

Abstract
Study Objectives:
To evaluate a novel sleep education program for low-income preschool children and their families.
Design:
Randomized trial of an educational intervention.
Setting:
Community-based.
Participants:
Head Start preschool families (n = 152) in greater Lansing and Detroit, Michigan.
Interventions:
Classrooms or Head Start sites were randomized to an intervention group (prompt intervention) versus a control group (delayed intervention). Parents attended a one-time, 45-min sleep education program and preschoolers received 2 w (320 total min) of classroom sleep curriculum.
Measurements:
Parent knowledge, attitudes, self-efficacy, and beliefs were assessed as the primary outcomes just before the 45-min sleep intervention, immediately postintervention, and approximately 1 mo postintervention. Parents reported their child's bedtimes and wake times on 7-day sleep diaries at baseline and at 1-mo follow-up. Average weeknight sleep durations and bedtimes served as secondary outcomes.
Results:
Linear mixed models showed a time × treatment effect for parents' knowledge, attitudes, and self-efficacy (each P < 0.05) but not beliefs. These improvements were found immediately postintervention but were not retained at 1-mo follow-up. Children in the intervention group improved their weeknight sleep duration at 1-mo follow-up by 30 min (11.0 ± 0.9 h vs. 10.5 ± 1.0 hours at baseline) compared to controls (10.4 ± 0.9 h versus 10.5 ± 0.9 h at baseline) (P = 0.04 for difference between groups). Children did not show statistically significant improvements in bedtime.
Conclusions:
Educational interventions in early childhood can have an effect on parents' sleep knowledge, attitudes, and self-efficacy, and on children's sleep behavior. However, repeated exposure to the new information may be important for parents as well as their children.
Citation:
Wilson KE, Miller AL, Bonuck K, Lumeng JC, Chervin RD. Evaluation of a sleep education program for low-income preschool children and their families. SLEEP 2014;37(6):1117-1125.
Keywords: bedtimes, curriculum, education, health behavior, intervention, preschool children, sleep, sleep duration, socioeconomic status
INTRODUCTION
Children require adequate sleep duration for optimal health, growth, and development,1 and meta-analytic data confirm the adverse effect of insufficient sleep on cognition and behavior.2 Preschoolers, generally age 3 to 5 y, are often reported to have insufficient sleep duration,3,4 which in turn is associated with limited parental knowledge about children's sleep needs.5 Lack of knowledge about children's sleep is common among parents, as 50–75% incorrectly estimate how much sleep children require.5–7 Parents need education about sleep, particularly when their children are young and the parents have complete control over sleep schedules. Tested interventions have increased children's knowledge about sleep8–13 and improved children's self-reported sleep behaviors,14–18 but these studies have included only school-age children or adolescents. To our knowledge, no published study has examined the effect of a sleep education program on the sleep of preschool-age children.
This report describes results from a randomized controlled study of a sleep education program targeted at preschool-age children and parents, in this case, participants in Head Start. Head Start provides early care and education, in addition to health and social services, to more than one million low-income children in the United States. Low-income infants15 and children3,4 are particularly likely to obtain insufficient sleep. The sleep education program, entitled “Sweet Dreamzzz Early Childhood Sleep Education Program”,” that we studied was developed by a Detroit area nonprofit organization, Sweet Dreamzzz Inc., that aims to improve sleep for children who live in low-income neighborhoods (see http://www.sweetdreamzzz.org/). The educational program involved a 2-w classroom curriculum for children and a 45-min (one-time) presentation for parents. Our research questions were: (1) Does the educational program improve parents' knowledge immediately after the presentation and at 1-month follow-up? and (2) Does the educational program cause sleep behaviors to improve, as demonstrated by longer nighttime sleep duration and earlier bedtimes?
METHODS
Study Setting
This study was conducted in the greater Lansing area (n = 7 Head Start sites) and in Detroit, Michigan (n = 6 sites). Lansing sites provided a predominantly white clientele in a rural setting with half-day Head Start programs, which did not include a daytime nap during the school day. In contrast, the urban Detroit sites served a predominantly black clientele and the majority of classes were full-day programs that did incorporate a daytime nap into the school day. The study was performed at the Lansing sites in the winter (January and February 2012) and at the Detroit sites in the fall (October and November 2012). The protocol was approved by the University of Michigan Institutional Review Board. Parents who attended the presentation—offered by Sweet Dreamzzz and Head Start, independent of the research protocol, to all families in the school—and in addition chose to participate in the research, signed written informed consents on site. Sites for this research were chosen solely by Sweet Dreamzzz, based on responses to inquiries with state of Michigan Head Start programs. Head Start centers in southeast Michigan were selected based on staff interest and desire to pilot this newly developed and potentially beneficial educational program, along with the associated research opportunity for interested participants.
Randomization
Limitations on the number of families that Sweet Dreamzzz could effectively plan to assist at the same time offered a natural opportunity for a randomized controlled design (Figure 1). Classrooms (in Lansing) or building sites with two to six classrooms each (in Detroit) were randomized using a computer-generated sequence into a prompt intervention group or a delayed intervention (control) group. Families could not be masked to treatment group status.
Figure 1.
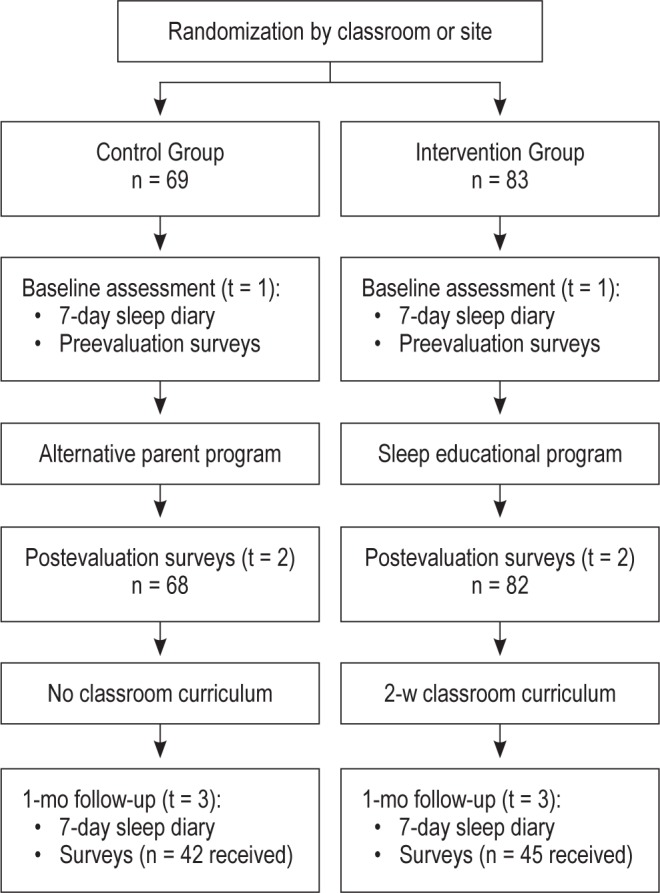
Study design for this randomized controlled assessment of a new sleep education program.
