

Abstract
Background:
Systemic sclerosis (SSc) is a chronic, multisystem connective tissue disorder characterized by autoimmune activation, microvascular endothelium damage, and excessive collagen proliferation. The most affected hand presents claw hand deformity and microvascular disease. Deformed hands can cause functional disability and decrease the quality of life. A daily home program can improve mobility of scleroderma patients.
Objective:
We sought to determine the effect of a daily home exercise program on hand mobility among scleroderma patients.
Materials and Methods:
This was a randomized control trial. Twenty-eight participants were divided into two groups, both of which received the same daily home treatment: Group 1 with gloves (n = 14) and Group 2 without gloves (n = 14). The 2-week daily home program combined traditional Thai massage (TTM) with stretching exercises and heat. Hand mobility was assessed using hand mobility in scleroderma (HAMIS). The study was conducted in patients who were already on vasodilator drugs.
Results:
Both groups showed a significant improvement in hand mobility after 2 weeks of daily home exercise program (P < 0.05). Wearing the glove, however, resulted in better thumb mobility.
Conclusions:
A daily home exercise program improved hand mobility among patients with scleroderma and wearing gloves may improve thumb mobility.
Keywords: Glove, systemic sclerosis, stretching exercises, traditional Thai massage, wearing gloves
INTRODUCTION
Systemic sclerosis (SSc) is an autoimmune disease within the scleroderma disease group. Autoimmune overactivation, vascular malfunction, and collagen overproduction are the primary causes of SSc;[1] a multisystem fibrotic disease causing vasculopathy the main complications of which affect the skin, muscles, joints, and internal organs. Musculoskeletal involvement is common among patients with SSc and it is also a main cause of disability.[2] The hands are the most commonly affected part of the body including: Hand deformities, loss of flexion of the metacarpophalangeal joints, loss of extension of the proximal and distal interphalangeal joints, loss of thumb abduction, flexion, and opposition, and loss of wrist motion in all planes resulting in the classic claw-hand deformity. The forearm can be involved in severe cases.
SSc generally results in disfigurement to visible and socially relevant parts of the body (particularly the hands, mouth, and face),[3] resulting in body image dissatisfaction not unlike patients with severe burn injuries.[4,5] Perhaps because deteriorating psychological function and psychological distress erode a person's self-esteem.[6,7] Women with SSc have a lower self-esteem than burn patients with observable deformities,[8,9] as thickening skin is both disabling and cosmetically disconcerting.[10] The typical hand deformations result in functional disability as related to activities in daily living requiring object manipulation, grasping, and pinching.[11] Approximately 90% of patients with SSc confirm the loss of both hand movement and dexterity (gross and fine motor control). Hand deformity, expanded fingers, and decreased wrist extension are the main risk factors leading to hand disability.[12] Hand function is one of the greatest concerns among patients with SSc including: Muscle strength, grasp patterns, precision and accuracy, anatomical integrity, sensation, motivation, coordination and dexterity, unilateral and bilateral tasks, and daily living tasks.[13]
Pharmacological treatments used include: (a) Vasodilators and antiplatelet aggregation drugs to improve peripheral blood circulation, (b) immunosuppressant drugs to prevent the synthesis and release of harmful cytokines, and (c) agents that reduce collagen synthesis to inhibit or reduce fibrosis;[14] while nonpharmacological treatments include manual therapies. Crucially, a hand rehabilitation program is needed for prevention of hand deformity and maintaining quality of life. Recent studies by Vannajak and colleagues reported that traditional Thai massage (TTM) on the upper extremities in patients with SSc can increase hand mobility in the immediate and short-term[15] and increase hand skin temperature for half an hour.[16] Hand exercises—including finger stretching, upper extremity stretching, occupational therapy, and McMennell joint manipulation—have been reported to improve hand function through active exercise (active range of motion) combined with connective tissue massage.[17,18] Both prior studies measured hand mobility in scleroderma (HAMIS) and the test results showed that the use of heating modalities in conjunction with physical therapy improved extensibility of collagen tissue along with tendon and joint capsules;[19] underscoring the importance of superficial heating modalities[20] or thermal glove insulation for keeping the hands warm[21] and increasing extensibility.
Secondary Raynaud's phenomenon (sRP) generally occurs and is serious in SSc when the patient is exposed to cold or to emotional stressors. In a cold environment, and especially in winter, even a small decrease in temperature can aggravate the vasculitis in the hands. In order to maintain good hand function for ADLs, when patients with SSc are exposed to cold the hands need to be protected against heat loss from heat convection and/or direct contact with cold. Wearing gloves is a simple, safe, and easy way to prevent hand heat loss and direct contact with cold.[21] Wearing gloves can decrease local heat transfer of healthy hands in cold conditions.[22]
The objective of this study was to evaluate the short-term effect on hand mobility of thermal insulation gloves in combination with a daily home program (including TTM, stretching, and superficial heating) among patients with SSc.
