

Abstract
Histamine2-receptor antagonists (H2RAs) are available over-the-counter (OTC) for the treatment and prevention of heartburn, but more than occasional, single-dose use can lead to rapid development of tachyphylaxis. The aim of this review is to assess the published evidence regarding the development of tachyphylaxis with repeat usage of H2RAs. PubMed and SCOPUS were searched across all years to identify clinical studies that examined the development of tachyphylaxis with repeated dosing of H2RAs. Although a single (first) dose of an H2RA can be effective for controlling gastric acid and preventing or relieving food-related heartburn, numerous studies confirm that tachyphylaxis, also known as tolerance, is consistently detected at the first time point assessed after the first dose, including the second day and/or second dose. Even if symptom relief is achieved with an H2RA, it may be due to desensitization of the esophagus to acid exposure, potentially providing symptom relief without significantly decreasing esophageal acid exposure. When recommending OTC drugs for treatment of frequent heartburn, clinicians should be aware of the potential for rapid development of tachyphylaxis in patients who use H2RAs for 2 or more consecutive days. Even if symptom relief is achieved, it may be due to desensitization of the esophagus to acid by the H2RA, potentially providing symptom relief without significantly decreasing esophageal acid exposure. Other strategies, such as an OTC proton pump inhibitor, may be needed to optimize management of frequent heartburn.
Keywords: Histamine2-receptor antagonist, Tachyphylaxis, Tolerance, Gastric pH
Core tip: Histamine2-receptor antagonists (H2RAs) are available over-the-counter (OTC) for the treatment and prevention of heartburn, but recommendations for use should be limited to those with infrequent heartburn. A single dose of an H2RA can be effective for controlling gastric acid and preventing or relieving heartburn, but tolerance (tachyphylaxis) develops rapidly, and is evident by the second day/second dose. Even if symptom relief is achieved, it may be due to desensitization of the esophagus to acid by the H2RA, potentially providing symptom relief without significantly decreasing esophageal acid exposure. For frequent heartburn (≥ 2 d/wk), an OTC proton pump inhibitor should be considered.
INTRODUCTION
Heartburn is a common complaint[1-4]. In a recent review of 29 published studies, the range of prevalence for experiencing heartburn at least once per week was estimated at 18%-28% in North America, 9%-26% in Europe, 3%-8% in East Asia, 9%-33% in the Middle East, 12% in Australia and 23% in South America[5]. More than 50 million Americans experience frequent heartburn, defined as occurring at least 2 d a week[2]. The majority of adults with frequent heartburn have consulted a healthcare provider[6], but they primarily rely on over-the-counter (OTC) heartburn remedies to manage their symptoms. Therefore, it is important that healthcare providers understand the benefits and limitations of different heartburn remedies.
The mainstay of pharmacologic therapy for frequent heartburn is acid suppressive therapy[7]. All OTC heartburn therapies may provide a benefit when taken as directed, but there are important differences among the available therapies. Antacids act to rapidly but transiently neutralize acid that has refluxed into the esophagus[8]. Histamine2-receptor antagonists (H2RAs) slow gastric acid production by competitively and reversibly binding to one of the pathways for stimulation of acid production, the H2 receptors on parietal cells[9,10]. H2RAs act relatively quickly, with gastric pH rising within 30 min of a single dose, and have a longer duration of action (up to 10 h) than antacids[9-11]. Proton pump inhibitors (PPIs) suppress acid production by binding to and inhibiting the H+/K+ ATPase enzyme system (“proton pump”, the final step in acid production) at the secretory surface of the gastric parietal cell[11,12]. PPIs inhibit gastric acid secretion by all known stimuli and are more potent anti-secretory agents than H2RAs[11-14]. Proton pump inhibitors have a slower onset of action (1-2 h), but exhibit comparable 24-h acid control to H2RAs on dosing day 1, and reach peak effect after several days, providing sustained acid suppression throughout the 14 d course of therapy (Figure 1)[14-16].
