

Abstract
Background:
Direct carotid cavernous fistula (CCF) secondary to ruptured carotid cavernous aneurysms (CCAs) is rare, but patients with this condition who develop acutely worsening and severe neuro-ophthalmic symptoms require urgent treatment. Endovascular methods are the first-line option, but this modality may not be available on an urgent basis.
Case Description:
In this article, we report a 45-year-old female with severe direct CCF due to rupture of the CCA. She presented with intractable headache and acute worsening of double vision and visual acuity. Emergent radiographic study revealed high-flow fistula tracked from the CCA toward the contralateral cavernous sinus and drained into the engorged left superior orbital vein. To prevent permanent devastating neuro-ophthalmic damages, urgent high-flow bypass with placement of a radial artery graft was performed followed by right cervical internal carotid artery (ICA) ligation and the clipping of the ICA at the C3 portion, proximal to the ophthalmic artery. In the immediate postoperative period, her symptoms resolved and angiography confirmed patency of the high-flow bypass and complete occlusion of the CCF.
Conclusion:
With due consideration of strategy and techniques to secure safety, open surgical intervention with trapping and bypass is a good treatment option for direct severe CCF when the endovascular method is not available, not possible, or is unsuccessful.
Keywords: Carotid cavernous aneurysm, carotid cavernous fistula, high-flow bypass, intracranial aneurysm
INTRODUCTION
Among all types of carotid cavernous fistulas (CCFs), especially direct CCF by carotid cavernous aneurysm (CCA) rupture sometimes requires urgent treatment due to acute cranial nerve and visual impairment, epistaxis, and, most devastatingly, subarachnoid hemorrhage.[2,7,9,10,13] Fistula occlusion via an endovascular approach is the treatment of choice, however, endovascular management is not always available on an urgent basis and is not always successful, in which case direct surgical trapping of the lesion and distal bypass might be indicated. The present report describes the case of a relatively young patient with severe direct CCF caused by rupture of a large CCA with acute worsening of ophthalmic symptoms. This patient was treated with urgent open surgical trapping of ruptured CCA in conjunction with high-flow bypass using a radial artery (RA) graft, and fairy good result was obtained.
CASE REPORT
History and examination
A 45-year-old female presented to our hospital with rapidly progressive double vision. She had a history of a right CCA (15 mm in diameter) [Figure 1] that was diagnosed at our hospital 5 years earlier when she presented with transient right third nerve palsy. She had been treated with strict blood pressure control in our outpatient clinic without recurrence of symptoms. Annual magnetic resonance (MR) imaging had not shown any morphological change in the aneurysm. Seventeen days before the present admission, she experienced onset of acute intractable headache accompanied by a “swishing sound” in the right side of her head, which worsened gradually and which was not responsive to analgesics. Three days prior to admission, her headache subsided abruptly, and she developed double vision and worsening visual acuity of her left eye. On admission, she was distressed. Neurological examination revealed left third nerve palsy, left ocular bruit, left chemosis, slight left exophthalmos, and subjective reduction in visual acuity in the left eye. Ophthalmologic examination showed reduced visual acuity in the left eye (20/67) when compared with the right eye (20/50). Computed tomography and MR imaging revealed a remarkable enlargement of the left superior orbital vein (SOV), and cerebral angiography confirmed direct CCF caused by CCA rupture. The fistula tracked toward the contralateral (left) cavernous sinus and drained into the left SOV [Figure 2a–c]. Given the acutely worsening neuro-ophthalmologic symptoms as well as the robust direct CCF with the resultant engorged left SOV, urgent treatment was indicated to prevent devastating permanent neuro-ophthalmologic deficits. Endovascular treatment was not available on an urgent basis at our hospital. Given her young age and her stable systemic condition, we elected to proceed with open surgical trapping of the aneurysm in conjunction with high-flow bypass using a RA graft after obtaining informed consent.
Figure 1.
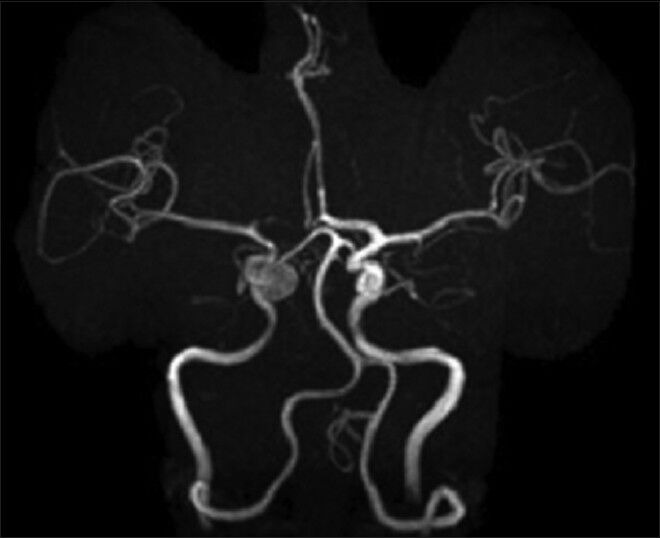
MR angiography performed 5 years before admission revealed a right carotid cavernous aneurysm (15 mm in diameter)
Figure 2.
