

Abstract
Objective:
To assess the level of fear of dental procedures among 6-12 year school children and correlate the prevalence of dental caries with their dental fears scores.
Materials and Methods:
The study sample of 444 school children, comprising of 224 girls and 220 boys in the age group of 6-12 years old from a private English medium school were selected. Each student was asked to independently complete a Children's Fear Survey Schedule – Dental Subscale (CFSS-DS) questionnaire. Children having a score of ≥ 38 were included in the “dental fear” group while those scoring <38 were placed in the “without dental fear” group. All dental examinations were performed in the classroom.
Results:
Fear scores were highest for “Injections,” (3.76 ± 0.68) “Choking,” (3.48 ± 0.63) and “Dentist drilling” (2.88 ± 0.69). The overall mean score of CFSS-DS in our study was 37.0 ± 8.89, mean score of DMFT and DMFS were 0.58 ± 0.74 and 0.73 ± 1.09, respectively. Mean score of deft and defs were 4.40 ± 2.34 and 7.28 ± 5.49, respectively.
Conclusion:
The study showed the prevalence of dental fear in 6-12 year old children and there was no statistically significant co-relation between the level of dental fear and dental caries in these children.
Keywords: Children, dental caries, dental fear, prevalence
INTRODUCTION
Dental fear in children has an overwhelming effect on their conduct which includes them to a have preconceived notion that the dental treatment will be of a painful nature. Dental fear hampers their ability to cope with clinical setting of a dental clinic, which in turn leads to failure to seek timely dental treatment.
Fear of the dentist has been ranked fourth among common fears.[1] Dental fear in children has been recognized in many countries as a public health problem.[2,3]
Dental fear has been also reported as one of the most important reasons for avoidance and negligence of regular dental care. Neglect of dental care may lead to dental decay and pain that usually results in a visit to the dentist which in turn increases the patient's original dental fear and thereby completing a vicious cycle. This problem may lead to neglect of dental care and therefore represents a problem to dentists and patient's alike.[3,4]
Therefore, it is of great importance that the dental health professional is able to identify children who have dental fear and apply appropriate pediatric management techniques at the earliest age possible.[5,6] The etiology of dental fear in children is multifactorial. Dental fear has been related to personality, increased general fears, and previous painful dental experiences, parental dental fear, age, and gender.[7,8] Girls and younger children are most often reported as more fearful than boys and older children.[8,9] Prevalence estimates of childhood dental fear vary considerably, from 3 to 43% in different populations.[9] These differences in prevalence estimates may be due to several parameters, such as methodological or cultural variables in the populations surveyed.[9] Dental fear scales have been used widely as a reliable tool to ascertain the level of dental fear in children so as to customize the various behavior management techniques and treatment plan based on the score. Hence, making the child's first dental experience an uneventful and pleasant one. Children's fear survey schedule was developed by Scherer and Nakamura. It consists of 80 items on a 5-point likert scale. It has been demonstrated to have high reliability and validity for measuring dental fear in children. The cumbersome nature of the questionnaire designed to be filled by the child patient has limited its use despite established validity report.[10] The Dental Subscale of Children's Fear Survey Schedule (CFSS-DS) developed by Cuthbert and Melamed[4,11] consists of 15 items and each item can be given five different scores ranging from “not afraid at all (1)” to “very much afraid (5).” The CFSS-DS has a total score range of 15 to 75 and a score of 38 or more has been associated with clinical dental fear.[11,12,13] It can be used to differentiate patients with high and low dental fears. Its reliability and validity have been aptly demonstrated.[14,15,16]
There are limited data correlating the level of dental fear among children and dental caries.
The aim of this cross sectional study was:
To assess the level of fear of dental procedures among 6-12 year school children and correlate the prevalence of dental caries with their dental fears scores.
To describe the gender distribution of these children according to level of dental fear.
Compare the mean DMFT, DMFS and deft, defs with CFSS-DS <38 and CFSS-DS ≥38 according to their age group.
