

Abstract
During the last decade, there has been a rapidly growing trend toward the use of cellphone-based devices (CBDs) in bioanalytical sciences. For example, they have been used for digital microscopy, cytometry, read-out of immunoassays and lateral flow tests, electrochemical and surface plasmon resonance based bio-sensing, colorimetric detection and healthcare monitoring, among others. Cellphone can be considered as one of the most prospective devices for the development of next-generation point-of-care (POC) diagnostics platforms, enabling mobile healthcare delivery and personalized medicine. With more than 6.5 billion cellphone subscribers worldwide and approximately 1.6 billion new devices being sold each year, cellphone technology is also creating new business and research opportunities. Many cellphone-based devices, such as those targeted for diabetic management, weight management, monitoring of blood pressure and pulse rate, have already become commercially-available in recent years. In addition to such monitoring platforms, several other CBDs are also being introduced, targeting e.g., microscopic imaging and sensing applications for medical diagnostics using novel computational algorithms and components already embedded on cellphones. This manuscript aims to review these recent developments in CBDs for bioanalytical sciences along with some of the challenges involved and the future opportunities.
Keywords: cellphone, bioanalytical sciences, diagnostics, point-of-care, digital health
Introduction
The use of cellphones in bioanalytical sciences has opened new opportunities and intensified research efforts for the development of next generation cellphone-based devices (CBDs) that will enable users to have access to cost-effective and compact bioanalytical technologies at any time and place. Such mobile Healthcare (mHealthcare) technologies based on CBDs will further improve the self-management of chronic patients, and will enable the supervision of physically-disabled, mentally ill or elderly individuals with minimum interference in their daily lives. Equipped with various advanced features, such as real-time geo-tagging, secure data management and analysis, high storage capacity, powerful processors, wireless connectivity through General Packet Radio Service and Wi-Fi, etc. the current generation of cellphones provides a promising digital platform for the development of various bioanalytical devices. A variety of sensors, such as Global Positioning System modules, light detectors, microphones, cameras, accelerometers as well as proximity sensors, are already integrated into the cellphones. Therefore, CBDs might especially be useful for bioanalytical applications in remote and resource-poor settings, generating real-time results, which can be remotely accessed by e.g., the analysts and certified professionals, thereby enabling the monitoring of emerging situations.
In addition to significant improvements in the state of the art for the cellphone technology, during the last decade, there has been also an enormous growth in the number of cellphone subscribers. According to “Measuring the Information Society” report by The International Telecommunication Union (2012) [1], there were 6 billion cellphone subscribers worldwide by the end of 2011 that accounts for 86% of the world population. The Mobile Factbook 2012 [2] predicts the cellphone subscribers to reach 6.9 and 8.0 billion by the end of 2013 and 2016, respectively. Furthermore, there has been a rapid increase in the number of cellphone users in developing countries as the telecommunication and internet services have become more affordable, as evident from 142 million cellphone subscriptions in 2011 in India only [2]. As another example, about 1.6 billion cellphones were sold in 2011 only and the smartphones account for ~32 % of the market, which is expected to increase to > 55% by 2016 [2].
This enormous growth in cellphone subscribers worldwide along with the rapidly evolving technological features of cellphones have vastly expanded the market size and effectively contributed to the emergence of new businesses. These advancements have sparked remarkable interest among researchers as well as investors to develop prospective technologies for bioanalytical sciences. Moreover, CBDs might have a significant global impact on healthcare as they can lead to transformative landscape changes by enabling real-time on-site analysis and telemedicine opportunities in remote areas. Here we present a timely review of these recent developments in CBDs for bioanalytical sciences (see e.g., Table 1), and highlight some of the challenges involved and the future opportunities that lie ahead of us.
Table 1.
Cellphone-based devices (CBD) for bioanalytical sciences.
| Bioanalytical application | Type of CBD | Developed By | Characteristics | Reference |
|---|---|---|---|---|
| Immunoassays | • Cellphone-based CRP detection | Dublin City University, Ireland | LOD of the developed hsCRP assay was 0.026±0.002 μg/mL. | [3] |
| • Cellphone-based detection of gold nanoparticle-labeled microfluidic immunoassay for human IgG | Chinese Academy of Sciences, China | The results of this on-chip immunoassay between anti-human IgG and human IgG were amplified by gold nanoparticle-enhanced staining and showed good correlation with hIgG concentration. | [4] | |
| • Cellphone-based personalized food allergen testing platform called iTube | UCLA, USA | Employs a light-weight, compact and cost-effective opto-mechanical attachment and a smart application that processes raw camera images within <1s. Detects allergen concentration in 20 min with a LOD of ~1 ppm. | [5] | |
| • Cellphone-based Escherichia coli detection platform | UCLA, USA | Employs a low-cost attachment, anti-E.coli O157:H7 antibody-functionalized capillary array and a quantum dot (QD)-based sandwich immunoassay. An LOD of ~5–10 cfu/mL is achieved for E.coli in water and milk samples. | [6] | |
| • Cellphone-based disposable immunoassay for diagnosing prostate cancer in urine using the PCADM-1 biomarkers | GENTAG, Inc. and MacroArray Technologies, LLC, USA | Non-invasive and highly cost-effective | [7] | |
| Lateral flow assays | • CBD for quantitative detection of thyroid stimulating hormone (TSH) | University of Arizona, USA | Detects TSH in <12 min with an LOD of 0.31 mIU L−1 using Mie scatter optimized lateral flow assay. Processing is done using an external PC. | [8] |
