

Albeit extremely rare, the rectum has ectopic tissues including the gastric mucosa, salivary gland, and pancreas [1-9]. Moreover, only one case of ectopic respiratory mucosa in the rectum has been reported [10]. Herein, we describe the second documented case of ectopic respiratory mucosa in the rectum and review the literature.
A 38-year-old Japanese female was incidentally detected with a submucosal tumor, measuring 7 x 3 mm in diameter, in the lower rectum. An endoscopic mucosal resection was performed.
Histopathological study of the endoscopically resected specimen revealed the presence of a unilocular cystic lesion under the rectal mucosa (Figure 1A). Smooth muscle bundles were recognized around the entire cyst (Figure 1A), and no connection with surface rectal mucosa was noted. The cyst wall was covered by pseudostratified ciliated epithelium (Figure 1B), and accumulation of neutrophils was observed within the cyst. The ciliated epithelium was without atypia, and no mitotic figures were observed. A few goblet cells were present. Mild lymphocytic infiltration and lymphoid follicle formation were also observed around the cyst (Figure 1A). No gastric, salivary, pancreatic, endometrial, and seromucinous gland tissues were present.
Figure 1.
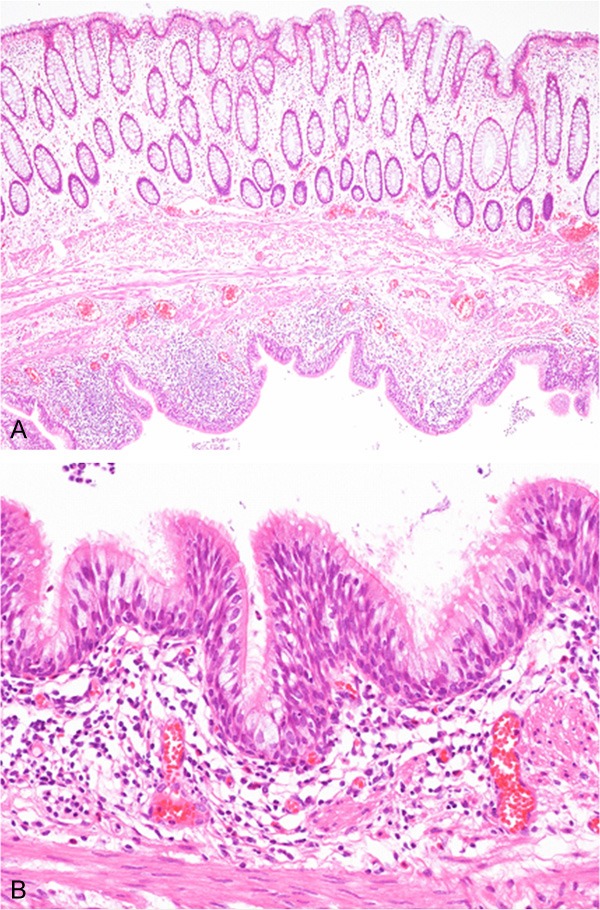
Histopathological features of the rectal submucosal tumor. A: A unilocular cystic lesion is present under the mucosa. Mild lymphocytic inflammation and smooth muscle bundles are present around the cyst. HE, x 40. B: The cyst is covered by pseudostratified ciliated epithelium without atypia. HE, x 200.
Immunohistochemical studies were performed using an autostainer (Ventana) by the same method as previously reported [11-15]. p63-positive basal cells were present in the ciliated epithelium (Figure 2), however, TTF-1 was not expressed. Estrogen and progesterone receptors were also not expressed in the ciliated epithelium. Moreover, no chromogranin A- or synaptophysin-positive cells were observed. Ki-67 labeling index was less than 1%.
Figure 2.
