

Abstract
This paper serves to provide a background for the topic of comorbidity than extends through this issue. Comorbidity is common within developmental disorders. It is shown that there are many possible reasons for comorbidity. Some of these can be viewed as artifacts as simple as chance occurrence or because of the way that the research participants were sampled. If these artifacts are eliminated, then comorbidity can be informative with respect to possible causes of the disorders that are comorbid. Several possible etiologic models are presented along with a general framework for considering levels of causality in developmental disorders.
Many speech-language clinicians working with children will experience a caseload in which children exhibit combinations of speech disorders (SD), language impairment (LI) and reading disorder (RD). Numerous studies have shown RD is substantially elevated among children with LI (see for instance: Bishop & Adams, 1990; Beitchman, Wilson, Brownlie, Walters, & et al., 1996; Catts, 1993; Catts, Fey, Tomblin, & Zhang, 2003; Silva, Williams, & McGee, 1987). Likewise, poor readers are likely to have poor language abilities (Bradley & Bryant, 1983; Catts, 1989; Lombardino, Riccio, Hynd, & Pinherio, 1997; Vellutino, Scanlon, Small, & Tanzman, 1991). SD and LI are found together (Shriberg, Tomblin, & McSweeny, 1999; Beitchman, Nair, Clegg, & Patel, 1986), as are SD and RD. It has recently been shown that co-occurrence of the latter two disorders is in fact due to the elevated rate of LI among children with SD, a finding which points to the complexity of the relationship between these disorders (Pennington & Bishop, 2009). Lastly, it is not uncommon to find that children with LI, SD, or RD are also being treated for attention-deficit hyperactivity disorder (ADHD) (Beitchman, Nair, Clegg, Ferguson, & al., 1986; Baker & Cantwell, 1992; Benasich, Curtiss, & Tallal, 1993; Coster, Goorhuis-Brouwer, Nakken, & Spelberg, 1999; 2007; Noterdaeme & Amorosa, 1999; Tomblin, Zhang, & Buckwalter, 2000).
This phenomenon occurs so frequently it has led to a general acceptance of the overlap between communication disorders and behavior disorders. In the health sciences, however, disease overlap, that is, comorbidity has been explored for the insight it can yield into the underpinnings of disease states and, in turn, the validity of diagnostic systems. In this series of articles in this issue we argue that by examining patterns of comorbidity among ADHD, LI, RD and SD, as well as the basis for these patterns, we are led to a deeper understanding of these disorders. In particular, we are forced to think about the relationships between features that exist at the symptom level – that which we term the ‘phenotype’ – and the underlying systems that are associated with, or perhaps even causal for these symptoms. Figure 1 depicts this layered structure of causality for LI, SD, RD (which will collectively be termed ‘communication disorders’) and ADHD. We can think of these causal systems on a continuum, ranging from those that are closest to the symptom level, down to those that are most distant. In a recent paper we presented such a model for LI (Tomblin & Christiansen, 2010). The continuum of causal systems was conceptualized as a hierarchy of layers beginning with genetics (the most distal point) and ending in cognitive systems (the most proximate), with brain systems lying in between, and the environment acting upon these systems. Note in our conceptualization, environmental factors could act on genes, brain systems, or cognitive systems. Figure 1 shows how that the same underlying systems can provide an explanation not only for the symptoms of one disorder, such as LI, but also for the comorbidity that exists between disorders.
Figure 1.
