

Abstract
Context:
The knowledge of the reasons for the placement of direct restorations makes possible to trace an epidemiological profile of a specific population and to direct the teaching of dentistry to techniques that are commonly used today and will be continued performed in the future.
Purpose:
The aim of this study was to verify the reasons for placement and replacement of direct restorations in patients treated in the Dental Clinic of the Uberaba University – Brazil.
Materials and Methods:
This study evaluated 306 restorative procedures carried out on 60 patients. During the treatment planning, a form that contained information about the patient's gender, tooth number, the classification of restorations, the reasons for placement and replacement of amalgam and tooth-colored restorations, the material that had to be removed and the new material used to fill the cavities was filled for each patient. Statistical analysis was carried out using Chi-square test (α = 0.05).
Results:
The data showed that most of the patients were female (66.7%). Of all the restorations placed, 60.45% were 1st-time placements, while 39.55% were replacements. For 1st-time restorations, the main reason for placement was primary caries (76.76%), followed by non-carious cervical lesions (15.14%). The amalgam restorations were replaced more frequently (67.77%). The primary reason for replacements was the presence of secondary caries (for both previous amalgam (42.68%) and composite (66.67%) restorations (P < 0.05). The resin composite was the most indicated material for the new restorations (98.04%) (P < 0.05).
Conclusions:
The main reason for placement of direct restorations was primary caries, while secondary caries was the main reason for replacements. In almost all cases, the material used to fill the cavities was the resin composite.
Keywords: Amalgam, caries, composite, direct restorations
Introduction
Dental caries is an infectious-contagious disease that has a chronic multifactorial pattern. The presence of microorganisms on dental surfaces is essential for the development of caries disease, but only their presence is not enough. Factors such as hygiene, alimentary habits, bacterial colonization, time and saliva composition influence the metabolism of bacteria on teeth, modulating caries activity.[1] Dental caries is a disease that promotes destruction of dental hard tissues initially by the acid dissolution of the enamel mineralized matrix. If the lesion is not properly treated, it can progress through the dentin and reach the dental pulp. The adoption of dental caries preventive actions, such as the use of fluoridated toothpaste and the fluoridation of water supply, promoted a significant decrease in the prevalence of dental caries throughout the world. However, that infectious disease still remains a significant problem in dentistry, being one of the main reasons that lead patients to the dental clinics.[2]
Teeth also have its structure compromised by trauma and by the occurrence of non-carious cervical lesions (NCCLs). As elderly population retains its teeth for longer, the issue of tooth wear is becoming of increasing importance to the dental profession. According to Wood et al.,[3] NCCL are classified as attrition, abrasion, erosion and abfraction. The prevalence of those lesions on the adult population is high. Previous studies showed that 73% of the patients evaluated had at least one tooth with one NCCL.[4,5] Most lesions are formed in first mandibular molar, first maxillary molar, first maxillary premolar, first mandibular premolar, second mandibular premolar.[3]
The development of dental restorative materials, as well as the restorative techniques, made possible the reconstruction of teeth with small or moderate degrees of destruction directly at the dental office. Currently, the most used materials used to restore a cavity definitively are the composite resin, the glass ionomer cement (GIC) and amalgam.
Dental amalgam is, basically, a mixture of a silver alloy with mercury and has been in use for over 200 years. This material provides strong, durable and good cost-effective direct posterior restoration. However, this material has some disadvantages such as poor esthetic characteristics, potential mercury exposure and lack of adhesion to the tooth structure. In addition, the use of channels, boxes, locks or pins for added retention in large amalgam restorations, involves the removal of additional tooth structure and therefore, weakens the remaining dental hard tissues.[6] In order to minimize tooth reduction, new materials that had adhesion to dental structures and could be used in more conservative cavities were developed, such as resin composites. The current composites do not have the same good mechanical properties then amalgam, but they also exhibit satisfactory clinical results and they are considered anesthetic material. Moreover, composites are multipurpose materials since they can be used in both anterior and posterior restorations.[7] Finally, GICs are widely applied to fill dental cavities thanks to its characteristic of releasing fluoride ions to the oral environment, preventing the occurrence of secondary caries. They have the capability to adhere to the tooth structure and they are also considered an esthetic material, because its color is similar to the tooth structure.[8]
Despite advances in the physical and mechanical properties, the restorations made with these materials are subject to failures, such as microleakage, fracture of the material, color change of both restorative material and tooth structure over the time, among others. When this happens, the dentist has to analyze each clinical case individually and choose the restorative material that best meets the needs of patients. The aim of this study was to verify the reasons for placement and replacement of direct restorations in patients treated in the dental clinic of the Uberaba University – Brazil, as well as the dental material used to fill the cavities.