| • Cellphone-based Integrated rapid-diagnostic-test (RDT) reader | UCLA, USA | Compact, light-weight and cost-effective; powered by external or cellphone battery; employs a smart Android application to digitally process raw cellphone images within <0.2 s to create a diagnostic report (for e.g., HIV, malaria, etc.). | [9] | |
| • Cellphone-based rapid lateral flow test reader | Mobile Assay, Inc., USA | Employs mobile image ratiometry (MIR) to quantify rapid lateral flow test strips in 5–10 min. Detects cocaine and benzoylecgonine in the concentration range of 0.1–300 ng/mL and 0.003–0.1 ng/mL, respectively. | [10–12] | |
| Electrochemical biosensing | • Compact cellphone platform-based electrochemical sandwich immunoassay for the detection of PfHRP2 biomarker for malaria | UCLA + Michigan State University, USA | Assay duration 15 min, LOD 16 ng/mL, employs a compact embedded circuit, disposable microfluidic chips and use of capillary flow. | [15] |
| • iHealth Wireless Smart Gluco-Monitoring System | iHealth Lab Inc., USA | Saves up to 500 blood glucose test results wirelessly, track the trends, set up medication alerts and warns the user about the expiry of test strip. | [16] | |
| • Cellphone-based technology using the audio jack interface of iPhone to communication with point-of-care devices | Progical LLC, USA | Demonstrated the operation of OneTouch® UltraMini® glucose meter using an iPhone. | [17] | |
| • Cradle-configured interface between blood glucose meter and modem | North America technology Services, Inc., USA | Employs a multi-electrical contact-containing battery door that enables automatic download of blood glucose data (stored in the glucose meter) to an internal modem within a meter cradle and the data transmission to a central facility. | [18] | |
| • Cellphone-based transdermal glucose monitoring system using disposable skin patches with wireless sensors | GENTAG, Inc., Georgetown University and Science Applications International Corporation, USA | Each patch can be used for >100 glucose measurements over an extended period of time. It obviates the finger-pricking technology as the interstitial fluid is withdrawn by applying heat that ablates the stratum corneum. | [7] | |
| Surface plasmon resonance-based biosensing | • Cellphone-based angle-resolved SPR detection system | Linkoping University, Sweden | LOD 0.1 μg/mL for the detection of β microglobulin; negligible non-specific binding; disposable; uses the conditioned illumination by cellphone's screen; and, SPR signal detection by the front camera of cellphone. | [21] |
| Microscopy | • Cellphone-based light microscope, integrated with a smart application for automated image analysis, for brightfield and fluorescence microscopy | UC Berkeley, USA | Clinical imaging of P. falciparum-infected and sickle RBC in brightfield imaging mode and M. tuberculosis-infected sputum samples in fluorescence imaging mode. | [22] |
| • Cellphone-based optical microscope and visible-light spectrophotometer. | UC Davis, USA | Cellphone microscope has transmission and polarized microscopy modes, resolution of 1.5 μm over an imaging field of view of ~150 × 150 μm. Cellphone spectrophotometer has a bandwidth of 300 nm with a spectral resolution of ~5 nm. | [23] | |
| • Lensfree holographic cellphone microscope | UCLA, USA | USB-powered stand-alone unit; light-weight and compact (4.2 × 4.2 × 5.8 cm); CMOS image sensor; spatial resolution of ~1.5 μm over a FOV of ~24 mm2. Demonstrated imaging of micro-particles, WBCs, RBCs, platelets and waterborne parasites. | [25] | |
| • Lensfree holographic pixel-super resolution microscope | UCLA, USA | Submicron resolution over a large imaging FOV (~24 mm2). Demonstrated imaging of malaria infected blood samples. | [27] | |
| • Cellphone-based wide-field fluorescent microscope | UCLA, USA | Cost-effective and compact; uses battery-powered LEDs and an additional lens. Demonstrated for imaging of labeled WBCs in whole blood samples and waterborne parasites in water. | [28] | |
| Flow cytometry | • Cellphone-based optofluidic fluorescent imaging flow cytometer | UCLA, USA | Compact, light-weight and cost-effective; uses a low-cost lens, a plastic color filter and coin cell batteries; analyse large sample volumes of >0.1 mL; fluorescent resolution of ~2 μm. | [29] |
| • Cellphone-based miniaturized and low-cost imaging cytometry platform for rapid and cost-effective blood analysis | UCLA, USA | Determines the density of RBCs and WBCs, and the hemoglobin concentration in blood. Requires minute sample (~10 μL); good analytical performance as shown by validation with Sysmex KN21 hematology analyser. | [30] | |
| Colorimetric detection | • Cellphone-based technique for precise POC colorimetric measurements in commercially-available urine test strips and pH papers | University of Cincinnati and Air Force Research Laboratory, USA | Uses the chromaticity values to determine the analyte concentration, which partially compensates for the variation in lighting conditions. | [31] |
Applications of cellphone-based devices in bioanalytical sciences
Immunoassays
Cellphone-based quantitative analysis of high-sensitivity C-reactive protein (hsCRP) based on sandwich enzyme-linked immunosorbent assay (ELISA) has been recently demonstrated [3] using a cellphone for imaging of the colorimetric product obtained after enzyme-substrate reaction in a 96-well microtiter plate (MTP). The MTP was placed on a plain white paper to get uniform background, and a standard desk lamp with a 40 W bulb inclined at an angle of 50 degrees to the bench top surface was employed to reduce shadowing effects. The cellphone was placed at a distance of ~12 cm above the MTP for imaging the colorimetric readout. The images were then analysed by custom-developed MATLAB software (running on a PC) that transforms the images from native RGB color space to normalised RGB color space, which minimizes the effect of variations in illumination intensity. The normalised blue channel was selected for further image analysis, where 121 pixels (11 × 11 pixel region) from each MTP well were taken into account. The limit of detection of the cellphone-based hsCRP ELISA was 0.026 ± 0.002 μg/mL with R2 of 0.998. Similarly, researchers from the Chinese Academy of Sciences also demonstrated cellphone-based detection of gold nanoparticle-enabled microfluidic immunoassay for the measurement of human IgG plasma concentrations [4].