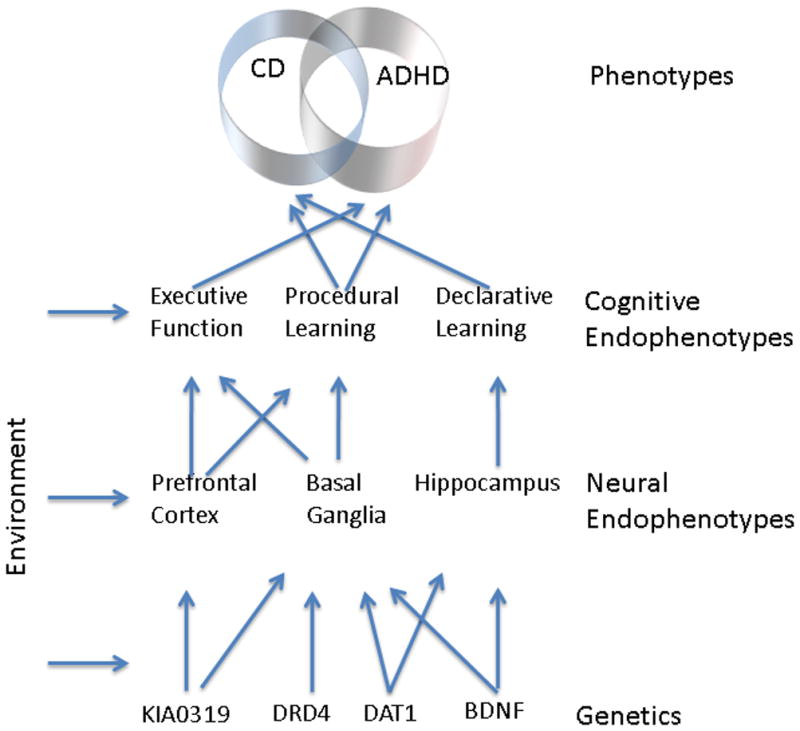
A hypothetical etiological scheme demonstrating shared etiologies at multiple levels resulting in comorbidity.
This conceptualization of a continuum of systems is also found in genetics. Here, the intermediate systems that link distal genetic factors to proximal phenotypic symptoms are termed endophenotypes (Gottesman & Gould, 2003). According to Gottesman and Gould, this term originated in a paper by John and Lewis (1966), and was first used to refer to the aspects of a phenotype that are not directly observable. This term later became applied to psychiatric disease where endophenotypes were used to identify intermediate systems that were influenced by genes and giving rise to clinical phenotypes. Thus, in this context, an endophenotype is an intermediate phenotype that lies between the etiology of a clinical disorder and the genes that confer susceptibility to the condition. Because endophenotypes influence the phenotype, we can also consider them to be risk factors when the phenotype is viewed as a disease or health condition. In this regard, endophenotypes are a useful tool for understanding the etiology of complex disorders in which several risk genes and environmental risk factors influence the phenotype. It is quite reasonable to propose, therefore, that they could also be used to further our understanding of comorbidity. In fact, in cases when disorders share common symptoms, or phenotypes, it is arguable they may provide a clearer picture of the basis of comorbidity than the symptoms themselves. This type of thinking underlies much of the material in this issue. In adopting this approach, we are able to consider the multiple different ways in which comorbidity can occur. We will consider the different ways in which the symptoms of comorbid disorders could be related, both between disorders, as well as to underlying risk factors. To do this, we will present various models of comorbidty and evaluate these within the context of current research on LI, SD, RD, and ADHD.
Models of Comorbidity
As we noted previously, the observation that LI, SD, RD and ADHD cluster together is not unusual. Clinical conditions of all sorts tend to cluster together, or co-occur. Events that are unrelated may also happen together, by chance. Take two unrelated events, the probability of rain and the probability of winning the lottery. These could occur with the probability of .15 and .005 respectively. The probability they will occur together is the product of these probabilities (0.00075). Although highly unlikely, this example illustrates that all instances of co-occurrence should be taken as evidence of some important relationship. In fact, the Nobel Laurette, Murray Gell-Mann stated with respect to particle physics, that “everything not forbidden is compulsory.” Thus, given enough time anything that can happen will happen. While such chance occurrences may be useful in particle physics, this type of joint appearance is not what we wish to understand and therefore we will be talking about the case of true comorbidity in which there is a reason for this joint occurrence.
