

Abstract
Background:
Increased requirement and decreased dietary intakes of micronutrients during pregnancy might affect maternal health and pregnancy outcomes. This study was aimed to examine the effects of two types of multiple micronutrient supplementations on pregnancy outcomes in Kashan, Iran.
Methods:
In a randomized single-blind controlled clinical trial, 104 primigravid singleton pregnant women aged 18-30 years were randomly assigned to receive either a multivitamin (n = 51) or a multivitamin-mineral (n = 53) supplements for 20 weeks. Participants consumed supplements once a day at week 16 of gestation. Maternal anthropometric data as well as newborn's weight, height, head circumference and 5-min Apgar score were also determined. Independent samples t-test was used for comparing between-group means. Multivariate linear regression analysis was used to identify determinants of newborn's weight, height and head circumference.
Results:
Women taking multivitamin-mineral supplements gained marginally less weight until week 28 than those taking multivitamin supplements (weight at week 28 of gestation: 67.5 ± 11.4 vs. 71.6 ± 10.3 kg, P = 0.06). Mean body mass index at week 28 (25.8 ± 4.0 vs. 28.4 ± 3.7 kg/m2, P = 0.001) as well as at delivery (28.0 ± 3.9 vs. 30.1 ± 3.8 kg/m2, P = 0.006) was lower among women taking multivitamin-mineral supplements than those taking multivitamin supplements. Although no significant difference was seen in newborns’ height and Apgar score between the two groups, mean birth weight (3.3 ± 0.4 vs. 3.1 ± 0.4 kg, P = 0.04) and head circumference (35 ± 1.4 vs. 34 ± 1.3 cm, P < 0.0001) of the infants whose mothers receiving multivitamin-mineral supplements were higher than those whose mothers received multivitamins. Multivitamin-mineral use by pregnant women was a significant predictor of infants’ weight (β =0.191, P = 0.03) and head circumference (β =0.907, P = 0.005).
Conclusions:
In conclusion, we found that birth weight and head circumference was increased in infants whose mothers received multivitamin-mineral supplements for 5 months during pregnancy compared with infants whose mothers received multivitamin supplements.
Keywords: Birth head circumference, birth weight, multivitamin, multivitamin-mineral, pregnancy outcome
INTRODUCTION
Appropriate nutrition during the pregnancy plays an important role in the growth and development of the fetus.[1,2,3] Pregnant women are one of the most susceptible groups for nutritional insufficiency due to increased requirements of micronutrients during the period of pregnancy. Several studies have reported insufficient dietary micronutrients intake in pregnant women.[1,2] Increased metabolic demands for micronutrients during pregnancy occur mainly due to changes in the women's physiology and the requirements of the growing fetus.[4,5] Micronutrient deficiencies during pregnancy might lead to spontaneous abortion, fetal malformation,[6] placental abruption,[7] increased maternal morbidity[8] as well as low birth weight (LBW) babies.[9] Approximately, 16% of all live births worldwide are LBW; 90% of which are born in low-income countries.[10] This rate is considerably high in Asian countries.[11] It is, therefore, expected that providing multiple micronutrients, rather than iron and folic acid (IFA) alone, as currently recommended, might beneficially affect both maternal health and fetal growth.
Several investigators have evaluated the effect of multiple micronutrients supplementation on pregnancy outcome.[12,13,14,15,16] Micronutrient supplementation during pregnancy has been reported to improve fetal growth compared with the placebo; however, no significant difference was found compared to iron or IFA supplementation.[17] In a study in Nepal, multiple micronutrient supplementations during pregnancy did not reduce early infant mortality;[18] however, it led to improved folate status and reduced the prevalence of riboflavin, vitamin B6, vitamin B12, folate and vitamin D deficiencies.[19] Evidence for the impact of micronutrient supplementation on pregnancy outcomes is still inadequate and further research is required before a switch from iron-folate supplementation is implemented.[17] Furthermore, most of the previous studies have been conducted in communities with a high prevalence of maternal malnutrition and it remains unknown if these supplementations would improve pregnancy outcomes in other populations. In addition, earlier studies have mostly compared micronutrient supplementation with the placebo intake. Although few studies have assessed maternal multiple micronutrient supplementation with IFA, to the best of our knowledge no report is available examining the efficacy of multivitamin supplements compared with multivitamin-mineral supplements on pregnancy outcomes. This study was therefore performed to investigate the effects of two types of maternal multiple micronutrient (multivitamin vs. multivitamin-mineral) supplementation on maternal health and pregnancy outcomes in Iranian pregnant women.