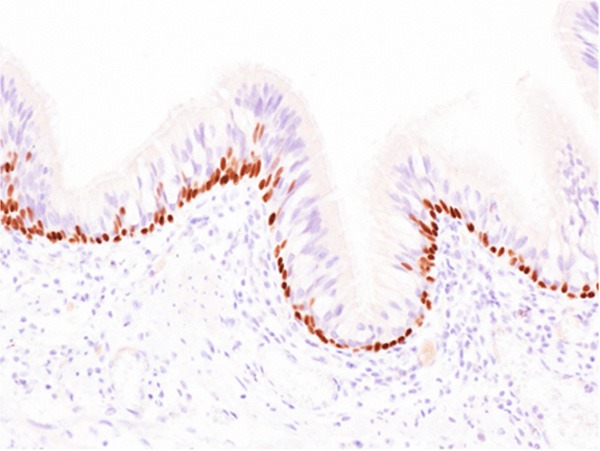
Immunohistochemical feature of the rectal submucosal tumor. p63-positive basal cells are present in the pseudostratified ciliated epithelium. x 200.
Accordingly, an ultimate diagnosis of ectopic respiratory mucosa in the rectum was made.
In this report, we describe the second documented case of ectopic respiratory mucosa in the rectum. In 2007, Kawahara et al. reported the first case of this type of lesion [10]. They reported a case of a 50-year-old Japanese female with a small submucosal tumor, measuring 13 x 12 mm, in the rectum accompanied by a Bormann type 1 rectal carcinoma [10]. The submucosal tumor was composed of branching tubular structures lined by pseudostratified ciliated epithelium and respiratory seromucinous glands [10]. There were smooth muscle bundles around the tubular structures [10]. Although their case contained both ciliated bronchial epithelium and seromucinous glands [10], the present case had only a ciliated bronchial epithelial component, and no seromucinous component was observed, thus, this is the first case of ectopic bronchial epithelium without seromucinous component in the rectum.
There have been only a few reports of ectopic salivary and pancreatic tissues in the rectum [4-9] although ectopic gastric mucosa is not an extraordinarily uncommon lesion [1-3]. Only four cases of ectopic salivary gland in the rectum have been documented [1,4,5,7]. Two of these four cases had both gastric mucosa and salivary tissue [1,4], and the remaining two cases contained only salivary tissue [5,7]. Gugulski et al. reported the first case of ectopic pancreas in the rectum [8], and only a few additional cases have been documented since the first report [9,16].
The histogenesis of ectopic tissue in the rectum remains unclear although some have proposed that ectopic gastric mucosa is found in the rectum due to the fact that the primitive intestinal tract is lined by cells that have the capacity to differentiate into a variety of epithelial types present at all levels of the gastrointestinal tract [5,6]. However, this does not explain the presence of salivary tissue in the rectum because it is endodermal in origin. Therefore, Weitzner speculated that during early embryogenesis some stem cells of the salivary gland evaded primary induction and migrated to the rectum, where a specific stimuli or a change in the milieu of the submucosa triggered their differentiation into salivary tissue [5]. Moreover, Downs-Kelly et al. also reported a case of ectopic salivary gland in the rectum and they speculated that this lesion may be a form of metaplasia or a developmental abnormality in which undifferentiated stem cells migrate to the rectum and then differentiate into salivary gland tissue [7]. The histogenesis of ectopic respiratory mucosa in the rectum also remains unclear. However, the concept of “foregut heterotopia” has been proposed, which suggests that ectopic respiratory mucosa in the rectum may result from developmental failure of the descent of the foregut, adhesion of ectoderm in 3- to 4- week old embryo, differentiation error of fetal rectal endodermal cells, or proliferation of pluripotential cells [10].
