

Abstract
Background:
One out of every two children sustains a dental injury most often between 8 and 10 years of age. Majority of these teeth subsequently become non-vital and most often with immature apex. Management of these teeth is an enormous challenge for lack of apical stop. Calcium hydroxide in various formulations has maximum literature support in favor of successful apexification or induced apical closure.
Aim:
The aim of the following study is to determine the efficacy of calcium hydroxide in a different formulation to induce apexification.
Materials and Methods:
The present study was undertaken on 51 children of 8-10 years of age (both sexes) at Dr. R Ahmed Dental College and Hospital from April 2006 to March 2007. All children had one or two maxillary permanent central incisor (s), non-vital and apices open. In all the cases, apexification was attempted with either calcium hydroxide mixed with sterile distilled water, or calcium hydroxide plus iodoform in methyl cellulose base, or calcium hydroxide plus iodoform in polysilicone oil base. The success of apexification was determined on the basis of clinical and radiographic criteria.
Results:
In the pre-operative asymptomatic cases (72.55%), failure occurred in only 5.45% cases and pre-operative symptomatic cases failure rate was as high as 35.71%. Success rate was 94.6% in cases with narrow open apices, whereas 64.28% in wide open apices. In cases with pre-existing apical radiolucencies, successful apexification occurred in 63.63% and success rate was 92.5% in the cases without pre-existing apical radiolucencies. Average time consumed for apexification was minimum with calcium hydroxide plus iodoform in polysilicone oil base.
Conclusion:
The overall success rate observed to be 86.27%, which is in close proximity to the findings of most of the previous studies across the globe.
Keywords: Apexification, calcium hydroxide, maxillary permanent incisor
Introduction
International Association of Dental Traumatology reported that one out of every two children sustain a dental injury most often between 8 and 12 years of age.[1] Many of these injuries subsequently make the teeth non-vital or pulpless. Successful management of pulpless young permanent teeth demands enormous clinical acumen. The main challenge in such cases is to overcome the lack of apical stop against, which endodontic fillers can be compacted. A number of procedures have been attempted ranging from upside down usage of Gutta-percha points in maxillary anteriors, orthograde use of many medicaments, e.g. polyantibiotic pastes, retrograde sealing of the open apices and recent recommendation of single appointment orthograde insertion of mineral trioxide aggregate. All these procedures are called as “apexification” or “induced apical closure.”
Apexification aims at control and/or elimination of periapical pathosis of endodontic origin to promote apical closure and achieve valuable root length for long-term success of restorations.
The success of calcium hydroxide in various forms and formulations as an intra-canal medicament for apexification has immense literature support. However, time taken for successful apexification varied in those studies.
Walia et al.,[2] noted that teeth with narrow open apices in older children took shorter treatment time than in younger children. On the contrary, Dominguez et al.,[3] observed that the presence or absence of apical pathology before treatment hardly influence the duration of treatment for successful apical closure. Sheehy and Roberts[4] found that the average length of time for apical barrier formation is approximately 5-20 months. Furthermore, the type of apical closure in apexification varies. A study by Ballesio et al.,[5] found three types of apical barrier formation, namely (i) a physiologic development of apical portion with a final root length, equal to contralateral tooth (ii) formation of a cap like barrier and (iii) an apical development with the final root length, slightly shorter than the contralateral sound tooth through the formation of different layers of mineralized tissue over the time.
As far as the success rate is concerned, Sheehy and Roberts,[4] Gu et al.,[6] Morse et al.,[7] showed 74-100%, 94% and 100% respectively with the use of different formulations of calcium hydroxide in apexification.
Slack and Jones[8] observed that the psychologic well being of children can be adversely influenced by an injury to the teeth that causes an unsightly fracture and this kind of injury requires proper management.
This study was aimed at estimating the efficacy of different forms and formulations of calcium hydroxide, applied intracanally for apexification through orthograde route in 8-10 years aged children of Kolkata and its suburbs.
Materials and Methods
Selection of samples
A total number of 51 children of mixed socio-economic status were selected for the study, ranging in age from 8 to 10 years irrespective of their caste, creed and sex from the patients at out-patient Department of Pedodontics and Preventive Dentistry, Dr. R Ahmed Dental College and Hospital, Kolkata between April 2006 to March 2007 on the basis of selection criteria and exclusion criteria.
