

Abstract
Purpose
Abdominal adiposity is associated with low BMD and decreased growth hormone (GH) secretion, an important regulator of bone homeostasis. The purpose of our study was to determine the effects of a short course of GH on markers of bone turnover and bone marrow fat in premenopausal women with abdominal adiposity.
Materials and Methods
In a 6-month, randomized, double-blind, placebo-controlled trial we studied 79 abdominally obese premenopausal women (21–45y) who underwent daily sc injections of GH vs. placebo. Main outcome measures were body composition by DXA and CT, bone marrow fat by proton MR spectroscopy, P1NP, CTX, 25(OH)D, hsCRP, undercarboxylated osteocalcin (ucOC), preadipocyte factor 1 (Pref 1), apolipoprotein B (ApoB), and IGF-1.
Results
GH increased IGF-1, P1NP, 25(OH)D, ucOC, bone marrow fat and lean mass, and decreased abdominal fat, hsCRP, and ApoB compared with placebo (p<0.05). There was a trend toward an increase in CTX and Pref-1. Among all participants, 6-month increase in IGF-1 correlated with 6-month increase in P1NP (p=0.0005), suggesting that subjects with the greatest increases in IGF-1 experienced the greatest increases in bone formation. Six-month decrease in abdominal fat, hsCRP, and ApoB inversely predicted 6-month change in P1NP, and 6-month increase in lean mass and 25(OH)D positively predicted 6-month change in P1NP (p≤0.05), suggesting that subjects with greatest decreases in abdominal fat, inflammation and ApoB, and the greatest increases in lean mass and 25(OH)D experienced the greatest increases in bone formation. Six-month increase in bone marrow fat correlated with 6-month increase in P1NP (trend), suggesting that subjects with the greatest increases in bone formation experienced the greatest increases in bone marrow fat. Forward stepwise regression analysis indicated that increase in lean mass and decrease in abdominal fat were positive predictors of P1NP. When IGF-1 was added to the model, it became the only predictor of P1NP.
Conclusion
GH replacement in abdominally obese premenopausal women for 6 months increased bone turnover and bone marrow fat. Reductions in abdominal fat, and inflammation, and increases in IGF-1, lean mass and vitamin D were associated with increased bone formation. The increase in bone marrow fat may reflect changes in energy demand from increased bone turnover.
Keywords: obesity, MR spectroscopy, bone, bone marrow fat, growth hormone, bone turnover
1. Introduction
Although obesity is traditionally viewed as protective against osteoporosis, recent studies have linked obesity to osteoporosis and increased fracture risk (1, 2). It has been suggested that visceral adipose tissue (VAT) plays a role in that it may exert detrimental effects on skeletal health (3–5), and a number of mechanisms have been potentially implicated, including dysregulation of the GH-IGF-1 axis, increased inflammation, and lower vitamin D. Visceral obesity is associated with reduced growth hormone (GH) secretion, an important regulator of bone homeostasis (6). Bone and fat cells arise from a common mesenchymal stem cell, capable of differentiating into osteoblasts or adipocytes under the control of hormones and transcription factors (7, 8). The role of GH in stem cell differentiation is complex. Replacement of GH in patients with GH deficiency due to hypopituitarism is associated with increased bone turnover (9). Expansion of the remodeling space leads to an initial decrease in bone mineral density (BMD) during the first year of GH replacement with a subsequent increase in BMD (9). GH administration has also been found to increase the size of the bone marrow preadipocyte pool in male rats (10). During puberty, a time of maximal GH secretion and peak bone acquisition, the conversion of hematopoietic to fatty marrow occurs, suggesting that bone marrow fat may be necessary for osteoblasts to produce new bone (11). No human studies on the effects of GH administration on bone turnover and bone marrow fat have been performed in obese individuals.
Obesity is also associated with chronic inflammation and proinflammatory cytokines and lipoproteins, which have been shown to promote osteoclast differentiation and bone resorption (12, 13). Furthermore, vitamin D, a regulator of bone metabolism, is inversely associated with obesity and fat mass, and vitamin D deficiency is emerging as a risk factor for the metabolic syndrome. We have shown that administration of GH in obese premenopausal women reduces abdominal fat, lipoproteins and inflammatory markers (14). However, the effects of GH on markers of bone turnover and stem cell differentiation and bone marrow fat in obesity are not known.
Utilizing this previously described cohort (14), we examined the effects of GH administration for 6 months on markers of bone turnover and stem cell differentiation and bone marrow fat in premenopausal women with abdominal obesity. We hypothesized that GH administration for 6 months would increase bone formation and increase bone marrow fat, and that increased bone formation is associated with or mediated by an improvement in body composition (decrease in abdominal fat and increase in muscle mass), an increase in circulating 25(OH)D, and a reduction in inflammatory cytokines and lipoproteins.
2. Material and Methods
The study was approved by the institutional review board of Partners HealthCare Inc. and was Health Insurance Portability and Accountability Act compliant. Written informed consent was obtained from all subjects prior to performance of any study procedures.