Recruitment
Recruitment flyers were sent home to all families at the participating sites. Flyers described the upcoming sleep education program, and invited parents to participate in a related research study “about their child's sleep” to involve: attending a workshop, completing baseline and follow-up questionnaires, and completing a 7-day sleep diary prior to the parent workshop. The 7-day baseline child sleep diaries were sent home to all parents in advance of the parent meeting. Preintervention surveys and baseline sleep diaries were collected at the beginning of the parent meeting; immediate postintervention surveys were collected at the end of the parent meeting. Reminder flyers and follow-up sleep diaries were sent home to participating parents approximately 3 w after the initial parent meeting. Parents completed follow-up surveys and returned the completed sleep diaries during a second parent meeting, at Head Start, approximately 1 mo after the initial parent educational intervention. For parents who were unable to attend, telephone reminders were used to encourage them to complete the follow-up surveys and sleep diaries, and return them to the Head Start classroom.
To be eligible for participation, the parent had to be able to complete the survey and written informed consent in English. The only exclusion criterion was that the child could not be a foster child for whom the legal signer of consent would be the state. Parents were asked to complete the surveys in reference only to their youngest child currently attending Head Start. Among 668 eligible families, 152 parents or guardians (23%) consented to participate. Of these, 83 were randomized to the prompt intervention and 69 to the control group.
Sleep Education Intervention
The “Sweet Dreamzzz Early Childhood Sleep Education Program”” was developed by Sweet Dreamzzz, Inc, with contributions from the Wayne State University School of Instructional Technology, to help fulfill the mission of the nonprofit organization, rather than for this or any other research study. The program is described in a short video available at http://youtu.be/rxlwP5dt_Mg. This new program was developed to be a creative and engaging complement to sleep educational programs already administered by Sweet Dreamzzz to well over 40,000 elementary and middle school children in southeast Michigan during the past 12 y. Although Head Start Performance Standards 1304.23(a)(1)(2)(3) require that enrolled children receive screening for nutritional problems, and that their parents receive information about possible dietary inadequacies and nutrient needs, no similar efforts are required or made, to our knowledge, to teach about sleep health at earlier ages when sleep habits and priorities are becoming established.16,17 The Early Childhood Sleep Education Program and associated research assessment surveys were initially piloted at a Head Start preschool program in Pontiac, Michigan (see following paragraphs), prior to use in a more refined form at the Lansing and Detroit sites. The initial pilot was granted institutional review board exemption because no data were collected for research.
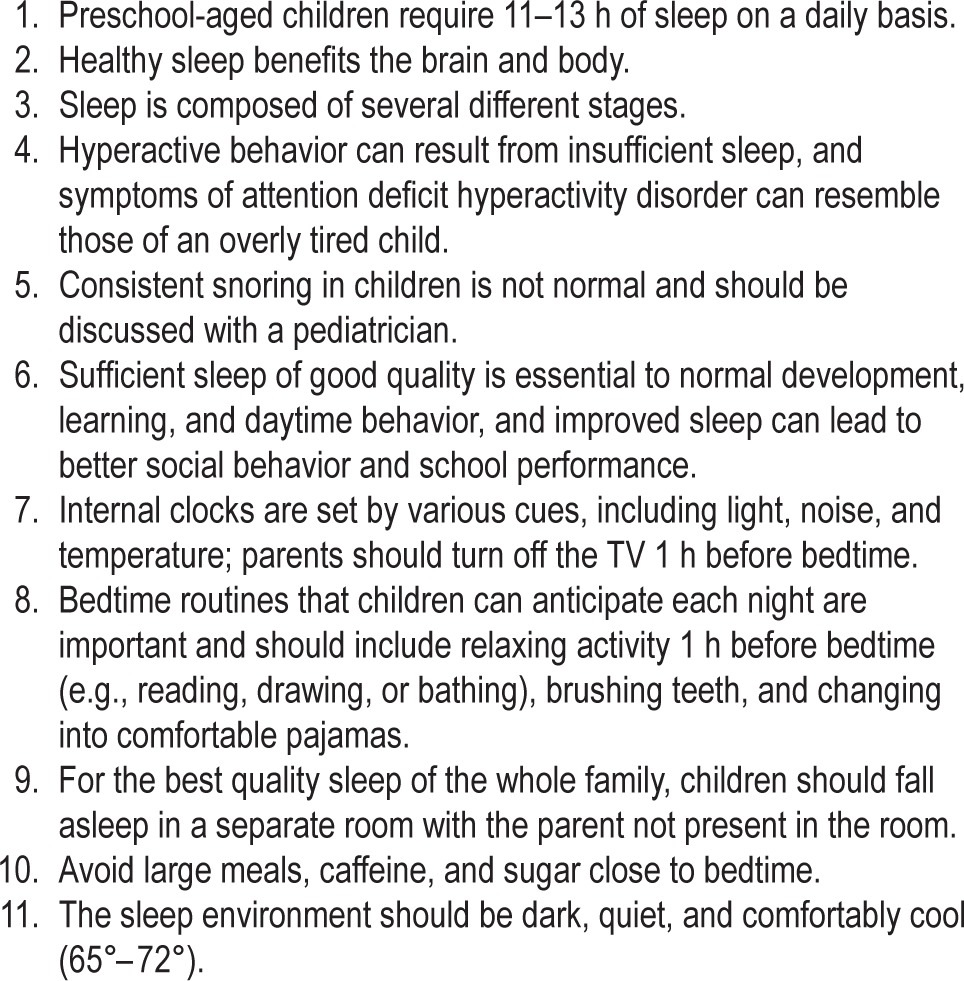
The Sweet Dreamzzz Early Childhood Sleep Education Program” is designed to create a home- and school-based triangle of support by educating teachers, parents, and preschoolers. Through a one-time, 45-min interactive Power-Point presentation for parents and another for teachers, each group learns about the importance of sleep, how many hours of sleep are required at specific ages, and how to establish and maintain a bedtime routine. Through interactive Sweet Dreamzzz lessons taught daily by the regular classroom teacher over 2 w, students gain an understanding of healthy sleep habits and how to follow a bedtime routine. The parent and teacher workshops are delivered by an experienced Sweet Dreamzzz instructor, a certified teacher who holds a master's degree in curriculum and instruction with 5 y of previous teaching experience in other Sweet Dreamzzz sleep education programs for older children. Teacher workshops are held during a Head Start planning meeting, and parent workshops are held at the Head Start site during a regularly scheduled monthly parent meeting. The content of the sessions is summarized in Table 1. Parents have an opportunity to ask questions during the presentation and at its conclusion. A take-home participant guide is distributed to review the bedtime routine steps and provide sleep tips and sleep articles.