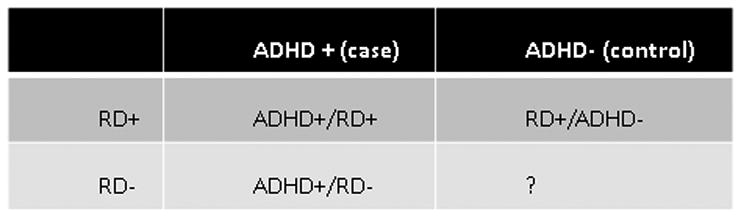
Even when joint occurrence is ruled out, there are many possible reasons for why this may be so, and each must be considered before drawing conclusions regarding comorbidity. Several papers on models of comorbidity have been published, each providing a rather lengthy list of the reasons why we might observe overlaps(seemingly) distinct disorders (Caron & Rutter, 1991; Klein & Riso, 1993; Neale & Kendler, 1995). We have summarized these in eight models, as shown in Table 1. The first two these models represent biases in methodology, which result in a picture of disease overlap that is not an accurate representation of the overlap in the general population. Thus, these may be viewed as examples of erroneous patterns of comorbidity. . Model 1 depicts the situation in which the study of comorbidity in patient populations leads to an overestimation of the relationship between disorders because children without disorders have not been factored into the model (i.e. we do not know what the rate of individuals without either of the two conditions are in the general population). This phenomenon is known as Berkson's bias. For instance if we were to examine the rate of LI and ADHD in a seen in a clinic that largely was comprised of children with RD or ADHD we would lack an accurate estimate of the proportion of children in the population without either. This is shown in Figure 2. We would argue that the Berkson bias underscores the importance of the control sample. Convienence samples of controls could either underestimate or overestimate the rate of RD shown in Figure 2. Often a patient population without the primary disorder ADHD, but with some other condition, is used to serve as a control population. We know, however, that children with comorbid conditions are more likely to be clinically served and thus this practice would elevate the estimate of comorbidty and explains why clinicians frequently perceive the conditions they treat as comorbid. To avoid this bias, it is best to study comorbidity in whole population samples, as opposed to clinical ones.
Table 1. Models of Comorbidity.
| Model | Description | |
|---|---|---|
| 1 | Sampling bias | Subjects with two disorders (A and B) are more likely to be sampled as part of clinical populations (e.g. Berkson's bias) |
| 2 | Method bias | Co-occurrence of A and B is due to overlap in operational definition or measurement |
| 3 | By-Product | Presence of disorder A markedly increases risk for disorder B (or vice versa) |
| 4 | Three independent etiology | Disorders A, B and AB have independent risk factors, but shared symptoms. |
| 5 | Alternate forms | A and B have the same underlying etiologic basis, but random or additional factors tip expression toward A or B |
| 6 | Correlated liabilities | Risk factors for disorders A and B are correlated |
| 7 | Reciprocal causation | Risk factors for A and B influence one another |
| 8 | Causal model | The presence of risk factors for disorder A is necessary and sufficient to cause disorder B |
|
|
||
Figure 2. A four-fold table used to compare comorbidity of RD in ADHD.
A second kind of bias that can give a false impression of comorbidity may arise when methods employed in diagnosis overlap between disorders (Model 2). This may be symptom overlap: for example, depression, shyness, and anxiety are distinct disorders, but social reticence is a common feature to all. Failure to note this could result in an overestimation of the overlap between the disorders. Another example is when a common instrument is used in diagnosis of both disorders. Pennington, Willcutt & Rhee (2005) describe the example of rater bias when the same rater (for example, a parent) provides information that will be used in the diagnosis of ADHD and conduct disorder (CD). Along with chance, Models 1 and 2 are said to be artifactual sources of comorbidity.
If the overlap between disorders is non-random, and cannot be attributed to biases in sampling or diagnostic criteria, this co-occurrence is considered to represent true comorbidity (Caron & Rutter, 1991; First, 2005). Models 3-8 in Table 1 are examples of this. Neale and Kendler have argued that the “co-occurrence of disorders [is] one of today's most important areas for methodological and substantive research (p.935)”. The significance of this stems from the fact that the overlap of symptoms between disorders should provide a small set of possible explanations for the basis of comorbidty, many of which bear on the etiology and diagnostic classification of complex disorders. Models 3-8 can be further subdivided into 1) models that attribute the basis of comorbidity to the relationship of interactions between symptoms at the phenotype level or to assume that the comorbid condition is a blend of the two rather than being a third distinct conditions and 2) models that attribute comorbidity to common etiology or risk factors that are somehow shared between the comorbid conditions.
An example of the first subgroup (symptom level) is seen in Model 3, where two conditions, each with their own separate etiology, are related because the symptoms one condition increases the likelihood of symptoms in the other, as depicted in panel A of Figure 3. In this model the basis of the comorbidity is at the symptom level only. An example of this, which pertains to the study of ADHD, would be when poor communication abilities cause a child to be inattentive in the classroom. It is possible that the attention problems are symptomatic of ADHD and arise from a separate cause, but the communication deficits increase the risk for inattentive behaviors. In Model 4 (Panel B, Figure 3), the combined form of ADHD and comorbid disorder (CD) has an etiology that is distinct from either ADHD or the CD alone. This kind of presentation is common to syndromes, where the constellations of symptoms that define the disorder are shared by other disorders. For example, Usher Syndrome shares features of sensori-neural hearing loss (SNHL) and blindness common to other disorders of either blindness or SNHL, but the syndrome has a different etiology to disorders in which SNHL and blindness occur in isolation.
