

Abstract
Background
Some early studies with robotic-assisted pedicle screw implantation have suggested these systems increase accuracy of screw placement. However, the relationship between the success rate of screw placement and the learning curve of this new technique has not been evaluated.
Questions/purposes
We determined whether, as a function of surgeon experience, (1) the success rate of robotic-assisted pedicle screw placement improved, (2) the frequency of conversion from robotic to manual screw placement decreased, and (3) the frequency of malpositioned screws decreased.
Methods
Between June 2010 and August 2012, the senior surgeon (IHL) performed 174 posterior spinal procedures using pedicle screws, 162 of which were attempted with robotic assistance. The use of the robotic system was aborted in 12 of the 162 procedures due to technical issues (registration failure, software crash, etc). The robotic system was successfully used in the remaining 150 procedures. These were the first procedures performed with the robot by the senior surgeon, and in this study, we divided the early learning curve into five groups: Group 1 (Patients 1–30), Group 2 (Patients 31–60), Group 3 (Patients 61–90), Group 4 (Patients 91–120), and Group 5 (Patients 121–150). One hundred twelve patients (75%) had spinal deformity and 80 patients (53%) had previous spine surgery. The accuracy of screw placement in the groups was assessed based on intraoperative biplanar fluoroscopy and postoperative radiographs. The results from these five groups were compared to determine the effect on the learning curve. The numbers of attempted pedicle screw placements were 359, 312, 349, 359, and 320 in Groups 1 to 5, respectively.
Results
The rates of successfully placed screws using robotic guidance were 82%, 93%, 91%, 95%, and 93% in Groups 1 to 5. The rates of screws converted to manual placement were 17%, 7%, 8%, 4%, and 7%. Of the robotically placed screws, the screw malposition rates were 0.8%, 0.3%, 1.4%, 0.8%, and 0%.
Conclusions
The rate of successfully placed pedicle screws improved with increasing experience. The rate of the screws that were converted to manual placement decreased with increasing experience. The frequency of screw malposition was similar over the learning curve at 0% to 1.4%. Future studies will need to determine whether this finding is generalizable to others.
Level of Evidence
Level III, therapeutic study. See the Instructions for Authors for a complete description of levels of evidence.
Introduction
Pedicle screws are the foundation of spinal fixation and can afford multidimensional control and provide substantial rigidity to facilitate fusion. These advantages have led to the wide use of pedicle screws in the treatment of different spinal pathology, such as degenerative, traumatic, and developmental spinal conditions [4]. The accuracy and safety of pedicle screw placement depend largely on the patient’s anatomic landmarks, the navigation system, and the surgeon’s experience. Screw malposition may lead to serious vascular and neurologic complications, especially in patients with severe spinal deformity and patients who need revision surgeries where the anatomic landmarks have been altered [5].
The need for improved accuracy and consistency in pedicle screw placement has led to the development of various new techniques, including computer-navigated and robotic-assisted spine surgery [13, 18, 20, 21]. Some reports have shown that these newer techniques have improved the accuracy of pedicle screw placement [3, 10, 16]. The computer-assisted robotic device used in this study (Renaissance™; Mazor Robotics Ltd, Caesarea, Israel) is a bone-mounted positioning tool that guides the surgeon in the placement of pedicle screws according to a preoperatively planned trajectory [13, 20]. This technology has shown some promising initial results by increasing the accuracy of spinal instrumentation, reducing potential complications, and reducing radiation exposure [3, 6, 7, 12, 15, 19]. However, the relationship between the success rate of screw placement and the learning curve of this new technique has not been evaluated. We therefore evaluated the relationship between the learning curve and the success rate of robotic-assisted pedicle screw implantation in a series of patients over time performed by a high-volume spine surgeon who was involved with the design and development of the system.
Specifically, we determined whether, as a function of surgeon experience, (1) the success rate of robotic-assisted pedicle screw placement improved, (2) the frequency of conversion from robotic to manual screw placement decreased, and (3) the frequency of malpositioned screws decreased.