Selection criteria
Strict compliance with IAP recommended Childhood Immunization Program
Selected children must have a full complement of teeth normal for 8-10 years of age
All the selected children must have teeth fracture 11 and/or 21 Ellis and Davey cl-III traumatic injury
The injured tooth/teeth must have restorability
The injured tooth/teeth must be free from fracture of root and/or alveolar bone
Absence of traumatic bite in teeth 11 and/or 12.
Exclusion criteria
Presence of any congenital abnormality
Presence of diabetes, human immunodeficiency virus/hepatitis B/hepatitis C or any chronic debilitating disease
Parents or caregivers have a poor concern about oral hygiene
Children receiving antibiotics or steroids
Children undergoing orthodontic mechanotherapy or having pernicious oral habits.
Required consent from the parents/caregivers duly procured and clearance from Institutional Ethical Committee duly collected.
Non-vitality of the teeth to be studied is confirmed through clinical and radiographic examination.
During the examination, several questions were asked and the implication of each answer was different but all these together helped in forming the correct diagnosis.[9]
The whole sample population was divided into three groups, consisting 17 patients in each group. Group 1 consisted those treated with calcium hydroxide (Ca[OH]2) powder mixed with distilled water, Group 2 and Group 3 consisted those treated with non-setting Ca (OH)2 without iodoform and non-setting Ca (OH)2 with iodoform respectively.
Other materials and armamentarium used are those recommended in apexification in standard text books.
Methods
Selected patients underwent a quick general and thorough oral examination after history taking, then after securing a desired level of co-operation through explaining the procedure to be done, local anesthesia was administered followed by rubber dam isolation, prior to it anesthesia was achieved. During the whole procedure, the children were praised for their co-operation and in addition other behavior modification techniques were also applied in a non-threatening manner.
The access cavity was prepared and a straight line access to the root canal was achieved. Then the canal patency was established, working length determined and cleaning, shaping of the canal was done, 2 mm short of radiographic apex. The canal was continuously irrigated with sterile normal saline solution without any force followed by drying. Thus, the canal was made ready to receive different forms of calcium hydroxide, predetermined for each group.
Calcium hydroxide was inserted inside the canal and access cavity was duly sealed with non-eugenol based zinc-oxide cement, Cavit. The patients were discharged keeping records of their contact numbers. The patients were then recalled after 24 h, then after 3 months and as per their requirement in case of any discomfort or objective symptoms relating to the tooth undergoing apexification.
After 3 months, the teeth were clinically and radiographically evaluated for:
Presence or absence of any subjective or objective symptoms
Radiographic evidence of any progression or regression of pre-existing pathology
Radiographic evidence of calcific barrier formation in the apical region, which was re-checked clinically with a paper point.
The canals were obturated, when the successful apical bridge formation was confirmed.
At the routine recall visits, the outcome of the procedures was assessed through evaluation on the following criteria:
Type of calcium hydroxide used and time taken for complete apical bridge formation in respective groups
Incidence of success in cases, having preexisting pathology
The association of patient compliance and success of apexification
Type of calcium hydroxide and mode of apical closure
Pretreatment status of root formation and time taken for apexification
Association of pre-existing symptoms and success of apexification.
On the basis of this evaluation, the data were statistically analyzed and distribution tables and charts were made. The data were analyzed by Z-test and Chi-square test to assess the statistical significance of the study, result and observations.
Result and Observations
The 51 children were equally divided into three groups, each group consisted of 17 children and each group received a particular calcium hydroxide.
Discussion
Dental injury is very common. International Association of Dental Traumatology reported one out of every two children sustain this injury, most often between 8 and 12 years of age.[1] This injury not only traumatize the tooth, but also psychosocial development, academic progression, general and mental health[8]. These injuries have a wide range of presentations. And so, there are many classifications of these injuries. But most important is proper addressal of this trauma at the right time. Unfortunately, lack of access and affordability act as a hindrance to it and the tooth involved becomes non-vital and the normal anatomical process of apex closure stopped. Apexification followed by restoration of these unsightly teeth is one of the most accepted treatments in children aged 8-10 years. Number of materials have been tried to induce apical closure in non-vital teeth with open apex. However, the success with calcium hydroxide is the zenith in the dental literature since its use in dentistry by Hermann[10]. Granath[11] first reported the use of Calcium Hydroxide for apical closure in 1959. The present study explored the efficacy of different forms of calcium hydroxide in apexification in the focus of various parameters.