Figure 3.
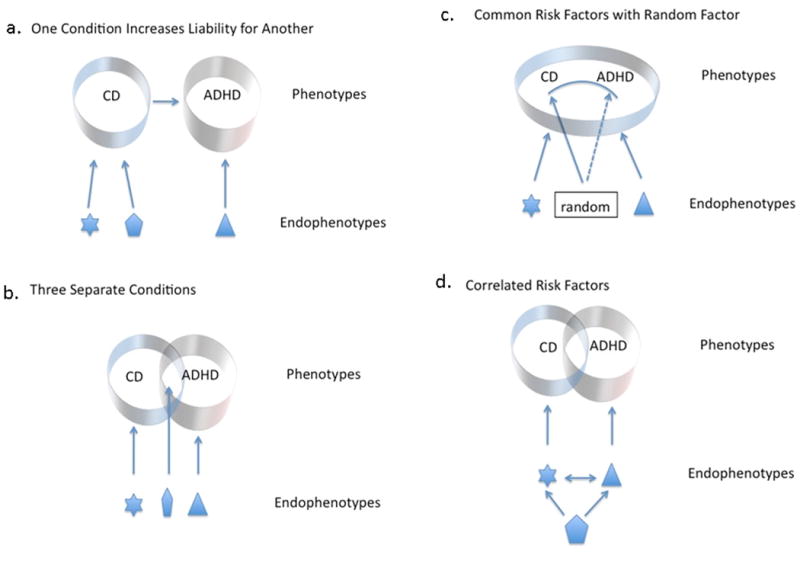
Models of comorbidity that arise from different configurations of etiologic sources. (A) A relationship in which the comorbidity is due to the influence of communication disorder (CD) on attention-deficit/hyperactivity disorder (ADHD). (B) A relationship in which the comorbid condition has a different etiology than the simple forms. (C) CD and ADHD have the same causes but a random or perhaps third factor determines whether it is realized as CD or ADHD. (D) CD and ADHD have different endophenotypes but these are themselves correlated.
In contrast, Models Five through Eight of comorbidity all involve shared etiology, or risk factors, as depicted in the bottom panel of Figure 2. Model Five is the simplest example: here, ADHD and CD essentially represent the same disorder, but other unknown or random factors tip the overall expression of symptoms so that, overall, the disorder appears as ADHD or CD. Models Six, Seven and Eight assume that there are separate risk factors for ADHD and CD; however, the underlying endophenotypes for the disorders are either correlated, or directly act upon one another, resulting in the co-occurrence of the symptoms.
As we examine these different models, we should begin to see how careful study of comorbidity can help us evaluate the validity of current diagnostic thinking. While we frequently talk about a disorder as a distinct diagnosis (e.g. A or B), most of the time we are in fact only hypothesizing this. In some cases, it might be better to think of disorders A and B as basically one in the same, as is the case in Models 5 and 6. Models 3 and 4, on the other hand, posit a clear distinction between conditions. From this, it should also be evident why careful thought about the nature of comorbidity is an essential part of clinical research. In the pages that follow in this issue, we will be examining the data on the comorbidity of ADHD with LI, SD, and RD, to determine how we might best characterize these diagnostic categories.