Patients and Methods
Patient Selection
Between June 2010 and August 2012, the senior surgeon (IHL) performed 174 posterior spinal procedures using pedicle screws. As a general principle, robotic-assisted placement of pedicle screws was the preferred guidance approach. For 12 procedures, we were unable to obtain the needed preoperative workup in a timely fashion for the robotic-assisted surgery. One hundred sixty-two procedures were attempted with robotic assistance. The use of the robotic system was aborted in 12 of the 162 procedures due to technical issues (registration failure, software crash, broken robot, etc). The robotic system was successfully used in the remaining 150 procedures. This study reviewed the radiographic results of these 150 procedures performed using this technique to evaluate the learning curve (Fig. 1).
Fig. 1.
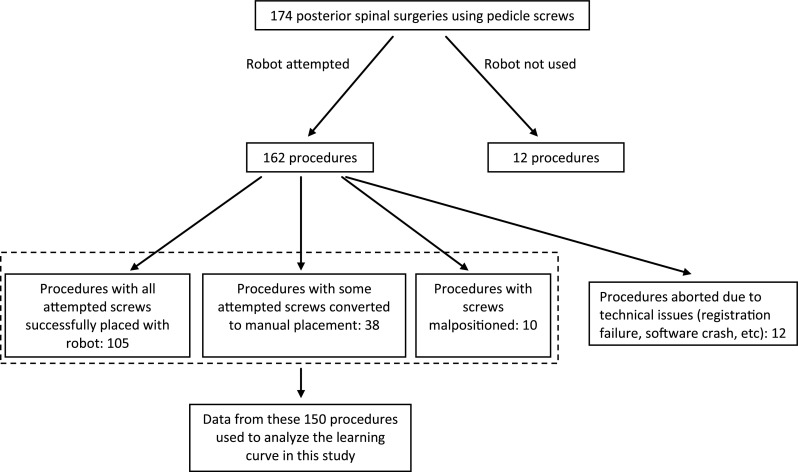
A flow diagram shows the overall distribution of the 174 posterior spinal surgeries using pedicle screws. The robotic-assisted pedicle screw placement was attempted in 162 procedures and was aborted in 12 procedures due to technical issues. The remaining 150 procedures were used for learning curve analysis in this study.
The patients’ age, sex, BMI, diagnosis, and history of previous spine surgery were documented. Operative route, intraoperative fluoroscopy images, and accuracy of screw placement were obtained from technical notes and operative records created immediately after each surgery. All surgeries were performed at the same hospital by a single surgeon. The 150 patients were classified into five subgroups: Group 1 (Patients 1–30), Group 2 (Patients 31–60), Group 3 (Patients 61–90), Group 4 (Patients 91–120), and Group 5 (Patients 121–150). The mean age of the 150 patients was 51 years (range, 12–82 years); 107 (71%) patients were female, and 79 (53%) patients were overweight or obese (BMI ≥ 25) (Table 1). One hundred twelve patients (75%) had spinal deformity and 80 patients (53%) had previous spine surgery (Table 1).
Table 1.
Characteristics of patients in the five groups
| Variable | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | p value |
|---|---|---|---|---|---|---|
| Male/female (number of patients) | 11/19 | 5/25 | 5/25 | 11/19 | 11/19 | 0.1 |
| Age (years)* | 46 (12–79) | 52 (14–77) | 51 (13–77) | 57 (17–79) | 49 (12–82) | 0.3 |
| BMI* | 25 (15–34) | 27 (19–42) | 25 (17–35) | 27 (18–44) | 26 (17–42) | 0.3 |
| Surgery route (number of patients) | 0.005 | |||||
| Open only | 18 | 22 | 27 | 27 | 28 | |
| Percutaneous only | 6 | 5 | 3 | 3 | 2 | |
| Open and percutaneous | 6 | 3 | 0 | 0 | 0 | |
| Patients with previous spine surgery (%) | 53 | 57 | 47 | 57 | 53 | 0.9 |
| Patients with deformity (%) | 80 | 80 | 83 | 67 | 63 | 0.3 |
* Values are expressed as mean, with range in parentheses.
The number of attempted robotic-assisted pedicle screw placements was 359 in Group 1, 312 in Group 2, 349 in Group 3, 359 in Group 4, and 320 in Group 5.
Robotic Guidance System and Surgical Techniques
The robotic guidance system consists of a cylindrical device with detachable arms that can move in six degrees of freedom and a workstation that runs an interface software that facilitates preoperative planning, intraoperative image acquisition and registration, kinematic calculations, and real-time robot motion control. This system has been approved by the FDA for the placement of pedicle screws and details of the device and related surgical techniques have been described previously [3, 13, 15, 20]. A CT scan using 1-mm cuts was obtained preoperatively in all patients for the surgery planning using the proprietary robotic software.