2.1. Subjects
Our study population has been described previously (14). Subjects were recruited from the community through advertisements. Inclusion criteria were: women from 18–45 years, eumenorrhea, BMI ≥ 25 kg/m2, waist circumference >88 cm (15), IGF-1 level within the lowest 2 quartiles for age (only 1 subject was excluded based on this criterion), stable weight (defined as weight loss or weight gain ≤ 5 pounds in the preceding 3 months). Exclusion criteria included smoking, pregnancy or breastfeeding, hypothalamic or pituitary disorders, diabetes mellitus or other chronic illnesses, estrogen or glucocorticoid use, use of statins, anti-hypertensives, or regular use of aspirin. Eighty subjects met criteria and were enrolled in the study; one subject was discontinued due to a positive pregnancy test at the baseline visit before any procedures were performed or study medication was dispensed. Seventy-nine subjects completed the baseline visit and 50 subjects completed the 6-month visit. Nineteen subjects withdrew for personal reasons, eight for medical causes, one for oral contraceptive initiation, and one due to IV access issues. Baseline clinical characteristics, body composition, and marrow fat have been previously reported on a subset of these subjects (3, 4, 16–21), and 6-month body composition and cardiovascular risk markers have been reported (14). No 6-month marrow fat, bone turnover markers, and vitamin D have been reported.
2.2. Study design
The study protocol, hormone doses employed, and assays has been described previously (14). Briefly, the study was a 6-month, double-blind, randomized, placebo-controlled trial performed at the Massachusetts General Hospital General Clinical Research Center. The following tests were performed at baseline and 6-month: serum IGF-1, bone formation marker procollagen type 1 amino-terminal propeptide (P1NP), bone turnover marker undercarboxylated osteocalcin (ucOC) and bone resorption marker carboxy-terminal collagen crosslinks (CTX), 25-hydroxyvitamin D [25(OH)D], preadipocyte factor 1 (Pref-1), a marker of stem cell differentiation, high sensitivity CRP (hsCRP), and apolipoprotein B (ApoB). Samples were drawn after an overnight fast. Computed tomography (CT) at the level of the 4th lumbar vertebra for abdominal fat, and dual-energy x-ray absorptiometry (DXA) for total fat and lean mass, and proton magnetic resonance spectroscopy (1H-MRS) of the 4th lumbar vertebral body for quantification of bone marrow fat content were performed at baseline and 6-month.
After baseline evaluation, subjects were randomized to receive daily subcutaneous recombinant human GH (Genentech, Inc., South San Francisco, CA) or placebo, which was identical in appearance to the GH, for 6 months. Starting GH dose was 4 micrograms per kilogram per day. Subjects were asked to inject the study medication before bed. GH doses were adjusted based on IGF-1 levels by a physician not involved in the study, using an algorithm based on pre-treatment IGF-1 level and an IGF-1 level target in the upper normal age-appropriate range. Participants in the placebo group were sham dose adjusted to maintain study-subject and investigator blinding. Compliance with GH administration was tested by analysis for the presence of 22-kDa hGH, which becomes predominant after administration of rhGH (14).
2.3. Endocrine testing
25(OH)D, P1NP, and CTX were measured by IDS-iSYS Multi-Discipline Automated Analyzer based on chemiluminescence technology (Immunodiagnostic Systems, Inc., Fountain Hills, AZ). Minimum detection limits are: 25(OH)D 3.6 ng/ml, P1NP <1.0 ng/ml, and CTX 0.023ng/ml. Pref-1 was measured with the Quantikine human Pref-1 immunoassay (ELISA) (R&D Systems, Minneapolis, MN) with a mean minimum detectable level of 0.012 ng/ml. ucOC was measured by solid phase enzyme immunoassay (Takara/Clontech) with a detection range of 0.125–8 ng/ml. Coefficient of variation (cv) are <5% for all assays. The assays used for IGF-1, hsCRP and ApoB have been described previously (14).
2.4. 1H-MR spectroscopy of bone marrow
1H-MRS of the 4th lumbar vertebral body was performed in 36 subjects at baseline and 23 subjects at 6-month to determine bone marrow lipid content using a 3.0T MR imaging system (Siemens Trio, Siemens Medical Systems, Erlangen, Germany) as previously described (22). Subjects who underwent 1H-MRS did not differ in baseline characteristics and response to GH compared to subjects who did not undergo 1H-MRS and were equally distributed between the GH and placebo groups. Fitting of all 1H-MRS data was performed using LCModel (version 6.3-0K, Stephen Provencher, Oakville, Canada). Metabolite quantification was performed using eddy current correction and water scaling. A customized fitting algorithm for bone marrow analysis provided estimates for all lipid signals combined (0.9, 1.3, and 2.3 ppm). LCModel bone marrow lipid estimates were automatically scaled to unsuppressed water peak (4.7 ppm) and expressed as lipid to water ratio [%]. CV for bone marrow fat quantification is 3% at our institution.
2.5. Dual-energy X-ray-absorptiometry
Total body fat and lean mass were assessed in all subjects on a Hologic QDR 4500 scanner (Hologic Inc., Waltham, MA) (precision error of 1.7% for fat mass and of 2.4% for fat-free mass).
2.6. Computed Tomography (CT)
Each subject underwent single-slice CT of the abdomen at the level of L4 as previously described (21). Abdominal subcutaneous adipose tissue (SAT), visceral adipose tissue (VAT), and total adipose tissue (TAT) were determined (CV <1% for fat area quantification).
2.7. Statistical analysis
JMP Statistical Database Software (version 5.0.1; SAS Institute, Cary, NC) was used for statistical analyses. The measures were secondary endpoints. The primary outcome variable was the bone formation marker P1NP.
Baseline means and mean 6-month changes (6-month value minus baseline value) were compared with ANOVA. Univariate regression models were constructed with the GH and placebo groups combined to determine hormonal and body composition predictors of bone markers and BM fat and non-parametric Spearman rank correlation coefficients are reported. Multivariate standard least squares regression modeling was performed to control for age and treatment group (GH vs placebo). Forward stepwise regression modeling was also performed to determine the strongest predictors of bone formation marker P1NP levels. P ≤ 0.05 was used to denote significance and p ≤ 0.1 was used to denote a trend. Data are presented as mean ± SEM.