MATERIALS AND METHODS
The study sample of 444 school children, comprising 224 girls and 220 boys in the age group of 6-12 years old from a private English medium school with moderate to high socioeconomic status were selected.
Inclusion criteria
Children above 6 years of age with good health and who had not received any dental treatment before but had visited a dental clinic with a parent and were familiar with all the dental procedures.
Exclusion criteria
Children below 6 years of age, with medical condition and who had sought dental treatment before.
Consent for conducting examination was obtained from all the parents and school authority. The study was approved by the Ethical Committee for Research.
The CFSS-DS consists of 15 items related to different aspects of dental treatment which were scored as follows: Not afraid = 1; a little afraid = 2; fairly afraid = 3; quite afraid = 4; and very afraid = 5. Total scores thus ranged from 15 to 75. Seventy-five indicating maximal fear [Table 1]. Children with CFSS-DS ≥38 were defined as dentally anxious.[17] The questionnaire was administered to the children in the classroom by teacher after explanation under the Pediatric dentist's supervision. The children were not allowed to discuss with each other and any doubts were clarified by a translator to their native language and then back to English for quality control. The survey took on an average 15 min to complete.
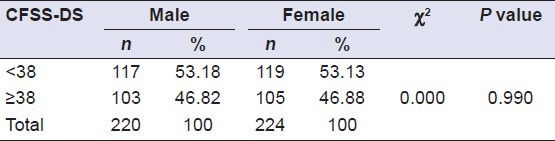
Table 1.
Gender distribution according to CFSS-DS score
Dental examination
All dental examinations were conducted in school by two trained and calibrated examiner. The diagnostic criteria used for caries were the same as those published by the WHO.[18] All decay-missing-filling teeth (DMF-T and DMF-S) were registered in permanent teeth, only decay, extracted filled teeth (def-t and def-s) were registered in deciduous teeth.
Caries prevalence data were collected using deft and DMFT by the same trained and calibrated examiner, according to the criteria of the World Health Organization (WHO). Examination was conducted by seating the child on a chair, using a disposable mouth mirror and probe and flash light was used to illuminate the oral cavity. White spot lesions were reported as normal and not recorded in deft or DMFT analyses.
The data obtained through the questionnaires were analyzed using Chi-Square test and Mann- Whitney U test.
RESULTS
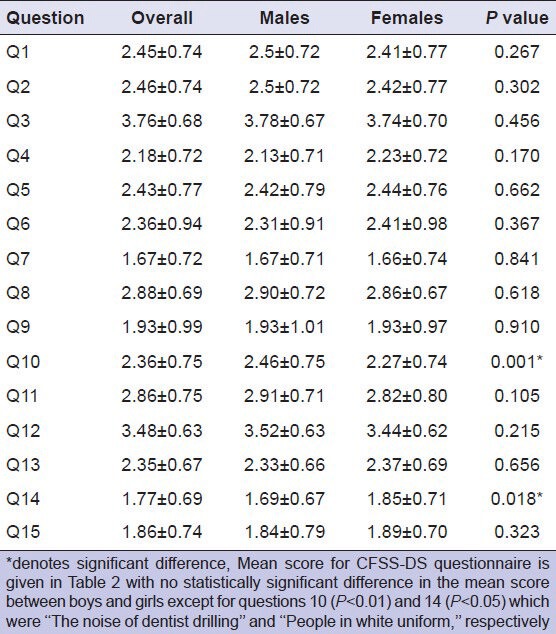
A total of 444 children were examined (males 220 and 224 females). Dental fear with CFSS-DS ≥38 was identified in 208 children [103 (46.82%) male and 105 (46.88% female]. A total of 236 children [117 (53.18%) male and 119 (53.13%) female] had CFSS-DS <38. There was no statistically significant difference between gender distribution and CFSS-DS (P > 0.05) as seen in Table 1. Mean score for CFSS-DS questionnaire is given in Table 2 with no statistically significant difference in the mean score between boys and girls except for questions 10 (P < 0.01) and 14 (P < 0.05) which were “The noise of dentist drilling” and “People in white uniform,” respectively. Fear scores were highest for “Injections” (3.76 ± 0.68), “Choking,” (3.48 ± 0.63) and “Dentist drilling” (2.88 ± 0.69).