In this study, the overall success rate of apexification with different forms of calcium hydroxide delivered in orthograde approach and judging by radiographic apical barrier formation is 86.27% (Avg.) [Table 1], which is in consensus with Sheehy and Roberts[4] (74-100%) in 1997, Walia et al.,[2] Rodd et al.[12] (90%) in 2002, Gu et al.,[6] (94.4%) in 2007 and Walia et al.,[2] (100%) in 2000 [Figures 1–4].
Table 1.
Type of calcium hydroxide used and outcome of apexification
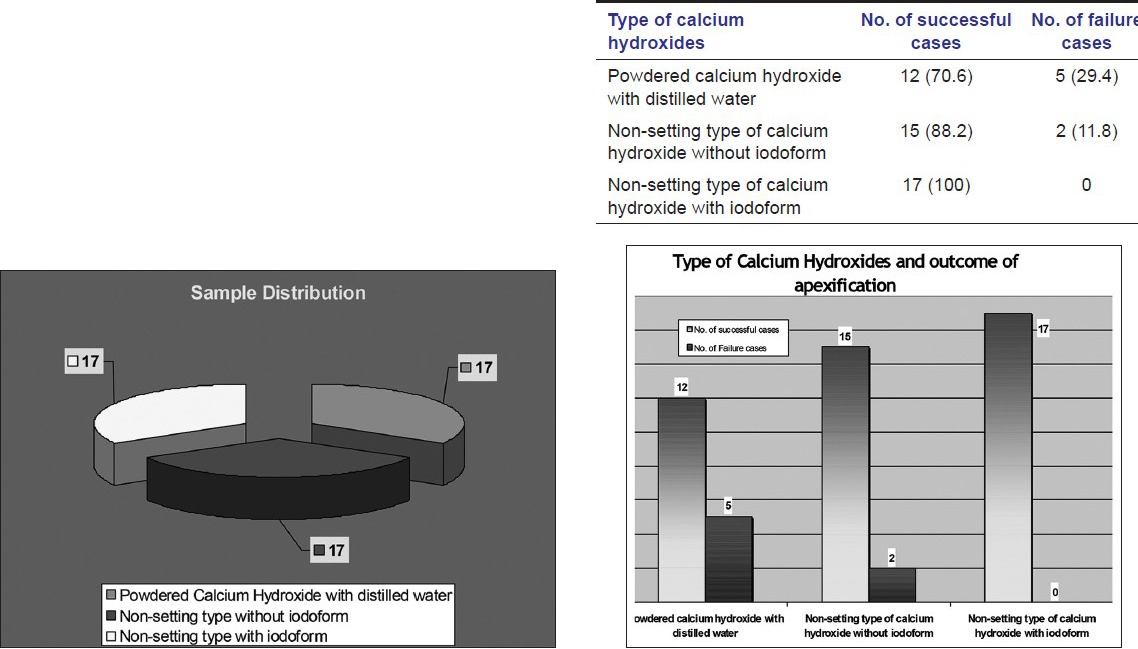
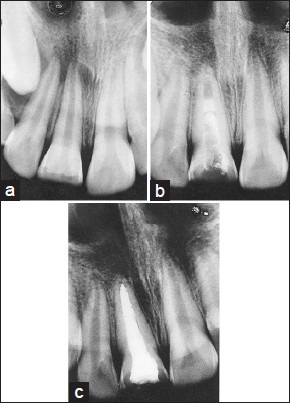
Figure 1.
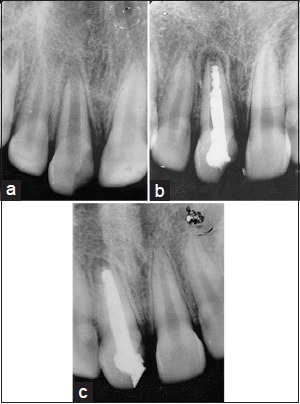
(a) Apexification induced by non-setting type of calcium hydroxide with iodoform pre-operative (b) apexification induced by non-setting type of calcium hydroxide with iodoform per-operative (c) apexification induced by non-setting type of calcium hydroxide with iodoform post-operative
Figure 4.