MATERIALS AND METHODS
This was a randomized control trial conducted with 28 scleroderma (SSc) patients (both males and females) from the Rheumatology Department, Srinagarind Hospital, Khon Kaen University, at the Faculty of Associated Medical Sciences, Khon Kaen University, Thailand. The study was conducted in patients who were already on vasodilator drugs (depending on rheumatologist, i.e. nifedipine), which was administered by rheumatologist, specialist in scleroderma. The study was approved by the Khon Kaen University Ethics Committee for Human Research based on the Declaration of Helsinki and the International Conference on Harmonization ICH Good Clinical Practice Guidelines (Order: 4.2.01: 38/2011, number: HE541337).
Scleroderma patients (diffuse subtype)[15] were recruited to the study, which was conducted in the Thai cool season (December 2012-January 2013). Exclusion criteria were: (a) A history of hand surgery within 6 months, (b) an open wound or ulceration on the hand, (c) loss of tactile and proprioceptive sensation in the hand, (d) diabetes mellitus, (e) smoking, or (f) a psychiatric condition. Participants were asked to sign a consent form after which they were randomly allocated into one of two groups (experimental treatment or control group). Then each was given a HAMIS hand function test[23,24] by a physical therapist.
The experimental group performed the daily home program wearing gloves, while the control group did the program without gloves. Both groups took their routine medication. All of the participants had superficial heat (i.e. warm water ~ 40°C) applied to the hands for 20 min. Then a relative gave TTM to the upper extremities, from the neck to the finger tips, for 30 min (15 min on each side). Seven stretching positions were done following the TTM: (a) forearm supination/pronation, (b) wrist flexion/extension, (c) radial/ulnar deviation, (d) finger abduction/flexion/extension, (e) thumb abduction/adduction, (f) flexion/extension, and (g) thumb opposition [Figure 1]. Patients began by gradually stretching to the point of resistance, then holding for 30 seconds. They repeated this four times on each side, once a day, for 2 weeks. (Patients did the stretching independently after instruction and supervision by the physical therapist.) Next, the patients in the glove group put on the gloves for 6 h per day.
Figure 1.
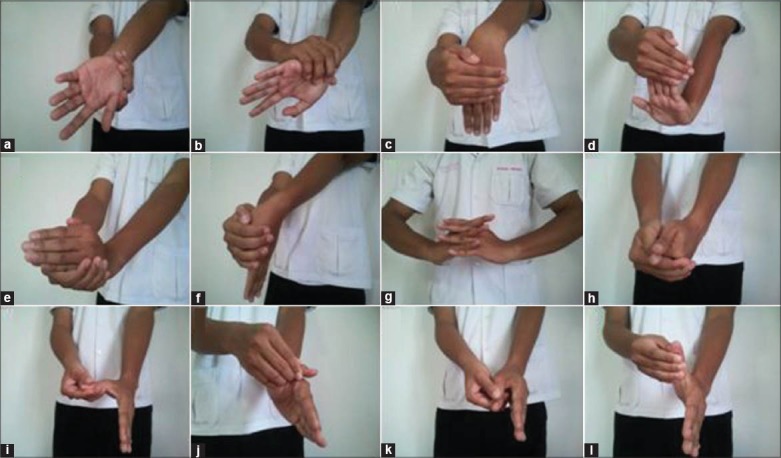
Stretching exercise in daily home program, (a) Forearm supination, (b) Forearm pronation, (c) Wrist flexion, (d) Wrist and finger extension, (e) Wrist radial deviation, (f) Wrist ulnar deviation, (g) Finger abduction, (h) Finger flexion, (i) Thumb abduction, (j) Thumb adduction, (k) Thumb flexion, and (l) Thumb extension
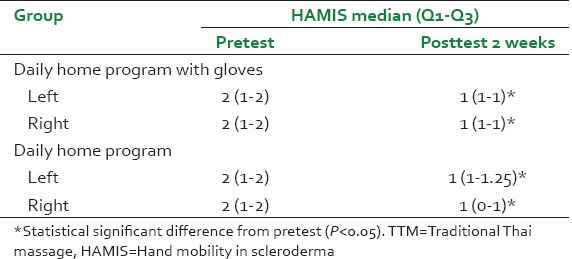
Data for HAMIS was collected and expressed as a median: (Q1–Q3). Any significant difference between the daily home program with gloves and without after 2 weeks of treatment was determined using Mann-Whitney U test. Differences between the groups would be considered significant at a P < 0.05 [Figures 2 and 3].
