

Abstract
Background:
Healthy teeth and oral tissues and the need for oral health care are important for any section of society. Dental caries is an infectious microbial disease of multifactorial origin in which diet, host, and microbial flora interacts over a period of time in such a way so as to encourage demineralization of the tooth enamel with resultant caries formation. Dental caries, the product of man's progress towards civilization, has a very high morbidity potential and thus, is coming into focus of the mankind.
Aims and Objectives:
To assess the prevalence of dental caries among 12-15 year old government and private school children of Bharatpur city.
Materials and Methods:
This was a cross-sectional study carried out on total 1400 school children, of which 700 school children were from government schools and 700 were from private schools. Simple random sampling methodology was used to select the sample. The subjects were examined for dental caries according to WHO 1997 assessment form. Significant Caries Index was also used to assess the prevalence of dental caries.
Results:
The prevalence of dental caries was found higher among government school children, that is, 53%, when compared to private school children, that is, 47% and this difference was found to be statistically significant. The mean decayed, missing, and filled teeth were found to be higher in government school children (7.61 ± 2.86) as compared to private school children (4.76 ± 2.42).
Conclusion:
Dental caries was found to be the major public health problems among both the government and private school children of Bharatpur city, which need immediate attention. Regular dental checkups and practice of routine oral hygiene procedures will enable them to lead a healthier life.
Keywords: Dental caries, school children, Significant Caries Index
INTRODUCTION
Oral health is an important component of general health, with dental caries affecting a person's ability to eat, speak or socialize.[1] Dental caries is an infectious microbial disease of multifactorial origin in which diet, host, and microbial flora interacts over a period of time in such a way so as to encourage demineralization of the tooth enamel with resultant caries formation. Dental caries, the product of man's progress toward civilization, has a very high morbidity potential and thus, is coming into focus of the mankind.[2] The caries experience varies greatly among countries and even within small regions of countries. It varies with age, and sex, socioeconomic conditions, ethnicity, diet, medical conditions of the patient, oral hygiene practices, etc., and even within oral cavity all the teeth and surfaces are not equally susceptible to caries.[3] It not only causes pain and discomfort, but also in addition, leads to a financial burden. The prevention of dental caries has long been considered as an important task for the health professionals. Scientists are continuing their research in identifying the best practices for diagnosis, treatment, and prevention of dental caries. Previous methods for the treatment of dental caries in a surgical manner has being replaced by newer strategies that emphasize disease prevention and conservation of tooth structure.[4] Voluminous literature exists on the status of the dental caries in the Indian population. It has been observed that in 1940 the prevalence of dental caries in India was 55.5%, and in 1960 it was reported to be 68%. Overall the general impression is that dental caries has increased in prevalence and severity in urban and cosmopolitan population since last two decades. However, there is no definite picture as yet regarding the disease status in rural and backward areas of country in the comparison where 80% of the population inhabits.[4,5] A very extensive and comprehensive National Health Survey conducted in 2004 throughout India has shown dental caries prevalence as follows: 51.9% in 5-year-old children, 53.8% in 12-year-old children and 63.1% in 15-year-old teenagers. The report concluded that a preventive program, such as water fluoridation, should be started to address this national crisis in dental caries.[6]
The scenario is different in developed countries where in recent years rapid changes have occurred in the prevalence of oral diseases. In the past decade, a substantial decline in dental caries has occurred among children of several developed countries mainly USA and several European countries.[7,8] Fluoride has been recognized as one of the most influential factor responsible for the observed decline of caries among children as well as adults of these countries.
The Bharatpur city comes under Bharatpur block which in turn comes under Bharatpur tehsil of Bharatpur district in the state of Rajasthan.[9] Since, no study showing the prevalence of dental caries has been done in this region and to recommend various preventive measures the present study was undertaken to know the prevalence of dental caries among 12-15 years old school children of Bharatpur city.