A personalized food allergen testing platform called iTube is one of the recent CBDs of the Biophotonics group at UCLA [5], which automatically analyses colorimetric assays performed in test tubes (i.e., 6-well tube arrays that are cut from a commercially available 96-well MTP) to digitally detect allergens in food samples (Fig. 1A). This light-weight (~40 g), compact (~22 mm × 67 mm × 75 mm) and cost-effective opto-mechanical attachment comprises an inexpensive plano-convex lens, two diffused light emitting diodes (LEDs) to vertically illuminate the test and control tubes that are loaded from the side, and circular apertures to spatially control the imaging field-of-view (FOV) (Fig. 1B). Allergen test and control assays (tubes) absorb the incident LED light, altering the intensity of the transmitted light recorded by the cellphone camera. The allergen concentrations are calculated using the iTube calibration equation [5] that takes into account the relative absorbance of the light passing through the test tube (with respect to the light passing the control tube) as well as the intensity variations between the two illumination LEDs. Based on this calibration equation, a smart application running on the same mobile unit processes raw camera images within <1s and provides the digitally quantified allergen (e.g., peanut) concentration in food samples. The performance of this platform is demonstrated by analysing several commercially-available cookies containing varying amounts (1–25 part per million, ppm) of peanut that were precisely quantified using this cellphone-based allergen testing platform within ~20 min per test, achieving a detection limit of ~1 ppm.
Fig. 1.
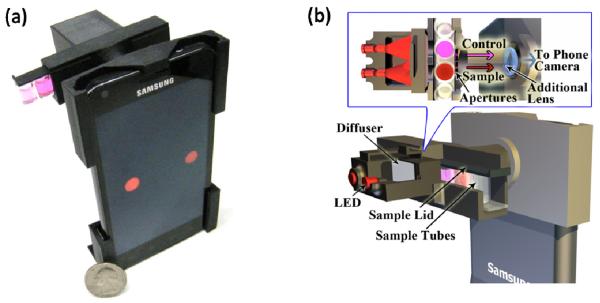
(A) Cellphone-based digital reader for colorimetric assays on iTube platform [5]. The opto-mechanical attachment (~22mm × 67mm × 75mm) that is installed at the back of the cellphone. (B) Schematics of the iTube platform. The iTube hardware attachment uses two interchangeable LEDs to illuminate the test and control tubes. Two diffusers are also inserted between the LEDs and the tubes to uniformly illuminate each tube. The transmitted light through each tube is then collected via a circular aperture and is imaged by the cellphone camera using an additional plano-convex lens (Focal length ~ 28 mm). A sample lid encloses the 6-well tube array and also works as an adaptor to insert the tube array inside the allergen tester attachment. Reproduced with permissions from the Royal Society of Chemistry.
The same group also introduced a cellphone-based E.coli detection platform that utilizes an anti-E.coli O157:H7 antibody-functionalized capillary array and a quantum dot (QD)-based sandwich immunoassay [6] (Fig. 2A). Achieving a detection limit of ~5–10 cfu/mL for E.coli in water and milk samples, this CBD employs a cost-effective attachment to the cellphone with dimensions of ~3.5 cm × 5.5 cm × 2.4 cm. It has an imaging FOV of e.g., 11 mm × 11 mm and can simultaneously monitor ~10 functionalized capillary tubes (length: ~11 mm; inner and outer diameters of ~100 μm and ~170 μm, respectively). Battery-powered ultra-violet LEDs are directly butt-coupled to the capillary array which acts as an opto-fluidic waveguide to enable uniform excitation of QD-labeled E.coli particles/fragments (Fig. 2B). An additional lens with a focal length of 15 mm is placed between the capillary array and the cellphone camera, enabling the emitted fluorescence light to be imaged by the cellphone camera unit.
Fig. 2.
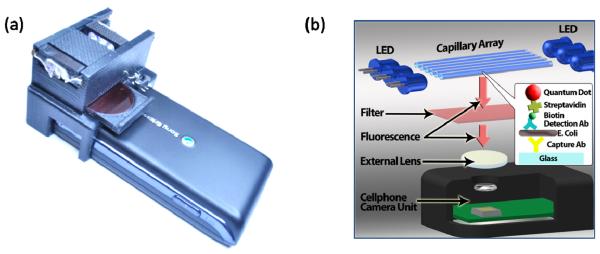
(A) Cellphone-based E.coli detection platform. (B) Schematic diagram of the optical attachment for E. coli detection on a cellphone using a quantum dot-based sandwich assay embedded in glass capillary tubes [6]. Reproduced with permissions from the Royal Society of Chemistry.
As another example, GENTAG, Inc. [7] and MacroArray Technologies, LLC jointly developed a cellphone-based urine analysis platform using a disposable immunoassay that employs the diagnostic marker PCADM-1 for prostate cancer diagnosis. It is a non-invasive and cost-effective consumer-based test for testing of prostate cancer that has an estimated market of about US$ 1.6 billion annually. The developed test can potentially replace the prostate specific antigen (PSA)-based blood tests that are currently being used worldwide.
Lateral flow assays
A prospective CBD has been developed by researchers at the University of Arizona for the quantitative measurement of thyroid stimulating hormone (TSH) in less than 15 min using Mie scattering-optimized lateral flow assay (LFA) [8] (Fig. 3). The limit-of-detection (LOD) of the developed CBD was 0.31 mIU L−1, which is below the minimum accepted TSH concentration of 0.4 mIU L−1 for hyperthyroidism. The human serum tests also yielded sensitive and reproducible results with an error of less than 7% that was comparable to the established clinical TSH immunoassay. The optimum angles of incident light and angles of detection from LFA bands were determined by minimizing the Mie scattering from the nitrocellulose membrane of the LFA, which resulted in maximized Rayleigh scattering detection from the gold nanoparticles embedded in the LFA strip. The developed CBD uses the flash already installed in cellphone camera module to illuminate the LFA strip using an optical fiber with a collimating lens. The quantified TSH levels were displayed and recorded on the cellphone and were digitally processed in MATLAB using a separate PC.