Table 2.
Comparison of mean scores of CFSS-DS between males and females
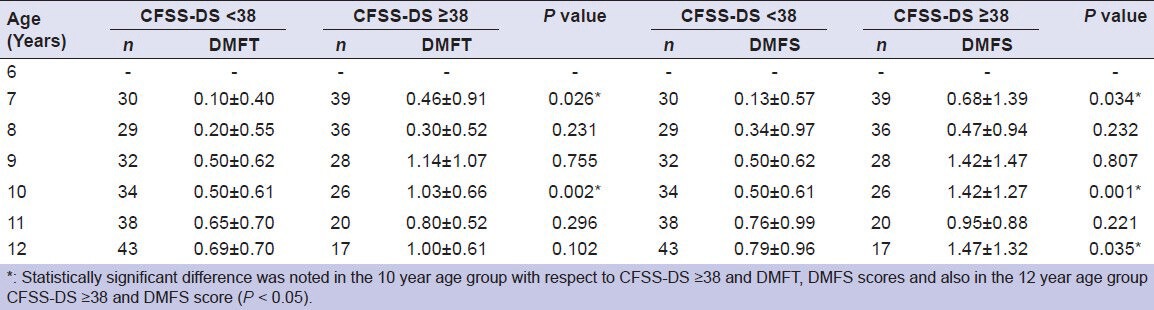
The overall mean score of CFSS-DS in our study was 37.0 ± 8.89, mean score of DMFT and DMFS were 0.58 ± 0.74 and 0.73 ± 1.09, respectively. Mean score of deft and defs were 4.40 ± 2.34 and 7.28 ± 5.49, respectively. There was no statistically significant difference in the mean scores between the males and females for any of the parameters mentioned above (P > 0.05) Table 3. Statistically significant difference in mean defs was noted in the 6 year age group children between those whose CFSS-DS was <38 and those whose CFSS-DS was ≥38 (P < 0.05). Similarly significant difference was noted in 9 year age group children with respect to deft (P < 0.01) and defs scores (P < 0.01) shown in Table 4. Statistically significant difference in mean DMFT, DMFS scores were noted in the 7 year age group children whose CFSS-DS was ≥38 (P < 0.05). Similarly significant difference was noted in the 10 year age group with respect to CFSS-DS ≥38 and DMFT, DMFS scores and also in the 12 year age group CFSS-DS ≥38 and DMFS score (P < 0.05) shown in Table 5.
Table 3.
Comparison of different parameters between males and females
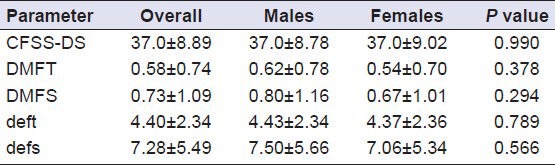
Table 4.
Comparison of mean deft and defs with CFSS-DS <38 and CFSS-DS ≥38 according to their age group
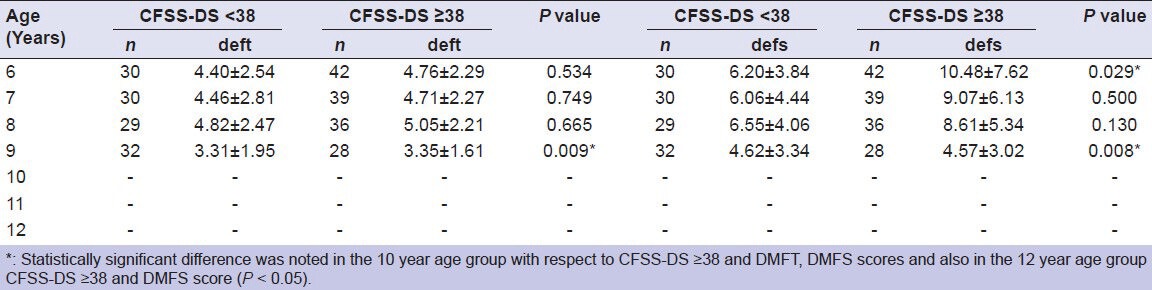
Table 5.