MATERIALS AND METHODS
A cross-sectional study was carried out in Bharatpur city to assess the prevalence of dental caries among school children in the age group of 12-15 years. List of schools was obtained from Bharat Shiksha Adhikari Office of Bharatpur, which comprised of 200 schools present in Bharatpur city, making a population of 105,000. Of these 105,000 students, 25,000 students of age group 12-15 years were included in the study.[10]
A pilot study was carried out in order to test the feasibility and the sample size was estimated to be 1400 school children (700 governments and 700 privates). The Bharatpur city had been divided into five zones, that is, central, north, south, east, and west. Areas representing each zone were New Mandi Chauraha, Ranjeet Nagar, Gopalgarh road, Kumher Gate and Surajpol Gate respectively. Zone I, that is, New Mandi Chauraha (central zone) had 40 schools, Zone II, that is, Ranjeet Nagar (north) had 52 schools, Zone III, that is, Gopalgarh road (south zone) had 35 schools, Zone IV, that is, Kumher Gate (east zone) had 35 schools and Zone V, that is, Surajpol (west zone) had 38 schools.
To obtain the total sample size of 1400, 280 school children from each of the five zones were randomly selected out of which 140 school children were from government schools and 140 were from private schools. Selection of schools from each zone had been done using simple random sampling (lottery) method (280 × 18 = 1400). The structured pretested proforma was used to assess dental caries in the school children of Bharatpur city that included information related to gender, age and brushing frequency. Clinical examinations included dental caries examination using WHO standard criteria as mentioned in WHO Oral Health Proforma, 1997[11] and Significant Caries Index (SiC) was also used to assess the prevalence of dental caries.[12] The clinical examination was carried out by a trained examiner who was initially trained in the Department of Public Health Dentistry. He was supervised by an expert clinician and 96% agreement (k = 0.96) was found in their results. The ethical clearance was approved from the Ethical Committee of K.D. Dental College and Hospital, Mathura prior to the start of the study and consent was obtained from school authorities as well as from parents of school children. The inclusion and exclusion criteria were as follows.
Inclusion criteria
School children aged 12-15 years
School children who were residents of Bharatpur city (lifelong).
Exclusion criteria
Individuals suffering from systemic illness
Individuals who were not willing to participate in the study
Individuals with orthodontic brackets and with severe extrinsic stains on their teeth.
The statistical analysis was performed using SPSS version 15(IBM Corporation). The mean and standard deviation of scores were calculated, comparison between government and private school children was done using Chi-square test, P ≤ 0.05 was considered as statistically significant.
RESULTS
A cross-sectional study was carried out in Bharatpur city to assess the prevalence of dental caries among school children in the age group of 12-15 years. The distribution of study population according to gender, age, brushing frequency and SiC are given in Tables 1–4.
Table 1.
Distribution of study population according to gender among government and private school children
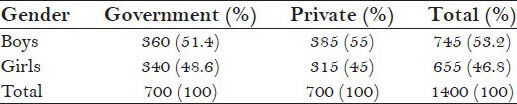
Table 4.
Distribution of study population according to significant caries index

Table 2.
Distribution of study population according to age among government and private school children
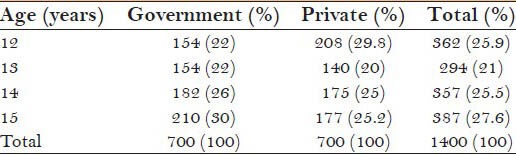
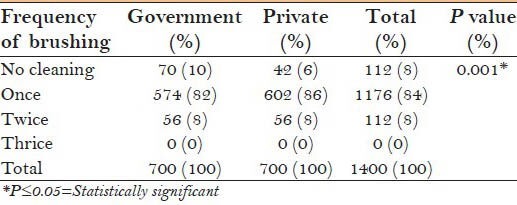
Table 3.