Fig. 3.

(A) Enlarged view of the CBD showing placement of collimating lens and optical fiber set at specific angles in reference to the LFA cassette [8]. (B) LFA device utilizes a nitrocellulose membrane with gold conjugate and absorbing pads that are protected by a plastic cassette enclosure. Though capillary flow, the specimen (i.e., analyte) propagates to the other end of the membrane, labelled by the gold nano-particles in the gold conjugate pad. Test and control lines in the membrane are previously coated with antibodies specific to the target analyte, i.e., anti-TSH immobilized antibodies and anti-IgG immobilized antibodies, respectively. Forming the antibody-antigen complexes, the control and test lines develop a color change, which indicates the validity and the test results (positive/negative). (C,D) The actual reader attached to cellphone with an inserted disposable TSH LFA cassette. Reproduced with permission from Elsevier B.V.
The Biophotonics group at UCLA developed a compact and light-weight (~65 g) cellphone-based universal rapid diagnostic test (RDT) reader [9] (Fig. 4A) that can read various lateral flow immuno-chromatographic assays for point-of-care (POC) and telemedicine applications. Powered by external batteries or the cellphone battery through a USB connection, this RDT reader attachment includes an inexpensive plano-convex lens, three LED arrays (two located underneath the RDT tray for reflection imaging and one at the top for transmission imaging) and a cost-effective microcontroller. This universal mobile reader can quantitatively interpret the signal changes/variations in various types of LFAs or RDTs due to a sample in reflection or transmission imaging modes under diffused LED illumination (Fig. 4B). The raw cellphone images are digitally processed within < 0.2 s through a smart application running on the same phone, which locally stores and also shares test results in the form of an evaluation report with a central server. Installed on Android- and iOS-based cellphones, this platform provides highly accurate and repeatable digital evaluation of RDTs such that it can even differentiate minor color signal variations, which are quite difficult to be quantified and observed by the human eye. Test results shared with the central database can be accessed through the same application or a remote computer using web browsers. Providing real-time spatio-temporal statistics for various infectious diseases (e.g., malaria, HIV, TB) and other conditions that can be diagnosed using LFAs or RDTs, this hybrid platform may assist healthcare professionals and policy makers to monitor, track and analyse emerging diseases and outbreaks.
Fig. 4.
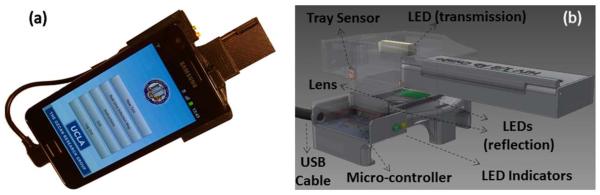
(a) The universal Rapid Diagnostic Test (RDT) reader installed on an Android phone [9]. The light-weight (65 g) opto-mechanical attachment can be repeatedly attached/detached to the cellphone body without the need for fine alignment and modification. (b) Schematic of the designed optical RDT reader attachment. RDT tray works as a mechanical adaptor to insert various RDT types into the same cellphone based reader attachment. The tray sensor is a conductive component that is used to sense the insertion of the tray and ensures the proper operation of the device. Controlled using a simple micro-chip, the illumination LEDs uniformly illuminate the RDT of interest that is imaged by the cell-phone camera through an additional plano-convex lens. Reproduced with permission from the Royal Society of Chemistry.
As another example, Mobile Assay, Inc. provides a cost-effective cellphone-based rapid lateral flow test reader together with Instantaneous Analysis™ software [10–11]. This platform employs Mobile Image Ratiometry (MIR) to quantify the rapid lateral flow test strips by the cellphone in 5–10 min. The quantification is achieved by digital analysis of the signal on the test strips, where the MIR subtracts background noise, selects the signal bands and provides their pixel density ratio. The test strip immunoassay involves the dispensing of the sample of interest at the specified area on the cassette. The capillary action then takes the liquid sample together with the nano-particle conjugated antibodies, which are specific for the analyte to be detected. If there is target analyte within the sample (and test strip is valid for operation), color will appear in two bands as the nano-particles will bind at both the test and the control areas. Labelled by the colloidal gold nano-particles, these target analyte - antibody complexes formed in the test band will generate a color signal due to enhanced light scattering. Therefore, increasing the target analyte concentration within the specimen will result in stronger signal in the immunochromatographic device. The Data Collection Module enables real-time data transfer to the Mobile Assay Cloud™ that can be accessed locally through Tracker™ or remotely through Mobile Assay Cloud™. Text alerts can then be pushed to the clients using the Tracker Manager™. The company has demonstrated the performance of their cellphone-based technologies for the screening of drugs (e.g., cocaine and benzoylecgonine), food pathogens (e.g., Botrytis cinerea) [12], water and aflatoxin that may be useful in industrial and clinical settings. This MIR-based CBD detected cocaine and benzoylecgonine in the concentration range of 0.1–300 ng/mL and 0.003–0.1 ng/mL, respectively. The technology has potential for the detection of food pathogens that might enable rapid and efficient tracking of the origin and severity of outbreaks. It may also help the food producers to take appropriate measures at an early stage to prevent the wide-scale distribution of contaminated food. Currently, there are about 48 million cases of foodborne illness annually in the United States [13], which incurs a financial burden of US$ 51–78 billion per year [14]. The same MIR-based CBD also enables the early detection and tracking of Botrytis cinerea (a fungus that causes significant damage to plants and flowers), which might increase agricultural productivity due to decreased crop losses.