Materials and Methods
After the Uberaba University Ethical Committee authorization, the patients signed an informed consent form authorizing the collection of their personal and clinical information. Totally 60 patients in good general health of both genders and aged between 18 and 60 years that were looking for dental treatment at Dental Clinic of the School of Dentistry of the Uberaba University were selected. Patients were examined by the need of direct restorative treatment by clinical and radiographic examination. Teeth that presented periapical lesions were not considered.
The clinical evaluation was carried out during 90 consecutive days, when 306 restorative procedures were evaluated. During the clinical evaluation, one of the following items was recorded as a reason for the 1st-time placement of each restoration: Primary caries, (NCCL; abrasion, erosion, or abfraction), fractured tooth (trauma) and other reasons (direct composite facets, diastema closure and recovery of canine guide occlusion and re-anatomization of anterior teeth).
If the new restoration replaced a failed restoration, they were also asked to record the cause of failure, according to the following reasons: Secondary caries, degradation, fracture of restoration, margin discolorations (for composites only), tooth fracture, poor anatomical form, pain/sensitivity, change of the material/esthetics (for amalgam only) and loss of the restoration (for amalgam only). The material indicated to fill the cavities were also recorded. Additional information, as the patient's age, gender and tooth treated, the class of restorations and restorative material used was also requested. The criteria used for assessing the reasons for placement or replacement of the restorations were similar to a previously published paper.[9]
After taking the data, all patients received complete dental treatment in the Dental Clinic of the Uberaba University.
All collected data were compared using the Chi-square test (α = 0.05). The data was analyzed using the software SPSS for Windows version 17.0 (IBM Corp, Armonk, New York, EUA).
Results
The obtained data showed that most of the patients were female (66.7%). The statistical analyses are shown in Figures 1–4. Figure 1 shows the reasons for 1st-time placement of direct restorations. These restorations represented 60.45% (185) of total cases evaluated and the presence of primary caries (76.76%) was the main reason for placement of direct restoration (P < 0.05). The NCCLs (15.14%), tooth fracture (2.94%) and other reasons (3.24%), as direct composite facets, diastema closure and recovery of canine guide occlusion and re-anatomization of anterior teeth showed no statistically significant differences among them.
Figure 1.
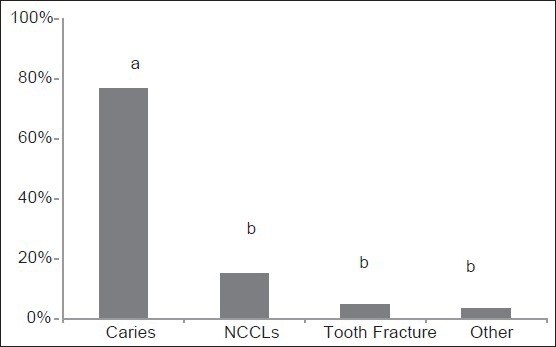
Reasons for placement of direct restorations. Similar letters mean no statistical differences
Figure 4.
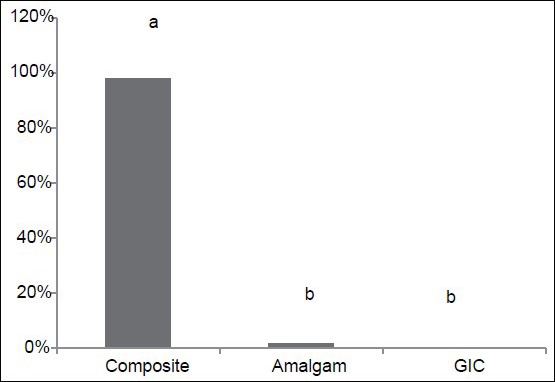
Dental material used to fill the cavities. Similar letters mean no statistical differences
Replacements represented 39.55% (121) of the total cases evaluated. The composite restorations were replaced in 32.23% of cases and amalgam restorations were removed in 67.77% of cases. Previous GIC restorations were not found during the clinical evaluation. Figure 2 shows the reasons for replacement of composite restorations. The obtained data showed that most composite restorations (42.68%) of fail due to the presence of secondary caries (P < 0.05). Other factors, as degradation (10.26%), fracture of the restoration (10.26%), margin discoloration (5.13%), poor anatomical form (5.13%) and tooth pain/sensitivity (2.56%) were also observed.