We should also begin to see how it is that research on the etiology and risk factors of developmental disorders is an important part of understanding these disorders. The discovery that two disorders, each distinctly defined, in fact have shared risk factors has far-reaching implications for how we should be conceptualizing developmental disorders. For example, there has been considerable controversy with regard to the relationship between specific language impairment (SLI) and autism spectrum disorders (ASD). Some researchers have hypothesized these two conditions are somewhat comorbid (Kjelgaard & Tager-Flusberg, 2001; Kjelgaard & Tager-Flusberg, 2001), probably within the framework of Models 5-7. Others (Whitehouse, Barry, & Bishop, 2007; Whitehouse, Barry, & Bishop, 2008; Williams, Botting, & Boucher, 2008) have argued comorbidity between these disorders follows the paradigm laid out in Model 3, wherein the presence of ASD results in SLI-like symptoms. Note the issue here is really whether there are shared etiology or risk factors common to ASD and SLI. Most of the data brought into this debate, however, is at the symptom level. More recently, however, a series of studies have shown that genetic variation in a single gene (CNTNAP2) is a risk factor for both ASD (Bakkaloglu et al., 2008; Alarcon et al., 2008; Arking et al., 2008) and SLI (Vernes et al., 2008). These findings need to be replicated, but if they hold, they provide evidence that any model of comorbidity in ASD and SLI must assume a shared risk/etiology (i.e. Models 5, 6, or 7). Most importantly these data show how efforts to examine comorbidity and, in particular, the use of genetics in this effort, should aid our understanding on the nature of developmental disorders in general, and developmental communication disorders in particular.
Ways that Genetic Research Methods can Aid the Study of Comorbidity
In the different models of comorbidity discussed above the notion of risk factor was treated in a generic fashion. In Figure 1 we showed a multilevel perspective on the etiologies of developmental disorders and from this we can see that a risk factor that could be contributing to comorbidity can be studied and understood at these different levels. In the past 20 years, the level of genetics has been a point of focus for the study of comorbidity of complex behavioral disorders. There are no doubt many reasons for this; however, we believe that there is merit in this largely because genetic influence must flow upward through the higher levels of the causal system. However, we also know that the higher levels in this system can flow downward to influence the expression of genetic information. For instance, neural activity at a synapse can result in a cascade of molecular messages that move to the cell nucleus and trigger expression of genes that code for proteins important for learning (Naeve, Ramakrishnan, Kramer, Hevroni, Citri & Theill, 1997). In this regard we can move from higher levels of the system to generate hypotheses about genetics or we can move from genetics to generate hypotheses regarding the pathways of genetic influence. In this respect, we are not assuming that genes are particularly privileged in this account and in fact, as with any scientific account, the value in understanding a complex system as depicted in Figure 1 will come from understanding the interactions within and across the levels. In this regard, when we begin to study the genetic contribution to a phenotype we cannot limit ourselves to DNA alone. Any genetic account will quickly take the investigator through the whole system. Genetics does offer a point of entry into this system that comes with a very rapidly advancing scientific knowledge base as well as methods of inquiry that improve by the year. As we will show below, with this growth comes an ever increasing understanding of the complexity of even this one level.
In the papers that follow, genetic research will be discussed as it has been used to understand the comorbidity of speech, language, reading disorders and ADHD. This is not surprising given that each of these conditions has been shown to be heritable (genetically influenced). When the two comorbid conditions are each heritable, we can begin to ask whether the two disorders share common genetic risk factors. Indeed, we believe that asking this question can be useful in helping us better understand each disorder as well as the basis for the comorbidity. In asking this question we need to place this question into a context of contemporary genetic research. The naïve view of genetics is that, as the name implies, genes are the ultimate cause of development. That is, that many things about us begin with the genes that we inherited from our parents. Furthermore, when we finally understand genetics, we will have a dictionary that lists genes and the traits that they control. Thus, there will be a tidy description that says that gene X is responsible for trait X. For example the androgen receptor gene (AR) is associated with male pattern baldness.. If you have one form of this gene and are male, you will very likely have a pattern of hair loss in adulthood. So we could say that male pattern baldness is the phenotype and the AR gene could be thought of as a gene for male pattern baldness. This is often how genes are characterized and it makes for easy communication, but the thinking that goes into this contains some traps that can mislead us.
An important way we are misled concerns how this view treats genetic effects. The simple account of male pattern baldness we just described suggests that for each phenotype we could expect to find a responsible gene. In fact, there are a number of examples of this rather simple relationship that can be described as single gene effects. However, even in cases such as the AR gene, this gene does not just influence baldness, there are number of other traits influenced by this gene. This observation that genes can influence more than one trait is captured in the term pleiotropy. In fact, pleiotropy at some level is a rule in genetics (Stearns, 2010). Genes are reused for a variety of phenotypic effects even when the phenotypes are relatively simple such as in the case of hair loss. Pleitropy is an essential way that a rather limited information system such as the DNA code can result in a vast and complex array of biologic form and function. Thus, given the ubiquity of pleitropy, we should not be surprised to see shared genetic influence across what appear to be different phenotypes or different disorders, thus resulting in patterns of phenotypic correlations that could be viewed as comorbidity.