(a) Apexification induced by powdered calcium hydroxide with distilled water pre-operative (b) apexification induced by powdered calcium hydroxide with distilled water per-operative (c) induced by powdered calcium hydroxide with distilled water post-operative
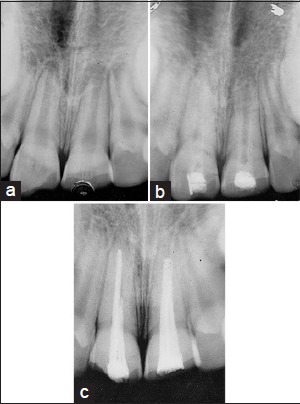
Figure 2.
(a) Apexification induced by non-setting type of calcium hydroxide with iodoform pre-operative (b) apexification induced by non-setting type of calcium hydroxide with iodoform per-operative (c) apexification induced by non-setting type of calcium hydroxide with iodoform post-operative
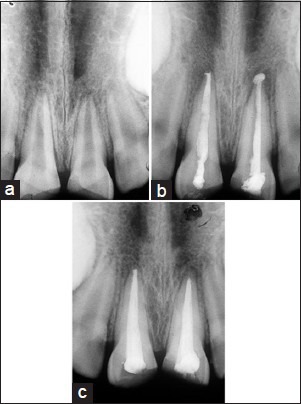
Figure 3.
(a) Apexification induced by non-setting type of calcium hydroxide pre-operative (b) apexification induced by non-setting type of calcium hydroxide per-operative (c) apexification induced by non-setting type of calcium hydroxide post-operative
However, Kleier and Barr[13] studied the clinical and radiographic success of calcium hydroxide apexification in 48 patients with non-vital teeth with open apices and found statistically significant relationship with the presence of radiolucency at periapex, presence or absence of symptoms pre-operatively and status of root-end closure and outcome of apexification.
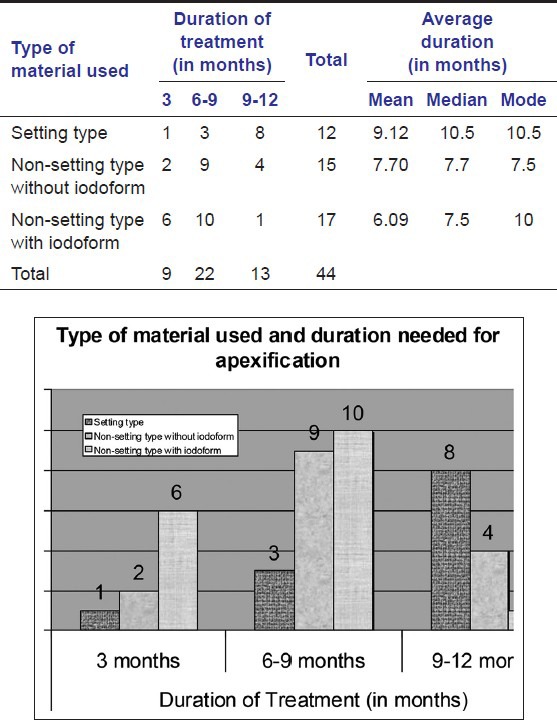
In the present study, [Table 2] the average time taken for apexification by different forms of calcium hydroxide are 9.12 months for calcium hydroxide with distilled water, 7.7 months for non-setting type calcium hydroxide without iodoform and 6.09 months for calcium hydroxide with iodoform respectively without any statistical significance in favor of any of these materials. Sheehy and Roberts,[4] Walia et al.,[2] Dominguez et al.,[3] Kleirer and Barr[13] observed for (on and average) 5-20 months, 7 ± 2.5 months, 6 months, 12 ± 7 months, respectively in their studies.
Table 2.