Table 1.
Examples of topics covered during parent and teacher education sessions
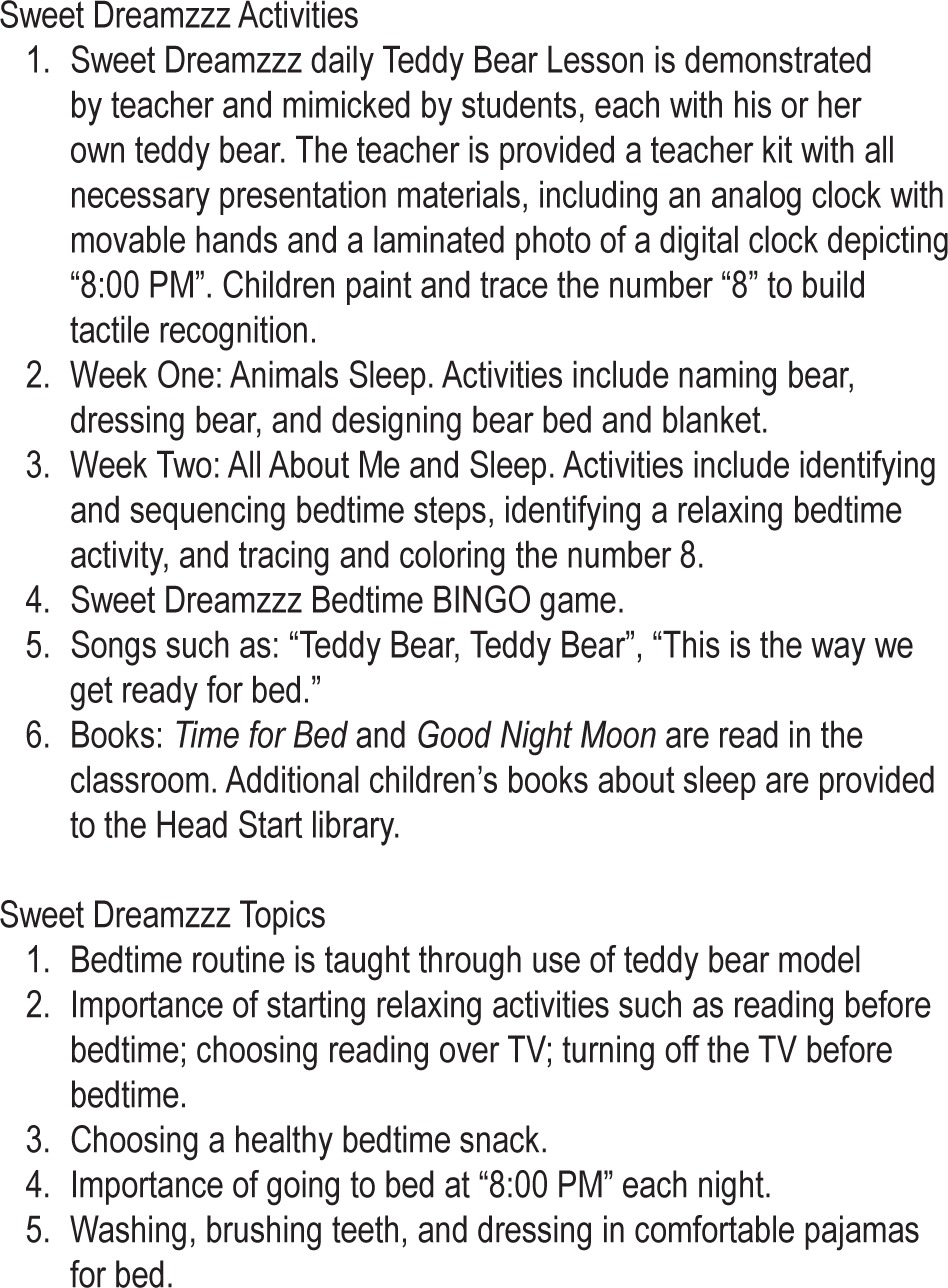
The classroom component was initiated within 1 w of the parent education workshop. The 2-w curriculum delivered by Sweet Dreamzzz-trained teachers includes a 20-min daily lesson followed by 20 min of related activity, on each of the 8 school days (Monday through Thursday) for 2 consecutive weeks. Children each receive a teddy bear to use in the classroom as they learn and mimic a bedtime routine and experience the daily Sweet Dreamzzz “Teddy Bear Lesson” (Table 2). In week 1, students learn through a story, Time For Bed by Mem Fox, that animals need sleep. The Teddy Bear Lesson is reinforced by activities throughout the week as students name their bear, design their bear's bed and blanket, and play Bedtime BINGO. In week 2, students understand that they need sleep and a sleep routine as they hear the story, Good Night Moon by Margaret Wise Brown, and complete age-appropriate activities that reinforce each of the bedtime routine steps. Parents do not participate in the preschool teaching, but lessons are reinforced in the home with a bedtime routine chart, a bedtime routine magnet, reading book, blanket, toothbrush, and toothpaste that are all given to children at no charge and brought home as part of the program. The bedtime routine chart, complete with stickers, provides incentive to follow the bedtime routine steps at home while the child is learning them in the classroom. The reading book provided for use at home (Good Night Moon) as a relaxing bedtime activity is the same book being read in the classroom by the teachers. The blanket provides comfort at bedtime and the toothbrush and toothpaste fulfill a bedtime routine step. After the 2 w of healthy sleep lessons in the classroom, each child brings the teddy bear home to care for and sleep with each night. The take-home items are discussed in a parent instruction guide that families receive, and reviewed with parents during their workshop. The guide includes general instructions for use of the materials and an overview of the classroom curriculum. Similar to the participant guide handed out at the parent workshop, the parent instruction guide includes bedtime routine steps and sleep tips. Finally, for reinforcement of sleep lessons and classroom continuity after the 2-w curriculum, Sweet Dreamzzz leaves teachers with a classroom bedtime routine poster, three teddy bears for play during the day, and an additional 10 sleep enrichment lessons to use throughout the school year.
Table 2.