Pleitropy reflects a one-to- many relationship between a gene and multiple phenotypes.. There other ways in which we can observe shared genetic influence on phenotypes. The kinds of phenotypes we are interested in such as speech, language, reading or ADHD must involve complex neurobiological processes that entail many genetically influenced activities. Thus, we have to consider that these traits arise from the influence of many genes. Such traits are described as complex or polygenic and these can be described as having a many-to-one relationship between the phenotype and the underlying genes (see Figure 1). Let's assume that the phenotype in this case is a person's height as an adult. We just noted that pleiotropy is essentially a universal feature of genetics and therefore these many-to-one relationships are likely to form many-to-many relationships. These would quite easily allow for phenotypes to be correlated resulting in patterns of comorbidity, but at the same time allowing partial overlap.
The many-to-many relationships between genes and phenotypes provide for considerable opportunities for comorbidity, but there is also another important source of complexity in genetics that could be the basis for phenotypic overlap. Most genes code for amino acids that form proteins. A common form of genetic variation is for the amino acid sequence coded by the gene to vary with respect to one or more amino acids. This difference in amino acid content can in some cases result in the protein functioning differently. We can think of this as genetic variation that results in different flavors of a kind of protein. Some of these proteins result in cellular and extracellular structure and function (making muscles, bones etc.). The AR gene mentioned earlier is of this type. Another subset of these proteins returns to the nucleus and acts on other genes by controlling their expression. This kind of action is a regulatory action and the genes that produce these proteins are called regulatory genes. The manner in which these regulatory mechanisms work with regard to the phenotype can be more subtle than the structural genes in that these regulatory genes can control the amount and timing of gene expression of the structural genes that they influence.. This gene interaction is called epistasis.
We should see from this that even when we limit ourselves to genetic risk factors, there are many ways in which phenotypes can be correlated. In fact, so long as the phenotypes are genetically influenced, it would be surprising to find that phenotypes that are not comorbid to some degree. We will certainly see, in the subsequent papers, that comorbidity is indeed more the rule than the exception with regard to common developmental disorders. By acknowledging this pattern of co-occurrence, we are acknowledging the complexity that exists both on the surface and among the underlying systems.
Conclusions
We have argued here that comorbdity has the potential to provide insights into the nature and in particular the causal pathways that lead to developmental disorders. Among developmental disorders these pathways are often long and complex. This requires that those who attempt to understand developmental disorders need to respect this complexity, but at the same time not be daunted by it. By exploiting the pervasive comorbidty among developmental disorders we are able to capitalize and extend progress in research on one disorder to those that are comorbid with it. It is this promise that underlies the thinking in the papers to follow. As will be shown in the following paper that we also coauthor (Mueller & Tomblin, this issue), there has been a substantial amount of research on ADHD. Although it is not possible to claim that ADHD is understood, this developmental disorder is one of the few where the cognitive endophenotypes are extensively studied and to some extent linked to underlying neurobiologial systems. We would contend that an important question is whether this understanding can aid in our understanding of SD as discussed in the paper by Lewis and colleagues, LI as we will discuss and RD as considered in the paper in this issue by Boada and colleagues.