Duration of treatment with different types of calcium hydroxide
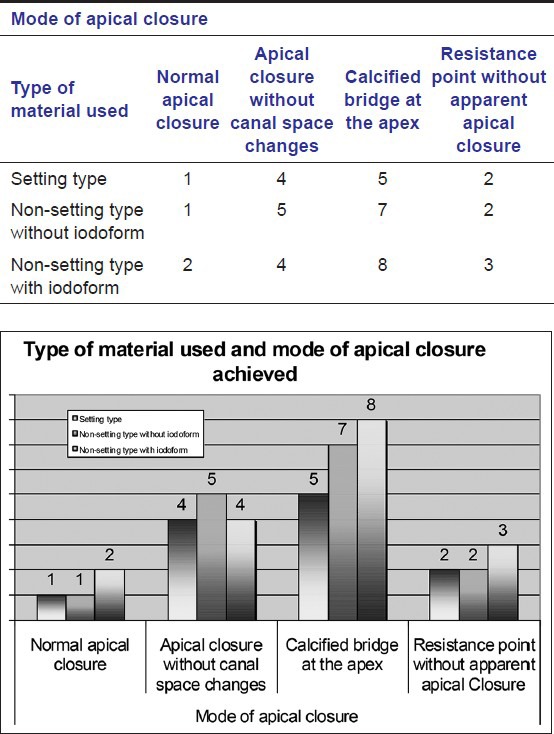
In the present study, [Table 3] suggests that there was significant variation in the mode of apical closure among different subjects (χ2 = 13.64; d.f = 3; P < 0.01). There was no significant correlation between the type of material used and mode of apical closure achieved. This is in correlation with the findings of Dominguez et al.[3].
Table 3.
Mode of apical closure in successful apexification
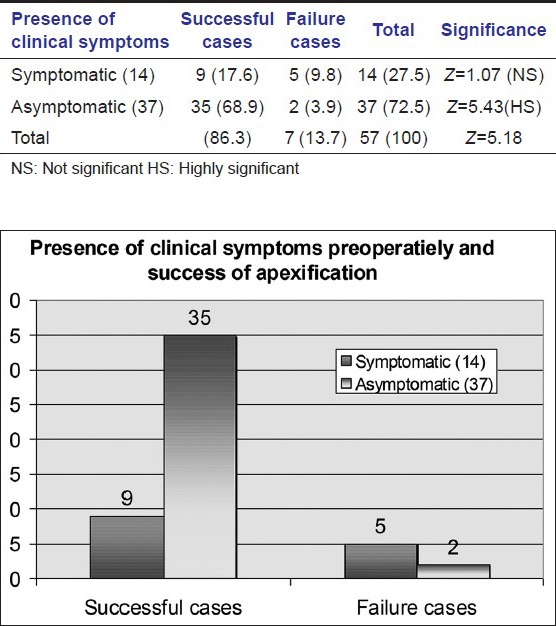
In the present study, [Table 4] illustrates success rate of pre-operative asymptomatic cases is very high and statistically highly significant (Z = 5.43, P < 0.001). The failure rate of the cases with pre-operative symptoms is not significant (Z = 1.07, P > 0.05). These findings of the present study is mostly similar with the studies mentioned in a review on apexification by Rafter.[14]
Table 4.
Presence of clinical symptoms pre-operatively and success of apexification
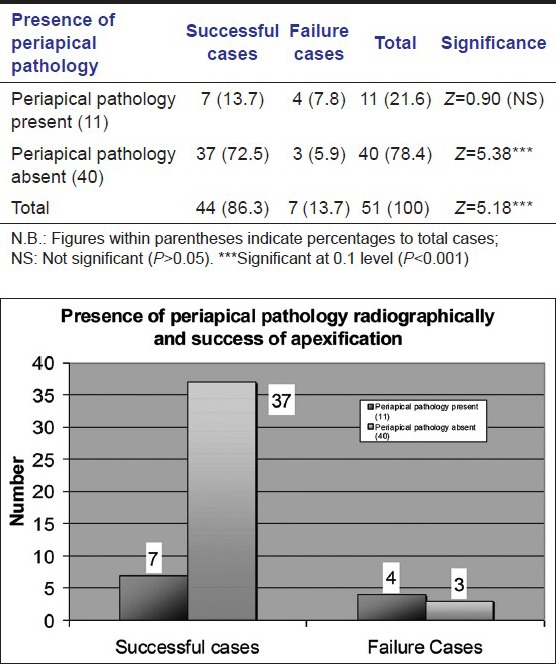
As far as root formation status and apexification success is concerned in the present study, it is revealed that significantly more success is obtained in narrow open apex cases (Z = 5.43, P < 0.001). Chi-square test also revealed this significance (χ2 = 7.88, d.f = 1; P < 0.01). Walia et al.,[2] Finucane and Kinirons[15] and Kleir and Barr[13] also found a similar result [Table 5]. Success rate of apexification in cases with the absence of preprocedural periapical radiolucencies is noted very highly significant (Z = 5.38; P < 0.001). On the contrary, the success rate of the cases with periapical radiolucencies prior to the starting of apexification, is only 21.6% and statistically not significant (Z = 0.9; P > 0.05). This findings is similar with the findings of Kalaskar et al.,[16] Kusgoz et al.,[17] [Table 6].