Electrochemical biosensing
A compact mobile phone platform [15] (see Fig. 5) has been developed and demonstrated for the rapid detection of Plasmodium falciparum histidine-rich protein 2 (PfHRP2), which is an important biomarker for malaria. The developed electrochemical sandwich immunoassay takes 15 min, employs two loading steps of the sample and reporter (PfHRP2 detection antibodies conjugated to horse radish peroxidase) solutions, and detects PfHRP2 in human serum with a limit of detection of 16 ng/mL. The system comprises of a compact embedded circuit for signal processing and data analysis; disposable microfluidic chips for fluidic handling and biosensing; and use of capillary flow for sample loading, processing and pumping. The sample was loaded by a pipette but subsequently driven by capillary flow. The microfluidic chip measuring 25 mm × 15 mm has a hydrophilic PDMS surface coating that enables autonomous capillary-driven flow with a steady flow rate. It has 2 inlets and an outlet, which are 1 mm in diameter, and has a 2 mm chamber downstream to merge the appropriate volumes of sample (0.5 μL) and reporter (2 μL) solutions before they enter the mixer region. Thereafter, the serpentine channels, with a narrow spacing of 40 μM, enable the uniform flow of sample-reporter mixture over the electrochemical sensor area. Finally, a secondary serpentine channel, 25 cm long and having channels (400 μm × 100 μm), acts as a capillary pump as well as a waste reservoir. It accommodates the 3, 3', 5, 5'-tetramethylbenzidine/hydrogen peroxide (TMB/H2O2) substrate for washing and the enzymatic reactions for subsequent amperometric measurements. The PfHRP2 capture antibodies are uniformly bound to the polypyrrole-coated electrode surface. In the absence of PfHRP2, the detection antibodies cannot bind to the electrode and gets washed away when TMB/H2O2 substrate is loaded. While when PfHRP2 is present, the detection antibodies bind to the electrode. The interaction with TMB/H2O2 substrate and application of a voltage potential lead to the generation of an electrochemical current that is proportional to the PfHRP2 concentration in the analyte sample. The user performs the measurement through a smart Android application that provides step-by-step instructions on the screen. After each measurement, the results are displayed on the cellphone's screen and stored in its memory for later transmission and future analysis of the data. This pocket-size CBD, having a disposable SIM card-size microfluidic chip, has potential for POC diagnostics in decentralized labs such as the ones located in rural and remote areas. The developed sensor had good specificity, which was tested using purified PfHRP2 recombinant protein and 5 non-specific target proteins at a concentration of ~1 μg/mL. Moreover, it had high sensitivity, which was validated by spiking of human serum with PfHRP2 concentrations in the range of ~4–1020 ng/mL. These electrochemical measurements were taken over 60 s, where the final 15 s window was averaged to generate the dose-response profile.
Fig. 5.

(A) Assembled smartphone-based electrochemical sensor [15]. The arrow indicates the microfluidic chip. (B) Photograph of the chip and a mobile phone SIM card for comparison. (C) An enlarged image of the chip with labeled components. The channels are filled with a dye for improved visualization of the fluidic network. Reproduced with permission from the Royal Society of Chemistry.
At the Consumer Electronics Show 2013, iHealth Lab Inc. [16] announced the iOS-enabled Wireless Smart Gluco-Monitoring System, which is one of the next-generation glucose monitoring devices that might be useful for diabetic monitoring and management as it can save up to 500 blood glucose test results, track the progress of the results, and set up medication alerts. Moreover, it can automatically warn the user if the test strip expires, thereby preventing potential false evaluations.
As another example, Progical LLC [17] has developed a cellphone-based technology that uses the 3.5 mm audio jack interface of iPhone for effective communication with point-of-care devices. Using this platform technology, they have demonstrated the operation of OneTouch® UltraMini® glucose meter using an iPhone. A cradle-configured interface between a blood glucose meter and a modem has also been developed by other researchers [18]. It has a multi-electrical contact-containing battery door, which enables the automatic download of blood glucose analysis data stored in the glucose meter to an internal modem within a meter cradle and data transmission to a central healthcare monitoring facility.
GENTAG, Inc., Georgetown University and Science Applications International Corporation (SAIC) have developed a cellphone-based painless transdermal glucose sensing and monitoring system using disposable skin patches with wireless sensors. Each patch can be used for more than 100 glucose measurements over an extended period of time at customized time intervals. Moreover, high density patches of up to 40,000 test sites can also be manufactured [19–20]. This technology obviates the finger-pricking technology as the interstitial fluid (IF) is withdrawn by applying heat that ablates the stratum corneum. The IF is then delivered to the detector area within the skin patch through simple capillary action. Apart from glucose measurements, the same cellphone based technology can potentially be programmed also for insulin delivery and for the geolocation of patients in case of an emergency.
Surface plasmon resonance based biosensing
An angle-resolved surface plasmon resonance (SPR) detection system [21] (Fig. 6A) was also developed and employed for the detection of β2 microglobulin (β2M), which is a biomarker for cancer, kidney disease and inflammatory disorders. It was based on a single disposable device that uses the conditioned illumination provided by the cellphone's screen and the optical detection of SPR signal by the front camera of the cellphone. The SPR coupler gently adheres to the cellphone's screen to couple the illumination provided by the screen. It is detached and disposed after the measurement. The cellphone display provides the desired wide-angle illumination for the angle-resolved SPR experiments, while the front camera (typically VGA or 2 MP with intensity measurements limited to 256 levels/channel) records the angle-resolved SPR signals when fitted with the SPR coupler. The illumination light was provided by the image of a red rectangle displayed on the cellphone screen, while the placement of the SPR coupler on the screen was outlined by the image of a displayed white frame [21]. The SPR coupler, made up of polydimethylsiloxane (PDMS) rubber and epoxy, has a refractive index of 1.5, roughly matching that of glass. The epoxy layer was required to achieve the desired illumination angles on the gold (Au)/water interface under red illumination. The angle-resolved SPR signal, carried in the light reflected from the Au interface, was conditioned by a PDMS cylindrical element followed by deflection due to the total internal reflection within the PDMS prism. The sensing operation is controlled by a custom-developed software, which sets the exposure of the camera to assure that the SPR signals are measured in identical/repeatable conditions. The developed SPR system was tested for the detection of β2M using the commercial Biacore sensor chip CM5 and a custom-made chip, which were both functionalized with monoclonal mouse-anti-human β2M. It detected pathophysiological range of β2M in humans with negligible non-specific binding and a limit of detection of about 0.1 μg/mL [21]. The custom-made chip was comprised of three channels i.e. two calibration channels for high and low concentrations, and the test channel for the test concentration to be determined (Fig. 6B). An iOS 5 based smart application was employed for the image acquisition. It allows the setting and locking of the camera exposure and related parameters so that all the signals are measured in identical conditions [21].