Distribution of study population according to frequency of brushing teeth among government and private school children
In this study, the mean decayed, missing, filled teeth (DMFT) among the government school children was higher, that is, 7.61 ± 2.86 when compared to private school children, that is, 4.76 ± 2.42 and a statistically significant difference, that is, P ≤ 0.05 (P = 0.000) was observed when dental caries among government and private school children was compared [Table 5]. The prevalence of dental caries was found higher among government school children, that is, 53%, when compared to private school children, that is, 47% and this difference was found to be statistically significant [Table 6].
Table 5.
Distribution of study population according to comparison of dental caries among government and private school children
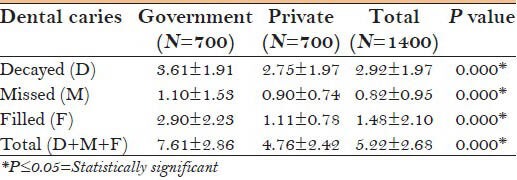
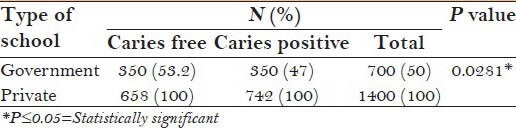
Table 6.
Distribution of study population according to comparison of dental caries with type of school
DISCUSSION
Healthy teeth and oral tissues and the need for oral health care are important for any section of society. Oral disorders can have a profound impact on the quality-of-life. Good oral health has real health gains, in that it can improve general health and quality-of-life and contribute to self-image and social interaction. Epidemiologic studies may be of value in assessing the prevalence of diseases, in disclosing trends in disease development, and in analyzing possible factors influencing the disease pattern.[13]
In this study, among the total 1400 (100%) study subjects, 745 (53.2%) were boys and 655 (46.8%) were girls. Among both government and private schools maximum school children were boys, that is, 360 (51.4%) and 385 (55%) respectively, which is in accordance to the study conducted by Adekoya-Sofowora et al.[14]
Maximum number of school children, that is, 387 (27.6%) were from the age group of 15 years which is in accordance with the study conducted by Pontigo-Loyola et al.[15] in which maximum number of school children belonged to the age group of 15 years, that is, 850 (55.3%).
In this study, a maximum number of children, that is, 1176 (84%) brushed once in a day. These results are in accordance with the study conducted by Shailee et al.[16] among both government and private school children in which also a maximum number of children, that is, 620 (52.9%) brushed once in a day.
In the total study population, 5.22 ± 2.68 was the mean DMFT. Among the government and private school children, 7.61 ± 2.86 and 4.76 ± 2.42 was the mean DMFT observed, respectively. In the study conducted by Wyne et al.[17] 2.92 ± 3.51 was the mean DMFT. Among the government and private school children, 2.85 ± 3.41 and 3.05 ± 3.72 was the mean DMFT observed, respectively.
In this study, 742 (100%) were caries positive, out of which 392 (53%) were government school children and 350 (47%) were private school children. In the study conducted by Piovesan et al.[18] of 141 (100%) caries positive school children, 86 (61%) were government school children and 55 (39%) were private school children.