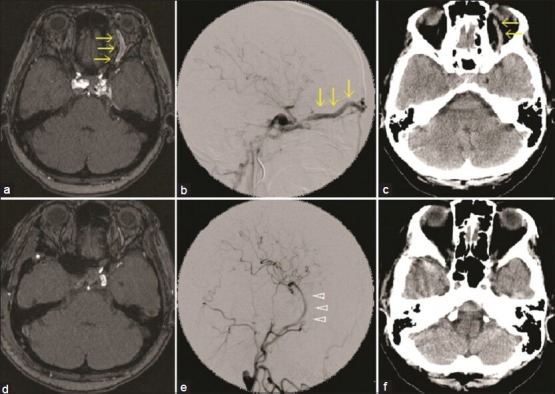
On the day of admission, MR imaging (a), right carotid angiogram (b), and CT (c) revealed an engorged right SOV (yellow arrows) due to direct CCF secondary to ruptured right CCA. Postoperatively, MR imaging (d), right carotid angiogram (e) and CT (f) revealed disappearance of the engorged SOV and no sign of CCF. White arrowheads indicate the patent radial artery graft
Operation
Standard neuroanesthesia with somatosensory evoked potentials (SSEP) of the left extremities was induced. With right cervical carotid bifurcation exposure, a curvilinear fronto-temporal skin incision was made, and the superficial temporal artery (STA) was meticulously prepared under a microscope. The RA graft was harvested concurrently by another surgeon. A fronto-temporal craniotomy was performed, and a subzygomatic tunnel was made for the RA graft. The Sylvian fissure was fully split under microscope, and the M1, M2, and M3 portions of the middle cerebral artery (MCA) and the supraclinoidal internal carotid artery (ICA) were exposed. First, an “insurance” STA-M4 bypass was made distal to the M2 portion for RA graft anastomosis.[3] Then, the harvested RA graft was gently pulled through the subzygomatic tunnel. The distal end of the RA graft was anastomosed to the M2 (inferior trunk) of the MCA, and the proximal end was anastomosed to the external carotid artery (ECA). The patency of the anastomosis was confirmed with microvascular Doppler assessment, and the right cervical ICA was then clamped. At this stage, due to bleeding from the cavernous sinus, we incompletely trapped the aneurysm to control the bleed by clipping the ICA just distal to the origin of the ophthalmic artery, leaving only retrograde flow from the ophthalmic artery into the cavernous aneurysm. Then, extradural anterior clinoidectomy was performed. We exposed the ICA proximal to the ophthalmic artery as well as the distal dural ring, and some bleeding from the cavernous sinus was controlled with packing with Gelfoam. The C3 portion of the ICA was finally clipped [Figure 3]. Microvascular Doppler exploration through the lateral wall of the cavernous sinus did not detect any flow signal. We also confirmed anterograde flow into the ophthalmic artery via retrograde ICA flow provided by the RA graft. Significant SSEP change was not observed at all throughout the operation.
Figure 3.
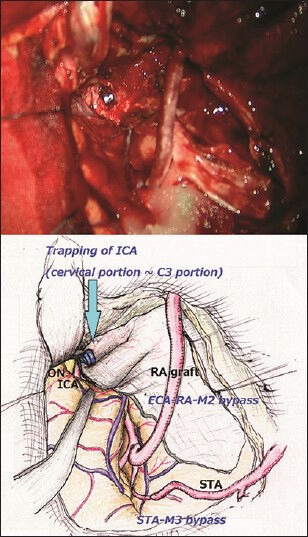
The upper picture is the final view of operation and the lower is its illustration. After removing the anterior clinoid process and opening the cavernous sinus, internal carotid artery was able to be trapped between cervical and C3 portion and the ruptured aneurysm got isolated from the circulation. Flow of the ipsilateral ICA was replaced with that of the ECA-RA-M2 bypass. The “insurance” STA-M3 bypass was performed to minimize ischemic damages during the RA-M2 bypass procedure
Postoperative course
Immediately after the operation, auscultation over the left eye confirmed disappearance of the ocular bruit. Furthermore, chemosis and exophthalmos resolved. Postoperative angiography confirmed patency of the high-flow bypass and complete occlusion of the CCF. MR imaging revealed no significant cerebral infarction in the revascularized distal right ICA area and showed marked shrinkage of the formerly engorged left SOV [Figure 2d–f]. An examination by an experienced ophthalmologist confirmed total resolution of the deficits. The patient returned to her daily life without any permanent neurological sequelae.