Comparison of mean DMFT and DMFS with CFSS-DS <38 and CFSS-DS ≥38 according to their age group
DISCUSSIONS
Associations between children's dental fear and oral health status have been reported.[4,19,20] Dental fear has been reported to be associated with a range of adverse behavioral and dental health characteristics. Studies of children and adults have shown that dental fear is associated with less favorable self-care behavior, avoidance of dental care, and also with poorer health outcomes.[19] The Dental Subscale of the Children's Fear Survey Schedule (CFSS-DS) is a well-known psychometric scale that was developed in 1982 for assessing dental fear in children. It has been shown to have good reliability-validity, and recently has been used in several countries and translated into several languages.[21,22] Community-based and other large studies conducted in schools or clinics typically rely on questionnaire data to assess the prevalence of dental fear. School-based samples offer the advantages of faster data collection (because the children can be surveyed in groups) and better representation of children of that locale (because even dental avoiders are likely to attend school).[21] CFSS-DS is used to register differences in dental fear between experimental and control groups to select fearful and non-fearful children from a larger reference population and to estimate the prevalence of dental fear in children.[9,22] CFSS-DS has been shown to be better in some situations than other scales such as the Venham Picture Test and the Dental Anxiety Scale.[23]
The mean CFSS-DS score in the present study was 37.0 ± 8.89 which is similar to findings in Singapore (30.6),[2] Canada (for Chinese children, 31.9)[15] and China (35.7)[24] and much higher than findings in Turkey (28.7),[25] USA (28.7)[11] and the mean score was higher than the findings in Finland (22.1),[14] Sweden (23.1),[17] and the Netherlands (23.2).[9]
No statistically significant difference in fear scores between boys and girls in our study. Some prevalence studies have shown that girls score higher on the CFSS-DS,[2,9] while others have found no difference.[15,22,24]
Children in the present study were most afraid of “injections,” “choking,” and “Dentist drilling” which similar to reports from other studies where “choking,” “injections,” and “have somebody put instruments in your mouth” were the most feared items.[2,5,9,20,21] This suggests that apprehension for particular dental items may be constant among various cultures even though the total fear score varied.
Kruger, et al.[19] stated that dental fear is likely to be a significant predictor of dental caries and may be a risk factor for incidence of dental caries. The present study showed no significant correlation between dental fear and DMFS-defs scores similar to studies.[3,26,27] Some studies have found that DMFT-dfs increased significantly with increasing CFSS-DS values[4,14,19,20] A probable explanation is that the caries experience of anxious individuals in some studies is not markedly worse than that of non-anxious counterparts, but the negative dental health attitudes and behavior of the former suggested that their dental health might have deteriorated over the time.[19] Dental anxiety is a serious problem which negatively affects the oral health of children and adults. Early detection of the causes of fear is very important in the solution of the problem. It is recognized that children who witness fear in their parents are likely to acquire that outlook and as a result experience painful experiences at an early age and that this is an important factor related to the problem. To reduce the level of dental fear among children, attention needs to be paid to the use of epidemiologic concepts of clinical risk ascertainment using caries activity tests and early intensive preventive efforts such as fissure sealants, routine oral health examinations, oral hygiene instructions and parental education to prevent the child from experiencing pain, and reduce the need for injections at a very early age.[2] This can go a long way in making the whole first time dental visit a friendly non-threatening experience to gain an anxious patients trust and instill a positive attitude in them about dental treatment.
Children with dental fear pose arduous challenge to the Pediatric dentist in terms of diagnosis, behavior management, and treatment modalities. Every effort should be made to evaluate the child for dental fear prior to dental treatment so that each child can be managed distinctively based on the reasons which induce fear and use necessary behavior modification techniques to be used to make the dental treatment a pleasant and uneventful occasion.
By assessing the Childs fear Pediatric dentist can help the child break the vicious cycle of dental fear and help cultivate a more optimistic attitude toward dental treatment to maintain good oral health.