Figure 1.
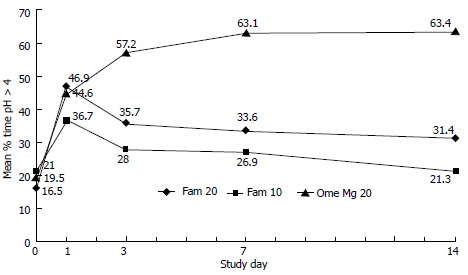
Famotidine vs omeprazole for 14-d gastric acid control. Mean percentage of time gastric pH > 4 across 14 d of dosing in subjects with frequent heartburn[14] Famotidine (Fam) 10 mg or 20 mg was dosed twice a day. Omeprazole (Ome Mg 20) was dosed once a day (omeprazole-magnesium 20.6 mg). Gastric pH was assessed for 24-h on day 0 (baseline) and dosing days 1, 3, 7 and 14. Both famotidine doses showed a rapid decline in gastric acid control by dosing day 3, followed by a more gradual decline across 14-d of dosing. Omeprazole showed similar gastric acid control to famotidine 20 mg on dosing day 1, with an increase in gastric acid control over the first several days, followed by a sustained effect across 14-d of dosing (reprinted with permission[14]).
Owing to their pharmacodynamic profiles, both antacids and OTC H2RAs are indicated for on-demand therapy when relief of an existing episode of heartburn is desired[8-10,17]. An OTC H2RA can also be useful for preventing symptoms that are associated with eating food or drinking beverages that cause heartburn[9,10]. Both antacids and H2RAs are indicated for a maximum of 14 d of therapy, after which consumers with persisting symptoms should seek advice from a physician[9,10,17]. In contrast, the OTC PPIs are indicated to treat frequent heartburn (occurring 2 or more days weekly), and are indicated for once daily use every day for 14 d, with a repeat 14-d course every 4 mo[12,13]. As with antacid and OTC H2RAs, consumers with symptoms persisting beyond 14 d are encouraged to consult a physician. Any patient presenting with “alarm” symptoms (e.g., dysphagia, odynophagia, bleeding, weight loss, anemia)[6] may have a more serious condition and should be referred to a physician for further evaluation. With the availability of OTC acid-suppressive therapies, it is important for health professionals to appreciate the strengths and weaknesses of these agents in order to help guide effective consumer-directed management of heartburn.
RESEARCH
We conducted a comprehensive search of PubMed and SCOPUS scientific databases across all years to identify clinical studies that examined the development of tachyphylaxis with repeated dosing of H2RAs. The terms “histamine receptor antagonist”, “H2RA”, “tachyphylaxis”, “tolerance”, “intragastric pH”, “gastric acid” and “heartburn” were used to identify clinical studies. Additionally, the reference section of each identified publication was explored for publications not identified in the PubMed and SCOPUS searches. Published clinical studies that assessed intragastric pH and/or gastric acid production following multiple days of dosing of an H2RA were included, and data regarding H2RA dose, timing of dosing, sample size, gastric acid production and/or intragastric pH were extracted and examined.
RESULTS
Fifteen publications, reporting a total of 18 clinical studies, were identified for this review, and the details of these studies are summarized in Table 1. With repeated doses of an H2RA, tachyphylaxis was consistently observed by the first time period tested after the initial dose, including the second day/second dose[14-16,18-32]. This effect was reported over a wide range of doses of H2RAs, including both prescription and OTC doses, and occurred regardless of route of administration (oral and IV). This phenomenon has been observed under both fasting and fed conditions, and in various populations, including healthy subjects, patients with gastro-esophageal reflux disease, and post-surgical patients. While the mechanism for H2RA tachyphylaxis remains speculative, it may involve the up-regulation of parietal cell receptors for other mediators of acid secretion (i.e., acetylcholine, gastrin), the sensitization of H2 receptors, the impairment of inhibitory neurohormonal control of acid secretion, and/or an alteration in receptor turnover after chronic competitive inhibition[19-21].