Fig. 6.

(A) (a) 3D scheme of a representative setup for angle-resolved SPR using cellphone screen illumination and front camera detection optically coupled by a disposable device [21]. (b) 2D ray-trace of the experimental arrangement showing the light path from the screen to the camera. (c) Picture of the actual experimental arrangement. (B) (a) Interaction analysis of a commercial Biacore CM5 test chip functionalized for β2 microglobulin detection and tested at 1.32 μg mL−1 and 0.132 μg mL−1 concentrations. The baseline of the measurement is indicated with a blue line, while red and orange lines indicate normal serum and urine levels, respectively. (b) Test chip with embedded calibrations (H and L for high and low references) providing direct quantification of the unknown test value (T). Reproduced with permission from Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim.
Microscopy
A cellphone-mounted light microscope was developed for cost-effective brightfield and fluorescence microscopy [22]. It was employed for imaging of P. falciparum-infected and sickle red blood cells (RBC) in brightfield imaging mode and M. tuberculosis-infected sputum samples in fluorescence imaging mode using LED excitation. Similarly, other cellphone attachments were developed [23] to transform the cellphone into an optical microscope and visible-light spectrophotometer. The cellphone microscope had transmission and polarized microscopy modes, with a resolution of ~1.5 μm over an imaging FOV of ~150 μm × 150 μm. The spectrophotometer had a bandwidth of 300 nm with a spectral resolution of ~5 nm.
UCLA Biophotonics group also developed various cellphone-based imaging technologies for healthcare, telemedicine and bioanalytical applications [5, 6, 9, 24–30]. In particular, the UCLA Group has introduced a set of compact, light-weight and computational microscopes that operate based on partially-coherent lensfree digital in-line holography, providing highly-sensitive and high-throughput alternatives to conventional lens-based microscopes, especially for field settings and remote locations. As a spin-off from UCLA, Holomic LLC [24] was formed in 2011 to commercialize these photonics-based imaging and sensing technologies. In 2008, the UCLA group initially implemented this lensfree holographic imaging technique on a USB-powered stand-alone unit [25] that weighs ~46 grams (Fig. 7A). It utilizes a single LED together with a large pinhole (an aperture of ~100 μm in front of the source) to illuminate the sample of interest that is loaded using a sample tray located on the side of the microscope. Spatially filtered LED light interacts with the sample and creates holographic signatures of individual particles/cells that are recorded by a complementary metal-oxide semiconductor (CMOS) image sensor-array. These lensfree holograms that are formed by the interference between the un-scattered background light and the scattered object fields are then rapidly processed using custom-developed holographic reconstruction algorithms to provide amplitude and phase images of the samples of interest. With dimensions smaller than 4.2 × 4.2 × 5.8 cm, this field-portable microscope achieves a spatial resolution of ~1.5 m over a FOV of ~24 mm2 that is an order of magnitude larger than the imaging area of a typical 10X objective lens. Moreover, the same imaging concept was also implemented on a commercially-available cellphone device [26] that is modified using a simple hardware attachment (~ 38 grams) on the phone (Fig. 7B). Installed at the back of the cellphone camera, this mechanical attachment encloses a battery-powered LED and a large pinhole to illuminate the sample. Instead of using an external imaging sensor, this lensfree cellphone microscope utilizes the CMOS imager chip already embedded on the cellphone camera module to acquire lensfree holographic images of the samples. The performance of these compact and light-weight microscopes was demonstrated by imaging micro-particles, white blood cells (WBCs), red blood cells (RBCs), platelets as well as waterborne parasites.
Fig. 7.

(a) A lensfree stand-alone microscope based on partially-coherent digital in-line holography [25]. (b) A lensfree cellphone microscope [26]. (c) Lensfree Holographic Pixel-Super Resolution Microscope [27]. (d) Picture of the fluorescent imager prototype utilizing an optical attachment for wide-field fluorescent imaging on a cellphone [28]. (e) Optofluidic fluorescent imaging cytometer on a cellphone [29]. (f) Cellphone based blood analysis platform. It includes a base attachment with two AA batteries and a universal port for adapting three different add-on components for white blood cell, red blood cell and hemoglobin density measurements [30]. Reproduced with permissions from The Royal Society of Chemistry and American Chemical Society.
It is important to note that this lensfree microscopy approach is based on unit magnification (since the pinhole-to-sample distance is much larger than the sample-to-sensor distance) and it differs from conventional holographic imaging techniques in terms of not only the use of optical components, but also the parameter regime. Therefore, this unique design of lensfree holographic on-chip microscopy can effectively use the entire active imaging area of the imaging sensor as its object FOV, which can easily reach >20–30 mm2. On the other hand, these lensfree holograms are spatially undersampled due to the unit magnification and finite pixel size of the imaging sensor, limiting the spatial resolution of this platform.