METHODS
Participants
This randomized single-blind controlled clinical trial was carried out in Kashan, Iran during March 2010 to May 2011. On the basis of sample size formula suggested for randomized clinical trials,[1] we considered the type I error of 5% (α =0.05) and type II error of 20% (β =0.2; Power = 80%) and birth weight as a key variable, we reached the sample size of 51 persons for each group. The present study was carried out in the Naghavi Maternity Clinic, Shaheed Beheshti Subspecialty Polyclinic and twenty four antenatal centers, affiliated to Kashan University of Medical Sciences. A total of 104 primigravida pregnant women aged range from 18 to 30 years who were carrying a singleton pregnancy participated in the current study. Multiparous women as well as those with hypertension, mild and severe pre-eclampsia, intrauterine growth retardation (IUGR), intra-uterine fetal death, gestational diabetes mellitus (GDM), completed bed rest (CBR), history or evidence of rheumatoid arthritis, thyroid, parathyroid or adrenal diseases, hepatic or renal failure and metabolic bone disease were not included in the current study. All pregnant women were taking 400 μg/d folic acid supplements from the beginning of pregnancy as well as 30 mg/d ferrous sulfate from the second trimester. The study was performed according to the guidelines expressed in the Declaration of Helsinki and approved by the Ethics Committee of Kashan University of Medical Sciences, Kashan, Iran. All participants provided informed written consent.
Study design
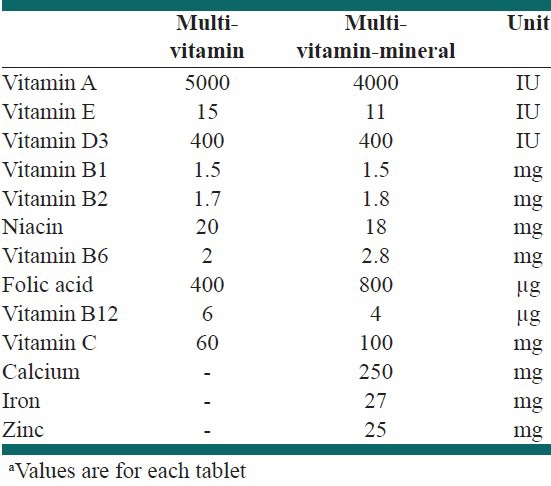
Subjects were randomly assigned to receive either a multivitamin (n = 51) or multivitamin-mineral supplements (n = 53) from week 16 of gestation through to delivery. All participants were asked to take one supplement a day orally. They were also asked not to alter their routine physical activity and usual diet throughout the study. The multivitamin and multivitamin-mineral supplements were provided by Shahre Daru Co., Tehran, Iran and NatureMade Co., USA, respectively. Supplements were provided to subjects monthly. We kept all supplements in a cool temperature before using. Compliance with the supplements consumption was monitored once per month through phone interviews. The composition of the supplements is provided in Table 1.
Table 1.
Composition of dietary supplements used in the studya
Data collection
Detailed information about health and reproductive status, supplement use and life-style were collected through the use of a questionnaire by face-to-face interview. Gestational age was calculated from the date of last menstrual period and concurrent clinical assessment.[20] Data on pre-pregnancy weight and height (measured values) were taken from the records of pregnant women existed in the clinic. Maternal weight at week 16 and 28 of gestation and on delivery was measured (Digital Floor Scale; Seca, Hamburg, Germany) without shoes and with minimum clothing to the nearest 0.1 kg. Height was measured using a non-stretchable tape measure and recorded to the nearest 0.1 cm (Seca, Hamburg, Germany). Body mass index (BMI) was calculated as weight in kilogram divided by height in meters squared. Newborn's height and weight were measured using standard methods (Seca 155 Scale, Hamburg, Germany) during the first 24 h after birth and were recorded to the nearest 1 mm and 10 g, respectively. Newborn's head circumference was measured to the nearest 1 mm with a Seca girth measuring tape. We also determined newborn's 5-min Apgar score as another measure of pregnancy outcome.