ACKNOWLEDGMENT
This study was conducted independently and not sponsored by any outside body. The author would like to thank all participants for their valuable help and cooperation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Parker EJ, Jamieson LM. Oral health comparisons between children attending an Aboriginal health service and a Government school dental service in a regional location. Rural Remote Health. 2007;7:625. [PubMed] [Google Scholar]
- 2.Sudha P, Bhasin S, Anegundi RT. Prevalence of dental caries among 5-13-year-old children of Mangalore city. J Indian Soc Pedod Prev Dent. 2005;23:74–9. doi: 10.4103/0970-4388.16446. [DOI] [PubMed] [Google Scholar]
- 3.Saravanan S, Anuradha KP, Bhaskar DJ. Prevalence of dental caries and treatment needs among school going children of Pondicherry, India. J Indian Soc Pedod Prev Dent. 2003;21:1–12. [PubMed] [Google Scholar]
- 4.Moses J, Rangeeth BN, Gurunathan D. Prevalence of dental caries, socio-economic status and treatment needs among 5-15 year old school going children of Chidambaram. J Clin Diagn Res. 2011;5:146–51. [Google Scholar]
- 5.Dash JK, Sahoo PK, Bhuyan SK, Sahoo SK. Prevalence of dental caries and treatment needs among children of Cuttack (Orissa) J Indian Soc Pedod Prev Dent. 2002;20:139–43. [PubMed] [Google Scholar]
- 6.Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A pending public health crisis. Am J Dent. 2009;22:3–8. [PubMed] [Google Scholar]
- 7.Meyer-Lueckel H, Paris S, Shirkhani B, Hopfenmuller W, Kielbassa AM. Caries and fluorosis in 6- and 9-year-old children residing in three communities in Iran. Community Dent Oral Epidemiol. 2006;34:63–70. doi: 10.1111/j.1600-0528.2006.00258.x. [DOI] [PubMed] [Google Scholar]
- 8.Wondwossen F, Astrøm AN, Bjorvatn K, Bårdsen A. The relationship between dental caries and dental fluorosis in areas with moderate- and high-fluoride drinking water in Ethiopia. Community Dent Oral Epidemiol. 2004;32:337–44. doi: 10.1111/j.1600-0528.2004.00172.x. [DOI] [PubMed] [Google Scholar]
- 9.Initial Environmental Examination: Bharatpur Water Supply. [Last accessed on 2013 Sep 15]. Available from: http://www.ruidp.rajasthan.gov.in/Water%20 Supply%20Sub-project,%20Bharatpur%20pdf .
- 10.Kila Road, Bharatpur, Rajasthan: Department of Education; Basic Shiksha Adhikaari. [Google Scholar]
- 11.Oral Health Surveys-Basic Methods. 4th ed. Geneva: WHO; 1997. WHO. [Google Scholar]
- 12.Bratthall D. Introducing the significant caries index together with a proposal for a new global oral health goal for 12-year-olds. Int Dent J. 2000;50:378–84. doi: 10.1111/j.1875-595x.2000.tb00572.x. [DOI] [PubMed] [Google Scholar]
- 13.Olsson B. Dental caries and fluorosis in Arussi province, Ethiopia. Community Dent Oral Epidemiol. 1978;6:338–43. doi: 10.1111/j.1600-0528.1978.tb01175.x. [DOI] [PubMed] [Google Scholar]
- 14.Adekoya-Sofowora CA, Nasir WO, Oginni AO, Taiwo M. Dental caries in 12-year-old suburban Nigerian school children. Afr Health Sci. 2006;6:145–50. doi: 10.5555/afhs.2006.6.3.145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pontigo-Loyola AP, Medina-Solis CE, Borges-Yañez SA, Patiño-Marín N, Islas-Márquez A, Maupome G. Prevalence and severity of dental caries in adolescents aged 12 and 15 living in communities with various fluoride concentrations. J Public Health Dent. 2007;67:8–13. doi: 10.1111/j.1752-7325.2007.00001.x. [DOI] [PubMed] [Google Scholar]
- 16.Shailee F, Sogi GM, Sharma KR, Nidhi P. Dental caries prevalence and treatment needs among 12- and 15- Year old schoolchildren in Shimla city, Himachal Pradesh, India. Indian J Dent Res. 2012;23:579–84. doi: 10.4103/0970-9290.107330. [DOI] [PubMed] [Google Scholar]
- 17.Wyne AH, Al-Ghannam NA, Al-Shammery AR, Khan NB. Caries prevalence, severity and pattern in pre-school children. Saudi Med J. 2002;23:580–4. [PubMed] [Google Scholar]
- 18.Piovesan C, Pádua MC, Ardenghi TM, Mendes FM, Bonini GC. Can type of school be used as an alternative indicator of socioeconomic status in dental caries studies? A cross-sectional study. BMC Med Res Methodol. 2011;11:37. doi: 10.1186/1471-2288-11-37. [DOI] [PMC free article] [PubMed] [Google Scholar]