

Recent progress in medical technology has markedly improved the prognosis for people with diabetic mellitus. In contrast, rapid changes in lifestyles have increased the number of people with impaired glucose metabolism, resulting in greater numbers of elderly diabetic patients.
It is generally accepted that impaired cognitive function is more common in patients with diabetes than those without, regardless of whether the diabetes is type 1 or type 21. Future progression to dementia reduces quality of life and imposes a burden on both patients themselves and the families supporting them. Therefore, preventing the complication of dementia will become even more important than it is now.
Although many factors are thought to be involved in impaired cognitive function, the mechanisms are very complex and have not been fully resolved1,2. We have to discuss mechanisms separately for patients with type 1 and type 2 diabetes mellitus, because of the different backgrounds. In particular, evaluation of the contribution of various factors to cognitive dysfunction, which include concomitant hypertension, dyslipidemia and complicated cerebral vascular disease, as well as changes in the brain and other organs as a result of aging, is difficult for elderly type 2 diabetes because they are very intricate in nature. Also, the two major types of dementia – cerebral vascular dementia and Alzheimer’s disease, and a mixed type including aspects of both – should be taken into consideration in middle‐aged and elderly subjects. However, in adolescent and middle‐aged type 1 diabetic patients, a consideration of the complications of Alzheimer’s disease might be excluded and only the direct effects as a result of hyperglycemia and hypoglycemia might be investigated. However, it is noteworthy that cognitive impairment observed in type 1 diabetes is generally subtle and it is unknown whether it will actually lead to future dementia. In addition, few large‐scale, longstanding longitudinal studies have been carried out.
The DCCT/EDIC study, in which 1144 patients with type 1 diabetes were followed up for an average of 18 years and a variety of cognitive function tests were carried out, is a very interesting and significant study. It did not find evidence for a substantial long‐term decline in cognitive function in the large group of patients who were carefully followed up, despite relatively high rates of recurrent severe hypoglycemia. Higher glycated hemoglobin levels were associated with moderate declines in motor speed and psychomotor efficiency, but not other domains3. Recently, an association of other biomedical risk factors and decreased cognitive functioning has been reported in Diabetologia4.
Although a modest association between cognitive impairment and smoking or hypertension was found by carrying out univariate analysis on the study results, retinal and renal complications, as well as glycemic control, were each independently associated with a decline in cognitive function, specifically affecting measures of psychomotor efficiency. These findings might indicate that long‐term hyperglycemia has an adverse effect not only on the microvasculature of the retina and kidney, but also on the small vessels in the brain. In fact, it has been previously reported that retinopathy was related to cognitive impairment in both type 1 and type 2 diabetes, and recently an association between the brain and kidney has been focused on, because of their similar microvasculature structures1,2.
Several mechanisms that mediate the toxic effects of hyperglycemia, such as oxidative stress, accumulation of advanced glycation end‐products and increased activity in the polyol pathway, have been implicated in damage to the brain, leading to cognitive dysfunction. However, most of the respective studies were carried out in animal models and such an association remains unclear. Interestingly, recent research using functional magnetic resonance imaging and positron emission tomography has detected elevated levels of brain glucose and glutamate, an excitatory neurotransmitter that can cause neuronal damage in high concentrations, in prefrontal regions in type 1 diabetic patients as compared with non‐diabetic controls. In addition, poorer metabolic control has been seen to be inversely correlated with levels of N‐acetylasparate and choline‐containing compounds in white matter and deep grey matter. These findings of study suggest that axonal injury, demyelination and increased membrane proliferation have occurred and might be a consequence of glucose neurotoxicity. This non‐vascular pathway could explain, at least in part, the recent observation that adults with a long history of type 1 diabetes manifest psychomotor slowing associated with microstructure damage to white matter fiber tracts1,4. In agreement with the present article, psychomotor efficiency, which reflects frontal lobe function, has been identified in other studies as the cognitive domain most often affected in patients with diabetes. Although the reason why frontal function is impaired in diabetic patients has not been clarified fully, it is thought to be a possible mechanism for prefrontal loop impairment as a result of silent brain infarct (SBI) in basal ganglia of the brain and hyperglycemia‐induced white matter lesions, which are likely to be found in diabetic patients.
In addition to hyperglycemia, an association between hypoglycemia attacks and decline in cognitive function has also been previously debated. Many studies on this theme have supported such a relationship, regardless of whether subjects have had type 1 or type 2 diabetes mellitus. However, clear evidence showing that frequent hypoglycemic episodes will lead to a longstanding decline in cognitive function in type 1 diabetes was not produced. In the DCCT/EDIC study, no associations between recurrent severe hypoglycemic attacks and a decline in cognitive function were observed. It might be because patients recruited for the DCCT/EDIC study were well controlled. Namely, if patients were carefully followed up, persistent hyperglycemia might have had a greater adverse effect on cognitive function than hypoglycemia. The relationship between cognitive function and hypoglycemic attacks is also discussed in a commentary in Diabetologia5.