Statistical analysis
To ensure normal distribution of variables, Kolmogrov-Smirnov test was applied. We used independent samples t-test to compare means between the two groups. To assess if the magnitude of the changes depended on pre-pregnancy and baseline BMI values, we conditioned all analyses on pre-pregnancy and baseline BMI values to avoid the potential bias that might have resulted. These adjustments were done using analysis of covariance. Multivariate linear regression analysis was used to identify determinants of pregnancy outcomes in this population. In these analyses, supplement use was treated as dichotomous variable (multivitamin use = 0 and multi-vitamin-mineral consumption = 1). All other possible determinants of pregnancy outcomes including maternal age, height, pre-pregnancy weight, maternal weight at week 16 and 28, maternal weight at delivery as well as gestational age were simultaneously considered in these regression models. Before entering the variables in the linear regression model, we examined the correlation between the variables. The stability of the models was considered to be disturbed by the multi-colinearity if tolerance was <0.1. As we did not find any evidence of multi-colinearity, therefore all variables were entered simultaneously to the model. P < 0.05 was considered to be statistically significant. All analyses were performed by the use of statistical package for social sciences (SPSS, version 17; SPSS Inc., Chicago, Illinois, USA).
RESULTS
Among individuals in a multivitamin group, 4 women (pre-eclampsia [n = 2], GDM [n = 1] and CBR [n = 1]) were excluded. The exclusions in a multivitamin-mineral group was 2 persons (pre-eclampsia [n = 1] and CBR [n = 1]). Finally, 104 participants a multivitamin group (n = 51) and a multivitamin-mineral (n = 53) completed the trial [Figure 1].
Figure 1.
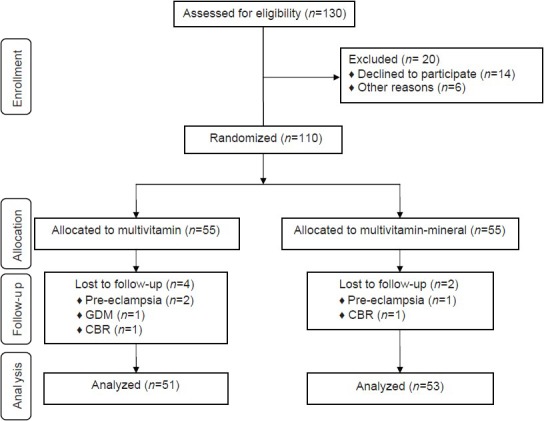
Summary of patient flow. GDM=Gestational diabetes mellitus, CBR=Completed bed rest
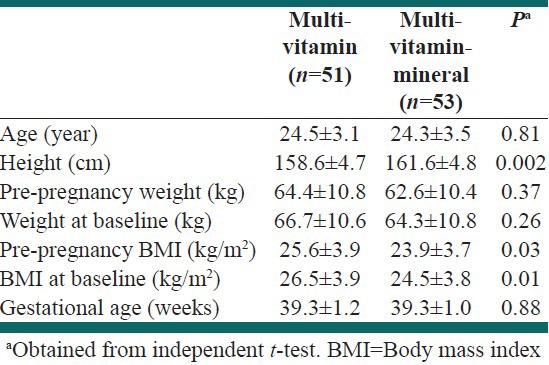
Characteristics of the study population are provided in Table 2. Mean age of the studied population was 24.4 years with no significant difference between the two groups. Women in the multi-vitamin-mineral group were significantly taller than those in the multivitamin group (161.6 ± 4.8 vs. 158.6 ± 4.7 cm, P = 0.002). Although we did not find a significant difference in pre-pregnancy weight between the two groups, pre-pregnancy BMI was significantly higher among women taking multi-vitamin compared with those taking multivitamin-mineral (25.6 ± 3.9 vs. 23.9 ± 3.7 kg/m2, P = 0.03). This was also the case for BMI at week 16 of gestation (26.5 ± 3.9 vs. 24.5 ± 3.8 kg/m2, P = 0.01). No significant difference in weight at week 16 was found between the two groups.
Table 2.