Acknowledgments
This research was supported by grants DC00496 and DC02746 the National Institutes of Health, National Institute on Deafness and Other Communication Disorders, Grant
Reference List
- Alarcon M, Abrahams BS, Stone JL, Duvall JA, Perederiy JV, Bomar JM, et al. Linkage, association, and gene-expression analyses identify CNTNAP2 as an autism-susceptibility gene. Am J Hum Genet. 2008;82:150–159. doi: 10.1016/j.ajhg.2007.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arking DE, Cutler DJ, Brune CW, Teslovich TM, West K, Ikeda M, et al. A common genetic variant in the neurexin superfamily member CNTNAP2 increases familial risk of autism. Am J Hum Genet. 2008;82:160–164. doi: 10.1016/j.ajhg.2007.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baker L, Cantwell DP. Attention deficit disorder and speech/language disorders. Comprehensive Mental Health Care. 1992;2:3–16. [Google Scholar]
- Bakkaloglu B, O'Roak BJ, Louvi A, Gupta AR, Abelson JF, Morgan TM, et al. Molecular cytogenetic analysis and resequencing of contactin associated protein-like 2 in autism spectrum disorders. Am J Hum Genet. 2008;82:165–173. doi: 10.1016/j.ajhg.2007.09.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beitchman JH, Nair R, Clegg M, Ferguson B, al e. Prevalence of psychiatric disorders in children with speech and language disorders. Journal of the American Academy of Child Psychiatry. 1986;25:528–535. doi: 10.1016/s0002-7138(10)60013-1. [DOI] [PubMed] [Google Scholar]
- Beitchman JH, Nair R, Clegg M, Patel PG. Prevalence of speech and language disorders in 5-year-old kindergarten children in the Ottawa-Carleton region. Journal of Speech and Hearing Disorders. 1986;51:98–110. doi: 10.1044/jshd.5102.98. [DOI] [PubMed] [Google Scholar]
- Beitchman JH, Wilson B, Brownlie EB, Walters H, et al. Long-term consistency in speech/language profiles: I. Developmental and academic outcomes. Journal of the American Academy of Child & Adolescent Psychiatry. 1996;35:804–814. doi: 10.1097/00004583-199606000-00021. [DOI] [PubMed] [Google Scholar]
- Benasich AA, Curtiss S, Tallal P. Language, learning, and behavioral disturbances in childhood: a longitudinal perspective. Journal of the American Academy of Child and Adolescent Psychiatry. 1993;32:585–594. doi: 10.1097/00004583-199305000-00015. [DOI] [PubMed] [Google Scholar]
- Bishop DVM, Adams C. A prospective study of the relationship between specific language impairment, phonological disorders and reading retardation. Journal of Child Psychology and Psychiatry and Allied Disciplines. 1990;31:1027–1050. doi: 10.1111/j.1469-7610.1990.tb00844.x. [DOI] [PubMed] [Google Scholar]
- Bradley L, Bryant P. Categorizing sounds and learning to read: A causal connection. Nature. 1983;30:419–421. [Google Scholar]
- Caron C, Rutter M. Comorbidity in child psychopathology: Concepts, issues and research strategies. Journal of Child Psychology & Psychiatry & Allied Disciplines. 1991;32:1063–1080. doi: 10.1111/j.1469-7610.1991.tb00350.x. [DOI] [PubMed] [Google Scholar]
- Catts HW. Defining dyslexia as a developmental language disorder. Annals of Dyslexia. 1989;39:50. doi: 10.1007/BF02656900. [DOI] [PubMed] [Google Scholar]
- Catts HW. The relationship between speech-language impairments and reading disabilities. Journal of Speech & Hearing Research. 1993;36:948–58. doi: 10.1044/jshr.3605.948. [DOI] [PubMed] [Google Scholar]
- Catts HW, Fey ME, Tomblin JB, Zhang X. A longitudinal investigation of reading outcomes in children with language impairments. Journal of Speech-Language-Hearing Research. doi: 10.1044/1092-4388(2002/093). in press. [DOI] [PubMed] [Google Scholar]
- Coster FW, Goorhuis-Brouwer SM, Nakken H, Spelberg HCL. Specific Language Impairments and Behavioural Problems. Folia Phoniatrica et Logopaedica. 1999;51:99–107. doi: 10.1159/000021484. [DOI] [PubMed] [Google Scholar]
- First MB. Mutually exclusive versus co-occurring diagnostic categories: the challenge of diagnostic comorbidity. Psychopathology. 2005;38:206–210. doi: 10.1159/000086093. [DOI] [PubMed] [Google Scholar]
- Gottesman II, Gould TD. The endophenotype concept in psychiatry. American Journal of Psychiatry. 2003;160:636–645. doi: 10.1176/appi.ajp.160.4.636. [DOI] [PubMed] [Google Scholar]