As aforementioned, it seems reasonable to suppose that brain damage based on hyperglycemia is associated with a decline in cognitive function. Therefore, exaggerating things a bit, we could say that cognitive impairment is the fourth diabetic microvascular disease. If this is so, a hypothesis might be developed. Impaired endothelial function is known to contribute to the progression of diabetic vascular complications. Also, damage to the brain has been reported to be associated with impairment of the blood–brain barrier and such endothelial dysfunction might cause focal neural damage or ischemic changes through small vascular vessels, leading to cognitive impairment in type 1 diabetic patients. A partially similar phenomenon was found in type 2 diabetic patients. We have reported that levels of soluble adhesion molecules reflect endothelial function, especially intercellular adhesion molecule‐1, and there were associations with progression of cerebral small vessel disease and cognitive function in our cross‐sectional and longitudinal studies in middle‐aged and elderly type 2 diabetic patients6. It is unlikely that there would be visual findings in magnetic resonance imaging indicating SBI and white matter lesions in relatively young type 1 diabetic patients. However, one could easily suppose that longstanding endothelial dysfunction would cause progression in cerebral small vessel lesions. Endothelial function is impaired by not only hyperglycemia, but also many other factors, such as hypertension, dyslipidemia and smoking, and it has been reported that such impairment in middle‐aged people will lead to a future decline in cognitive function. Therefore, the early inhibition of such risk factors is important in the prevention of dementia7.
However, in contrast with young type 1 diabetes patients, the complications of Alzheimer’s disease should be always taken into account in elderly people. Although an association between Alzheimer’s disease and diabetes is becoming clearer, much still remains to be discovered. It has been suggested that the weakened action of insulin as a result of hyperinsulinemia or lack of insulin might interfere with Aβ metabolism by stimulating its secretion and inhibiting its breakdown. In fact, impaired cognition has been reported in patients with hyperinsulinemia and hypertension, and poorly controlled diabetic patients1,2,8.
Last, the effect of genetic factors should also be considered. The APOE ε4 allele is a representative genetic factor for Alzheimer’s disease. However, having this genetic factor is not necessarily associated with incidence of Alzheimer’s disease and it is thought that daily habits have a great impact in this regard. Recently, a variety of interesting studies have been carried out on modification of diabetes by this genotype.
In summary, many factors, as shown in Figure 1, contribute to cognitive dysfunction in type 1 and type 2 diabetes mellitus. Therefore, one might say that better control of hyperglycemia, hypertension and dyslipidemia, in addition to improvement of daily lifestyle – with respect to such aspects as smoking, exercise and diet – will prevent not only the progression of diabetic vascular disease, but also a future decline in cognitive function. Further examination of the results of large scale, longstanding research, such as the DCCT/EDIC study, is expected to clarify the respective mechanisms and help the prevention of dementia in people with diabetes mellitus.
Figure 1.
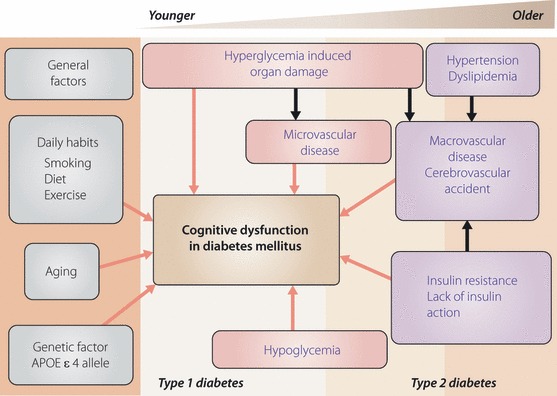
Summary of possible mechanistic contributors to cognitive dysfunction seen in diabetes mellitus.
References
- 1.Kodl CT, Seaquist ER. Cognitive dysfunction and diabetes mellitus. Endocr Rev 2008; 29: 494–511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Biessels GJ, Staekenborg S, Brunner E, et al. Risk of dementia in diabetes mellitus: a systematic review. Lancet Neurol 2006; 5: 69–74 [DOI] [PubMed] [Google Scholar]
- 3.The Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complicationa (DCCT/EDIC) Study Research Group . Long‐term effect of diabetes and its treatment on cognitive function. N Engl J Med 2007; 356: 1842–1852 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Jacobson AM, Ryan CM, Cleary PA, et al. Biomedical risk factors for decreased cognitive functioning in type 1 diabetes: an 18 year follow‐up of diabetes control and complications trial (DCCT) cohort. Diabetologia 2011; 54: 245–255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Frier BM. Cognitive functioning in type 1 diabetes: the Diabetes Control and Complicatins Trial (DCCT) revisited. Diabetologia 2010; 54: 233–236 [DOI] [PubMed] [Google Scholar]
- 6.Umemura T, Kawamura T, Umegaki H, et al. Endothelial and inflammatory markers in relation to progression of ischaemic cerebral small‐vessel disease and cognitive impairment: a 6‐year longitudinal study in patients with type 2 diabetes mellitus. J Neurol Neurosurg Psychiatry 2011. doi: 10.1136/jnnp.2010.217380 [DOI] [PubMed] [Google Scholar]
- 7.Alonso A, Mosley TH Jr, Gottesman RF, et al. Risk of dementia hospitalization associated with cardiovascular risk factors in midlife and older age: the Atherosclerosis Risk in Communities (ARIC) study. J Neurol Neurosurg Psychiatry 2009; 80: 1194–1201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Umegaki H, Kawamura T, Kawano N, et al. Factors associated with cognitive decline in elderly diabetics. Dement Geriatr Cogn Disord 2011; 1: 1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]