert DT, Fiske ST, Lindzey G, editors. The Handbook of Social Psychology. 4. New York: McGraw-Hill; 2009. pp. 915–81. [Google Scholar]
- 36.Cummings KM, Morley CP, Hyland A. Failed promises of the cigarette industry and its effect on consumer misperceptions about the health risks of smoking. Tob Control. 2002;22(Suppl 1):i110–i17. doi: 10.1136/tc.11.suppl_1.i110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Cummings KM, Brown A, O’Connor R. Focus on tobacco: the cigarette controversy. Cancer Epidemiol Biomarkers Prev. 2007;16:1070–6. doi: 10.1158/1055-9965.EPI-06-0912. [DOI] [PubMed] [Google Scholar]
- 38.McGuire W. Resistance to persuasion conferred by active and passive prior refutation of the same and alternative counter-arguments. J Abnorm Soc Psychol. 1961;63:326–32. [Google Scholar]
- 39.Dickerson CA, Thibodeau R, Aronson E, et al. Using cognitive dissonance to encourage water conservation. J Appl Soc Psychol. 1992;22:841–54. [Google Scholar]
- 40.Stone J, Fernadez NC. To practice what we preach: the use of hypocrisy and cognitive dissonance to motivate behaviour change. Soc Pers Psychol Compass. 2008;2:1024–51. [Google Scholar]
- 41.Stone J, Aronson E, Crain AL, et al. Inducing hypocrisy as a means of encouraging young adults to use condoms. Pers Soc Psychol Bull. 1994;20:116–28. [Google Scholar]
- 42.Stone J, Wiegand AW, Cooper J, et al. When exemplification fails: hypocrisy and the motive for self-integrity. J Pers Soc Psychol. 1997;72:54–65. doi: 10.1037//0022-3514.72.1.54. [DOI] [PubMed] [Google Scholar]