Examples of activities and topics covered in the classroom curriculum during the Sweet Dreamzzz Early Childhood Sleep Education Program™:
Control Group
Parents of children in control classrooms or sites were invited to attend a 45-min nutrition program on picky eating (Lansing sites) or their regularly scheduled parent meeting to engage parents in the upcoming school year (Detroit sites). At the end of the study, control families were able to participate in the sleep education program, including both the parent program and the classroom curriculum, although outcome measures were not collected.
Assessment
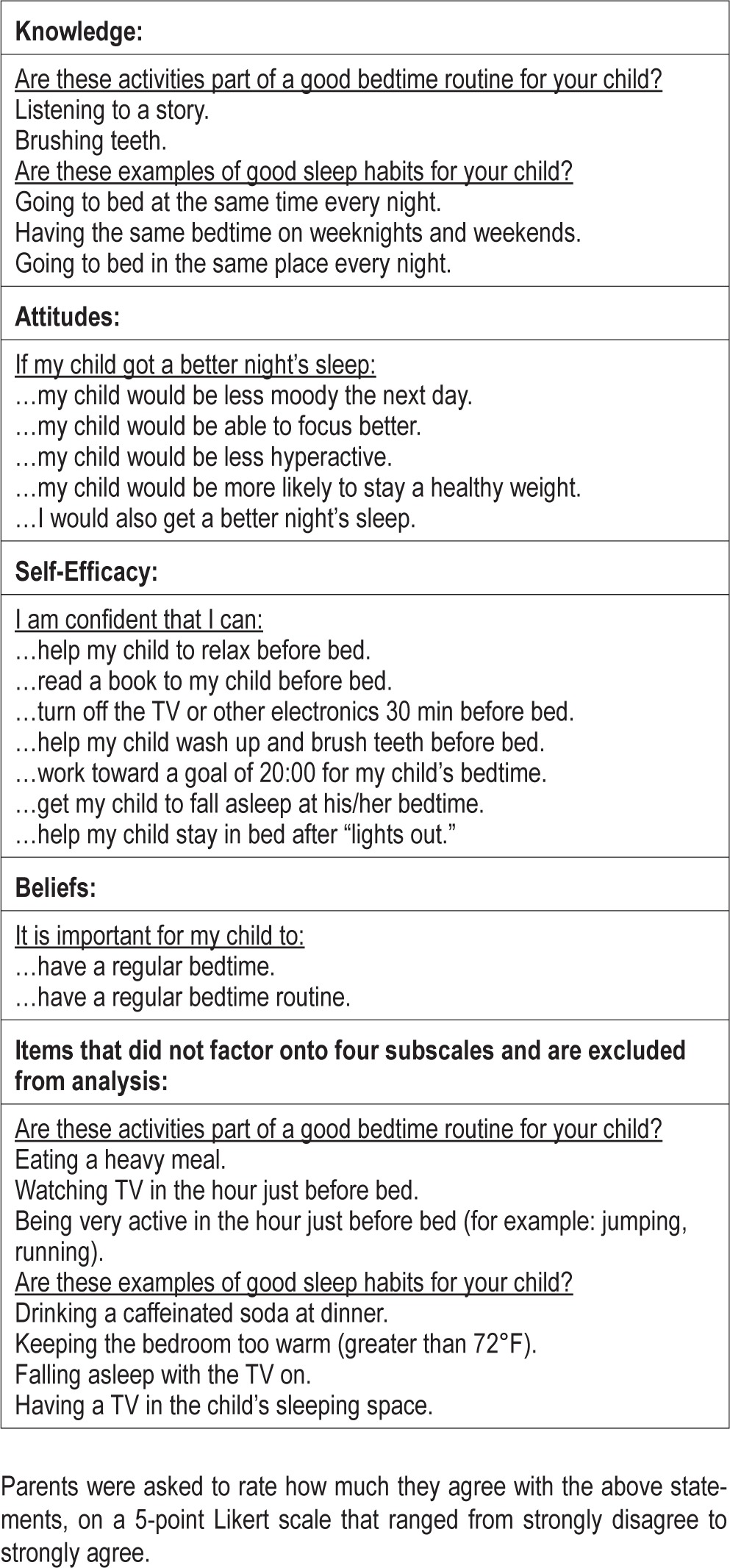
A survey to assess parent knowledge, attitudes, self-efficacy, and beliefs (known by the acronym KASB) about sleep was developed specifically for the current study, for completion independently by parents at three time points: (1) prior to the start of the parent program (pre-intervention, time 1); (2) immediately after the parent program (postintervention, time 2); and (3) approximately 1 mo after the parent program (follow-up, time 3). For the initial administration, all parents (except those who arrived late, including seven in the intervention group and one in the control group) turned in their questionnaires before the educational program had started. The investigators designed the question-items, with responses on 5-point Likert scales that ranged from strongly disagree to strongly agree (0 = strongly disagree, 4 = strongly agree), to assess parents' KASB about sleep as the primary outcomes for this study. The items were developed based on social-cognitive theory to reflect parent KASB specifically regarding the topics that were the focus of the Sweet Dreamzzz intervention. The items were adapted in part from questionnaires that have been used by the authors in other intervention studies.18 The 26-item survey (see Appendix) was initially piloted with 104 families in a similar Head Start sample in Pontiac, Michigan. Poorly worded questions were identified, and reworded or eliminated. For the current study sample, a factor analysis was performed on the 26 survey items. Conceptually similar items loaded onto four factors with coefficients between 0.50 and 0.85. These four subscales are: knowledge (five items, alpha = 0.78), attitudes (five items, alpha = 0.90), self-efficacy (seven items, alpha = 0.89), and beliefs (two items, alpha = 0.96). Individual survey items were then averaged accordingly to create subscales for analyses. The seven items that did not load onto one of the four subscales were excluded from analysis. One additional multiple-choice knowledge item also asked parents, “How many hours of sleep do most preschool children need?” Responses included “7-8 h,” “9-10 h,” “11-13 h,” “14 h or more,” or “don't know.” Responses of “11-13 h” were identified as correct based on recommendations by the National Sleep Foundation19 whereas all other responses were identified as incorrect. Parents provided basic demographic information including child age, child sex, race, ethnicity, and maternal education level.
Sleep Diaries
To provide information on children's sleep durations and bedtimes as secondary outcomes for this study, parents were asked to complete 7-day sleep diaries prior to the parent meetings and again about 1 mo after the parent meeting. Parents recorded what time their child “fell asleep” and “woke up.” From the sleep diaries, average weeknight bedtime and week-night sleep duration were calculated. We planned to focus our analysis on weekdays because they tend to have less variability than weekend days and should be more pertinent for classroom consequences of insufficient sleep. Information on the importance of consistent bedtimes was included in the parent education sessions, but we assumed that in most families bedtimes and wake times are influenced by working parent schedules (on Monday through Friday) more than children's preschool schedules (Monday through Thursday). Therefore, weeknight bedtimes were defined as Sunday and Monday-Thursday whereas weekday wake times were Monday-Friday.