3. Results
Baseline subject characteristics are shown in Table 1. Thirty-nine subjects were randomized to receive GH and 40 subjects to receive placebo. Of the 50 subjects who completed the 6-month visit, 28 were on GH and 22 on placebo. Both groups were of comparable age, BMI, body composition, IGF-1 levels and bone marker levels. The mean GH dose for the GH treatment group at 6 months was 1.7±0.1 mg/day. These doses resulted in a mean IGF-1 level increase from 137.9±81 ng/ml at baseline to 212.3±12.2 ng/ml at 6-months and a mean IGF-1 standard deviation score (SDS) increase from −1.7±0.1 ng/ml at baseline to −0.1±0.3 at 6 months (p<0.0001 compared to placebo). As previously reported, compliance analysis revealed full compliance in 46%, intermittent rhGH use in 43%, and non-compliance in 11% of subjects in the GH group (14). There was no significant difference in reported side effects between the GH and placebo groups. There was one serious unrelated adverse event: development of cancer in a study subject who was receiving placebo. One subject was discontinued from the study at 3 months secondary to a 2-hour glucose greater than 200 mg/ml, a pre-specified drop criterion. Four subjects had 2-hour glucose levels greater than 200 mg/ml at six months, one of whom was receiving placebo. No other serious related or unrelated adverse events occurred during this study (14).
Table 1.
Baseline characteristics
| GH group | Placebo group | p | |
|---|---|---|---|
| Age (years) | 35.7±1.1 | 36.1±1.1 | 0.8 |
| BMI (kg/m2) | 34.8±0.8 | 34.9±0.9 | 0.9 |
| P1NP (ng/ml) | 45.7±3.2 | 44.3±2.6 | 0.7 |
| CTX (ng/ml) | 0.33±0.04 | 0.25±0.03 | 0.06 |
| uc Osteocalcin (ng/ml) | 2.6±0.4 | 2.3±0.4 | 0.6 |
| 25OHD (ng/ml) | 24.2±2.9 | 24.3±1.6 | 1.0 |
| Pref-1 (ng/ml) | 0.22±0.01 | 0.27±0.04 | 0.2 |
| Bone marrow fat l/w ratio (%) | 0.57±0.09 | 0.59±0.05 | 0.9 |
Data presented as mean±SEM. BMI: body mass index, P1NP: procollagen type 1 amino-terminal propeptide, CTX: carboxy-terminal collagen crosslinks, uc: undercarboxylated, Pref-1: preadipocyte factor 1
3.1. Effects of GH administration on bone
6-month changes in the GH and placebo groups are summarized in Table 2. Six months of GH increased the bone formation marker P1NP and bone turnover marker ucOC compared to placebo (p=0.0007 and p=0.01, respectively) (Figure 1), and there was a trend toward an increase in the bone resorption marker CTX in the GH group at 6 months compared to placebo (p=0.08). GH also increased 25(OH)D at 6 months compared to placebo (p=0.0002), and there was a trend toward an increase in Pref-1 levels (p=0.07). At baseline (pre-treatment), 32 subjects were vitamin D deficient [25(OH)D < 20 ng/ml] and 25 subjects were vitamin D insufficient [25(OH)D < 30 ng/ml]. Within the GH group, a 6-month increase in vitamin D levels from insufficient to normal was seen in 3 subjects, from deficient to insufficient in 4 subjects, and from deficient to normal in 1 subject. Within the placebo group, 1 subject increased her vitamin D level from deficient to insufficient, while 3 subjects decreased their vitamin D levels from insufficient to deficient and 2 subjects decreased their vitamin D levels from normal to insufficient.
Table 2.
Bone parameters in premenopausal obese women who completed both baseline and 6-month visits treated with GH or placebo for 6 months
| Variable | Treatment | Baseline | 6 months | Delta 6 months | p-baseline | p-between groups |
|---|---|---|---|---|---|---|
| P1NP (ng/ml) | GH | 44.3±4.1 | 74.4±7.2 | 30.0±6.5 | 0.7 | 0.0007 |
| Placebo | 41.9±4.3 | 41.2±4.2 | −0.8±2.8 | |||
| CTX (ng/ml) | GH | 0.32±0.05 | 0.46±0.06 | 0.15±0.06 | 0.07 | 0.08 |
| Placebo | 0.21±0.03 | 0.23±0.02 | 0.02±0.03 | |||
| uc Osteocalcin (ng/ml) | GH | 2.6±0.4 | 5.0±0.6 | 2.4±0.6 | 0.6 | 0.01 |
| Placebo | 2.3±0.4 | 2.8±0.5 | 0.5±0.2 | |||
| 25OHD (ng/ml) | GH | 20.2±2.1 | 24.9±2.4 | 4.7±1.4 | 0.5 | 0.0002 |
| Placebo | 22.4±2.3 | 18.2±2.2 | −4.2±1.6 | |||
| Pref-1 (ng/ml) | GH | 0.22±0.01 | 0.25±0.03 | 0.02±0.02 | 0.2 | 0.07 |
| Placebo | 0.27±0.04 | 0.25±0.01 | −0.02±0.02 | |||
| Bone marrow fat l/w ratio (%) | GH | 0.53±0.08 | 0.57±0.08 | 0.04±0.03 | 0.3 | 0.003 |
| Placebo | 0.62±0.07 | 0.53±0.06 | −0.9±0.03 |
Data presented as mean±SEM. P1NP: procollagen type 1 amino-terminal propeptide, CTX: carboxy-terminal collagen crosslinks, uc: undercarboxylated, Pref-1: preadipocyte factor 1
Figure 1.