- Kjelgaard M, Tager-Flusberg H. An investigation of language impairment in autism: Implications for genetic subgroups. Language and Cognitive Processes. 2001;16:287–308. doi: 10.1080/01690960042000058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein DN, Riso LP. Psychiatric disorders: Problems of boundaries and comorbidity. In: Costello CG, editor. Basic issues in psychopathology. New York, NY, US: Guilford Press; 1993. pp. 19–66. [Google Scholar]
- Lindsay G, Dockrell JE, Strand S. Longitudinal patterns of behaviour problems in children with specific speech and language difficulties: Child and contextual factors. British Journal of Educational Psychology. 2007;77:811–828. doi: 10.1348/000709906X171127. [DOI] [PubMed] [Google Scholar]
- Lombardino LJ, Riccio CA, Hynd G, Pinherio SB. Linguistic deficits in children with reading disabilities. American Journal of Speech-Language Pathology. 1997;6:71–78. [Google Scholar]
- Naeve G, Ramakrishnan M, Kramer R, Hevroni D, Citri Y, Theill L. Proceedings of the National Academy of Science. 1997;94:2648–2653. doi: 10.1073/pnas.94.6.2648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neale MC, Kendler KS. Multifactorial Models of Comorbidity. Behavior Genetics. 1995;25:281. [PMC free article] [PubMed] [Google Scholar]
- Nicolae D, Gamazon E, Zhang W, Duan S, Dolan ME, Cox NJ. Trait associated SNPs are more liekly to be eQTLs: Annotation to Enhance Discovery from GWAS. 2010 doi: 10.1371/journal.pgen.1000888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Noterdaeme M, Amorosa H. Evaluation of emotional and behavioral problems in language impaired children using the Child Behavior Checklist. European Child & Adolescent Psychiatry. 1999;8:71–77. doi: 10.1007/s007870050087. [DOI] [PubMed] [Google Scholar]
- Pennington BF, Bishop DV. Relations among speech, language, and reading disorders. Annu Rev Psychol. 2009;60:283–306. doi: 10.1146/annurev.psych.60.110707.163548. [DOI] [PubMed] [Google Scholar]
- Pennington BF, Willcutt E, Rhee SH. Analyzing comorbidity. Adv Child Dev Behav. 2005;33:263–304. doi: 10.1016/s0065-2407(05)80010-2. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Tomblin JB, McSweeny JL. Prevalence of speech delay in 6-year-old children and comorbidity with language impairment. J Speech Lang Hear Res. 1999;42:1461–1481. doi: 10.1044/jslhr.4206.1461. [DOI] [PubMed] [Google Scholar]
- Silva PA, Williams S, McGee R. A longitudinal study of children with developmental language delay at age three: Later intelligence, reading and behaviour problems. Developmental Medicine and Child Neurology. 1987;29:630–640. doi: 10.1111/j.1469-8749.1987.tb08505.x. [DOI] [PubMed] [Google Scholar]
- Stearns FW. One Hundred Years of Pleiotropy: A Retrospective. Genetics. 2010;186:767–773. doi: 10.1534/genetics.110.122549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomblin JB, Christiansen MH. In: Explaining developmental communication disorders. Paul R, editor. Speech Disorders San Diego, CA: Plural; 2009. [Google Scholar]
- Tomblin JB, Zhang X, Buckwalter P. The association of reading disability, behavioral disorders, and language impairment among second-grade children. Journal of Child Psychology & Psychiatry & Allied Disciplines. 2000;41:473–482. [PubMed] [Google Scholar]
- Vellutino FR, Scanlon DM, Small SG, Tanzman MS. The linguistic bases of reading ability: Converting written to oral language. Text. 1991;11:99–133. [Google Scholar]
- Vernes SC, Newbury DF, Abrahams BS, Winchester L, Nicod J, Groszer M, et al. A functional genetic link between distinct developmental language disorders. N Engl J Med. 2008;359:2337–2345. doi: 10.1056/NEJMoa0802828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitehouse AJO, Barry JG, Bishop DVM. The broader language phenotype of autism: a comparison with specific language impairment. Journal of Child Psychology and Psychiatry. 2007;48:822–830. doi: 10.1111/j.1469-7610.2007.01765.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitehouse AJO, Barry JG, Bishop DVM. Further defining the language impairment of autism: Is there a specific language impairment subtype? Journal of Communication Disorders. 2008;41:319–336. doi: 10.1016/j.jcomdis.2008.01.002. [DOI] [PubMed] [Google Scholar]
- Williams D, Botting N, Boucher J. Language in autism and specific language impairment: where are the links? Psychol Bull. 2008;134:944–963. doi: 10.1037/a0013743. [DOI] [PubMed] [Google Scholar]