Table 1.
Intragastric pH studies demonstrating histamine2-receptor antagonists1 tachyphylaxis
| Ref. | Design | Treatment regimen | Dosing duration | n | Days pH recorded | Tachyphylaxis observed |
| Wilder-Smith et al[38], 1990 | OL | Famotidine 40 mg QD | 28 d | 14 | 1, 14, 28 | Day 14 |
| R, PC, DB, crossover | Ranitidine 300 mg QID | 7 d | 10 | 1, 7, 28 | Day 7 | |
| Ranitidine 300 mg QHS | 21 d | |||||
| R, PC, DB, crossover | Ranitidine 300 mg TID | 14 d | 14 | 1, 14 | Day 14 | |
| Ranitidine 300 mg QHS | Day 14 | |||||
| Smith et al[39], 1990 | R, PC, crossover | Famotidine 40 mg QD | 28 d | 13 | 0, 1, 14, 28 | Day 14 |
| R, PC, crossover | Ranitidine 300 mg QID | 7 d | 13 | 1, 8 | Day 8 | |
| Ranitidine 300 mg QHS | 21 d | Day 8 | ||||
| Nwokolo et al[24], 1990 | R, OL | Cimetidine 800 mg QD | 29 d | 48 | 0, 1, 15, 29 | Day 15 |
| Nizatidine 300 mg QD | Day 15 | |||||
| Famotidine 40 mg QD | Day 15 | |||||
| Ranitidine 150 mg BID | Day 15 | |||||
| Ranitidine 150 mg QD | Day 15 | |||||
| Ranitidine 300 mg QD | ||||||
| Nwokolo et al[40], 1991 | R, DB, PC | Ranitidine 150 mg QHS | 5 mo | 17 | 1, 29, 57, 85, 113, 141 | Day 29 |
| Ranitidine 150 mg prn | Day 29 | |||||
| Wilder-Smith et al[23], 1992 | R, PC, blinded, crossover | Ranitidine IV 0.25 mg/kg per hour | 6 d | 10 | 1, 6 | Day 6 |
| Ranitidine IV by pH-feedback, up to 800 mg/24 h | Day 6 | |||||
| Ranitidine 300 mg PO QID | Day 6 | |||||
| Merki et al[31], 1993 | R, PC, crossover | Ranitidine IV ≤ 600 mg/24 h, pre/post 300 mg QD for 9 d | 9 d | 11 | 1, 9 | Day 9 |
| Merki et al[30], 1994 | R, DB, crossover | Ranitidine IV, ≤ 576 mg/24 h | 3 d | 12 | 1, 3 | Day 3 |
| Omeprazole IV, ≤ 288 mg/24 h | Not observed | |||||
| Hurlimann et al[22], 1994 | R, DB, parallel | Ranitidine 150 mg QID | 14 d | 28 | 1, 2, 7, 14 | Day 2 |
| Omeprazole 40 mg QD | Not observed | |||||
| Lachman et al[41], 2000 | OL | Ranitidine 150 mg QID | 5 d | 28 | 1, 5 | Day 5 |
| Komazawa et al[20], 2003 | R, crossover | Ranitidine 150 mg BID | 14 d | 7 | 1, 14 | Day 14 |
| Famotidine 150 mg BID | Day 14 | |||||
| Hsu et al[18], 2004 | R, OL | Cimetidine IV 1200 mg/24 h | 5 d | 80 | 1, 2, 3, 4, 5 | Day 2 |
| Ranitidine IV 200 mg/24 h | Day 2 | |||||
| Omeprazole IV 40 mg BID | Not observed | |||||
| Miner et al[14], 2006 | R, PC, crossover | Famotidine 10 mg BID | 14 d | 31 | 1, 3, 7, 14 | Day 3 |
| Famotidine 20 mg QD | Day 3 | |||||
| Omeprazole 20 mg QD | Not observed | |||||
| Shimatani et al[25], 2007 | R, OL, crossover | Famotidine 20 mg BID | 15 d | 8 | 1, 8, 15 1, 8, 15 | Day 8 |
| Omeprazole 10 mg QD | Not observed | |||||
| Fändriks et al[16], 2007 | R, crossover | Famotidine 10 mg | 8 d | 8 | 1, 8 | Day 8 |
| Omeprazole 20 mg | Not observed | |||||
| Ono et al[15], 2008 | R, crossover | Ranitidine 150 mg BID | 10 d | 7 | -1, 1-7, 11-12 (no dose 8-10) | Day 2 |
| Rabeprazole 20 mg QD | Not observed |
1Includes only histamine2-receptor antagonists marketed in the United States. All doses were administered orally unless specified otherwise. BID: Twice daily; HS: Bedtime; IV: Ntravenous; OL: Open-label; PC: Placebo-controlled; PRN: As needed; QD: Daily; QID: Four times daily; QHS: Every bedtime; R: Randomized.