Mean (±SEM) change in P1NP (A) and undercarboxylated (uc) osteocalcin (B), over 6 months of GH administration versus placebo. *, p< 0.05 vs. placebo
Six months of GH therapy increased L4 bone marrow fat compared to placebo (p=0.003) (Figure 2).
Figure 2.
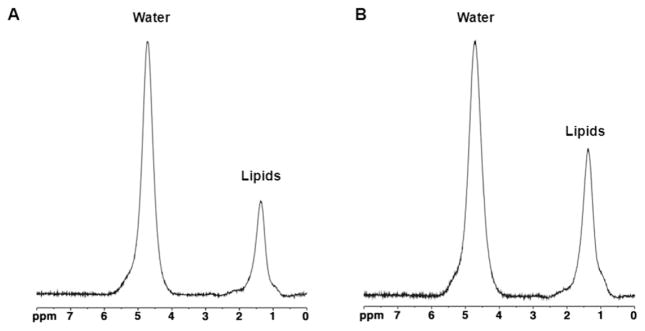
1H-MR spectroscopy of bone marrow in a 40 year-old obese woman (BMI 34.9 kg/m2) before (A) and after (B) 6 months of GH administration. There is increased bone marrow lipid content following GH administration (0.44 vs 0.63 lipid-water ratio). For purposes of visual comparison, the amplitude of unsuppressed water was scaled identically.
3.2. Effects of GH administration on body composition, inflammatory markers and apo B
As previously reported, GH decreased abdominal TAT and SAT by CT at 6 months compared to placebo (delta 6-month TAT GH vs placebo: −28±9.7 vs 1.5±11.0 cm2, p=0.04, delta 6-month SAT: −19.9±7.4 vs 5.2±8.6 cm2p=0.02), while there was no significant change in VAT between the two groups (p=0.6) (14). There was a significant increase in lean mass in the GH group at 6 months compared to placebo (delta 6-month lean mass: 1.9± 0.5 vs 0.1±0.4 kg, p=0.04) (14). GH decreased hsCRP (delta 6-month hsCRP: −1.1±0.3 vs 0.07±0.3, p=0.002) and ApoB (delta 6-month Apo B: −9.1±3.4 vs 3.9±4.2 p=0.04) at 6-month compared to placebo (14).
3.3. Predictors of bone formation marker P1NP and bone marrow fat
Within the entire group, six-month change in P1NP correlated with 6-month change in CTX (r=0.35, p=0.03) and 6-month change in ucOC (r=0.42, p=0.008), likely reflecting the coupling of bone formation and resorption. Six-month change in IGF-1 correlated with 6-month change in P1NP (r=0.55, p=0.0005) (Figure 3a), suggesting that, in general, subjects with the greatest increases in IGF-1 levels experienced the greatest increases in bone formation. The association remained significant after controlling for age (p=0.01). Six-month change in abdominal fat was inversely associated with 6-month change in P1NP (r= −0.40, p=0.05) (Figure 3b), independent of age and treatment group (GH vs placebo) (p=0.02), suggesting that subjects with the greatest reductions of abdominal fat experienced, in general, the greatest increases in bone formation. Six-month increase in P1NP correlated with 6-month increase in lean mass (r=0.46, p=0.003), independent of age and treatment group (GH vs placebo) (p=0.04), suggesting that subjects with the greatest increases in lean mass experienced, in general, the greatest increases in bone formation marker levels. Six-month change in P1NP levels correlated with 6-month change in 25(OH)D (r= 0.48, p=0.003) (Figure 3c), suggesting that subjects with the greatest increase in circulating 25(OH)D had, in general, the greatest increase in bone formation marker levels. However, after controlling for age and treatment group, the association became a trend (p=0.08). Six-month change in hsCRP inversely correlated with 6-month change in P1NP (r= −0.41, p=0.04) (Figure 3d), independent of age (p=0.04), suggesting that subjects with the greatest decreases in inflammation experienced, in general, the greatest increases in bone formation. The association lost significance after controlling for treatment group (p=0.7). Six-month change in ApoB correlated inversely with 6-month change in P1NP (r= −0.31, p= 0.05), suggesting that subjects with the greatest decreases in lipoproteins experienced, in general, the greatest increases in bone formation marker levels. However, the association lost significance after controlling for age and treatment group (p=0.2)
Figure 3.

Regression analysis of 6-month change in P1NP on 6-month change in IGF-1 (A), abdominal total adipose tissue (TAT) (B), 25-OH Vitamin D (C), and hsCRP (D).
Six-month change in bone marrow fat correlated with 6-month change in P1NP (trend) (r=0.45, p=0.08), suggesting that subjects with the greatest increases in bone formation experienced, in general, the greatest increases in bone marrow fat. Six-month change in bone marrow fat correlated with 6-month change in IGF-1 (trend) (r=0.42, p=0.07), suggesting that subjects with the greatest increases in IGF-1 experienced, in general, the greatest increases in bone marrow fat formation. There was a trend toward a positive correlation between 6-month change in Pref-1 with 6-month change in bone marrow fat (r= 0.41, p=0.07), consistent with known effects of Pref-1 as a regulator of stem cell differentiation into the adipocyte lineage.