Assessment of Screw Placement Accuracy and Learning Curve
Assessment of screw placement accuracy was based on intraoperative biplanar fluoroscopy, intraoperative neural monitoring, and postoperative radiographs. We believed it was inappropriate to perform postoperative CT scans routinely simply for evaluation of screw placement. The senior surgeon performed all assessments by visually evaluating screw position relative to known landmarks and by comparison to preoperative planning. Briefly, the final radiographs were compared to the preoperative plan for screw position and trajectory. Screw positions were assessed on AP radiographs for their starting points relative to the pedicle and transverse process and for their trajectories as viewed in relation to the midline of the vertebral body. Screw positions were assessed on lateral radiographs for their starting points relative to the superior and inferior borders of the pedicle and for their trajectories in relation to the superior endplates and not extending past the anterior border of the vertebral body (Fig. 2). No intraobserver reliability testing was assessed. Similar methods have been used to evaluate the position of pedicle screws by other researchers [9].
Fig. 2A–E.

(A) AP and (B) lateral views show the preoperative planning. (C) An intraoperative AP view shows that the right L5 screw is misplaced. Intraoperative (D) AP and (E) lateral views show the right L5 screw position after manual correction.
Each attempted screw placement was classified as (1) screw successfully placed using robotic guidance, (2) use of robot aborted and screw placed manually, and (3) screw malpositioned using robot. The success rate of pedicle screw placement among the five groups was analyzed and compared to determine the learning curve effect.
Results
The rate of successfully placed pedicle screws improved with increasing experience. The rates of successfully placed screws using robotic guidance were 82%, 93%, 91%, 95%, and 93% in Groups 1 to 5, respectively (Fig. 3).
Fig. 3.

A graph demonstrates the percentage of screws that were successfully placed, had to be converted to manual placement, and malpositioned using robotic-assisted pedicle screw placement in the five groups. Over time, the success rate of robotic pedicle screw placement improved, the frequency of conversion from robotic to manual screw placement decreased, and the frequency of malpositioned screws was similar.
The rate of the screws that were converted to manual placement decreased with increasing experience. The rates of screws converted to manual placement were 17%, 7%, 8%, 4%, and 7% in Groups 1 to 5, respectively (Fig. 3).
The frequency of screw malposition was similar over the learning curve. The screw malposition rates were 0.8%, 0.3%, 1.4%, 0.8%, and 0% in Groups 1 to 5, respectively (Fig. 3).
Discussion
Surgical robotics emerged during the 1990s and since then much progress has been made to optimize the use of robotic technology in the operating room. Surgical robots aim to enhance and complement the surgeon’s free-hand abilities during surgery. With the significant advances in the image guidance field, several robotic systems have been developed to address the challenges encountered in spine surgeries, especially for the accurate placement of spinal instrumentation [13, 14]. However, the learning curve with these systems is only poorly understood [1, 11]. In this study, we determined whether, as a function of surgeon experience, (1) the successful rate of robotic-assisted pedicle screw placement improved, (2) the frequency of conversion from robotic to manual screw placement decreased, and (3) the frequency of malpositioned screws decreased. We found that the success rate of robotic pedicle screw placement improved and the frequency of conversion from robotic to manual screw placement decreased after the first 30 procedures. Interestingly though, the frequency of malpositioned screws was similar over time.