Statistical Analysis
Data were double entered to confirm accuracy. Statistical analysis was performed using SAS 9.3 (SAS Institute, Cary, NC). To assess treatment group differences in participant characteristics, t-tests and chi-square tests were used. For our primary KASB outcomes, we constructed separate linear mixed models for each of the four subscale scores to assess treatment group differences from preintervention (time 1) to immediate postintervention (time 2) and 1-mo follow-up (time 3). Mixed models were adjusted for demographic variables that proved different between the control and intervention group, and for maternal education level (at least a high school (HS) degree or equivalent versus more), which was assumed to be relevant to the primary outcome (KASB). In part because of colinearity between Head Start sites and child race/ethnicity, additional mixed models with interaction terms for site effects tested for any difference in intervention impact between sites (Lansing versus Detroit). The least squares means with Bonferroni adjustments were used to compare individual time points within each group. To test the hypothesis that parents' responses for “How many hours of sleep do most preschool children need?” improved in the intervention group as compared to the control group, the McNemar test was used. To test the hypotheses that the intervention improved children's weeknight sleep durations and bedtimes, we used a 2 × 2 factorial analysis of variance as defined by treatment group and time.
For this study, we anticipated that detection of changes in sleep duration rather than KASB alone might be more challenging. We estimated that a sample size of at least 100 families (n = 50 in each arm) with a one-sided test for improved sleep duration would provide power ≥ 0.80 if the Cohen d statistic is ≥ 0.5, which is a moderate effect size.
RESULTS
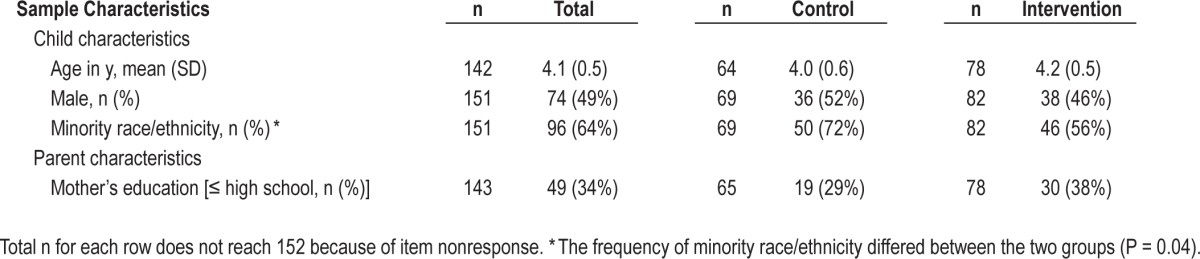
As shown in Table 3, the child participant's mean age was 4.1 ± 0.5 (standard deviation) years (range, 2.9–5.2 y). Nearly half of the participants (49%) were male and two thirds (64%) were identified by parents as a minority race or ethnicity (non-white or Hispanic). The intervention group had a somewhat lower percentage of minority children than did the control group (56% versus 72%, P = 0.04); therefore, child race/ethnicity (nonwhite or Hispanic versus white, non-Hispanic) was taken into account in the KASB mixed models discussed in the next paragraphs. Among the respondents, 88% were mothers and 34% had an education level that was less than or equal to a HS degree or equivalent.
Table 3.
Sample demographics among n = 152 participants.
Knowledge, Attitudes, Self-Efficacy, and Beliefs
Overall, 57% of participants returned the KASB surveys at 1-mo follow-up. Linear mixed models showed a significant time × treatment effect for knowledge (P = 0.02), attitudes (P = 0.001), and self-efficacy (P = 0.02), but not for beliefs (P = 0.20) after adjustment for child race/ethnicity and maternal education. These models were based on results from n = 143 children whose mothers' education levels were known. Least squares means from the linear mixed models are plotted in Figure 2. After a Bonferroni adjustment, immediate post-intervention improvement was evident in all four KASB subscales (knowledge P < 0.0001; attitudes P < 0.0001; self-efficacy P < 0.0001; and beliefs P = 0.004). However, none of these improvements were sustained at the 1-mo follow-up (each P > 0.05). The control group showed no statistically significant increases in scores over time, at either time 2 or time 3. Additional linear models that adjusted for site (Lansing versus Detroit) did not show a main effect for site or a time × treatment × site effect for any of the four subscales (each P > 0.05).
Figure 2.

The least means squares with Bonferroni adjustment in linear mixed models, adjusted for child race/ethnicity and maternal education, are plotted for: (A) knowledge; (B) attitudes; (C) self-efficacy; and (D) beliefs. In the intervention group, each subscale score improved from pre-intervention (time 1) to postintervention (time 2), but not from postintervention (time 2) to follow-up (time 3) or preintervention (time 1) to follow-up (time 3) (significant P values are shown). No significant improvement in scores occurred for the control group. In the overall linear mixed models, adjusted for child race/ethnicity and maternal education, a significant time × treatment interaction emerged for self-efficacy (P = 0.02), attitudes (P = 0.001), and knowledge (P = 0.02), but not for beliefs (P = 0.20).
The proportion of intervention group parents who correctly identified the recommended hours of sleep for preschool children increased from baseline (time 1) at the postintervention (time 2) (McNemar test P < 0.0001) and at 1-mo follow-up (time 3) (P < 0.0001). Parents in the control group did not change their response significantly from time 1 to time 2 (P = 0.56), but did improve their responses from time 1 to time 3 (P = 0.02).
Sleep Diaries
In total, 54% of parents returned a baseline sleep diary and 44% returned a 1-mo follow-up sleep diary. A significant time × treatment interaction in sleep duration was apparent between children in the intervention vs. control group (P = 0.04). Children in the intervention group improved their nocturnal sleep durations on weeknights by 30 min, from 10.5 ± 1.0 h at baseline to 11.0 ± 0.9 h on follow-up (Figure 3). The control group did not show improved sleep durations (10.5 ± 0.9 h at baseline and 10.4 ± 0.9 h on follow-up). Children in the intervention group also went to bed 22 min earlier on average after the intervention (20:37 ± 45 min versus 20:59 ± 47 min at baseline), whereas the control group did not change (20:58 ± 50 min versus 20:55 ± 41 min on baseline, Figure 4). However, despite this selective improvement in the intervention group, the time × treatment interaction did not reach statistical significance for bedtimes (P = 0.12). We also explored whether changes in KASB scores predicted changes in sleep duration using linear regression models and found no associations (each P > 0.05).
Figure 3.