When 6-month change in P1NP levels was entered as a dependent variable and 6-month change in total abdominal fat, lean mass, 25(OH)D, and hsCRP as independent variables in a forward stepwise regression model, 6-month change in lean mass and abdominal fat were the only predictors of 6-month change in P1NP (p=0.004 for both measures) and explained 19% and 17% of P1NP variability, respectively. When 6-month change in IGF-1 was added as independent variable into the model, 6-month change in IGF-1 was the only predictor of 6-month change in P1NP (p<0.0001) and explained 52% of P1NP variability.
4. Discussion
Our study showed that a short course (6 months) of GH administration to abdominally obese premenopausal women increases bone formation markers and bone marrow fat. Direct effects of GH and IGF-1 likely play a role, and in addition, the increase in bone formation with GH administration may be in part mediated by an improvement in body composition with a reduction in abdominal fat and an increase in lean mass, an increase in circulating 25(OH)D, and a decrease in inflammatory cytokines and lipoproteins.
Although obesity has been thought to be protective against the development of osteoporosis, strong evidence now links accumulation of fat, particularly in the abdominal depot, with bone loss (1, 2). Potential mechanisms for obesity-induced bone loss include deleterious effects of inflammatory cytokines and lipoproteins on bone and low levels of circulating 25(OH)D. Inflammatory cytokines, such as hsCRP, which are elevated in abdominal obesity, promote osteoclast differentiation and bone resorption (12). In a large prospective study of older men and women, elevated inflammatory markers were a strong predictor of fracture risk (23). Moreover, lipids and lipoproteins, which are elevated in abdominal obesity, have been shown to inhibit osteoblast differentiation and to enhance osteoclast differentiation and survival (12, 24). Statin therapy to lower hyperlipidemia is associated with increased BMD and decreased fracture risk (25, 26) and bisphosphonates lower serum LDL cholesterol and apoB (27), supporting a connection between bone and lipid metabolism. In addition, vitamin D levels are reduced in patients with abdominal adiposity (28), in part due to sequestration of vitamin D, a fat soluble molecule, in adipose tissue.
Obesity is also a state of relative GH and IGF-1 deficiency, critical regulators of bone homeostasis, and abdominal adipose tissue is a strong negative determinant of GH secretion (29). Adult-onset GH deficiency is also complicated by reduced BMD and increased fracture risk, and GH replacement in these patients leads to an increase in markers of bone turnover (9, 30). Bone remodeling, with a prominent augmentation in bone formation, increases within a few months of GH therapy, before an increase in BMD is apparent. The expansion of the remodeling space may lead to an initial decrease in BMD; a subsequent increase in BMD ensues in 12 to 18 months (9, 30). GH also directly stimulates the carboxylation of osteocalcin, a marker of bone turnover (31). Consistent with these data, our study showed that GH administration for 6 months to obese women increased markers of bone turnover. Recent studies have shown that the bone turnover marker ucOC also functions as a regulator of bone and glucose homeostasis (32–34). In fact, genetically modified mice with increased ucOC activity were protected from diet-induced obesity and type 2 diabetes (34). Our study is the first to show that GH administration increases ucOC in obese individuals.
The effect of GH administration on stem cell differentiation and bone marrow fat has not been studied in humans, and our study is the first to examine the effects of GH administration on bone marrow fat content in obese women. Animal studies have shown that GH deficient rats have an increased number and size of bone marrow adipocytes which return to normal following GH administration (7). A study in hypophysectomized rats has shown increased bone lipid levels, despite reduced adipocyte precursors, compared to controls, and administration of GH enhanced the adipocyte and osteoblast precursor pool size, supporting the hypothesis that GH increases adipocyte and osteoblast precursors in bone marrow (35). We found increased bone marrow fat content of the lumbar spine following 6 months of GH administration compared to placebo, and the increase in marrow fat content was positively associated with an increase in bone formation, suggesting that the bone marrow adipocytes may serve as an energy source for the increased bone turnover. Furthermore, the increase in marrow may serve to fill the incompletely mineralized remodeling space. We also found an increase in Pref-1, an important regulator of stem cell differentiation, following GH administration compared to placebo, and the increase in Pref-1 was associated with an increase in bone marrow fat. Our results are consistent with a prior study in GH deficient subjects in which GH administration for 3 months increased serum Pref-1 levels compared to placebo (36). This is in contrast to a study in mice, in which GH administration using hydrodynamic-based gene transfer procedure reduced serum Pref-1 levels (37). The reason for the discrepant results is unclear and may reflect a differential response to GH in humans and mice. We hypothesize that longer-term GH administration for 18-month would decrease bone marrow fat and Pref-1 after more complete mineralization of the remodeling space.
In addition to the anabolic effects on bone, GH is also an important regulator of lipolysis. GH increases adipocyte lipolysis and lipid turnover, and states of GH deficiency due to pituitary disease are associated with increased abdominal fat (38). GH is also an important mediator of inflammation. GH has cytokine-like effects and its administration results in decreased hsCRP levels in patients with GH deficiency due to pituitary disorders or obesity (14, 39). GH administration also decreases cholesterol and apoB (14, 39). GH and IGF-1 also act on the renal tubules to increase production of active 1,25 dihydroxyvitamin D (40). Our data show that GH administration for 6 months to obese premenopausal women decreases abdominal fat, hsCRP and apoB, and increases circulating 25(OH)D, and that these changes are associated with an increase in bone formation. The increase in circulating 25(OH)D may be due to GH-induced loss of abdominal fat and subsequent release of sequestered fat soluble 25(OH)D from adipose tissue into the blood stream.