In a study assessing the gastric acid control of OTC doses of an H2RA, 31 healthy adults with frequent heartburn (occurring ≥ 2 d/wk) underwent 24-h gastric pH monitoring over a 14-d period while taking famotidine 10 mg twice daily, famotidine 20 mg twice daily, or omeprazole 20 mg once daily, in a double-blind, 3-period crossover fashion[14]. As depicted in Figure 1, the mean percentage of time gastric pH > 4 was at its highest level on dosing day 1 for both doses of famotidine, then decreased on subsequent days of continued dosing, consistent with H2RA tachyphylaxis reported previously with prescription doses[20,22-24]. A similar loss of H2RA antisecretory effect has been reported in other studies examining OTC doses of famotidine (versus omeprazole; Table 1)[16,25]. In contrast to H2RAs, PPIs do not exhibit tachyphylaxis, but rather show similar efficacy to H2RAs on dosing day 1, then increase in effectiveness over several days before reaching a sustained plateau effect for the duration of dosing (Figure 1)[14-16,18,22,25-29].
Tachyphylaxis to H2RAs does not appear to be progressive, as studies have typically demonstrated no further reduction in antisecretory effect after the initial loss of potency is detected[21-23]. In one of the longest studies assessing H2RA tolerance, Nwokolo et al[24] demonstrated no further reduction in acid inhibitory efficacy from 1 to 5 mo of dosing in 17 healthy patients taking ranitidine 150 mg nightly. However, once tachyphylaxis to an H2RA has developed, increasing the dose does not appear to be effective in overcoming the loss of anti-secretory effect[29,30]. Merki et al[31] found that the tolerance observed with ranitidine infusion could not be overcome by individual pH-regulated titrated doses of ranitidine of more than 500 mg/24 h, even after three days of treatment.
The physiologic effect of tachyphylaxis has been found to persist for 3 d after H2RA dosing is discontinued. In one study, ranitidine was dosed twice daily for 7 d, dosing was stopped for 3 d, and then dosing was resumed for 3 d[15]. Tachyphylaxis was evident by day 2 of dosing in the first period, and the physiological effects of tachyphylaxis were still evident (decreased response to the H2RA) when dosing was re-initiated after the 3-d hiatus[15]. This study showed that it took longer than 3 d to recover the beneficial effects of an H2RA once tachyphylaxis had occurred, supporting that only occasional, isolated doses of an H2RA provide the maximum benefit of the drug.