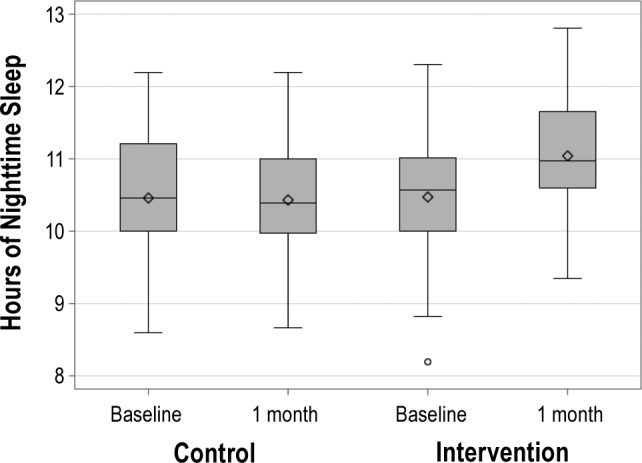
Average weeknight sleep duration for the intervention and control group at baseline and 1-mo follow-up. Using a 2 × 2 analysis of variance, a significant time × treatment interaction emerged (P = 0.04). Plots show medians, means (diamonds), 25th and 75th percentiles, 10th and 90th percentiles (serifs), and outliers.
Figure 4.
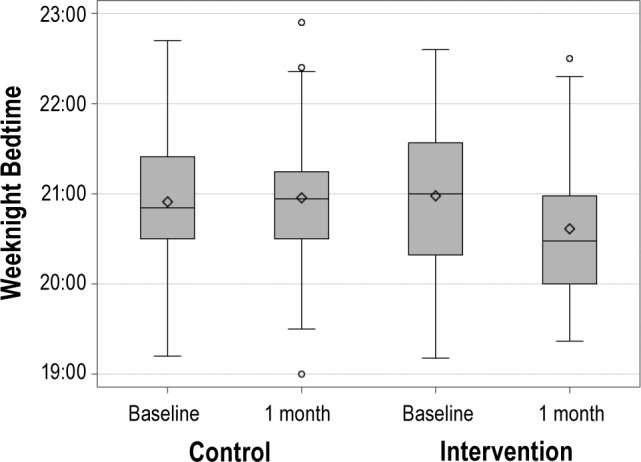
Average weeknight bedtime for the intervention and control group at baseline and 1-mo follow-up. Using a 2 × 2 analysis of variance, no significant time × treatment interaction emerged (P = 0.12). Plots show medians, means (diamonds), 25th and 75th percentiles, 10th and 90th percentiles (serifs), and outliers.
DISCUSSION
The most intriguing result of this randomized controlled assessment among 152 low-income preschool children and their families was that a sleep education program produced a 30-min increase in sleep duration at 1 mo follow-up. Parents' sleep-related KASB, the primary outcome measures, also improved immediately after an intervention as simple as a 45-min sleep education presentation. However, this effect was not sustained at 1-mo follow-up. Our results suggest that 2 w of daily exposure in the preschool classroom after an initial presentation to parents may be an effective strategy to change sleep behaviors in preschoolers. However, reinforcement beyond the first parent session or other approaches may be necessary to maintain the improvements in KASB over time.
To our knowledge, this study is the first to investigate the effectiveness of a sleep education program for low-income preschool families. Our study focused on changes in parents' KASB about sleep, as parents are still the primary external regulators of children's sleep in the preschool years. In contrast, previously published studies have focused mainly on changes in sleep knowledge among children and adolescents. One previous study found similarly that parent knowledge increased immediately after reading a sleep education brochure.20 However, this study differed from ours in that it included parents with children age 3 mo to 12 y, whereas ours focused on low-income preschool children. Additionally, the sleep education brochure was distributed to parents to read on their own in a pediatric clinic, whereas the Sweet Dreamzzz sleep program described in the current report was led by a sleep educator in an interactive session for parents at Head Start sites. Finally, the previous study did not assess intervention effects 1 mo later, so whether those study participants also would have shown low retention of newly acquired sleep knowledge at an extended follow-up remains unknown.
We can only speculate why parents in this study failed to demonstrate improved sleep related knowledge 1 mo after their educational session. Although children in this study had reinforcement of their learning activities, during eight sessions over 2 w, parents had only one 45-min learning opportunity. Abundant evidence suggests that repeated exposure is necessary to teach concepts well, and future iterations of the Early Childhood Sleep Education Program may need to incorporate repeated parent sessions, in combination with child sessions.21 Sweet Dreamzzz is now designing a Train-the-Trainer package to enhance the Parent Workshop. This will provide, after the initial training session, reinforcement workshops throughout the school year. Other potential solutions may require increased parent motivation, through presentation of more detailed information about potential gains to children who obtain sufficient sleep; reinforcement through more extensive written materials that parents can take home; or inclusion of repeated messages about sleep through emailed Head Start newsletters or online social media.
An interesting observation in the current study was that children's sleep appeared to improve, at 1-mo follow-up, despite lack of evidence that parents retained the knowledge they had demonstrated immediately after their education session. One possible explanation lies in the Sweet Dreamzzz emphasis on a triangle of learning, involving parents, teachers, and children. The students brought their lessons home: they would see “8:00 PM” on the clock at home as at school; have their copy of Good Night Moon to read at home (the same book read by the teacher in the classroom); and bring home their Sweet Dreamzzz teddy bears after the 2 w of lessons to help them sleep at night. Anecdotally, teachers told Sweet Dreamzzz staff that parents reported their children recognized “8:00 PM” at home and told them “It's time for bed!”
With regard to the changes in sleep behavior, our results build on two smaller studies of n = 2722 and n = 2614 preadolescent seventh graders, respectively, that produced improvement in children's sleep duration on weeknights22 and earlier weeknight bedtimes.14 Both interventions involved one to two sessions per week, over a period of 5-7 w, led by research staff. In contrast, our classroom intervention “dosage” was 40 min/ day over a period of 2 w (8 sessions). The current classroom programs were led by trained Head Start teachers as opposed to research staff, in a “train the trainer” strategy that may facilitate larger scale implementation in classroom settings.