In order to eliminate this pixel-size limitation on achievable resolution, the UCLA group later introduced a field-portable lensfree pixel super-resolution microscope (Fig. 7C) that achieves deeply submicron resolution over the same imaging FOV (e.g., ~24 mm2) [27]. This approach depends on the acquisition of multiple holographic images that are spatially shifted with respect to each other by sub-pixel pitch distances, after which higher resolution holograms of the sample can be synthesized through pixel super-resolution based reconstruction techniques. Increasing the effective sampling rate of the lensfree holograms, this approach significantly improved the spatial resolution (e.g., down to <0.3 μm) of lensfree amplitude and phase images that are reconstructed. To demonstrate its proof of concept, malaria infected blood samples are also imaged using this pixel super-resolved on-chip microscope to distinguish healthy RBCs from parasite infected ones over large a field of view [27].
The UCLA group has also demonstrated a cellphone-based fluorescent and dark-field microscope that employs a cost-effective and compact (~28 g) opto-mechanical attachment installed on a cellphone [28] (Fig. 7D). This cellphone attachment uses battery-powered butt-coupled LEDs to pump the sample of interest that is loaded to the attachment using a cuvette, which acts as an opto-fluidic waveguide and enables uniform excitation of the sample. An additional lens is also utilized in the attachment to image the fluorescent emission that is filtered through a plastic color filter using the cellphone camera. This cellphone based fluorescent microscope was used to image labeled WBCs in whole blood samples and waterborne parasites in drinking water.
Flow cytometry
A cellphone based optofluidic fluorescent imaging flow cytometer was developed by the Biophotonics group at UCLA to analyse large sample volumes of >0.1 mL [29]. A compact, lightweight (~18 g) and cost-effective cellphone attachment was developed, using an inexpensive lens, a plastic color filter (cost <0.1 USD), two LEDs (cost ~ 0.6 USD) and coin cell batteries (cost ~0.5 USD). Using a syringe pump, the sample is continuously delivered to the imaging volume through a disposable microfluidic channel, which acts as a multi-layered opto-fluidic waveguide (Fig. 7E). The dark-field background is created by using an inexpensive plastic absorption filter as the guided excitation light propagates perpendicular to the detection path. The motion of the cells flowing through the microfluidic channel was recorded and processed automatically to determine the cell count and the density. Providing a fluorescence resolution of ~2 μm, this platform can be used for whole blood analysis and screening of waterborne parasites in drinking water.
The same group also developed a CBD that involves a miniaturized and low-cost imaging cytometry platform along with the smart application running on the phone, to measure the density of RBCs and WBCs that are imaged in bright-field and fluorescent modes, respectively, and to simultaneously determine the hemoglobin (Hb) concentration in human blood samples [30] (Fig. 7G). The developed CBD for rapid blood analysis has a small sample requirement of ~10 μL, and provides a decent analytical performance that is validated using a standard bench-top Sysmex KN21 hematology analyser [30]. The platform employs a universal base that attaches to the cellphone camera unit, and three add-on components for WBC and RBC counting, and Hb density measurements. The desired add-on component can be clicked into the same port on the base attachment to perform the specific blood test of interest using the smart application running on the same cellphone that is used for image analysis and cell counting.
Colorimetric detection
A prospective cellphone-based technique was also developed by researchers from the University of Cincinnati and Air Force Research Laboratory, USA for POC colorimetric detection [31]. It was developed for the quantification of colorimetric paper test strips i.e. commercially-available urine test strips and pH paper tests (Fig. 8). The technique employs the use of chromaticity values in acquired images for the determination of the analyte concentration and to partially compensate the variation in external lighting conditions (e.g., sunlight or room light). It can be potentially useful for the development of various colorimetric CBDs for remote and POC settings.
Fig. 8.

Cellphone-based technique for colorimetric measurements in urine test strips [31]. Reproduced with permission from the Royal Society of Chemistry.
Conclusions and Future Opportunities
The initial proof-of-concept designs and the prototypes of CBDs that have already been developed, clearly demonstrate the tremendous potential of cellphones for various bioanalytical applications, as also summarized in Table 1. The most recent FDA approved AliveCor Heart Monitor platform (Fig. 9) [32] is one of these significant achievements, which may inspire the development of other commercially-viable CBDs in the coming years. Cellphone technology has already attracted considerable attention as a promising platform for mHealthcare and telemedicine applications [3–48] that can significantly improve healthcare delivery and provide better health management tools globally. This has led to rapid growth in public interest and significant increase in funding, enabling convergence of various scientific disciplines, such as engineering, biomedical sciences, chemistry and physical sciences, etc., to develop innovative and interdisciplinary technologies and solutions. These on-going research and development efforts are expected to significantly expand the cellphone-based bioanalytical applications, leading to next-generation POC devices and systems. Motivated by the massive market opportunity, CBDs have already been developed for e.g., physiological monitoring of the heart rate, ECG, blood pressure and weight. However, the recently introduced CBDs developed for chemical and biochemical sciences will further lead to significant advances in these fields.
Fig. 9.

AliveCor's Heart Monitor [32]. It is an FDA approved device that has recently been cleared for sale in US for use by medical professionals to record, display, store, and evaluate single-channel electrocardiogram (ECG) rhythms. Reproduced with permission from David McCaman, AliveCor, Inc.
Current efforts are especially focused on overcoming the challenges associated with miniaturization, clinical validation, reproducibility, robustness, adaptability to various and rapidly evolving models of cellphones, and compliance with industrial and healthcare requirements. The FDA-approved LFA test strips are already commercially-available for several disease biomarkers, infectious diseases, hormones and drug screening tests. Similarly, most of the POC glucose meters are also FDA-approved. Therefore, the use of such FDA-approved or CE-certified devices that are integrated with various CBDs might enable creation of new cellphone-based technologies and eventually products, entering the consumer market. Motivated by these, several funding agencies, governmental/non-governmental organizations and institutions are specifically interested in the use of CBDs in healthcare. Various countries have already started focused mHealthcare initiatives to take action and lead the efforts for providing an integrated telemedicine based healthcare system digitally merging clinics, laboratories, nursing homes, POC offices, hospitals and healthcare professionals as well as patients. Various CBDs and smart applications are already commercially-available and being used by cellphone users worldwide.