CLINICAL IMPLICATIONS OF H2RA TACHYPHYLAXIS
Although prospective data evaluating the clinical relevance of H2RA tachyphylaxis for patients with frequent heartburn are limited, decreasing gastric acid production is the accepted mechanism of action for H2RAs, studies have demonstrated a link between gastric acid suppression and heartburn relief[32,33], and the percentage of time that the gastric pH is > 4.0 over a 24-h period is frequently used as a surrogate marker for the clinical efficacy of acid suppressive therapies[14,34,35]. If tachyphylaxis is a class effect for H2RAs that significantly decreases acid control starting the second day/second dose, why do some frequent heartburn sufferers appear to achieve symptom control with daily dosing? A 2004 study sought to determine if daily doses of ranitidine decreased esophageal sensitivity to chemical and/or mechanical stimulation[36]. Eighteen patients who experienced functional heartburn (normal esophageal pH) received oral ranitidine 150 mg bid or placebo for 7 consecutive days (double-blind, randomized, crossover study) and underwent mechanical (Barostat balloon distention) and chemical (Bernstein acid infusion) stimulation on study day 1 (90 min post-dose) and study day 7. After a single dose of ranitidine 150 mg, time to pain with esophageal acid infusion was increased by 29% (P < 0.05) and heartburn pain was decreased by 20% (VAS score, P < 0.06) and 23% (Likert score, P < 0.02) compared with placebo. After 1 wk of ranitidine dosing, subjects still exhibited decreased sensitivity to esophageal acid exposure. In contrast, mechanical (balloon distention) sensory parameters were not altered by ranitidine[36]. These data show that an H2RA can significantly decrease esophageal sensitivity to acid exposure, potentially providing symptom relief without significantly decreasing esophageal acid exposure.
Taken together, these data support that patients with frequent heartburn may be better managed by daily use of an OTC PPI, rather than repeated doses of H2RAs. Two well-controlled clinical studies showed that an OTC dose of omeprazole was superior to OTC doses of ranitidine for the management of frequent heartburn[28,37]. In a randomized controlled trial in 144 patients with endoscopically verified erosive esophagitis, Sandmark et al[37] found that symptoms had resolved in 51% of patients treated with omeprazole 20 mg daily by the end of the first week of treatment compared with 27% of patients treated with ranitidine 150 mg twice daily (P = 0.009). Similar results were found in a larger controlled study in 677 patients with heartburn and either no or mild erosive esophagitis[28]. Patients were randomized to one of three treatment regimens, and omeprazole was found to be superior to ranitidine, with 55%, 40%, and 26% of patients symptom-free who were treated with omeprazole 20 mg, omeprazole 10 mg, or ranitidine 150 mg, respectively (P < 0.001)[28].
CONCLUSION
While a single dose of an H2RA can be effective for controlling gastric acid and preventing or relieving isolated heartburn episodes, repeat dosing for more frequent heartburn may lead to the rapid development and sustained effects of tachyphylaxis. Even if symptom relief is achieved with multiple doses of an H2RA, it may be due to desensitization of the esophagus to acid, potentially providing symptom relief without significantly decreasing esophageal acid exposure. Other OTC strategies, such as a PPI, may be needed to optimize management of frequent heartburn.