This study had a number of limitations. First, the assessment of screw placement accuracy was based on intraoperative biplanar fluoroscopy and postoperative radiographs because postoperative CT scans were not routinely performed in our patients. In a systematic review of the complications of pedicle screw fixation in scoliosis surgery, Hicks et al. [5] found that 4.2% of screws were reported as malpositioned. However, in studies in which postoperative CT scans were done systematically, the rate of screw malpositioning was as high as 15.7% [5]. Therefore, it is very likely that the screw malposition rate would be higher if we were to obtain routine postoperative CT scans on our patients. In contemporary clinical practice, most spine surgeons use intra- and postoperative radiographs to judge the accuracy of screw placement and postoperative CT scans are usually not ordered unless there is a clinical indication. Meanwhile, plain radiography has been used to assess the accuracy of pedicle screw placement in several previous studies and we have used similar criteria in our study [9]. We thus believe that our result is still valid and meaningful. Second, the surgeon who did all the surgeries in this series is a relatively high-volume deformity specialist who also participated in the conception, design, and development of this robotic system. The actual learning curve could be different for a new, unfamiliar spine surgeon with a different patient population. Further studies will be needed to answer this question. Third, Group 1 had significantly more percutaneous-only procedures than Groups 3 to 5. This variable may have accounted for some of the differences. As there were limited percutaneous procedures in this study, a subanalysis was not feasible. Future studies will be needed to address this issue. Fourth, it would be ideal if we could compare our data before and after the use of the robotic system. However, the senior author of this study joined the current practice in April 2010 and started to use the robotic technique in June 2010. Thus, we do not have enough data to do this comparison.
We found that, after the first 30 patients, the rate of successful robotic-assisted pedicle screw placement remained consistently more than 90%. This result is consistent with some previous reports. Pechlivanis et al. [15] evaluated the accuracy of percutaneous pedicle screw placement in the lumbar spine using this same robotic system. As analyzed by postoperative CT scans, of 133 total pedicle screws placed, 91.7% screws were placed exactly within the pedicle and 6.8% screws deviated less than 2 mm in the axial plane. In the longitudinal plane, 81.2% screws were placed exactly within the pedicle and 9.8% screws deviated less than 2 mm [15].
We found that the rate of the screws that were converted to manual placement decreased from 17% in the first group to between 4% and 8% in the later four groups. This suggests that, with increasing experience and confidence with the robotic system, the surgeon was able to carry out the preoperatively planned robotic surgery more successfully. In a previous report, Devito et al. [3] reported that, in 682 procedures with 3912 screw/guide wire insertions executed, 16.4% of them were initiated under robotic guidance but were manually placed by the surgeon. However, for the last 276 procedures, they found that the manual conversion rate decreased to 9.2% and they attributed this improvement to the surgeon’s accumulated experience and structural and software improvements of the robotic system. However, no detailed analysis regarding the learning curve was provided in their report [3].
The screw malposition rates ranged between 0% and 1.4% in the five groups and the overall malposition rate was 0.7%. Pedicle screw malposition using the robotic-assisted system studied here was uncommon; however, our specific data are hard to compare to published values, as many of the published studies used CT to judge screw placement, whereas we used plain radiographs and biplanar fluoroscopy. In a recent prospective randomized study that compared pedicle screw placement in the lumbar and sacral spine, the authors found that more screws in the robotic group were in suboptimal position compared to the free-hand group. This result was surprising as most prior cadaveric and retrospective studies reported improved screw placement accuracy with robotic assistance. However, several technique factors such as the fixation method used in that study could have had a negative influence on the performance of the robotic system. There are currently three robotic fixation techniques. In that study, the authors used the bed mount technique (a platform fixed to a cranial spinous process with a K-wire and caudally attached to the operating table) and this might be an insufficient method of fixation as a relative movement of robot to patient can occur [2, 17]. Further prospective, randomized, and postoperative CT-based studies will thus be necessary to more accurately evaluate the outcome of robotic-assisted spine surgery.
The use of new technology always raises some important questions, such as skill development and assessment, teaching, and ease of translation into the operating room [8]. Navigation- and robotic-assisted spine surgery faces these same challenges. The learning curve of a novel surgical procedure is considered the process during which a surgeon gains knowledge and improves skills with the novel procedure. It is an objective assessment of technical ability and a benchmark to compare different surgical techniques. Bai et al. [1] found that the learning curve of spinal navigation dropped sharply after 6 months and reached a plateau after 12 months, which was shown by the improvement in screw perforation rate and operative time. A recent study showed that the learning curve of navigation-assisted pedicle screw placement is not prolonged and experience with fewer than 10 patients was adequate to provide familiarity with the system [11]. However, the actual learning curve of spinal navigation may vary among different systems, different spinal procedures, and different surgeons.