GH also increases lean mass (9, 14), an important positive predictor of bone formation. In our study, the increase in lean mass was positively associated with the increase in bone formation.
Our study had several limitations. First is the relatively high drop-out rate. However, our dropout rate was similar compared to other obesity studies (41, 42) and was similar in the GH and placebo groups. Second, bone marrow fat was only assessed in a subset of subjects. We were able to detect a significant difference between the groups in bone marrow fat content, which suggests that we had adequate power for this endpoint. Third, we did not have BMD measurements available to assess the effects of GH on BMD.
In conclusion, our study showed that short-term GH administration to abdominally obese premenopausal women increases markers of bone formation and bone marrow fat. The increase in bone formation is associated with a decrease in abdominal fat, inflammation and lipoproteins and an increase in IGF-1 levels, 25(OH)D and lean mass. Whether the increases in bone formation reflects direct effects of GH and/or IGF-1 levels or is in part mediated by changes in body composition, increases in circulating 25(OH)D levels and decreases in systemic inflammation and Apo B is unknown and warrants further study. The effects of a longer course of GH therapy in obese individuals, such as has been shown to increase BMD in hypopituitary populations, are unknown and warrant further investigation.
Highlights.
6-month GH administration to obese premenopausal women increases bone formation and bone marrow fat.
Increased bone formation is associated with decreased abdominal fat, inflammation and lipoproteins.
Increased bone formation is associated with increased lean mass and vitamin D.
Acknowledgments
This work was supported in part by National Institutes of Health Grants R01 HL-077674, UL1 RR-025758, K24 HL092902-03 and K23 RR-23090
Footnotes
The authors have no conflict of interest to declare.
Study medication (GH and placebo) only was provided by Genentech, Inc., South San Francisco, CA. Clinical trials registration number:NCT00131378
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Cohen A, Dempster DW, Recker RR, Lappe JM, Zhou H, Zwahlen A, et al. Abdominal fat is associated with lower bone formation and inferior bone quality in healthy premenopausal women: a transiliac bone biopsy study. J Clin Endocrinol Metab. 2013 Jun;98(6):2562–72. doi: 10.1210/jc.2013-1047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Compston JE, Watts NB, Chapurlat R, Cooper C, Boonen S, Greenspan S, et al. Obesity is not protective against fracture in postmenopausal women: GLOW. Am J Med. 2011 Nov;124(11):1043–50. doi: 10.1016/j.amjmed.2011.06.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bredella MA, Torriani M, Ghomi RH, Thomas BJ, Brick DJ, Gerweck AV, et al. Determinants of bone mineral density in obese premenopausal women. Bone. 2011 Apr 1;48(4):748–54. doi: 10.1016/j.bone.2010.12.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bredella MA, Torriani M, Ghomi RH, Thomas BJ, Brick DJ, Gerweck AV, et al. Vertebral bone marrow fat is positively associated with visceral fat and inversely associated with IGF-1 in obese women. Obesity (Silver Spring) 2011 Jan;19(1):49–53. doi: 10.1038/oby.2010.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gilsanz V, Chalfant J, Mo AO, Lee DC, Dorey FJ, Mittelman SD. Reciprocal relations of subcutaneous and visceral fat to bone structure and strength. J Clin Endocrinol Metab. 2009 Sep;94(9):3387–93. doi: 10.1210/jc.2008-2422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Giustina A, Mazziotti G, Canalis E. Growth hormone, insulin-like growth factors, and the skeleton. Endocr Rev. 2008 Aug;29(5):535–59. doi: 10.1210/er.2007-0036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gevers EF, Loveridge N, Robinson IC. Bone marrow adipocytes: a neglected target tissue for growth hormone. Endocrinology. 2002 Oct;143(10):4065–73. doi: 10.1210/en.2002-220428. [DOI] [PubMed] [Google Scholar]
- 8.Takada I, Suzawa M, Matsumoto K, Kato S. Suppression of PPAR transactivation switches cell fate of bone marrow stem cells from adipocytes into osteoblasts. Ann N Y Acad Sci. 2007 Nov;1116:182–95. doi: 10.1196/annals.1402.034. [DOI] [PubMed] [Google Scholar]
- 9.Baum HB, Biller BM, Finkelstein JS, Cannistraro KB, Oppenhein DS, Schoenfeld DA, et al. Effects of physiologic growth hormone therapy on bone density and body composition in patients with adult-onset growth hormone deficiency. A randomized, placebo-controlled trial. Ann Intern Med. 1996 Dec 1;125(11):883–90. doi: 10.7326/0003-4819-125-11-199612010-00003. [DOI] [PubMed] [Google Scholar]
- 10.Appiagyei-Dankah Y, Tapiador CD, Evans JF, Castro-Magana M, Aloia JF, Yeh JK. Influence of growth hormone on bone marrow adipogenesis in hypophysectomized rats. Am J Physiol Endocrinol Metab. 2003 Mar;284(3):E566–73. doi: 10.1152/ajpendo.00213.2002. [DOI] [PubMed] [Google Scholar]