Table 5.
Pretreatment status of root end development and success of apexification
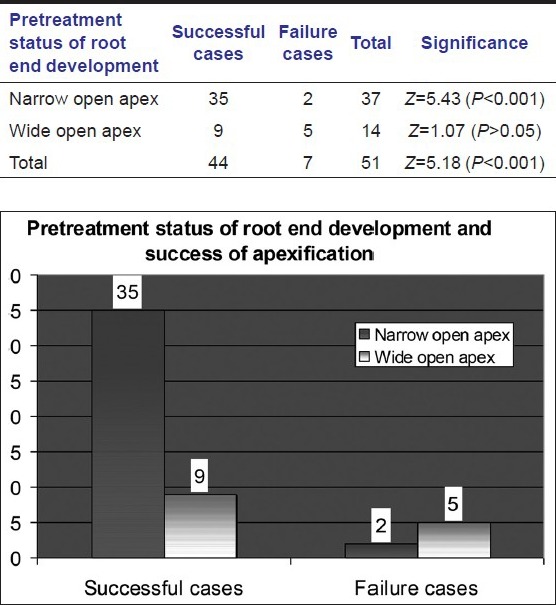
Table 6.
Presence of periapical pathology radiographically and success of apexification
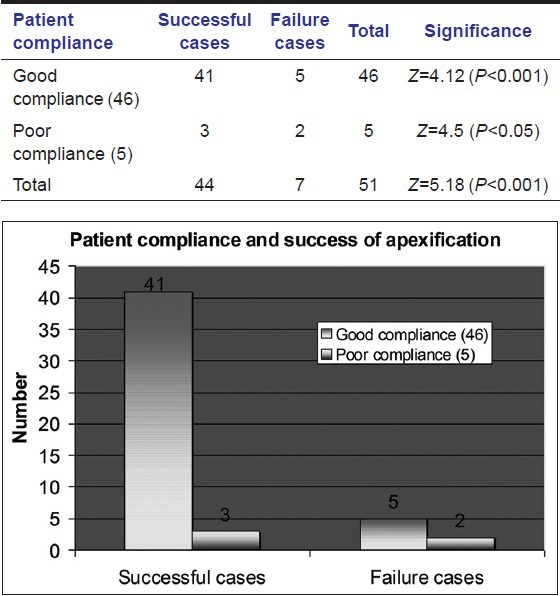
Present study also demonstrates that success occurs in 60% cases with poor patient compliance [Table 7], which is in consensus with Gupta and Sharma.[18]
Table 7.
Patient compliance and success of apexification
In this study, conservative approach was preferred as it saved surgical trauma along with accelerated calcific bridge formation. Puri et al.[19] had a similar conclusion in their study.
These wide variations of results in this present study might be related to the usage of the different proprietary preparations of calcium hydroxide on the patients of different geographic location, ethnicity and socio-economic status etc.