In conclusion, we found that the success rate of robotic-assisted pedicle screw placement increased after the first 30 patients and was maintained at that rate over the remaining time period. In addition, we found that the rate of the screws converted to manual placement decreased after the first 30 patients. This phenomenon was believed to be related to the surgeon’s ability to plan the alignment of the screws more efficiently in the preoperative planning and to technical and software improvements in the robotic system. Furthermore, we found that the frequency of screw malposition was similar over the learning curve at 0% to 1.4%. In addition, we note that a second independent high-volume surgeon who was involved with the development of the system was able to achieve similar consistent results using the robotic system after the first 30 patients; future studies will be needed to determine whether this finding is generalizable to others.
Footnotes
One of the authors certifies that he (XH), or a member of his or her immediate family, has received or may receive payments or benefits, during the study period, an amount of less than USD 10,000 from Mazor Robotics Ltd (Caesarea, Israel). One of the authors certifies that he (IHL), or a member of his or her immediate family, has received or may receive payments or benefits, during the study period, an amount of USD 10,000 to USD 100,000 from Mazor Robotics Ltd.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1.Bai YS, Zhang Y, Chen ZQ, Wang CF, Zhao YC, Shi ZC, Li M, Liu KP. Learning curve of computer-assisted navigation system in spine surgery. Chin Med J (Engl). 2010;123:2989–2994. [PubMed] [Google Scholar]
- 2.Cahill KS, Wang MY. Evaluating the accuracy of robotic assistance in spine surgery. Neurosurgery. 2012;71:N20–N21. doi: 10.1227/01.neu.0000417535.07871.36. [DOI] [PubMed] [Google Scholar]
- 3.Devito DP, Kaplan L, Dietl R, Pfeiffer M, Horne D, Silberstein B, Hardenbrook M, Kiriyanthan G, Barzilay Y, Bruskin A, Sackerer D, Alexandrovsky V, Stuer C, Burger R, Maeurer J, Donald GD, Schoenmayr R, Friedlander A, Knoller N, Schmieder K, Pechlivanis I, Kim IS, Meyer B, Shoham M. Clinical acceptance and accuracy assessment of spinal implants guided with SpineAssist surgical robot: retrospective study. Spine (Phila Pa 1976). 2010;35:2109–2115. doi: 10.1097/BRS.0b013e3181d323ab. [DOI] [PubMed] [Google Scholar]
- 4.Gaines RW., Jr The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am. 2000;82:1458–1476. doi: 10.2106/00004623-200010000-00013. [DOI] [PubMed] [Google Scholar]
- 5.Hicks JM, Singla A, Shen FH, Arlet V. Complications of pedicle screw fixation in scoliosis surgery: a systematic review. Spine (Phila Pa 1976). 2010;35:E465–E470. doi: 10.1097/BRS.0b013e3181d1021a. [DOI] [PubMed] [Google Scholar]
- 6.Hu X, Ohnmeiss DD, Lieberman IH. Robotic-assisted pedicle screw placement: lessons learned from the first 102 patients. Eur Spine J. 2013;22:661–666. doi: 10.1007/s00586-012-2499-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kantelhardt SR, Martinez R, Baerwinkel S, Burger R, Giese A, Rohde V. Perioperative course and accuracy of screw positioning in conventional, open robotic-guided and percutaneous robotic-guided, pedicle screw placement. Eur Spine J. 2011;20:860–868. doi: 10.1007/s00586-011-1729-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kaul S, Shah NL, Menon M. Learning curve using robotic surgery. Curr Urol Rep. 2006;7:125–129. doi: 10.1007/s11934-006-0071-4. [DOI] [PubMed] [Google Scholar]
- 9.Kim YJ, Lenke LG, Bridwell KH, Cho YS, Riew KD. Free hand pedicle screw placement in the thoracic spine: is it safe? Spine (Phila Pa 1976). 2004;29:333–342. doi: 10.1097/01.BRS.0000109983.12113.9B. [DOI] [PubMed] [Google Scholar]