Figure 2.
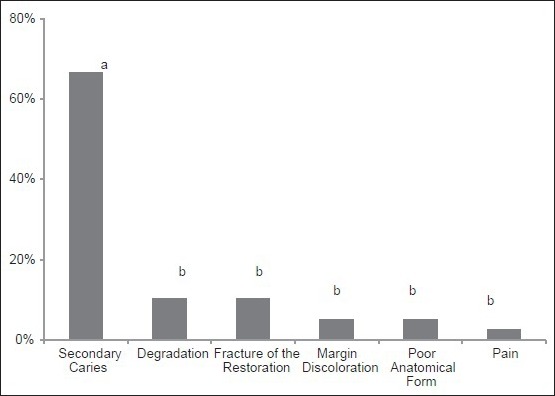
Reasons for replacement of composite restorations. Similar letters mean no statistical differences
Figure 3 shows that the main reasons that led to the replacement amalgam restorations were the presence of secondary caries (42.68%) and esthetics (36.59%). These results were similar by themselves but were higher than fracture of the restoration (13.41%), poor anatomical form (4.88%) and loss of the restoration (2.44%) (P < 0.05).
Figure 3.
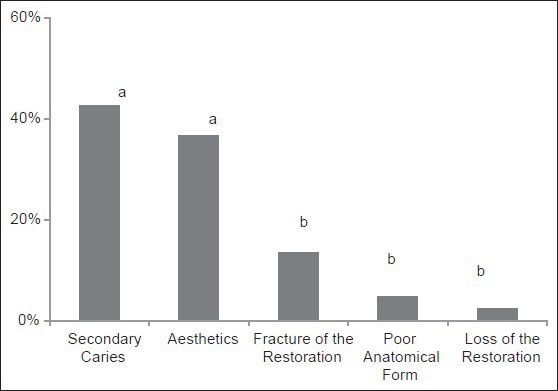
Reasons for replacement of amalgam restorations. Similar letters mean no statistical differences
Finally, Figure 4 shows the material used to fill the cavities. In almost all cases (98.04%) the resin composite was the dental material chosen to restore teeth (P < 0.05). The other materials used were amalgam (1.63%) and GIC (0.33%).
Discussion
The Dental Clinic of the Uberaba University is a reference in the city of Uberaba – Brazil, for dental treatment for low-income population, because most of dental procedures executed in the institution have no cost to the patient, or when it has, the cost is much lower than those charged in private dental offices. The patients usually come to the university clinic for emergency dental care or to do a checkup of the current situation of their oral cavity. In the latter situation, teeth that have primary or secondary caries, imperfect restorations and other problems that patients report no symptoms but need to be treated are often diagnosed. Therefore, the patient has the opportunity to do all the necessary dental treatment for free, or at a minimum cost.
The indication of placement or replacement of direct restorations depends on the ability and knowledge of the dentist who is examining the patient. In this way, the subjectivity is an important factor that must be considered, since a clinician can indicate the replacement of a restoration while other can suggest only the polishment of the same restoration. In the present research, the planning of clinical cases and dental procedures were performed by the last-year undergraduate dental students. These actions were always performed under supervision of expertise tutors in all dental specialties, what reduced the subjective factor and left the results more consistent.
The present study showed that dental caries, whether primary or recurrent, was the main reason that led to the placement or the replacement of direct dental restorations, indicating that caries is still a significant dental problem in the population. It is possible to believe that the occurrence of dental caries is not limited only to the individual issues, but also to social, economic, cultural, environmental and health-system-related factors. Health care systems are important for educating, promoting, improving and maintaining health of the population. Through a competent health service, patients can be warned of disease that may be present and so facilitate treatment; risks factors whose modification could reduce the incidence of disease and illness in the future can be identified and further, how controlling such factors can contribute to maintain a good quality of life. Now-a-days, Brazil, a development country, holds the 85th position in the UN human development ranking.[10] Despite the health conditions in the country are improving, the oral health preventive policy is still deficient, because it does not cover the entire population, especially the low-income people. As a result, the patient comes to the dental clinic with an installed disease that could have been prevented if he was concerned with oral hygiene and its importance.