- 11.Rosen CJ, Ackert-Bicknell C, Rodriguez JP, Pino AM. Marrow fat and the bone microenvironment: developmental, functional, and pathological implications. Crit Rev Eukaryot Gene Expr. 2009;19(2):109–24. doi: 10.1615/critreveukargeneexpr.v19.i2.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Koh JM, Khang YH, Jung CH, Bae S, Kim DJ, Chung YE, et al. Higher circulating hsCRP levels are associated with lower bone mineral density in healthy pre- and postmenopausal women: evidence for a link between systemic inflammation and osteoporosis. Osteoporos Int. 2005 Oct;16(10):1263–71. doi: 10.1007/s00198-005-1840-5. [DOI] [PubMed] [Google Scholar]
- 13.Parhami F, Jackson SM, Tintut Y, Le V, Balucan JP, Territo M, et al. Atherogenic diet and minimally oxidized low density lipoprotein inhibit osteogenic and promote adipogenic differentiation of marrow stromal cells. J Bone Miner Res. 1999 Dec;14(12):2067–78. doi: 10.1359/jbmr.1999.14.12.2067. [DOI] [PubMed] [Google Scholar]
- 14.Bredella MA, Lin E, Brick DJ, Gerweck AV, Harrington LM, Torriani M, et al. Effects of GH in women with abdominal adiposity: a 6-month randomized, double-blind, placebo-controlled trial. Eur J Endocrinol. 2012 Apr;166(4):601–11. doi: 10.1530/EJE-11-1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lean ME, Han TS, Morrison CE. Waist circumference as a measure for indicating need for weight management. Bmj. 1995 Jul 15;311(6998):158–61. doi: 10.1136/bmj.311.6998.158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bredella MA, Ghomi RH, Thomas BJ, Miller KK, Torriani M. Comparison of 3.0 T proton magnetic resonance spectroscopy short and long echo-time measures of intramyocellular lipids in obese and normal-weight women. J Magn Reson Imaging. 2010 Aug;32(2):388–93. doi: 10.1002/jmri.22226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bredella MA, Ghomi RH, Thomas BJ, Ouellette HA, Sahani DV, Miller KK, et al. Breath-hold 1H-magnetic resonance spectroscopy for intrahepatic lipid quantification at 3 Tesla. J Comput Assist Tomogr. 2010 May-Jun;34(3):372–6. doi: 10.1097/RCT.0b013e3181cefb89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bredella MA, Ghomi RH, Thomas BJ, Torriani M, Brick DJ, Gerweck AV, et al. Comparison of DXA and CT in the assessment of body composition in premenopausal women with obesity and anorexia nervosa. Obesity (Silver Spring) 2010 Nov;18(11):2227–33. doi: 10.1038/oby.2010.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bredella MA, Torriani M, Ghomi RH, Thomas BJ, Brick DJ, Gerweck AV, et al. Adiponectin is inversely associated with intramyocellular and intrahepatic lipids in obese premenopausal women. Obesity (Silver Spring) 2011 May;19(5):911–6. doi: 10.1038/oby.2010.296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Bredella MA, Torriani M, Thomas BJ, Ghomi RH, Brick DJ, Gerweck AV, et al. Peak growth hormone-releasing hormone-arginine-stimulated growth hormone is inversely associated with intramyocellular and intrahepatic lipid content in premenopausal women with obesity. J Clin Endocrinol Metab. 2009 Oct;94(10):3995–4002. doi: 10.1210/jc.2009-0438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bredella MA, Utz AL, Torriani M, Thomas B, Schoenfeld DA, Miller KK. Anthropometry, CT, and DXA as predictors of GH deficiency in premenopausal women: ROC curve analysis. J Appl Physiol. 2009 Feb;106(2):418–22. doi: 10.1152/japplphysiol.90998.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bredella MA, Fazeli PK, Miller KK, Misra M, Torriani M, Thomas BJ, et al. Increased bone marrow fat in anorexia nervosa. J Clin Endocrinol Metab. 2009 Jun;94(6):2129–36. doi: 10.1210/jc.2008-2532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cauley JA, Danielson ME, Boudreau RM, Forrest KY, Zmuda JM, Pahor M, et al. Inflammatory markers and incident fracture risk in older men and women: the Health Aging and Body Composition Study. J Bone Miner Res. 2007 Jul;22(7):1088–95. doi: 10.1359/jbmr.070409. [DOI] [PubMed] [Google Scholar]
- 24.Parhami F, Morrow AD, Balucan J, Leitinger N, Watson AD, Tintut Y, et al. Lipid oxidation products have opposite effects on calcifying vascular cell and bone cell differentiation. A possible explanation for the paradox of arterial calcification in osteoporotic patients. Arterioscler Thromb Vasc Biol. 1997 Apr;17(4):680–7. doi: 10.1161/01.atv.17.4.680. [DOI] [PubMed] [Google Scholar]
- 25.Edwards CJ, Hart DJ, Spector TD. Oral statins and increased bone-mineral density in postmenopausal women. Lancet. 2000 Jun 24;355(9222):2218–9. doi: 10.1016/s0140-6736(00)02408-9. [DOI] [PubMed] [Google Scholar]
- 26.Hernandez JL, Olmos JM, Romana G, Martinez J, Castillo J, Yezerska I, et al. Bone mineral density in statin users: a population-based analysis from a Spanish cohort. J Bone Miner Metab. 2013 Jun 20; doi: 10.1007/s00774-013-0481-6. [DOI] [PubMed] [Google Scholar]