Cutaneous ciliated cyst is a rare benign skin lesion, which is characterized histopathologically by the presence of cuboidal to columnar or focally pseudostratified ciliated epithelium in the dermis or subcutis [17]. This lesion is commonly found in the lower extremities of young females and typically occurs in the postpubertal period [17]. Therefore, the müllerian hypothesis regarding the development of cutaneous ciliated cyst has been proposed [17]. According to this theory, sequestration and migration of müllerian rests occur during early embryogenesis. Bivin et al. revealed that the ciliated epithelium of cutaneous ciliated cyst resembles that of fallopian tubes and estrogen and progesterone receptors are strongly expressed in the ciliated epithelium of this type of lesion [17]. This suggests that hormonal stimulation contributes to the development of this lesion [17]. However, only rare cases of cutaneous ciliated cyst occurring in males have been reported [18], and thus, a hypothesis of ciliated metaplasia of eccrine or apocrine glands has also been proposed. This report is the first to demonstrate that estrogen and progesterone receptors are not expressed in the ectopic ciliated epithelium of the rectum; analysis of these hormone receptors was not performed in the first reported case of ectopic respiratory mucosa in the rectum [10]. Therefore, this indicated that the müllerian hypothesis is not associated with the occurrence of ectopic respiratory epithelium in the rectum.
Further, albeit extremely rare, adenocarcinoma arising from ectopic tissue in the rectum has been documented [16]. Goodarzi et al. reported the first case of invasive adenocarcinoma arising from ectopic pancreatic tissue in the rectum [16]. In their case, the ectopic pancreatic tissue had exocrine acini and small ducts without islets and the focal area with ducts had micropapillary architecture and mild to severe cytologic atypia reminiscent of pancreatic intraepithelial neoplasia, which suggested the origin of the invasive adenocarcinoma [16]. Moreover, a case of pyloric gland adenoma arising from the ectopic gastric mucosa in the rectum has also been documented [19]. Therefore, albeit extremely rare, occurrence of neoplastic lesions must be considered when ectopic tissues are found in the rectum.
Disclosure of conflict of interest
None.
References
- 1.Wolff M. Heterotopic gastric epithelium in the rectum: a report of three new cases with a review of 87 cases of gastric heterotopia in the alimentary canal. Am J Clin Pathol. 1971;55:604–616. doi: 10.1093/ajcp/55.5.604. [DOI] [PubMed] [Google Scholar]
- 2.Steele SR, Mullenix PS, Martin MJ, Ormseth E, Weppler E, Graham J, Place RJ. Heterotopic gastric mucosa of the anus: a case report and review of the literature. Am Surg. 2004;70:715–719. [PubMed] [Google Scholar]
- 3.Limidi JK, Sapundzieski M, Chakravarthy R, George R. Gastric heterotopia in the rectum. Gastrointest Endosc. 2010;72:190–191. doi: 10.1016/j.gie.2010.01.045. [DOI] [PubMed] [Google Scholar]
- 4.Shindo K, Bacon HE, Holmes EJ. Ectopic gastric mucosa and glandular tissue of a salivary type in the anal canal concomitant with a diverticulum in hemorrhoidal tissue: report of a case. Dis Colon Rectum. 1972;15:57–62. doi: 10.1007/BF02587671. [DOI] [PubMed] [Google Scholar]
- 5.Weitzner S. Ectopic salivary gland tissue in submucosa of rectum. Dis Colon Rectum. 1983;26:814–817. doi: 10.1007/BF02554758. [DOI] [PubMed] [Google Scholar]
- 6.Srinivasan R, Loewenstine H, Mayle JE. Sessile polypoid gastric heterotopia of rectum: a report of 2 cases and review of the literature. Arch Pathol Lab Med. 1999;123:222–224. doi: 10.5858/1999-123-0222-SPGHOR. [DOI] [PubMed] [Google Scholar]