Baseline characteristics of the study participants
Women taking multivitamin-mineral supplements gained marginally less weight until week 28 than those taking multivitamin supplements (weight at week 28 of gestation: 67.5 ± 11.4 vs. 71.6 ± 10.3 kg, P = 0.06). Mean BMI at week 28 (25.8 ± 4.0 vs. 28.4 ± 3.7 kg/m2, P = 0.001) as well as at delivery (28.0 ± 3.9 vs. 30.1 ± 3.8 kg/m2, P = 0.006) was lower among women taking multivitamin-mineral supplements than those taking multivitamin supplements. Although no significant difference was seen in newborns’ height and Apgar score between the two groups, mean birth weight (3.3 ± 0.4 vs. 3.1 ± 0.4 kg, P = 0.04) and head circumference (35 ± 1.4 vs. 34 ± 1.3 cm, P < 0.0001) of the infants whose mothers receiving multivitamin-mineral supplements were higher than those whose mothers received multivitamins [Table 3]. After adjustment for pre-pregnancy and baseline BMI values, the above-mentioned findings remained significant, except for weight at delivery (P = 0.02) and BMI at delivery (P = 0.22).
Table 3.
The effect of dietary supplements on maternal weight gain and pregnancy outcomesa

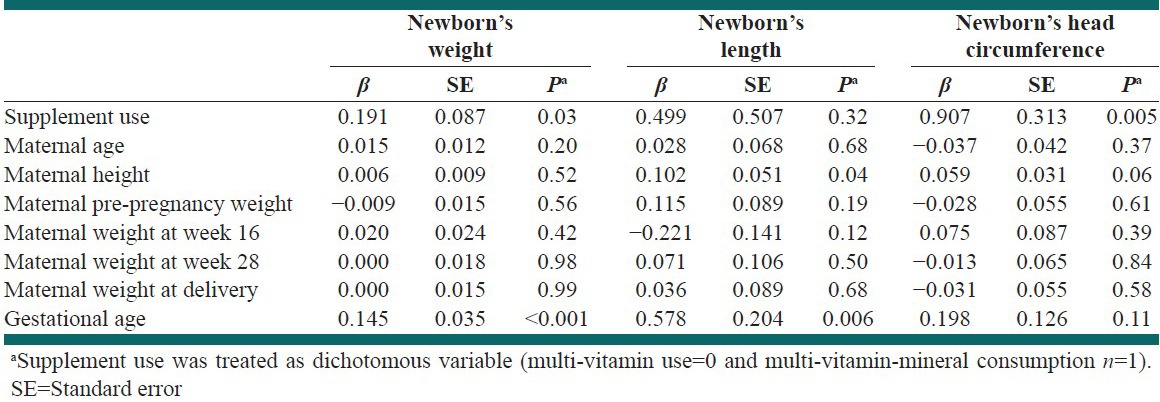
Regression coefficients for identification of factors influencing infants’ weight, length and head circumference are indicated in Table 4. Multivitamin-mineral use by pregnant women was a significant predictor of infants’ weight (β = 0.191, P = 0.03) and head circumference (β = 0.907, P = 0.005). Gestational age has been found as a significant contributor to infants’ birth weight (β = 0.145, P < 0.0001) and length (β = 0.578, P = 0.006). We also found that infants’ length is affected by maternal height as well (β = 0.102, P = 0.04). No significant associations were found between mothers’ weight and their infants’ birth sizes.
Table 4.
Regression coefficients to identify determinants of pregnancy outcomes
DISCUSSION
In the present study, we found that multivitamin-mineral supplementations along with other routine supplements used in pregnancy would significantly affect infants’ birth weight and head circumference compared with multivitamin supplements.
Earlier studies have assessed the effect of multiple micronutrients supplementation during pregnancy on birth size.[21,22,23,24,25,26,27,28] Most of the previous studies have compared multivitamin-mineral supplements with placebo or IFA supplement. To the best of our knowledge, this is the first study in which the use of multivitamin-mineral supplements in pregnant women has been compared with multivitamin supplements. Furthermore, this study has assessed this comparison along with the other routine supplements administered during pregnancy.