Figure 2.
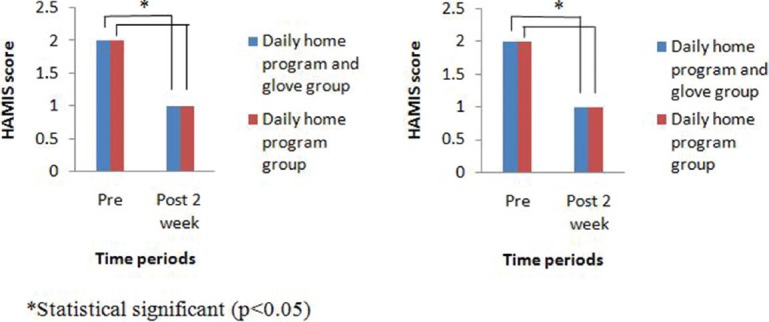
Change in left and right hand mobility after 2 weeks of daily home program
Figure 3.
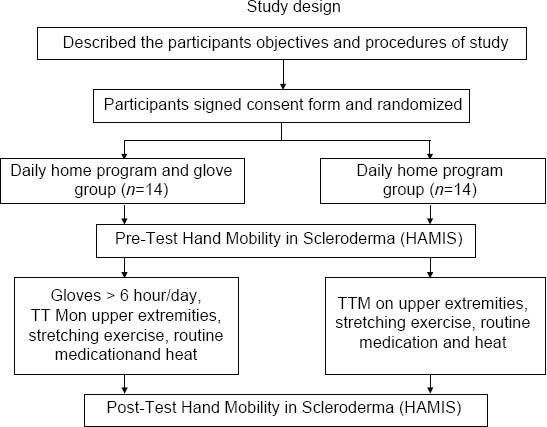
Flow chart of the study
RESULTS
The study had 28 participants: The glove-wearing group (nine females; five males) and daily home program group (four females; 10 males). The diagnosis was the diffuse, cutaneous systemic sclerosis (dcSSc) subtype in the indurative phase. The modified Rodnan skin thickness score (MRSS) was 1-2 at the dorsum of the forearm, hand and between 3 and 6 at the proximal phalange of the 3rd finger (0 = normal skin thickness, 1 = mild, 2 = moderate, and 3 = severe). HAMIS[23] is a performance index comprising nine items normally constituting in an ordinary range of motion (a score between 9 and 18 reflects a high degree of deformity).[24] Patients had good consciousness and were cooperative. Baseline characteristics of participants are presented in Table 1, while changes in hand mobility after the 2 week study is shown in Table 2 and Figure 1.
Table 1.
Baseline characteristic of patients with SSc
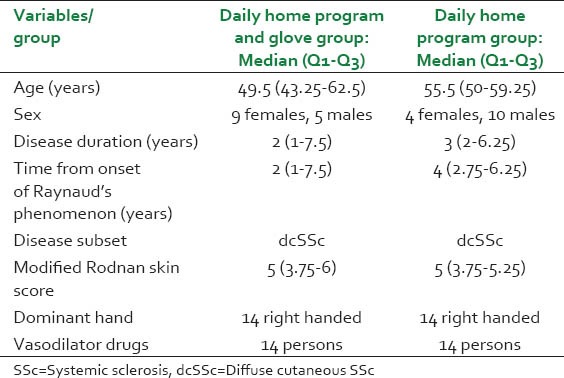
Table 2.
Hand mobility in scleroderma patients’ change after gloving in combination with TTM
DISCUSSION
Prevention of hand deformity is a core goal and is one reason for the need for physical therapy. The aim of the current study was to compare the therapeutic effect between a daily home program with and without thermal insulation (wearing gloves) as measured by hand mobility (HAMIS). Accordingly, wearing gloves as part of the daily home program represented a benefit viz-à-viz hand mobility. Vannajak and colleagues reported that TTM also aids with hand mobility among patients with SSc.[15] Although their study did not include any stretching exercise because they were focused on isolating the effect of TTM on hand mobility, other studies used TTM augmented by daily home programs with heat[19] and/or stretches[10] appropriate to the individual's condition, disease stage, and expectation for improvement of hand mobility in the indurative phase. Wearing gloves in combination with TTM and a daily home program may be particularly useful in winter.[21] The combination of TTM + heat + stretching produced a synergistic therapeutic effect.