Footnotes
P- Reviewers: Fishman P, Karatapanis S S- Editor: Ma YJ L- Editor: A E- Editor: Wu HL
References
- 1.Eisen G. The epidemiology of gastroesophageal reflux disease: what we know and what we need to know. Am J Gastroenterol. 2001;96:S16–S18. doi: 10.1016/s0002-9270(01)02580-1. [DOI] [PubMed] [Google Scholar]
- 2.Shaker R, Castell DO, Schoenfeld PS, Spechler SJ. Nighttime heartburn is an under-appreciated clinical problem that impacts sleep and daytime function: the results of a Gallup survey conducted on behalf of the American Gastroenterological Association. Am J Gastroenterol. 2003;98:1487–1493. doi: 10.1111/j.1572-0241.2003.07531.x. [DOI] [PubMed] [Google Scholar]
- 3.Moayyedi P, Axon AT. Review article: gastro-oesophageal reflux disease--the extent of the problem. Aliment Pharmacol Ther. 2005;22 Suppl 1:11–19. doi: 10.1111/j.1365-2036.2005.02605.x. [DOI] [PubMed] [Google Scholar]
- 4.El-Serag HB. Time trends of gastroesophageal reflux disease: a systematic review. Clin Gastroenterol Hepatol. 2007;5:17–26. doi: 10.1016/j.cgh.2006.09.016. [DOI] [PubMed] [Google Scholar]
- 5.El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2013:Jul 13; Epub ahead of print. doi: 10.1136/gutjnl-2012-304269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Oliveria SA, Christos PJ, Talley NJ, Dannenberg AJ. Heartburn risk factors, knowledge, and prevention strategies: a population-based survey of individuals with heartburn. Arch Intern Med. 1999;159:1592–1598. doi: 10.1001/archinte.159.14.1592. [DOI] [PubMed] [Google Scholar]
- 7.DeVault KR, Castell DO. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastroenterol. 2005;100:190–200. doi: 10.1111/j.1572-0241.2005.41217.x. [DOI] [PubMed] [Google Scholar]
- 8.Collings KL, Rodriguez-Stanley S, Proskin HM, Robinson M, Miner PB. Clinical effectiveness of a new antacid chewing gum on heartburn and oesophageal pH control. Aliment Pharmacol Ther. 2002;16:2029–2035. doi: 10.1046/j.1365-2036.2002.01380.x. [DOI] [PubMed] [Google Scholar]
- 9. Available from: http: //www.zantacotc.com/products/zantac75.jsp.
- 10.Tagamet HB. OTC Medication Information. Available from: http: //otclabels.com/lib/otc/otc-meds/tagamet-hb/
- 11.Schubert ML, Peura DA. Control of gastric acid secretion in health and disease. Gastroenterology. 2008;134:1842–1860. doi: 10.1053/j.gastro.2008.05.021. [DOI] [PubMed] [Google Scholar]
- 12. Available from: http: //www.prilosecotc.com/AboutPrilosecOTC.
- 13. Available from: http: //www.prevacid24hr.com/now-available.jsp.
- 14.Miner PB, Allgood LD, Grender JM. Comparison of gastric pH with omeprazole magnesium 20.6 mg (Prilosec OTC) o.m. famotidine 10 mg (Pepcid AC) b.d. and famotidine 20 mg b.d. over 14 days of treatment. Aliment Pharmacol Ther. 2007;25:103–109. doi: 10.1111/j.1365-2036.2006.03129.x. [DOI] [PubMed] [Google Scholar]
- 15.Ono S, Kato M, Ono Y, Imai A, Yoshida T, Shimizu Y, Asaka M. Immediate acid-suppressing effects of ranitidine hydrochloride and rabeprazole sodium following initial administration and reintroduction: A randomized, cross-over study using wireless pH monitoring capsules. J Gastroenterol Hepatol. 2009;24:639–645. doi: 10.1111/j.1440-1746.2008.05644.x. [DOI] [PubMed] [Google Scholar]
- 16.Fändriks L, Lönroth H, Pettersson A, Vakil N. Can famotidine and omeprazole be combined on a once-daily basis? Scand J Gastroenterol. 2007;42:689–694. doi: 10.1080/00365520601026665. [DOI] [PubMed] [Google Scholar]
- 17.Mylanta® Regular Strength. The trusted antacid, anti-gas formula of Regular Strength MYLANTA® delivers fast, safe heartburn relief when used as directed. Available from: http: //www.mylanta.com/mylanta-regular-strength.