Further studies should be carried out to correlate the CFSS-DS score to the actual behavioral observations in the dental clinic.
CONCLUSION
The study showed the prevalence of dental fear to be 46.82% among males and 46.88% among females in 6-12 year old children and there was no statistically significant co-relation between the level of dental fear and dental caries in these children. The level of fear was highest for injections, choking, and dentist drilling these factors could influence the child's behavior in the dental clinic and hence it is imperative that as Pediatric dentist we make the child's dental treatment experience a pleasant one and instill a positive outlook towards future dental procedures.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared
REFERENCES
- 1.Milgrom P, Weinstein P. Dental fears in General Practice: New Guidelines for assessment and treatment. Int Dent J. 1993;43:288–93. [PubMed] [Google Scholar]
- 2.Chellappah NK, Vignehsa H, Milgrom P, Lo GL. Prevalence of dental anxiety and fear in children in Singapore. Community Dent Oral Epidemiol. 1990;18:269–71. doi: 10.1111/j.1600-0528.1990.tb00075.x. [DOI] [PubMed] [Google Scholar]
- 3.Taani DQ, El-Qaderi SS, Abu Alhaija ES. Dental anxiety in children and its relationship to dental caries and gingival condition. Int J Dent Hyg. 2005;3:83–7. doi: 10.1111/j.1601-5037.2005.00127.x. [DOI] [PubMed] [Google Scholar]
- 4.Bedi R, Sutcliffe P, Donnan P, Barrett N, McConnachie J. Dental caries experience and prevalence of children afraid of dental treatment. Community Dent Oral Epidemiol. 1992;20:368–71. doi: 10.1111/j.1600-0528.1992.tb00701.x. [DOI] [PubMed] [Google Scholar]
- 5.Yamada MK, Tanabe Y, Sano T, Noda T. Cooperation during dental treatment: The Children's Fear Survey Schedule in Japanese children. Int J Paediatr Dent. 2002;12:404–9. doi: 10.1046/j.1365-263x.2002.00399.x. [DOI] [PubMed] [Google Scholar]
- 6.Holmes RD, Girdler NM. A study to assess the validity of clinical judgement in determining paediatric dental anxiety and related outcomes of management. Int J Pediatr Dent. 2005;15:169–76. doi: 10.1111/j.1365-263X.2005.00633.x. [DOI] [PubMed] [Google Scholar]
- 7.Klaassen MA, Veerkamp JSJ, Aartman IHA, Hoogstraten J. Stressful situations for toddlers: Indications for dental anxiety? J Dent Child. 2002;11:306–9. [PubMed] [Google Scholar]
- 8.Baier K, Milgrom P, Russell S, Mancl L, Yoshida T. Children's fear and behavior in private pediatric dentistry practices. Pediatr Dent. 2004;26:316–21. [PubMed] [Google Scholar]
- 9.Ten Berge M, Veerkamp JS, Hoogstraten J, Prins PJ. Childhood dental fear in the Netherlands: Prevalence and normative data. Community Dent Oral Epidemiol. 2002;30:101–7. doi: 10.1034/j.1600-0528.2002.300203.x. [DOI] [PubMed] [Google Scholar]
- 10.Scherer MW, Nakamura CY. A fear survey schedule for children: A factor analytic comparison with manifest anxiety (CMAS) Behav Res Ther. 1968;6:173–82. doi: 10.1016/0005-7967(68)90004-1. [DOI] [PubMed] [Google Scholar]
- 11.Cuthbert ML, Melamed BG. A screening device: Children at risk for dental fear and management problems. ASDC J Dent Child. 1982;49:432–6. [PubMed] [Google Scholar]