DISCUSSION
This technical case report shows a successful urgent surgical repair of severe direct CCF due to ruptured CCA of relatively young female patient.
CCAs are relatively benign lesions and are associated with an extremely low risk of fatal subarachnoid hemorrhage when compared with intracranial aneurysms.[9] This low risk of subarachnoid hemorrhage is due to the extracranial location of CCAs and to the hard surrounding structure of the cavernous sinus dura. Unruptured CCAs can result in symptoms such as diplopia, ptosis, facial pain, and loss of visual acuity due to a mass effect causing compression to the cranial nerves.[9,13] Rupture of CCA results in direct CCF causing severe neuro-ophthalmological symptoms. Furthermore, CCA rupture can cause intracerebral hemorrhage due to cortical venous drainage or subarachnoid hemorrhage if the aneurysm ruptures into the subarachnoid space, thereby disrupting the normal confines of the cavernous sinus dura.[2,7,9,10,13] In general, direct CCFs due to ruptured CCAs progress rapidly and require urgent treatment. Progressive visual decline, papilledema, and refractory elevation of the intraocular pressure are all indications for emergent intervention.[1]
The goal of CCF treatment is to completely occlude the fistula while simultaneously preserving normal blood flow through the ICA. Endovascular embolization of the fistula is now the first-line treatment modality.[1] However, reopening and enlargement of a coiled aneurysm may occur, or the excessive packing of coiling material into the cavernous sinus might aggravate visual symptoms. Sometimes, sacrifice of ICA itself is required to achieve hemostasis, which may bring unexpected ischemic complications. Even after confirmation of ischemic tolerance in response to abrupt ICA occlusion by the balloon occlusion test, ICA sacrifice without distal revascularization might cause de novo contralateral CCA formation or ruptured anterior communication aneurysm in the long term due to chronic hemodynamic stress.[11] Covered stents or a flow diverter with embolic material into the aneurysm might initially demonstrate dramatic results with ICA preservation, but delayed thrombosis remains a problem with currently available stents. Therefore, in cases in which endovascular treatment is not possible or is unsuccessful, open surgical intervention may be warranted.[1]
As for the open surgical approaches, direct clipping of CCAs is extremely challenging, given the complex surrounding structures. For example, it is nearly impossible to avoid manipulating/injuring the cranial nerves when creating a direct surgical corridor for aneurysm clipping. In addition, lengthy temporal occlusion and multiple complex clipping are necessary for direct clipping of such aneurysms, leading to a risk of devastating distal ischemia. In contrast, distal bypass with parent vessel occlusion can completely exclude the aneurysms from the circulation, promptly inducing thrombosis inside aneurysms, and can be performed with predictable ischemia time and a relatively low complication rate, obviating the dangers associated with direct complex aneurysm manipulation.[14]
Although high-flow bypass procedure is regarded as complex and technically challenging, various previous studies have demonstrated its relative safety, excellent long-term graft patency, as well as acceptable morbidity and mortality rates.[4,6,8,12,14] We routinely use the supportive STA-M4 bypass before the RA-M2 anastomosis. Although the use of supportive STA-M4 bypass could be still controversial and might increase the total time of the operation, it would be useful to alleviate major ischemia during cross clamping of proximal large vessel and resultant possible reperfusion injury.[3,5,6] In addition, it can be utilized to confirm and monitor appropriate high flow bypass function by evaluating the arterial pressure of the graft through the pressure transducer inserted in another branch of the STA during ICA sacrifice and restoration of high-flow bypass.[5,6] The great benefit of direct surgical repair is, as shown in the present case, that trapping of the aneurysm can successfully occlude the aneurysm and fistula without causing any mass effect, leading to immediate decrease of intracavernous sinus pressure, which results in rapid and complete resolution of neuro-ophthalmic symptoms.
Although the unavailability of urgent endovascular methods was the main reason for direct surgical intervention in the present case, other reasons to consider direct surgical intervention include the possible disadvantages of endovascular methods and the effectiveness, safety, and durability of open surgical treatment, particularly in stable and/or young patients. However, this is just a case report and further research is needed to validate the conditions in which these respective approaches should be optimally used.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2014/5/1/49/130772
Contributor Information
Hirotaka Hasegawa, Email: ayhi_hase_dani@yahoo.co.jp.
Tomohiro Inoue, Email: t.inoue.fujinsu@beige.plala.or.jp.
Akira Tamura, Email: tamura.nsu@umin.ac.jp.
Isamu Saito, Email: saito-kyr@umin.ac.jp.