- 18.Hsu TC, Su CF, Leu SC, Huang PC, Wang TE, Chu CH. Omeprazole is more effective than a histamine H2-receptor blocker for maintaining a persistent elevation of gastric pH after colon resection for cancer. Am J Surg. 2004;187:20–23. doi: 10.1016/j.amjsurg.2002.10.002. [DOI] [PubMed] [Google Scholar]
- 19.Fackler WK, Ours TM, Vaezi MF, Richter JE. Long-term effect of H2RA therapy on nocturnal gastric acid breakthrough. Gastroenterology. 2002;122:625–632. doi: 10.1053/gast.2002.31876. [DOI] [PubMed] [Google Scholar]
- 20.Komazawa Y, Adachi K, Mihara T, Ono M, Kawamura A, Fujishiro H, Kinoshita Y. Tolerance to famotidine and ranitidine treatment after 14 days of administration in healthy subjects without Helicobacter pylori infection. J Gastroenterol Hepatol. 2003;18:678–682. doi: 10.1046/j.1440-1746.2003.03041.x. [DOI] [PubMed] [Google Scholar]
- 21.Gillen D, McColl KE. Problems related to acid rebound and tachyphylaxis. Best Pract Res Clin Gastroenterol. 2001;15:487–495. doi: 10.1053/bega.2001.0190. [DOI] [PubMed] [Google Scholar]
- 22.Hurlimann S, Abbühl B, Inauen W, Halter F. Comparison of acid inhibition by either oral high-dose ranitidine or omeprazole. Aliment Pharmacol Ther. 1994;8:193–201. doi: 10.1111/j.1365-2036.1994.tb00278.x. [DOI] [PubMed] [Google Scholar]
- 23.Wilder-Smith CH, Merki HS. Tolerance during dosing with H2-receptor antagonists. An overview. Scand J Gastroenterol Suppl. 1992;193:14–19. doi: 10.3109/00365529209096000. [DOI] [PubMed] [Google Scholar]
- 24.Nwokolo CU, Smith JT, Gavey C, Sawyerr A, Pounder RE. Tolerance during 29 days of conventional dosing with cimetidine, nizatidine, famotidine or ranitidine. Aliment Pharmacol Ther. 1990;4 Suppl 1:29–45. [PubMed] [Google Scholar]
- 25.Shimatani T, Inoue M, Kuroiwa T, Moriwaki M, Xu J, Ikawa K, Morikawa N, Tazuma S. Which has superior acid-suppressive effect, 10 mg omeprazole once daily or 20 mg famotidine twice daily? Effects of single or repeated administration in Japanese Helicobacter pylori-negative CYP2C19 extensive metabolizers. Dig Dis Sci. 2007;52:390–395. doi: 10.1007/s10620-006-9490-9. [DOI] [PubMed] [Google Scholar]
- 26.Lanzon-Miller S, Pounder RE, Hamilton MR, Ball S, Chronos NA, Raymond F, Olausson M, Cederberg C. Twenty-four-hour intragastric acidity and plasma gastrin concentration before and during treatment with either ranitidine or omeprazole. Aliment Pharmacol Ther. 1987;1:239–251. doi: 10.1111/j.1365-2036.1987.tb00623.x. [DOI] [PubMed] [Google Scholar]
- 27.Allgood LD, Grender JM, Shaw MJ, Peura DA. Comparison of Prilosec OTC (omeprazole magnesium 20.6 mg) to placebo for 14 days in the treatment of frequent heartburn. J Clin Pharm Ther. 2005;30:105–112. doi: 10.1111/j.1365-2710.2004.00620.x. [DOI] [PubMed] [Google Scholar]
- 28.Bardhan KD, Müller-Lissner S, Bigard MA, Bianchi Porro G, Ponce J, Hosie J, Scott M, Weir DG, Gillon KR, Peacock RA, et al. Symptomatic gastro-oesophageal reflux disease: double blind controlled study of intermittent treatment with omeprazole or ranitidine. The European Study Group. BMJ. 1999;318:502–507. doi: 10.1136/bmj.318.7182.502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Huang JQ, Hunt RH. Pharmacological and pharmacodynamic essentials of H(2)-receptor antagonists and proton pump inhibitors for the practising physician. Best Pract Res Clin Gastroenterol. 2001;15:355–370. doi: 10.1053/bega.2001.0184. [DOI] [PubMed] [Google Scholar]