- 7.Downs-Kelly E, Hoschar AP, Prayson RA. Salivary gland heterotopia in the rectum. Ann Diagn Pathol. 2003;7:124–126. doi: 10.1053/adpa.2003.50017. [DOI] [PubMed] [Google Scholar]
- 8.Gugulski A, Regula J, Orlowska J, Butruk E. Heterotopic pancreas in the rectum. Endoscopy. 1994;26:372. doi: 10.1055/s-2007-1009001. [DOI] [PubMed] [Google Scholar]
- 9.Yamagishi H, Fukui H, Tomita S, Ichikawa K, Imura J, Ishizuka M, Kubota K, Fujimori T. Ectopic gastric mucosa and pancreatic ducts in the rectum. Intern Med. 2011;50:1587–1589. doi: 10.2169/internalmedicine.50.5252. [DOI] [PubMed] [Google Scholar]
- 10.Kawahara K, Mishima H, Nakamura S. Heterotopic respiratory mucosa in the rectum: a first case report. Virchows Arch. 2007;451:977–980. doi: 10.1007/s00428-007-0510-8. [DOI] [PubMed] [Google Scholar]
- 11.Ishida M, Iwai M, Yoshida K, Kagotani A, Okabe H. Sebaceous carcinoma associated with Bowen’s disease: a case report with emphasis on the pathogenesis of sebaceous carcinoma. Int J Clin Exp Pathol. 2013;6:3029–3032. [PMC free article] [PubMed] [Google Scholar]
- 12.Toriyama A, Ishida M, Amano T, Nakagawa T, Kaku S, Iwai M, Yoshida K, Kagotani A, Takahashi K, Murakami T, Okabe H. Leiomyomatosis peritonealis disseminata coexisting with endometriosis within the same lesions: a case report with review of the literature. Int J Clin Exp Pathol. 2013;6:2949–2954. [PMC free article] [PubMed] [Google Scholar]
- 13.Ishida M, Hodohara K, Yoshida K, Kagotani A, Iwai M, Yoshii M, Okuno K, Horinouchi A, Nakanishi R, Harada A, Yoshida T, Okabe H. Occurence of anaplastic large cell lymphoma following IgG4-related autoimmune pancreatitis and cholecystitis and diffuse large B-cell lymphoma. Int J Clin Exp Pathol. 2013;6:2560–2568. [PMC free article] [PubMed] [Google Scholar]
- 14.Ishida M, Yoshida K, Kagotani A, Iwai M, Yoshii M, Okuno K, Horinouchi A, Nakanishi R, Harada A, Yoshida T, Okuno T, Hodohara K, Okabe H. Anaplastic lymphoma kinase-positive large B-cell lymphoma: A case report with emphasis on the cytological features of the pleural effusion. Int J Clin Exp Pathol. 2013;6:2631–2635. [PMC free article] [PubMed] [Google Scholar]
- 15.Ishida M, Hodohara K, Yoshii M, Okuno H, Nakanishi R, Horinouchi A, Nakanishi R, Harada A, Iwai M, Yoshida K, Kagotani A, Yoshida T, Okabe H. Methotrexate-related Epstein-Barr virus-associated lymphoproliferative disorder occurring in the gingiva of a patient with rheumatoid arthritis. Int J Clin Exp Pathol. 2013;6:2237–2241. [PMC free article] [PubMed] [Google Scholar]
- 16.Goodarzi M, Rashid A, Maru D. Invasive ductal adenocarcinoma arising from pancreatic heterotopia in rectum: case report and review of literature. Hum Pathol. 2010;41:1809–1813. doi: 10.1016/j.humpath.2010.06.005. [DOI] [PubMed] [Google Scholar]
- 17.Bivin WW Jr, Heath JE, Drachenberg CB, Strauch ED, Papadimitriou JC. Cutaneous ciliated cyst: a case report with focus on mullerian heterotopia and comparison with eccrine sweat glands. Am J Dermatopathol. 2010;32:731–734. doi: 10.1097/DAD.0b013e3181d43f01. [DOI] [PubMed] [Google Scholar]
- 18.Santos LD, Mendelsohn G. Perineal cutaneous ciliated cyst in a male. Pathology. 2004;36:369–370. doi: 10.1080/00313020410001721618. [DOI] [PubMed] [Google Scholar]
- 19.Vieth M, Kushima R, de Jonge JP, Borchard F, Oelling F, Stolte M. Adenoma with gastric differentiation (so-called pyloric gland adenoma) in heterotopic gastric corpus mucosa in the rectum. Virchows Arch. 2005;446:542–545. doi: 10.1007/s00428-005-1242-2. [DOI] [PubMed] [Google Scholar]