In this study, almost 16% of the 1st-time restorations were due to the presence of NCCLs. It is important to state that this number represents the quantity of lesions that have been treated and not the total number of cases found in the research. According to Wood et al.,[3] the prevalence of NCCL's increases with the aging of the population. In the present study, the option for treating these lesions was based on the esthetic involvement and tooth sensibility, always in conjunction with treatment of parafunctional habits and occlusal adjustments. In the present research, it was noted the occurrence of traumatized teeth. As discussed before, the dental service provided in the Uberaba University School of Dentistry is a reference in town for emergency treatment. Thus, it was expected that cases of dental trauma appear with some frequency. When the fracture caused little loss of tooth structure, teeth were treated with direct restorations.
In the present research, current techniques for caries diagnosis were used, such as visual and tactile clinical examination, radiographic examination, transillumination and caries detector dyes. Those methods are considered effective and they reduce the chance of obtaining false positive results.[11] They were useful to diagnosis secondary caries, which are lesions formed at the margin of an existing restoration and represented, in the current study, the main reason for replacement of amalgam and composite restorations, what is in accordance to previously published data.[9] The occurrence of secondary caries is closely related to the degradation of the margins of the restoration and consequently, to the microleakage, that is the clinically detectable passage of bacteria, fluids, molecules or ions between the cavity wall and the restorative material. This may occur due to polymerization contraction stress of the composite, the use of incorrect adhesive and restorative techniques and if the dentist fills a cavity that has carious infected dentin. In the latter case, the microleakage would be a gateway to the supply of substrate for cariogenic bacteria present in the cavity. Thus, it is recommended to clean the remaining dentin with a bactericidal agent, such as chlorhexidine, before filling the cavity, in order to decrease the viability of the bacteria. Furthermore, it has been demonstrated that the use of chlorhexidine prior to restoration has no adverse effect on the microleakage of composite restorations.[12] Other factors that can lead to secondary caries lesions are fracture of the margins of the restoration, degradation of the restorative material, the presence of erosive lesions around the restoration and accumulation of biofilm on the margins of the restoration. These factors emphasize the importance of adopting an effective policy of prevention in oral health.
Esthetics (36.59%) was another main reason that led to the replacement of amalgam restorations. Dental amalgam has many advantages when used as a restorative material, such as high compressive strength, excellent wear characteristics, is easier to use than other materials, is less technique-sensitive and present satisfactory long-term results.[6] However, its poor esthetics is one major disadvantage, especially nowadays, where the concepts of esthetics are most valued. The decision to replace an amalgam restoration for esthetics purposes was based on the desire of the patient to have a restoration similar to tooth structure. Evidently, this was possible only after careful evaluation of the risks and benefits of changing an old, but clinically satisfactory, restoration by a new esthetic filling.
In this same aspect, factors related to the appearance of composite restorations, such as discoloration of the entire restorative material, margin discoloration and poor anatomic form were reasons that led to the replacement of composite restorations. However, the replacement occurred only after the clinicians were sure that the polishing of restorations would not provide satisfactory results.
Composites are the universally used tooth-colored direct restorative materials. Thanks to their properties, such as esthetics and advantages of adhesive technology and the to their constant development, such as an increase in wear resistance, tensile bond strength, fracture strength and improved polishing properties, composites have taken over the place that was occupied by amalgam.[7] The present study showed that composite was the most selected material to fill the cavities (98.04%). Obviously this material has its disadvantages, such as the use of an adhesive sensitive-technique and the necessity to do operatory field isolation, but its clinical success justifies its use in all types of cavities and in NCCLs.[13]
Despite amalgam has lost its place, it still has its indications, such as its use in patients with high caries risk and in cases where it is not possible to realize the operatory field isolation. Conventional or resin-modified GICs is also indicated in cases in which the humidity of the operative field cannot be fully controlled, but their poorer mechanical properties when compared with composites limits their use to cavity restorations in permanent teeth.[14]
Conclusion
The present research showed that the main reason for placement of direct restorations was primary caries, while secondary caries was the main reason for replacements. In almost all cases, the material used to fill the cavities was the resin composite. Understanding the reasons for treatment, pattern of use and failure of restorative materials are important to recognize many aspects of contemporary clinical practice. The knowledge of current tendencies in restorative procedures is useful to guide dental schools to upgrade the teaching of dentistry. In addition, information on the motives for the placement and replacement of direct restorations is important as a basis for the recording of treatment patterns and for the prevention of future failures.