Replacing IFA supplements with multiple micronutrient supplements during pregnancy has been reported to improve both birth weight and child growth. Furthermore, meaningful improvements have been shown in height and cognitive development of children by 2 years of age.[16] Multiple micronutrient supplements from week 12 to 16 of gestation to delivery resulted in a significant increase in birth size compared with placebo, but did not affect head circumference.[29] Unlike these studies, Sunawang et al. in a cluster-randomized controlled trial among pregnant women found no significant difference in birth weight of infants whose mothers receiving multiple micronutrients supplements for 5 days/week compared with those whose mothers taking IFA supplements.[21] Such finding has also been reached when the pregnant women receiving multiple micronutrients supplement for 6 days/week from week 13 of gestation through delivery was compared with those receiving iron supplements.[25] In a double-blind randomized controlled trial in rural Burkina Faso, multiple micronutrient supplementations was associated with increased birth weight and height compared with standard IFA, but the differences were not statistically significant.[11] Multiple micronutrients supplementation has also been reported to have no additional benefits over folic acid-iron supplements on birth length and infants’ head circumference and on lowering incidence of preterm birth; however, it has led to increased birth weight by 7 g.[30] Different findings might be explained by the different study designs, sample sizes, duration and dosage of supplementation as well as composition of nutrients used in supplements. Most of previous studies have used usual multi-micronutrient supplements available in the marker, but we used supplements that were prepared for pregnancy period. For instance, the supplements used in previous studies did not contain some potentially important micronutrients, like calcium, but the high amount of calcium (250 mg) and zinc (27 mg) in multi-prenatal supplements we used might affect birth weight and head circumference. In a study in India, when 14 other micronutrients were added to UNICEF/WHO/UNU-designed supplements for pregnant women; impressive results on birth size were observed.[31] Furthermore, several studies have indicated that deficiencies of zinc,[5,13] iron[32,33] and calcium[34] during pregnancy could affect birth size. In the current study, the folic acid content of the multivitamin-mineral supplement was 2 times higher than the multivitamin supplement alone. It seems that folic acid has a positive effect on infants’ size. In a study by Rao et al.[35] has been reported that maternal erythrocyte folate at 28 week gestation was positively associated with birth weight. Some randomized trials have also been shown that prenatal use of vitamins, including folic acid, is associated with infant birth size.[36,37] The improvement in the birth size due to high content of folic acid in the multivitamin-mineral supplement group may be resulted from its effect in the increase of placental size, cell number[38] and rescue the gene expressions negatively induced by IUGR.[39] Despite the non-significant effect of received supplements by pregnant women in this study, we found a significant predictor of between the two groups in terms of their effects on infants’ weight and length. In consistent our study, several researchers have also been shown that birth size is associated with gestational age.[40,41] Emerging evidence indicates that the use of micronutrient-containing prenatal vitamins during pregnancy is associated with reduced risk of congenital defects, preterm delivery, LBW and pre-eclampsia.[42] It must be kept in mind that the current study has been performed in a developing country setting. The dietary reference intakes of micronutrients for pregnant women is based on requirements of women residing in the United States or Canada. Such levels might be insufficient to meet the requirements of pregnant women living in communities with mild to moderate deficiencies of micronutrients. In Guinea-Bissau, providing supplements containing twice the RDA of micronutrients resulted in a lower incidence of LBW infants by 69%.[43] In Tanzania, when micronutrient supplements providing amounts twice the recommended dietary allowance (RDA) for vitamin E and 6-10 times for vitamin C and several B vitamins were administered, mean birth weight increased by 67 g.[36] Finally, the provision of multivitamin and multivitamin-mineral supplements from two different pharmaceutical companies might be influenced infants’ size.
Our findings must be interpreted in the context of some limitations. As the current study included both underweight (BMI < 20) and obese (BMI ≥ 30 kg/m2) participants, therefore the findings must be interpreted cautiously because both underweight and overweight has been shown to influence pregnancy outcomes. In addition, we could not assess the effects of micronutrients supplementation on biochemical indicators of newborns.
CONCLUTIONS
we found that compared with those who had multivitamin supplements, pregnant women that received multivitamin-mineral supplements for 5 months during pregnancy had babies with higher birth weight and head c ircumference.
ACKNOWLEDGMENT
The present study was supported by a grant from the Vice-chancellor for Research, KUMS and Iran. The authors would like to thank the staff of Naghavi and Shaheed Beheshti Clinics, Kashan, Iran for their assistance in this project.