- 12.Klingman A, Melamed BG, Cuthbert ML, Hormecz DA. Effects of participant modeling on information acquisition and skill utilization. J Consult Clin Psychol. 1984;52:414–22. doi: 10.1037//0022-006x.52.3.414. [DOI] [PubMed] [Google Scholar]
- 13.Klingberg G, Berggen U, Noren JG. Dental fear in an urban Sweden child population: Prevalence and concomitant factors. Comm Dent Health. 1994;11:208–14. [PubMed] [Google Scholar]
- 14.Alvesalo I, Murtomaa H, Honkanen A, Karjalainen M, Tay KM. The Dental fear survey schedule: A study of Finnish children. Int Paediatr Dent. 1993;3:193–8. doi: 10.1111/j.1365-263x.1993.tb00083.x. [DOI] [PubMed] [Google Scholar]
- 15.Milgrom P, Jie Z, Yang Z, Tay KM. Cross cultural validity of a parent's version of the Dental fear survey schedule for children in Chinese. Behav Res Ther. 1994;32:131–5. doi: 10.1016/0005-7967(94)90094-9. [DOI] [PubMed] [Google Scholar]
- 16.Milgrom P, Mancl L, King B, Weinstein P. Origins of childhood dental fear. Behav Res Ther. 1995;33:313–9. doi: 10.1016/0005-7967(94)00042-i. [DOI] [PubMed] [Google Scholar]
- 17.Klingberg G, Berggren U, Noren JG. Dental fear in an urban Swedish population; prevalence and concomitant factors. Community Dent Health. 1994;11:208–14. [PubMed] [Google Scholar]
- 18.4th ed. Geneva: WHO; 1997. World Health Organisation. Oral Health Surveys, Basic Methods. [Google Scholar]
- 19.Kruger E, Thomson WM, Poulton R, Davies S, Brown RH, Silva PA. Dental caries and changes in dental anxiety in late adolescence. Community Dent Oral Epidemiol. 1998;26:355–9. doi: 10.1111/j.1600-0528.1998.tb01973.x. [DOI] [PubMed] [Google Scholar]
- 20.Rantavuori K, Lahti S, Hausen H, Seppa L, Karkkainen S. Dental fear and oral health and family characteristics of Finnish children. Acta Odontol Scand. 2004;62:207–13. doi: 10.1080/00016350410001586. [DOI] [PubMed] [Google Scholar]
- 21.Nakai Y, Hirakawa T, Milgrom P, Coolidge T, Heima M, Mori Y, et al. The Children's Fear Survey Schedule-Dental Subscale in Japan. Community Dent Oral Epidemiol. 2005;33:196–204. doi: 10.1111/j.1600-0528.2005.00211.x. [DOI] [PubMed] [Google Scholar]
- 22.Ten Berge M, Hoogstraten J, Veerkamp JS, Prins PJ. The Dental Subscale of the Children's Fear Survey Schedule: A factor analytic study in The Netherlands. Community Dent Oral Epidemiol. 1998;26:340–3. doi: 10.1111/j.1600-0528.1998.tb01970.x. [DOI] [PubMed] [Google Scholar]
- 23.Aartman IHA, van Everdingen T, Hoogstraten J, Schuurs AH. Self-report measurements of dental anxiety and fear in children: A critical assessment. J Dent Child. 1998;22:252–8. [PubMed] [Google Scholar]
- 24.Wogelius P, Poulsen S, Sorensen HT. Prevalence of dental anxiety and behavior management Problems among six to eight years old Danish children. Acta Odontol Scand. 2003;61:178–83. doi: 10.1080/00016350310003468. [DOI] [PubMed] [Google Scholar]
- 25.Akbay Oba A, Dülgergil CT, Sönmez IS. Prevalence of dental Anxiety in 7 to 11 year old Children and its relationship to Dental caries. Med Princ Pract. 2009;18:453–7. doi: 10.1159/000235894. [DOI] [PubMed] [Google Scholar]
- 26.Vignehsa H, Chellappah NK, Milgrom P, Going R, Teo CS. A clinical evaluation of high- and low-fear children in Singapore. ASDC J Dent Child. 1990;57:224–8. [PubMed] [Google Scholar]
- 27.Wright FA, Lucas JO, McMurray NE. Dental anxiety in five-to-nine-year-old children. J Pedod. 1980;4:99–115. [PubMed] [Google Scholar]