In the current study, the gloves were made of nylon fabric, selected because of the results of a previous in vitro study about the characteristics of material and insulation properties. The aim was increased blood circulation, optimal hand temperature, and hand flexibility. After the 2 weeks of routine treatment there was no difference between the two groups in mobility, on the basis of TTM and stretching alone, but wearing gloves plus the other treatments clearly improved finger flexion, finger extension, thumb abduction, and pincer grip aspects. Improvements in finger and thumb movement are important for hand function in daily living. Even though the median HAMIS score was equal between groups, wearing gloves in combination with TTM and the daily home program was a better method. In winter, gloves provide protection from exposure to cold which aggravates severe sRP in SSc. If an sRP attack is not prevented, vascular permeability and vasospasm will result in sclerosis of vascular, severe pain, and disturbed daily living.[25] The daily home program in our study indicated an increase in hand mobility among patients with SSc, which agrees with a previous study on active range of motion[17] and another on individual rehabilitation programs.[18]
Vannajak and colleagues demonstrated that TTM can increase hand skin temperature[16] and hand mobility in both the immediate and short-term.[15]
The results of the current study underscore that primary self-care by hand exercise is beneficial in increasing hand mobility which leads to improved quality of life among patients with SSc, and is especially effective when combined with manual therapy and wearing gloves to prevent cold exposure leading to sRP.[21]
A limitation of this study was its short duration; notwithstanding, the results indicate a measurable benefit for the group wearing gloves with the daily home program. Further study will be conducted on microvascular structure alteration with a longer duration follow-up.
CONCLUSION
After 2 weeks, the daily home program helped to improve hand mobility among patients with SSc. The study was conducted in patients who were already on vasodilator drugs. Wearing gloves in combination with daily stretching and heat significantly improved hand mobility. Wearing gloves in combination with the daily home exercises was effective, safe, and led to increased self-esteem. The quality of life score among patients with SSc also improved as a result of increased hand mobility. The suggestion was larger sample size and longer duration of study is desired to further confirm these observations. Finally, wearing gloves in combination with TTM, heat, and stretching may help to improve hand mobility among patients with scleroderma.
ACKNOWLEDGMENTS
The authors thank (a) the patients and families for their participation, (b) the nursing and physiotherapy staff, and (c) Mr. Bryan Roderick Hamman and Mrs. Janice Loewen-Hamman for assistance with the English language presentation and Ms. Jackie Hall for help with revision.
Financial support for this study was provided by the Research and Training Center for Enhancing Quality of Life of Working Age People, Faculty of Nursing, Khon Kaen University, Thailand.
Footnotes
Source of Support: The Research and Training Center for Enhancing Quality of Life of Working Age People, Faculty of Nursing, Khon Kaen University, Thailand.
Conflict of Interest: None declared.
REFERENCES
- 1.Black CM, Denton CP. Scleroderma and related disorders in adults and children. In: Isenberg DA, Maddison PJ, Woo P, Glass D, Breedveld FC, editors. Oxford Textbook of Rheumatology. 3rd ed. Oxford: Oxford University Press; 2004. pp. 872–95. [Google Scholar]
- 2.Randone SB, Guiducci S, Cerinic MM. Musculoskeletal involvement in systemic sclerosis. Best Pract Res Clin Rheumatol. 2008;22:339–50. doi: 10.1016/j.berh.2008.01.008. [DOI] [PubMed] [Google Scholar]
- 3.Joachim G, Acorn S. Life with a rare chronic disease: The scleroderma experience. J Adv Nurs. 2003;42:598–606. doi: 10.1046/j.1365-2648.2003.02663.x. [DOI] [PubMed] [Google Scholar]
- 4.Benrud-Larson LM, Heinberg LJ, Boling C, Reed J, White B, Wigley FM. Body image dissatisfaction among women with scleroderma: Extent and relationship to psychosocial function. Health Psychol. 2003;22:130–9. [PubMed] [Google Scholar]