Footnotes
Source of Support: The study was supported by a grant from Kashan University of Medical Sciences, Kashan, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Shah PS, Ohlsson A. Knowledge synthesis group on determinants of low birth weight and preterm births. Effects of prenatal multimicronutrient supplementation on pregnancy outcomes: A meta-analysis. CMAJ. 2009;180:E99–108. doi: 10.1503/cmaj.081777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Allen LH. Multiple micronutrients in pregnancy and lactation: An overview. Am J Clin Nutr. 2005;81:1206S–12. doi: 10.1093/ajcn/81.5.1206. [DOI] [PubMed] [Google Scholar]
- 3.Asemi Z, Jazayeri S, Najafi M, Samimi M, Mofid V, Shidfar F, et al. Effects of daily consumption of probiotic yoghurt on inflammatory factors in pregnant women: A randomized controlled trial. Pak J Biol Sci. 2011;14:476–82. doi: 10.3923/pjbs.2011.476.482. [DOI] [PubMed] [Google Scholar]
- 4.King JC. Determinants of maternal zinc status during pregnancy. Am J Clin Nutr. 2000;71:1334S–43. doi: 10.1093/ajcn/71.5.1334s. [DOI] [PubMed] [Google Scholar]
- 5.Hess SY, King JC. Effects of maternal zinc supplementation on pregnancy and lactation outcomes. Food Nutr Bull. 2009;30:S60–78. doi: 10.1177/15648265090301S105. [DOI] [PubMed] [Google Scholar]
- 6.Ashworth CJ, Antipatis C. Micronutrient programming of development throughout gestation. Reproduction. 2001;122:527–35. [PubMed] [Google Scholar]
- 7.Pathak P, Kapil U. Role of trace elements zinc, copper and magnesium during pregnancy and its outcome. Indian J Pediatr. 2004;71:1003–5. doi: 10.1007/BF02828116. [DOI] [PubMed] [Google Scholar]
- 8.Seshadri S. Prevalence of micronutrient deficiency particularly of iron, zinc and folic acid in pregnant women in South East Asia. Br J Nutr. 2001;85(Suppl 2):S87–92. [PubMed] [Google Scholar]
- 9.Pathak P, Kapil U, Kapoor SK, Saxena R, Kumar A, Gupta N, et al. Prevalence of multiple micronutrient deficiencies amongst pregnant women in a rural area of Haryana. Indian J Pediatr. 2004;71:1007–14. doi: 10.1007/BF02828117. [DOI] [PubMed] [Google Scholar]
- 10.de Onis M, Blössner M, Villar J. Levels and patterns of intrauterine growth retardation in developing countries. Eur J Clin Nutr. 1998;52:S5–15. [PubMed] [Google Scholar]
- 11.Roberfroid D, Huybregts L, Lanou H, Henry MC, Meda N, Menten J, et al. Effects of maternal multiple micronutrient supplementation on fetal growth: A double-blind randomized controlled trial in rural Burkina Faso. Am J Clin Nutr. 2008;88:1330–40. doi: 10.3945/ajcn.2008.26296. [DOI] [PubMed] [Google Scholar]
- 12.Brough L, Rees GA, Crawford MA, Morton RH, Dorman EK. Effect of multiple-micronutrient supplementation on maternal nutrient status, infant birth weight and gestational age at birth in a low-income, multi-ethnic population. Br J Nutr. 2010;104:437–45. doi: 10.1017/S0007114510000747. [DOI] [PubMed] [Google Scholar]
- 13.Christian P. Micronutrients, birth weight, and survival. Annu Rev Nutr. 2010;30:83–104. doi: 10.1146/annurev.nutr.012809.104813. [DOI] [PubMed] [Google Scholar]
- 14.Haider BA, Yakoob MY, Bhutta ZA. Effect of multiple micronutrient supplementation during pregnancy on maternal and birth outcomes. BMC Public Health. 2011;11:S19. doi: 10.1186/1471-2458-11-S3-S19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Margetts BM, Fall CH, Ronsmans C, Allen LH, Fisher DJ Maternal Micronutrient Supplementation Study Group. Multiple micronutrient supplementation during pregnancy in low-income countries: Review of methods and characteristics of studies included in the meta-analyses. Food Nutr Bull. 2009;30:S517–26. doi: 10.1177/15648265090304S406. [DOI] [PubMed] [Google Scholar]