- 27.Adami S, Braga V, Guidi G, Gatti D, Gerardi D, Fracassi E. Chronic intravenous aminobisphosphonate therapy increases high-density lipoprotein cholesterol and decreases low-density lipoprotein cholesterol. J Bone Miner Res. 2000 Mar;15(3):599–604. doi: 10.1359/jbmr.2000.15.3.599. [DOI] [PubMed] [Google Scholar]
- 28.Snijder MB, van Dam RM, Visser M, Deeg DJ, Dekker JM, Bouter LM, et al. Adiposity in relation to vitamin D status and parathyroid hormone levels: a population-based study in older men and women. J Clin Endocrinol Metab. 2005 Jul;90(7):4119–23. doi: 10.1210/jc.2005-0216. [DOI] [PubMed] [Google Scholar]
- 29.Pijl H, Langendonk JG, Burggraaf J, Frolich M, Cohen AF, Veldhuis JD, et al. Altered neuroregulation of GH secretion in viscerally obese premenopausal women. J Clin Endocrinol Metab. 2001 Nov;86(11):5509–15. doi: 10.1210/jcem.86.11.8061. [DOI] [PubMed] [Google Scholar]
- 30.Hansen TB, Brixen K, Vahl N, Jorgensen JO, Christiansen JS, Mosekilde L, et al. Effects of 12 months of growth hormone (GH) treatment on calciotropic hormones, calcium homeostasis, and bone metabolism in adults with acquired GH deficiency: a double blind, randomized, placebo-controlled study. J Clin Endocrinol Metab. 1996 Sep;81(9):3352–9. doi: 10.1210/jcem.81.9.8784096. [DOI] [PubMed] [Google Scholar]
- 31.Hubina E, Lakatos P, Kovacs L, Szabolcs I, Racz K, Toth M, et al. Effects of 24 months of growth hormone (GH) treatment on serum carboxylated and undercarboxylated osteocalcin levels in GH-deficient adults. Calcif Tissue Int. 2004 Jan;74(1):55–9. doi: 10.1007/s00223-002-2149-4. [DOI] [PubMed] [Google Scholar]
- 32.Ferron M, Wei J, Yoshizawa T, Del Fattore A, DePinho RA, Teti A, et al. Insulin signaling in osteoblasts integrates bone remodeling and energy metabolism. Cell. 2010 Jul 23;142(2):296–308. doi: 10.1016/j.cell.2010.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Fulzele K, Riddle RC, DiGirolamo DJ, Cao X, Wan C, Chen D, et al. Insulin receptor signaling in osteoblasts regulates postnatal bone acquisition and body composition. Cell. 2010 Jul 23;142(2):309–19. doi: 10.1016/j.cell.2010.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lee NK, Sowa H, Hinoi E, Ferron M, Ahn JD, Confavreux C, et al. Endocrine regulation of energy metabolism by the skeleton. Cell. 2007 Aug 10;130(3):456–69. doi: 10.1016/j.cell.2007.05.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Menagh PJ, Turner RT, Jump DB, Wong CP, Lowry MB, Yakar S, et al. Growth hormone regulates the balance between bone formation and bone marrow adiposity. J Bone Miner Res. 2010 Apr;25(4):757–68. doi: 10.1359/jbmr.091015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Andersen M, Jensen CH, Stoving RK, Larsen JB, Schroder HD, Teisner B, et al. Fetal antigen 1 in healthy adults and patients with pituitary disease: relation to physiological, pathological, and pharmacological GH levels. J Clin Endocrinol Metab. 2001 Nov;86(11):5465–70. doi: 10.1210/jcem.86.11.7990. [DOI] [PubMed] [Google Scholar]
- 37.Abdallah BM, Ding M, Jensen CH, Ditzel N, Flyvbjerg A, Jensen TG, et al. Dlk1/FA1 is a novel endocrine regulator of bone and fat mass and its serum level is modulated by growth hormone. Endocrinology. 2007 Jul;148(7):3111–21. doi: 10.1210/en.2007-0171. [DOI] [PubMed] [Google Scholar]
- 38.Jorgensen JO, Vahl N, Hansen TB, Skjaerbaek C, Fisker S, Orskov H, et al. Determinants of serum insulin-like growth factor I in growth hormone deficient adults as compared to healthy subjects. Clin Endocrinol (Oxf) 1998 Apr;48(4):479–86. doi: 10.1046/j.1365-2265.1998.00424.x. [DOI] [PubMed] [Google Scholar]
- 39.Bollerslev J, Ueland T, Jorgensen AP, Fougner KJ, Wergeland R, Schreiner T, et al. Positive effects of a physiological dose of GH on markers of atherogenesis: a placebo-controlled study in patients with adult-onset GH deficiency. Eur J Endocrinol. 2006 Apr;154(4):537–43. doi: 10.1530/eje.1.02125. [DOI] [PubMed] [Google Scholar]
- 40.Wei S, Tanaka H, Kubo T, Ono T, Kanzaki S, Seino Y. Growth hormone increases serum 1,25-dihydroxyvitamin D levels and decreases 24,25-dihydroxyvitamin D levels in children with growth hormone deficiency. Eur J Endocrinol. 1997 Jan;136(1):45–51. doi: 10.1530/eje.0.1360045. [DOI] [PubMed] [Google Scholar]
- 41.Fidler MC, Sanchez M, Raether B, Weissman NJ, Smith SR, Shanahan WR, et al. A one-year randomized trial of lorcaserin for weight loss in obese and overweight adults: the BLOSSOM trial. J Clin Endocrinol Metab. 2011 Oct;96(10):3067–77. doi: 10.1210/jc.2011-1256. [DOI] [PubMed] [Google Scholar]
- 42.James WP, Caterson ID, Coutinho W, Finer N, Van Gaal LF, Maggioni AP, et al. Effect of sibutramine on cardiovascular outcomes in overweight and obese subjects. N Engl J Med. 2010 Sep 2;363(10):905–17. doi: 10.1056/NEJMoa1003114. [DOI] [PubMed] [Google Scholar]