REFERENCES
- 1.Ellis JA, Goldstein H, Connolly ES, Jr, Meyers PM. Carotid-cavernous fistulas. Neurosurg Focus. 2012;32:E9. doi: 10.3171/2012.2.FOCUS1223. [DOI] [PubMed] [Google Scholar]
- 2.Hodes JE, Fletcher WA, Goodman DF, Hoyt WF. Rupture of cavernous carotid artery aneurysm causing subdural hematoma and death. J Neurosurg. 1988;69:617–9. doi: 10.3171/jns.1988.69.4.0617. [DOI] [PubMed] [Google Scholar]
- 3.Hongo K, Horiuchi T, Nitta J, Tanaka Y, Tada T, Kobayashi S. Double-insurance bypass for internal carotid artery aneurysm surgery. Neurosurgery. 2003;52:597–602. doi: 10.1227/01.neu.0000047892.12003.58. [DOI] [PubMed] [Google Scholar]
- 4.Houkin K, Kamiyama H, Kuroda S, Ishikawa T, Takahashi A, Abe H. Long- term patency of radial artery graft bypass for reconstruction of the internal carotid artery. Technical note. J Neurosurg. 1999;90:786–90. doi: 10.3171/jns.1999.90.4.0786. [DOI] [PubMed] [Google Scholar]
- 5.Ishikawa T, Kamiyama H, Kobayashi N, Tanikawa R, Takizawa K, Kazumata K. Experience from “double-insurance bypass.” Surgical results and additional techniques to achieve complex aneurysm surgery in a safer manner. Surg Neurol. 2005;63:485–90. doi: 10.1016/j.surneu.2004.10.014. [DOI] [PubMed] [Google Scholar]
- 6.Ishishita Y, Tanikawa R, Noda K, Kubota H, Izumi N, Katsuno M, et al. Universal extracranial-intracranial graft bypass for large or giant internal carotid aneurysms: Techniques and results in 38 consecutive patients. World Neurosurg. 2013 doi: 10.1016/j.wneu.2013.02.063. [In press, DOI: 10.1016/j.wneu.2013.02.063] [DOI] [PubMed] [Google Scholar]
- 7.Jiamsripong P, Mookadam M, Mookadam F. An uncommon cause of Epistaxis: Cartoid Cavernous Fistula. Emerg Med J. 2007;24:e28. doi: 10.1136/emj.2006.045195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kalani MY, Zabramski JM, Hu YC, Spetzler RF. Extracranial-intracranial bypass and vessel occlusion for the treatment of unclippable giant middle cerebral artery aneurysms. Neurosurgery. 2013;72:428–36. doi: 10.1227/NEU.0b013e3182804381. [DOI] [PubMed] [Google Scholar]
- 9.Kupersmith MJ, Hurst R, Berenstein A, Choi IS, Jafar J, Ransohoff J. The benign course of cavernous carotid artery aneurysms. J Neurosurg. 1992;77:690–3. doi: 10.3171/jns.1992.77.5.0690. [DOI] [PubMed] [Google Scholar]
- 10.McLaughlin MR, Jho HD, Kwon Y. Acute subdural hematoma caused by a ruptured giant intracavernous aneurysm: Case report. Neurosurgery. 1996;38:388–92. doi: 10.1097/00006123-199602000-00032. [DOI] [PubMed] [Google Scholar]
- 11.Niiro M, Shimozuru T, Nakamura K, Kadota K, Kuratsu J. Long-term follow-up study of patients with cavernous sinus aneurysm treated by proximal occlusion. Neurol Med Chir (Tokyo) 2007;40:88–97. doi: 10.2176/nmc.40.88. [DOI] [PubMed] [Google Scholar]
- 12.Sekhar LN, Bucur SD, Bank WO, Wright DC. Venous and arterial bypass grafts for difficult tumors, aneurysms, and occlusive vascular lesions: Evolution of surgical treatment and improved graft results. Neurosurgery. 1999;44:1207–23. doi: 10.1097/00006123-199906000-00028. [DOI] [PubMed] [Google Scholar]
- 13.Stiebel-Kalish H, Kalish Y, Bar-On RH, Setton A, Niimi Y, Berenstein A, et al. Presentation, natural history, and management of carotid cavernous aneurysms. Neurosurgery. 2005;57:850–7. doi: 10.1227/01.neu.0000179922.48165.42. [DOI] [PubMed] [Google Scholar]
- 14.Sughrue ME, Saloner D, Rayz VL, Lawton MT. Giant intracranial aneurysms: Evolution of management in a contemporary surgical series. Neurosurgery. 2011;69:1261–71. doi: 10.1227/NEU.0b013e31822bb8a6. [DOI] [PMC free article] [PubMed] [Google Scholar]