- 16.Shrimpton R, Huffman SL, Zehner ER, Darnton-Hill I, Dalmiya N. Multiple micronutrient supplementation during pregnancy in developing-country settings: Policy and program implications of the results of a meta-analysis. Food Nutr Bull. 2009;30:S556–73. doi: 10.1177/15648265090304S410. [DOI] [PubMed] [Google Scholar]
- 17.Haider BA, Bhutta ZA. Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst Rev. 2006;18:CD004905. doi: 10.1002/14651858.CD004905.pub2. [DOI] [PubMed] [Google Scholar]
- 18.Christian P, Osrin D, Manandhar DS, Khatry SK, de L Costello AM, West KP., Jr Antenatal micronutrient supplements in Nepal. Lancet. 2005;366:711–2. doi: 10.1016/S0140-6736(05)67166-8. [DOI] [PubMed] [Google Scholar]
- 19.Christian P, Jiang T, Khatry SK, LeClerq SC, Shrestha SR, West KP., Jr Antenatal supplementation with micronutrients and biochemical indicators of status and subclinical infection in rural Nepal. Am J Clin Nutr. 2006;83:788–94. doi: 10.1093/ajcn/83.4.788. [DOI] [PubMed] [Google Scholar]
- 20.Gupta P, Narang M, Banerjee BD, Basu S. Oxidative stress in term small for gestational age neonates born to undernourished mothers: A case control study. BMC Pediatr. 2004;4:14. doi: 10.1186/1471-2431-4-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sunawang, Utomo B, Hidayat A, Kusharisupeni, Subarkah Preventing low birthweight through maternal multiple micronutrient supplementation: A cluster-randomized, controlled trial in Indramayu, West Java. Food Nutr Bull. 2009;30:S488–95. doi: 10.1177/15648265090304S403. [DOI] [PubMed] [Google Scholar]
- 22.Shah D, Sachdev HP. Maternal micronutrients and fetal outcome. Indian J Pediatr. 2004;71:985–90. doi: 10.1007/BF02828113. [DOI] [PubMed] [Google Scholar]
- 23.Rasmussen KM, Habicht JP. Maternal supplementation differentially affects the mother and newborn. J Nutr. 2010;140:402–6. doi: 10.3945/jn.109.114488. [DOI] [PubMed] [Google Scholar]
- 24.Ramakrishnan U, González-Cossío T, Neufeld LM, Rivera J, Martorell R. Effect of prenatal multiple micronutrient supplements on maternal weight and skinfold changes: A randomized double-blind clinical trial in Mexico. Food Nutr Bull. 2005;26:273–80. doi: 10.1177/156482650502600304. [DOI] [PubMed] [Google Scholar]
- 25.Ramakrishnan U, González-Cossío T, Neufeld LM, Rivera J, Martorell R. Multiple micronutrient supplementation during pregnancy does not lead to greater infant birth size than does iron-only supplementation: A randomized controlled trial in a semirural community in Mexico. Am J Clin Nutr. 2003;77:720–5. doi: 10.1093/ajcn/77.3.720. [DOI] [PubMed] [Google Scholar]
- 26.Nilsen RM, Vollset SE, Monsen AL, Ulvik A, Haugen M, Meltzer HM, et al. Infant birth size is not associated with maternal intake and status of folate during the second trimester in Norwegian pregnant women. J Nutr. 2010;140:572–9. doi: 10.3945/jn.109.118158. [DOI] [PubMed] [Google Scholar]
- 27.Neggers Y, Goldenberg RL. Some thoughts on body mass index, micronutrient intakes and pregnancy outcome. J Nutr. 2003;133:1737S–40. doi: 10.1093/jn/133.5.1737S. [DOI] [PubMed] [Google Scholar]
- 28.Muthayya S. Maternal nutrition and low birth weight-what is really important? Indian J Med Res. 2009;130:600–8. [PubMed] [Google Scholar]
- 29.Hininger I, Favier M, Arnaud J, Faure H, Thoulon JM, Hariveau E, et al. Effects of a combined micronutrient supplementation on maternal biological status and newborn anthropometrics measurements: A randomized double-blind, placebo-controlled trial in apparently healthy pregnant women. Eur J Clin Nutr. 2004;58:52–9. doi: 10.1038/sj.ejcn.1601745. [DOI] [PubMed] [Google Scholar]