This early-stage study does have some limitations. The low recruitment rate (23%) may have yielded a biased sample, for example, one that was highly motivated or particularly concerned about children's sleep, though this level of participation is typical in community-based research within neighborhoods that face socioeconomic challenges.23,24 By chance, the intervention group contained fewer minority children than did the control group, though all mixed models adjusted for this difference. Only about half (54%) of enrolled families completed baseline sleep diaries. The overall 1-mo return rate of 57% for the KASB surveys and 44% for the sleep diaries resemble results of previous follow-up efforts in the Head Start population.25 However, the return rates could have underpowered our analyses, particularly at the follow-up time point (time 3) when improvements in parent KASB were not retained. Families that returned the surveys at all three time points may have been more engaged than families who did not return all the surveys, particularly at the 1-mo follow up. This could potentially explain why the control parents improved marginally in their knowledge of “How many hours of sleep do most preschool children need?” at 1-mo follow-up. However, we cannot rule out the possibility that parents of control children may have learned something inadvertently from school staff or friends during the interval that elapsed between time 1 and 3 assessments. Parents completed the written surveys independently, which may have biased our sample to those parents with a higher literacy level.
Furthermore, bedtimes and sleep duration were assessed by parent diaries rather than a more objective measure, such as actigraphy. Sleep diaries are commonly used in both sleep research and clinical settings, because they provide bedtime and wake time data that are largely congruent with actigraphy and more accurate than parental recall or questionnaires,26 but confirmation of our findings using objective measures, such actigraphy, would still be useful. This is especially true in light of the puzzling discrepancy we found, in that sleep duration improved at 1 mo despite our inability to demonstrate that the parent knowledge newly demonstrated after the parent education session was retained at 1 mo. Our study did not include formal measures of what children, as opposed to parents, may have learned. However, an anecdotal report from Sweet Dreamzzz staff suggested that child learning did occur. Specifically, they found from their own preintervention and postintervention data that preschoolers at the same Lansing and Detroit Head Start sites demonstrated a statistically significant increase in their ability to (1) distinguish “8:00 PM” from “9:00 PM” as the desirable bedtime, (2) indicate that an apple before bedtime is a better snack than a candy bar, and (3) identify reading rather than watching TV as a relaxing activity before bedtime. Finally, our sample was restricted to low-income preschoolers, in one US state region, which may limit applicability to other socioeconomic groups, ages, and locations.
Nevertheless, several strengths of this study include its randomized design, novel focus on a socioeconomic group likely to have particular need for sleep education, sample size in relation to previous studies of sleep education programs, and combination of parental and child outcomes. The findings do indicate that a sleep education program focused on low-income preschoolers and their families in Michigan successfully increased preschoolers' sleep duration by an average of 30 min on weeknights. An increase in sleep duration of this magnitude has been associated with improvements in daytime functioning in children. Gruber and colleagues reported that 27 min of sleep extension resulted in improvements in daytime sleepiness, emotional lability, and restless-impulsive behaviors in elementary school children.27 Also among elementary school children, Sadeh and colleagues found that sleep extension of 30 min or more as compared to no change or sleep restriction improved vigilance and motor reaction on a simple reaction-time test and reaction time on a continuous performance test.28 Although similar daytime outcomes were not measured in the current study, these authors' results in combination with ours suggest that sleep education programs could achieve important, tangible improvements in children's daytime functioning by extension of their sleep duration.
Although some investigators have debated recently how well we know the amount of sleep children need,29,30 available evidence seems clear that many children obtain insufficient sleep, and that this has substantial adverse consequences for cognition, development, and metabolism.31 Studies such as the current one now provide critical demonstrations that minimal, relatively inexpensive interventions can be effective, even at early ages when lifelong effect may be the greatest. Family sleep education during early childhood years, when sleep habits are being established, could prove to be a most cost-effective strategy to improve children's sleep and overall health.
DISCLOSURE STATEMENT
This study was funded by the Michigan Center for Integrative Approaches to Health Disparities and the National Institute on Minority Health and Health Disparities (P60 MD002249); an Humanitarian Award from the American Sleep Medicine Foundation to Sweet Dreamzzz, Inc; a Physician Scientist Training Award to K.E.W. from the American Sleep Medicine Foundation; and by a training grant from the National Institute for Neurological Disorders and Stroke (5T32 NS007222). Dr. Chervin has received research grants from the National Institutes of Health, Fox Foundation, and University of Michigan. He has received support for an educational program from Philips Respironics and Fisher Paykel. He serves on boards of directors for the American Academy of Sleep Medicine, American Sleep Medicine Foundation, American Board of Sleep Medicine, Associated Professional Sleep Societies, and International Pediatric Sleep Association. He has consulted for Proctor and Gamble, Zansors, and MC3. He serves as a section editor for UpToDate and a book editor for Cambridge University Press. He serves as a volunteer on the advisory board of Sweet Dreamzzz, which developed and administered the educational intervention described in this report. He is named in patents, patents pending, and copyrighted material related to sleep disorder diagnosis and assessment, and owned by the University of Michigan. The other authors have indicated no financial conflicts of interest.
ACKNOWLEDGMENTS
The authors are grateful to Ann Raftery, MA, Director of Sleep Programs, and Nancy Maxwell, Executive Director, Sweet Dreamzzz Inc. for the opportunity to assess the “Sweet Dreamzzz Early Childhood Sleep Education Program”, for facilitating collection of data for this research, and for their review and feedback on this manuscript; to Teresa Spitzer, Jeanne Kott, Eva Wilson, Sophia Burton, and Capital Area Community Services and Renaissance Head Start staff for their assistance; to Kenneth E. Guire, MS, for valuable assistance with statistical analyses; to Bianca Jiddou and Arshia Vahabzadeh for their assistance with database management; and to the families who volunteered to assist in this research.
Appendix.
Knowledge, attitudes, self-efficacy, and beliefs (KASB) questionnaire
Footnotes
A commentary on this article appears in this issue on page 1033.