Acknowledgments
The authors are grateful to the Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) Brazil, for providing financial support (Grant no. PEE-01203-10).
Footnotes
Source of Support: The authors are grateful to the Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG) Brazil, for providing financial support (Grant no. PEE.01203.10).
Conflict of Interest: None declared.
References
- 1.Featherstone JD, Doméjean S. The role of remineralizing and anticaries agents in caries management. Adv Dent Res. 2012;24:28–31. doi: 10.1177/0022034512452885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Nascimento MM, Gordan VV, Qvist V, Litaker MS, Rindal DB, Williams OD, et al. Reasons for placement of restorations on previously unrestored tooth surfaces by dentists in The Dental Practice-Based Research Network. J Am Dent Assoc. 2010;141:441–8. doi: 10.14219/jada.archive.2010.0197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wood I, Jawad Z, Paisley C, Brunton P. Non-carious cervical tooth surface loss: A literature review. J Dent. 2008;36:759–66. doi: 10.1016/j.jdent.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 4.Bergström J, Eliasson S. Cervical abrasion in relation to toothbrushing and periodontal health. Scand J Dent Res. 1988;96:405–11. doi: 10.1111/j.1600-0722.1988.tb01575.x. [DOI] [PubMed] [Google Scholar]
- 5.Telles D, Pegoraro LF, Pereira JC. Incidence of noncarious cervical lesions and their relation to the presence of wear facets. J Esthet Restor Dent. 2006;18:178–83. doi: 10.1111/j.1708-8240.2006.00015.x. [DOI] [PubMed] [Google Scholar]
- 6.Parolia A, Kundabala M, Gupta V, Verma M, Batra C, Shenoy R, et al. Microleakage of bonded amalgam restorations using different adhesive agents with dye under vacuum: An in vitro study. Indian J Dent Res. 2011;22:252–5. doi: 10.4103/0970-9290.84298. [DOI] [PubMed] [Google Scholar]
- 7.Ferracane JL. Resin composite – State of the art. Dent Mater. 2011;27:29–38. doi: 10.1016/j.dental.2010.10.020. [DOI] [PubMed] [Google Scholar]
- 8.Yengopal V, Mickenautsch S. Caries-preventive effect of resin-modified glass-ionomer cement (RM-GIC) versus composite resin: A quantitative systematic review. Eur Arch Paediatr Dent. 2011;12:5–14. doi: 10.1007/BF03262772. [DOI] [PubMed] [Google Scholar]
- 9.Braga SR, Vasconcelos BT, Macedo MR, Martins VR, Sobral MA. Reasons for placement and replacement of direct restorative materials in Brazil. Quintessence Int. 2007;38:e189–94. [PubMed] [Google Scholar]
- 10.ed. 1. Canada: y Gilmore Printing Services Inc; 2013. United Nations. Human development report 2013. In: The Rise of the South: Human Progress. [Google Scholar]
- 11.Rochlen GK, Wolff MS. Technological advances in caries diagnosis. Dent Clin North Am. 2011;55:441–52. doi: 10.1016/j.cden.2011.02.018. vii. [DOI] [PubMed] [Google Scholar]
- 12.Geraldo-Martins VR, Robles FR, Matos AB. Chlorhexidine's effect on sealing ability of composite restorations following Er: YAG laser cavity preparation. J Contemp Dent Pract. 2007;8:26–33. [PubMed] [Google Scholar]
- 13.van Dijken JW, Pallesen U. A six-year prospective randomized study of a nano-hybrid and a conventional hybrid resin composite in Class II restorations. Dent Mater. 2013;29:191–8. doi: 10.1016/j.dental.2012.08.013. [DOI] [PubMed] [Google Scholar]
- 14.Kim KL, Namgung C, Cho BH. The effect of clinical performance on the survival estimates of direct restorations. Restor Dent Endod. 2013;38:11–20. doi: 10.5395/rde.2013.38.1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]