- 30.Christian P, Khatry SK, Katz J, Pradhan EK, LeClerq SC, Shrestha SR, et al. Effects of alternative maternal micronutrient supplements on low birth weight in rural Nepal: Double blind randomised community trial. BMJ. 2003;326:571. doi: 10.1136/bmj.326.7389.571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ashworth A. Effects of intrauterine growth retardation on mortality and morbidity in infants and young children. Eur J Clin Nutr. 1998;52(Suppl 1):S34–41. [PubMed] [Google Scholar]
- 32.Stewart CP, Christian P, LeClerq SC, West KP, Jr, Khatry SK. Antenatal supplementation with folic acid+iron+zinc improves linear growth and reduces peripheral adiposity in school-age children in rural Nepal. Am J Clin Nutr. 2009;90:132–40. doi: 10.3945/ajcn.2008.27368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Veghari G. Iron supplementation during pregnancy and birth weight in Iran: A retrospective study. Pak J Biol Sci. 2009;12:427–32. doi: 10.3923/pjbs.2009.427.432. [DOI] [PubMed] [Google Scholar]
- 34.Morley R, Carlin JB, Dwyer T. Maternal calcium supplementation and cardiovascular risk factors in twin offspring. Int J Epidemiol. 2004;33:1304–9. doi: 10.1093/ije/dyh284. [DOI] [PubMed] [Google Scholar]
- 35.Rao S, Yajnik CS, Kanade A, Fall CH, Margetts BM, Jackson AA, et al. Intake of micronutrient-rich foods in rural Indian mothers is associated with the size of their babies at birth: Pune Maternal Nutrition Study. J Nutr. 2001;131:1217–24. doi: 10.1093/jn/131.4.1217. [DOI] [PubMed] [Google Scholar]
- 36.Fawzi WW, Msamanga GI, Urassa W, Hertzmark E, Petraro P, Willett WC, et al. Vitamins and perinatal outcomes among HIV-negative women in Tanzania. N Engl J Med. 2007;356:1423–31. doi: 10.1056/NEJMoa064868. [DOI] [PubMed] [Google Scholar]
- 37.Rolschau J, Kristoffersen K, Ulrich M, Grinsted P, Schaumburg E, Foged N. The influence of folic acid supplement on the outcome of pregnancies in the county of Funen in Denmark. Part I. Eur J Obstet Gynecol Reprod Biol. 1999;87:105–10. [PubMed] [Google Scholar]
- 38.Bergen NE, Jaddoe VW, Timmermans S, Hofman A, Lindemans J, Russcher H, et al. Homocysteine and folate concentrations in early pregnancy and the risk of adverse pregnancy outcomes: The Generation R Study. BJOG. 2012;119:739–51. doi: 10.1111/j.1471-0528.2012.03321.x. [DOI] [PubMed] [Google Scholar]
- 39.Liu JB, Chen DW, Yu B, Mao XB. Effect of maternal folic acid supplementation on hepatic one-carbon unit associated gene expressions in newborn piglets. Mol Biol Rep. 2011;38:3849–56. doi: 10.1007/s11033-010-0500-9. [DOI] [PubMed] [Google Scholar]
- 40.Oshiro C, Grove J, Novotny R. PS2-27: Birth size, gestational age, and BMI at age 5y. Clin Med Res. 2012;10:186. [Google Scholar]
- 41.Camarano L, Alkon A, Nachtigall RD, Schembri M, Weiss S, Croughan MS. Preterm delivery and low birth weight in singleton pregnancies conceived by women with and without a history of infertility. Fertil Steril. 2012;98:681–6.e1. doi: 10.1016/j.fertnstert.2012.04.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Scholl TO. Maternal nutrition before and during pregnancy. Nestle Nutr Workshop Ser Pediatr Program. 2008;61:79–89. doi: 10.1159/000113172. [DOI] [PubMed] [Google Scholar]
- 43.Kaestel P, Michaelsen KF, Aaby P, Friis H. Effects of prenatal multimicronutrient supplements on birth weight and perinatal mortality: A randomised, controlled trial in Guinea-Bissau. Eur J Clin Nutr. 2005;59:1081–9. doi: 10.1038/sj.ejcn.1602215. [DOI] [PubMed] [Google Scholar]