- 30.Merki HS, Wilder-Smith CH. Do continuous infusions of omeprazole and ranitidine retain their effect with prolonged dosing? Gastroenterology. 1994;106:60–64. doi: 10.1016/s0016-5085(94)94341-9. [DOI] [PubMed] [Google Scholar]
- 31.Merki HS, Halter F, Wilder-Smith CH. Diurnal secretory patterns and tolerance during individually titrated infusions of ranitidine. Gastroenterology. 1993;105:748–754. doi: 10.1016/0016-5085(93)90892-g. [DOI] [PubMed] [Google Scholar]
- 32.Furuta K, Adachi K, Komazawa Y, Mihara T, Miki M, Azumi T, Fujisawa T, Katsube T, Kinoshita Y. Tolerance to H2 receptor antagonist correlates well with the decline in efficacy against gastroesophageal reflux in patients with gastroesophageal reflux disease. J Gastroenterol Hepatol. 2006;21:1581–1585. doi: 10.1111/j.1440-1746.2006.04323.x. [DOI] [PubMed] [Google Scholar]
- 33.Katz PO, Ginsberg GG, Hoyle PE, Sostek MB, Monyak JT, Silberg DG. Relationship between intragastric acid control and healing status in the treatment of moderate to severe erosive oesophagitis. Aliment Pharmacol Ther. 2007;25:617–628. doi: 10.1111/j.1365-2036.2006.03235.x. [DOI] [PubMed] [Google Scholar]
- 34.Hunt RH. Importance of pH control in the management of GERD. Arch Intern Med. 1999;159:649–657. doi: 10.1001/archinte.159.7.649. [DOI] [PubMed] [Google Scholar]
- 35.Armstrong D. Review article: gastric pH -- the most relevant predictor of benefit in reflux disease? Aliment Pharmacol Ther. 2004;20 Suppl 5:19–26; discussion 38-39. doi: 10.1111/j.1365-2036.2004.02140.x. [DOI] [PubMed] [Google Scholar]
- 36.Rodriguez-Stanley S, Ciociola AA, Zubaidi S, Proskin HM, Miner PB. A single dose of ranitidine 150 mg modulates oesophageal acid sensitivity in patients with functional heartburn. Aliment Pharmacol Ther. 2004;20:975–982. doi: 10.1111/j.1365-2036.2004.02217.x. [DOI] [PubMed] [Google Scholar]
- 37.Sandmark S, Carlsson R, Fausa O, Lundell L. Omeprazole or ranitidine in the treatment of reflux esophagitis. Results of a double-blind, randomized, Scandinavian multicenter study. Scand J Gastroenterol. 1988;23:625–632. doi: 10.3109/00365528809093923. [DOI] [PubMed] [Google Scholar]
- 38.Wilder-Smith CH, Ernst T, Gennoni M, Zeyen B, Halter F, Merki HS. Tolerance to oral H2-receptor antagonists. Dig Dis Sci. 1990;35:976–983. doi: 10.1007/BF01537246. [DOI] [PubMed] [Google Scholar]
- 39.Smith JT, Gavey C, Nwokolo CU, Pounder RE. Tolerance during 8 days of high-dose H2-blockade: placebo-controlled studies of 24-hour acidity and gastrin. Aliment Pharmacol Ther. 1990;4 Suppl 1:47–63. [PubMed] [Google Scholar]
- 40.Nwokolo CU, Prewett EJ, Sawyerr AM, Hudson M, Lim S, Pounder RE. Tolerance during 5 months of dosing with ranitidine, 150 mg nightly: a placebo-controlled, double-blind study. Gastroenterology. 1991;101:948–953. doi: 10.1016/0016-5085(91)90720-6. [DOI] [PubMed] [Google Scholar]
- 41.Lachman L, Howden CW. Twenty-four-hour intragastric pH: tolerance within 5 days of continuous ranitidine administration. Am J Gastroenterol. 2000;95:57–61. doi: 10.1111/j.1572-0241.2000.01701.x. [DOI] [PubMed] [Google Scholar]