Acknowledgment
We would like to thank, Department of Pedodontics and Preventive Dentistry, Dr. R Ahmed Dental College and Hospital, 114 A.J.C Bose Road, Kolkata-700 014, West Bengal, India.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.McDonald RE, Avery DR, Dean JA. Management of trauma to the teeth and supporting tissues. 8th ed. St. Louis, Missouri: MOSBY; 2004. Dentistry for the Child and Adolescent; p. 455. [Google Scholar]
- 2.Walia T, Chawla HS, Gauba K. Management of wide open apices in non-vital permanent teeth with Ca (OH) 2 paste. J Clin Pediatr Dent. 2000;25:51–6. doi: 10.17796/jcpd.25.1.n224g827014n02n2. [DOI] [PubMed] [Google Scholar]
- 3.Dominguez Reyes A, Muñoz Muñoz L, Aznar Martín T. Study of calcium hydroxide apexification in 26 young permanent incisors. Dent Traumatol. 2005;21:141–5. doi: 10.1111/j.1600-9657.2005.00289.x. [DOI] [PubMed] [Google Scholar]
- 4.Sheehy EC, Roberts GJ. Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: A review. Br Dent J. 1997;183:241–6. doi: 10.1038/sj.bdj.4809477. [DOI] [PubMed] [Google Scholar]
- 5.Ballesio I, Marchetti E, Mummolo S, Marzo G. Radiographic appearance of apical closure in apexification: Follow-up after 7-13 years. Eur J Paediatr Dent. 2006;7:29–34. [PubMed] [Google Scholar]
- 6.Gu HJ, Xu Q, Liu LM, Ouyang Y. Treatment of chronic apical periodontitis teeth complicated by open apices with Vitapex in the adults. Shanghai Kou Qiang Yi Xue. 2007;16:140–3. [PubMed] [Google Scholar]
- 7.Morse DR, O’Larnic J, Yesilsoy C. Apexification: Review of the literature. Quintessence Int. 1990;21:589–98. [PubMed] [Google Scholar]
- 8.Slack GL, Jones JM. Psychological effect of fractured incisors. Br Dent J. 1955;99:386–8. [Google Scholar]
- 9.Marwah N. Text Book of Pediatric Dentistry. 2nd ed. New Delhi: Jaypee Brothers Medical Publishers; 2009. Traumatic injuries to anterior teeth; p. 554. [Google Scholar]
- 10.Hermann BW. Calcium hydroxid als mittel zum be handle und fullen. Med Diss V German Dissertation; 1920 Adopted from Siqueira JF Jr, Lopes HP Mechanisms of antimicrobial activity of calcium hydroxide: a critical review. International Endodontic Journal. 1999;32:361–369. doi: 10.1046/j.1365-2591.1999.00275.x. [DOI] [PubMed] [Google Scholar]
- 11.Granath LE. Odontol Revy. 3rd ed. Vol. 10. Copenhagen, Munksgaard, 1994: Wiley; 1959. Nagra Synpunkter pa dehaudiligen aV trauma tiserade Incisiver pabarn; p. 272. Adopted from Andreasen JO, Andreasen FM Textbook and Colour Atlas of Traumatic Injuries to the teeth. Reference No: 109. [Google Scholar]
- 12.Rodd HD, Davidson LE, Livesey S, Cooke ME. Survival of intentionally retained permanent incisor roots following crown root fractures in children. Dent Traumatol. 2002;18:92–7. doi: 10.1034/j.1600-9657.2002.180209.x. [DOI] [PubMed] [Google Scholar]
- 13.Kleier DJ, Barr ES. A study of endodontically apexified teeth. Endod Dent Traumatol. 1991;7:112–7. doi: 10.1111/j.1600-9657.1991.tb00194.x. [DOI] [PubMed] [Google Scholar]
- 14.Rafter M. Apexification: A review. Dent Traumatol. 2005;21:1–8. doi: 10.1111/j.1600-9657.2004.00284.x. [DOI] [PubMed] [Google Scholar]
- 15.Finucane D, Kinirons MJ. Non-vital immature permanent incisors: Factors that may influence treatment outcome. Endod Dent Traumatol. 1999;15:273–7. doi: 10.1111/j.1600-9657.1999.tb00787.x. [DOI] [PubMed] [Google Scholar]
- 16.Kalaskar R, Tiku A, Damle SG. Periapical repair and apical closure of a pulpless tooth using calcium hydroxide: A case report. J Indian Soc Pedod Prev Dent. 2004;22:158–61. [PubMed] [Google Scholar]
- 17.Kusgoz A, Yildirim S, Gokalp A. Nonsurgical endodontic treatments in molar teeth with large periapical lesions in children: 2-year follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:e60–5. doi: 10.1016/j.tripleo.2007.01.022. [DOI] [PubMed] [Google Scholar]
- 18.Gupta S, Sharma A. Unmonitored apexification of wide open apex in nonvital, immature incisor: A case report. J Clin Pediatr Dent. 1996;20:145–7. [PubMed] [Google Scholar]
- 19.Bal CS, Padda B, Puri P. Comparative study to evaluate the efficacy of surgical and conservative techniques for apexification in young permanent teeth with open apices. Indian J Dent Res. 1989;1:102–8. [PubMed] [Google Scholar]