REFERENCE
- 1.Mindell JA, Owens JA. Philadelphia, PA: Lippincott Williams & Wilkins; 2003. A Clinical Guide to Pediatric Sleep: Diagnosis and Management of Sleep Problems. [Google Scholar]
- 2.Astill RG, Van der Heijden KB, Van Ijzendoorn MH, Van Someren EJ. Sleep, cognition, and behavioral problems in school-age children: a century of research meta-analyzed. Psychol Bull. 2012;138:1109–38. doi: 10.1037/a0028204. [DOI] [PubMed] [Google Scholar]
- 3.Hale L, Berger LM, LeBourgeois MK, Brooks-Gunn J. A longitudinal study of preschoolers' language-based bedtime routines, sleep duration, and well-being. J Fam Psychol. 2011;25:423–33. doi: 10.1037/a0023564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Taveras EM, McDonald J, O'Brien A, et al. Healthy Habits, Happy Homes: methods and baseline data of a randomized controlled trial to improve household routines for obesity prevention. Prev Med. 2012;55:418–26. doi: 10.1016/j.ypmed.2012.08.016. [DOI] [PubMed] [Google Scholar]
- 5.Owens JA, Jones C, Nash R. Caregivers' knowledge, behavior, and attitudes regarding healthy sleep in young children. J Clin Sleep Med. 2011;7:345–50. doi: 10.5664/JCSM.1186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Owens JA, Jones C. Parental knowledge of healthy sleep in young children: results of a primary care clinic survey. J Dev Behav Pediatr. 2011;32:447–53. doi: 10.1097/DBP.0b013e31821bd20b. [DOI] [PubMed] [Google Scholar]
- 7.Schreck KA, Richdale AL. Knowledge of childhood sleep: a possible variable in under or misdiagnosis of childhood sleep problems. J Sleep Res. 2011;20:589–97. doi: 10.1111/j.1365-2869.2011.00922.x. [DOI] [PubMed] [Google Scholar]
- 8.Blunden S. The implementation of a sleep education program in primary school children. Sleep Biol Rhythms. 2007;5:A32. [Google Scholar]
- 9.Cain N, Gradisar M, Moseley L. A motivational school-based intervention for adolescent sleep problems. Sleep Med. 2011;12:246–51. doi: 10.1016/j.sleep.2010.06.008. [DOI] [PubMed] [Google Scholar]
- 10.Cortesi F, Giannotti F, Sebastiani T, Bruni O, Ottaviano S. Knowledge of sleep in Italian high school students: pilot-test of a school-based sleep educational program. J Adolesc Health. 2004;34:344–51. doi: 10.1016/j.jadohealth.2003.07.003. [DOI] [PubMed] [Google Scholar]
- 11.Blunden S, Kira G, Hull M, Maddison R. Does sleep education change sleep parameters? Comparing sleep education trials for middle school students in Australia and New Zealand. Open Sleep J. 2012;5:12–8. [Google Scholar]
- 12.Bakotic M, Radosevic-Vidacek B, Koscec A. Educating adolescents about healthy sleep: experimental study of effectiveness of educational leaflet. Croat Med J. 2009;50:174–81. doi: 10.3325/cmj.2009.50.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Moseley L, Gradisar M. Evaluation of a school-based intervention for adolescent sleep problems. Sleep. 2009;32:334–41. doi: 10.1093/sleep/32.3.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Vo O, LeChasseur K, Wolfson A, Marco C. Sleepy pre-teens: second pilot of sleep-smart program in 7th graders. Sleep. 2003;26:A411. (abstract suppl) [Google Scholar]
- 15.Nevarez MD, Rifas-Shiman SL, Kleinman KP, Gillman MW, Taveras EM. Associations of early life risk factors with infant sleep duration. Acad Pediatr. 2010;10:187–93. doi: 10.1016/j.acap.2010.01.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Touchette E, Petit D, Paquet J, et al. Factors associated with fragmented sleep at night across early childhood. Arch Pediatr Adolesc Med. 2005;159:242–9. doi: 10.1001/archpedi.159.3.242. [DOI] [PubMed] [Google Scholar]
- 17.Owens J. Socio-cultural considerations and sleep practices in the pediatric population. Sleep Med Clin. 2008;3:97–107. [Google Scholar]
- 18.Miller AL, Horodynski MA, Herb HE, et al. Enhancing self-regulation as a strategy for obesity prevention in Head Start preschoolers: the growing healthy study. BMC Public Health. 2012;12:1040. doi: 10.1186/1471-2458-12-1040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.National Sleep Foundation. Children and sleep. [Accessed May 5, 2012]. http://www.sleepfoundation.org/article/sleep-topics/children-and-sleep.
- 20.Jones C, Owens JA, Pham B. Can a brief educational intervention improve parents' knowledge of healthy children's sleep? A pilot test. Health Education J. 2013;72:601–10. [Google Scholar]
- 21.Webster-Stratton C, Hammond M. Treating children with early-onset conduct problems: a comparison of child and parent training interventions. J Consult Clin Psychol. 1997;65:93–109. doi: 10.1037//0022-006x.65.1.93. [DOI] [PubMed] [Google Scholar]
- 22.Rossi C, Campbell AL, Vo OT, Charron T, Marco CA, Wolfson AR. Middle school sleep-smart program: a pilot evaluation. Sleep. 2002;25:A279. (abstract suppl) [Google Scholar]
- 23.Chervin RD, Clarke DF, Huffman JL, et al. School performance, race, and other correlates of sleep-disordered breathing in children. Sleep Med. 2003;4:21–7. doi: 10.1016/s1389-9457(02)00243-5. [DOI] [PubMed] [Google Scholar]
- 24.O'Brien LM, Lucas NH, Felt BT, et al. Aggressive behavior, bullying, snoring, and sleepiness in schoolchildren. Sleep Med. 2011;12:652–8. doi: 10.1016/j.sleep.2010.11.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Carrillo Zuniga G, Kirk S, Mier N, Garza NI, Lucio RL, Zuniga MA. The impact of asthma health education for parents of children attending head start centers. J Community Health. 2012;37:1296–1300. doi: 10.1007/s10900-012-9571-y. [DOI] [PubMed] [Google Scholar]
- 26.Werner H, Molinari L, Guyer C, Jenni OG. Agreement rates between actigraphy, diary, and questionnaire for children's sleep patterns. Arch Pediatr Adolesc Med. 2008;162:350–8. doi: 10.1001/archpedi.162.4.350. [DOI] [PubMed] [Google Scholar]
- 27.Gruber R, Cassoff J, Frenette S, Wiebe S, Carrier J. Impact of sleep extension and restriction on children's emotional lability and impulsivity. Pediatrics. 2012;130:e1155–61. doi: 10.1542/peds.2012-0564. [DOI] [PubMed] [Google Scholar]
- 28.Sadeh A, Gruber R, Raviv A. The effects of sleep restriction and extension on school-age children: what a difference an hour makes. Child Dev. 2003;74:444–55. doi: 10.1111/1467-8624.7402008. [DOI] [PubMed] [Google Scholar]
- 29.Matricciani LA, Olds TS, Blunden S, Rigney G, Williams MT. Never enough sleep: a brief history of sleep recommendations for children. Pediatrics. 2012;129:54–556. doi: 10.1542/peds.2011-2039. [DOI] [PubMed] [Google Scholar]
- 30.Owens JA. A letter to the editor in defense of sleep recommendations. Pediatrics. 2012;129:987–8. doi: 10.1542/peds.2012-0755A. author reply 989–91; discussion 988–9. [DOI] [PubMed] [Google Scholar]
- 31.Kong AP, Wing YK, Choi KC, et al. Associations of sleep duration with obesity and serum lipid profile in children and adolescents. Sleep Med. 2011;12:659–65. doi: 10.1016/j.sleep.2010.12.015. [DOI] [PubMed] [Google Scholar]