- 5.Paquette DL, Falanga V. Cutaneous concerns of scleroderma patients. J Dermatol. 2003;30:438–43. doi: 10.1111/j.1346-8138.2003.tb00413.x. [DOI] [PubMed] [Google Scholar]
- 6.Heatherton TF, Polivy J. Development and validation of a scale for measuring state self-esteem. J Pers Soc Psychol. 1991;60:895–910. [Google Scholar]
- 7.Vamos M. Body image in chronic illness-A reconceptualization. Int J Psychiatry Med. 1993;23:163–78. doi: 10.2190/BLL4-EVAL-49Y3-4G66. [DOI] [PubMed] [Google Scholar]
- 8.Haythornthwaite JA, Heinberg LJ, McGuire L. Psychological factors in scleroderma. Rheum Dis Clin North Am. 2003;29:427–39. doi: 10.1016/s0889-857x(03)00020-6. [DOI] [PubMed] [Google Scholar]
- 9.Malcarne VL, Hansdottir I, Greenbergs HL. Appearance self-esteem in systemic sclerosis. Cognit Ther Res. 1999;23:197–208. [Google Scholar]
- 10.Nalebuff EA. Surgery in patients with systemic sclerosis of the hand. Clin Orthop Relat Res. 1999;366:91–7. doi: 10.1097/00003086-199909000-00012. [DOI] [PubMed] [Google Scholar]
- 11.Silman A, Akesson A, Newman J, Henricksson H, Sandquist G, Nihill M, et al. Assessment of functional ability in patients with scleroderma: A proposed new disability assessment instrument. J Rheumatol. 1998;25:79–83. [PubMed] [Google Scholar]
- 12.Poole JL, Watzlaf VJ, D’Amico F. Hand risk factors for development of disability in scleroderma. Arthritis Rheum. 1996;39:312. [Google Scholar]
- 13.McPhee SD. Functional hand evaluations: A review. Am J Occup Ther. 1987;41:158–63. doi: 10.5014/ajot.41.3.158. [DOI] [PubMed] [Google Scholar]
- 14.Sapadin AN, Fleischmajer R. Treatment of scleroderma. Arch Dermatol. 2002;138:99–105. doi: 10.1001/archderm.138.1.99. [DOI] [PubMed] [Google Scholar]
- 15.Vannajak K, Boonprakob Y, Nanagara R. The immediate and short term effects of Traditional Thai Massage on alteration of skin temperature and hand mobility in Scleroderma patients. Thai J Phys Ther. 2010;32:81–9. [Google Scholar]
- 16.Vananjak K, Boonprakob Y, Nanagara R. The immediate effects of traditional Thai massage on alteration of skin temperature and hand mobility in scleroderma patients: A preliminary study. J Med Technol Phys Ther. 2010;22:92–102. [Google Scholar]
- 17.Bongi SM, Del Rosso A, Galluccio F, Sigismondi F, Miniati I, Conforti ML, et al. Efficacy of connective tissue massage and Mc Mennell joint manipulation in the rehabilitative treatment of the hands in systemic sclerosis. Clin Rheumatol. 2009;28:1167–73. doi: 10.1007/s10067-009-1216-x. [DOI] [PubMed] [Google Scholar]
- 18.Antonioli CM, Bua G, Frigè A, Prandini K, Radici S, Scarsi M, et al. An individualized rehabilitation program in patients with systemic sclerosis may improve quality of life and hand mobility. Clin Rheumatol. 2009;28:159–65. doi: 10.1007/s10067-008-1006-x. [DOI] [PubMed] [Google Scholar]
- 19.Mancuso T, Poole JL. The effect of paraffin and exercise on hand function in persons with scleroderma: A series of single case studies. J Hand Ther. 2009;22:71–7. doi: 10.1016/j.jht.2008.06.009. [DOI] [PubMed] [Google Scholar]
- 20.Lehmann SF, Masock AJ, Warren CG, Koblanski JN. Effect of therapeutic temperatures on tendon extensibility. Arch Phys Med Rehabil. 1970;51:481–7. [PubMed] [Google Scholar]
- 21.Vannajak K, Boonprakob Y, Nanagara R, Eungpinich pong W. Thermal insulation character of fabric glove: The immediate and sustain effects of paraffin bath on alteration of skin temperature and hand mobility in scleroderma patients: A preliminary study. J Med Tech Phy Ther. 2013;25:76–86. [Google Scholar]
- 22.Sari H, Gartner M, Hoeft A, Candas V. Glove thermal insulation: Local heat transfer measures and relevance. Eur J Appl Physiol. 2004;92:702–5. doi: 10.1007/s00421-004-1136-z. [DOI] [PubMed] [Google Scholar]
- 23.Sandqvist G, Eklund M. Hand mobility in scleroderma (HAMIS) test: The reliability of a novel hand function test. Arthritis Care Res. 2000;13:369–74. [PubMed] [Google Scholar]
- 24.Sandqvist G, Eklund M. Validity of HAMIS: A test of hand mobility in scleroderma. Arthritis Care Res. 2000;13:382–7. [PubMed] [Google Scholar]
- 25.Sunderkotter C, Riemekasten G. Pathophysiology and clinical consequences of Raynaud's phenomenon related to systemic sclerosis. Rheumatology (Oxford) 2006;45(Suppl 3):iii33–5. doi: 10.1093/rheumatology/kel280. [DOI] [PubMed] [Google Scholar]