- 10.Kotani Y, Abumi K, Ito M, Takahata M, Sudo H, Ohshima S, Minami A. Accuracy analysis of pedicle screw placement in posterior scoliosis surgery: comparison between conventional fluoroscopic and computer-assisted technique. Spine (Phila Pa 1976). 2007;32:1543–1550. doi: 10.1097/BRS.0b013e318068661e. [DOI] [PubMed] [Google Scholar]
- 11.Lee MH, Lin MH, Weng HH, Cheng WC, Tsai YH, Wang TC, Yang JT. Feasibility of Intra-operative Computed Tomography Navigation System for Pedicle Screw Insertion of the Thoraco-lumbar Spine. J Spinal Disord Tech. 2012 December 3 [Epub ahead of print]. [DOI] [PubMed]
- 12.Lieberman IH, Hardenbrook MA, Wang JC, Guyer RD. Assessment of pedicle screw placement accuracy, procedure time, and radiation exposure using a miniature robotic guidance system. J Spinal Disord Tech. 2012;25:241–248. doi: 10.1097/BSD.0b013e318218a5ef. [DOI] [PubMed] [Google Scholar]
- 13.Lieberman IH, Togawa D, Kayanja MM, Reinhardt MK, Friedlander A, Knoller N, Benzel EC. Bone-mounted miniature robotic guidance for pedicle screw and translaminar facet screw placement. Part I. Technical development and a test case result. Neurosurgery. 2006;59:641–650. doi: 10.1227/01.NEU.0000229055.00829.5B. [DOI] [PubMed] [Google Scholar]
- 14.Ortmaier T, Weiss H, Hagn U, Grebenstein M, Nickl M, Albu-Schaffer A, Ott C, Jorg S, Konietschke R, Le-Tien L, Hirzinger G. A hands-on-robot for accurate placement of pedicle screws. In: Proceedings of the 2006 IEEE International Conference on Robotics and Automation. Washington, DC: IEEE; 2006.
- 15.Pechlivanis I, Kiriyanthan G, Engelhardt M, Scholz M, Lucke S, Harders A, Schmieder K. Percutaneous placement of pedicle screws in the lumbar spine using a bone mounted miniature robotic system: first experiences and accuracy of screw placement. Spine (Phila Pa 1976). 2009;34:392–398. doi: 10.1097/BRS.0b013e318191ed32. [DOI] [PubMed] [Google Scholar]
- 16.Rajasekaran S, Vidyadhara S, Ramesh P, Shetty AP. Randomized clinical study to compare the accuracy of navigated and non-navigated thoracic pedicle screws in deformity correction surgeries. Spine (Phila Pa 1976). 2007;32:E56–E64. doi: 10.1097/01.brs.0000252094.64857.ab. [DOI] [PubMed] [Google Scholar]
- 17.Ringel F, Stuer C, Reinke A, Preuss A, Behr M, Auer F, Stoffel M, Meyer B. Accuracy of robot-assisted placement of lumbar and sacral pedicle screws: a prospective randomized comparison to conventional freehand screw implantation. Spine (Phila Pa 1976). 2012;37:E496–E501. doi: 10.1097/BRS.0b013e31824b7767. [DOI] [PubMed] [Google Scholar]
- 18.Shoda N, Nakajima S, Seichi A, Kan A, Iwasaki M, Kitagawa T, Kawaguchi H, Nakamura K. Computer-assisted anterior spinal surgery for a case of recurrent giant cell tumor. J Orthop Sci. 2002;7:392–396. doi: 10.1007/s007760200065. [DOI] [PubMed] [Google Scholar]
- 19.Sukovich W, Brink-Danan S, Hardenbrook M. Miniature robotic guidance for pedicle screw placement in posterior spinal fusion: early clinical experience with the SpineAssist. Int J Med Robot. 2006;2:114–122. doi: 10.1002/rcs.86. [DOI] [PubMed] [Google Scholar]
- 20.Togawa D, Kayanja MM, Reinhardt MK, Shoham M, Balter A, Friedlander A, Knoller N, Benzel EC, Lieberman IH. Bone-mounted miniature robotic guidance for pedicle screw and translaminar facet screw placement. Part 2. Evaluation of system accuracy. Neurosurgery. 2007;60:ONS129–ONS139. doi: 10.1227/01.NEU.0000249257.16912.AA. [DOI] [PubMed] [Google Scholar]
- 21.Wang HC, Yang YL, Lin WC, Chen WF, Yang TM, Lin YJ, Rau CS, Lee TC. Computer-assisted pedicle screw placement for thoracolumbar spine fracture with separate spinal reference clamp placement and registration. Surg Neurol. 2008;69:597–601. doi: 10.1016/j.surneu.2007.04.006. [DOI] [PubMed] [Google Scholar]