In the meantime, healthcare spending worldwide has been increasing continuously due to increased chronic diseases and aging population. In 2010, United States alone spent US$ 2.6 trillion on healthcare i.e., US$ 8402 per person [49], where medical diagnosis related expenses account for about 10%, i.e., $250 billion per year [50]. According to the Institute of Medicine, $750 billion in healthcare spending was wasted in 2009 [51]. Therefore, there is tremendous potential for CBDs that can significantly trim down some of these healthcare related costs by providing cost-effective personalized diagnosis and monitoring platforms with decent analytical performance. Some of these increased health issues due to rapid changes in lifestyle and nutrition are unbalanced by evolution and biological adaptation [52], which need to be addressed by healthcare management through disease prevention and health promotion initiatives [53]. Similarly, significant treatment efforts are required for metabolic diseases arising from overweight, malnutrition, reduced physical activities and major negative impact of mental stress factors. Cellphone-based personalized, predictive and preventive diagnostics and monitoring technologies would be highly prospective to address some of these issues and fall in line with the current trends toward “actionable diagnostics”, where new “personalized medicine” technologies are used by healthcare professionals to rapidly and accurately diagnose patients and prescribe more effective customized therapies. These strategies might significantly reduce healthcare costs and improve patient outcomes globally.
CBDs, incorporating highly sensitive, specific and multiplexed analyte detection capabilities, will lead to earlier detection of detrimental physiological and behavioural changes in individuals. These earlier medical interventions using CBD-based continuous and multi-parametric diagnostics might prevent the manifestations of later disease states requiring more expensive, chronic and often painful treatments. Therefore, CBDs might potentially provide the basis for the next-generation healthcare devices that can shift the instantaneous diagnostics regimen toward continuous, adaptive and non-invasive measurements using various bodily fluids, including blood, urine and saliva, or even physical properties such as pH and composition of electrolytes in sweat glands [54]. Based on all the technological advantages and the features that are pre-existing or can be built around CBDs, the next decade will likely witness a wide-spread usage of CBDs and related devices for a wide range of bioanalytical applications, significantly impacting human life and the quality of healthcare globally.
It should be emphasized that the conventional bioanalytical measurement technologies that are currently being used in various industrial, clinical and research settings have exceptional analytical performance and comply with the regulatory guidelines and established bioanalytical standards. Moreover, advanced data analysis and reporting software packages have been developed for these technologies. Most of these advanced instruments, such as GE Healthcare's BIAcore systems, Tecan's microtiter plate readers and Metroohm's Autolab platform, among others, are highly robust yielding specific, sensitive and reproducible results. Compared to these well-established bench-top based bioanalytical tools, cellphone-based technologies may not yet provide the same performance levels; however due to their extreme cost-effectiveness, compactness, light-weight and connectivity CBDs provide complementary solutions to existing bioanalytical tools. It will take some more time before CBDs can be adapted in large scale and be customized to the specifics of various bioanalytical measurement needs. Moreover, considering the rapidly evolving and constantly increasing number of cellphone models, each with a different set of technical specifications, CBD developers and manufacturers could face considerable challenges in the regulatory approval processes in various countries. This challenge, however, might also create a business opportunity to provide device designers and diagnostics companies with a supply of reliable and cost-effective older-generation cellphones. As an example, an intermediate company could invest in a large supply of a particular smartphone in order to provide CBD developers a reliable and regulated supply of cellphones for an extended duration of time, with a guarantee on the quality, parts/features and software.
In summary, the constant technological advances, strenuous research efforts as well as innovate business practices will counteract some of these challenges highlighted above, paving the way for the development of next-generation CBDs addressing the needs of various emerging bioanalytical settings. Towards this end, co-operation of healthcare professionals, policy makers, CBD developers, researchers and other medical device manufacturers in a multi-disciplinary environment may create sustainable advancements and improvements in CBDs and their applications in bioanalytical sciences, providing cost-effective and field-portable alternatives to conventional bench-top technologies that cannot be used beyond well-established laboratories.
Acknowledgements
Ozcan Research Group gratefully acknowledges the support of the Presidential Early Career Award for Scientists and Engineers (PECASE), Army Research Office (ARO) Life Sciences Division, ARO Young Investigator Award, National Science Foundation (NSF) CAREER Award, NSF CBET Biophotonics Program, NSF EFRI Award, Office of Naval Research (ONR) Young Investigator Award and National Institutes of Health (NIH) Director's New Innovator Award DP2OD006427 from the Office of the Director, National Institutes of Health. Finally, the authors acknowledge various clinicians working in the field of intensive care for their intellectual support toward this review of future applications of smartphone based diagnostics tools to facilitate better patient monitoring.
Abbreviations
- CBD
Cellphone-based devices
- POC
Point-of-care
- mHealthcare
Mobile Healthcare
- ELISA
Enzyme-linked immunosorbent assay
- LED
Light-emitting diodes
- QD
Quantum dot
- hsCRP
High-sensitivity C-reactive protein
- PCADM-1
Prostate cancer antigen diagnostic marker 1
- MTP
Microtiter plate
- TSH
Thyroid stimulating hormone (TSH)
- LFA
Lateral flow assay
- RDT
Rapid diagnostic test
- LFI
Lateral flow immunoassay
- MIR
Mobile image ratiometry
- PfHRP
Plasmodium falciparum histidine-rich protein 2
- SPR
Surface plasmon resonance
- β2M
β2 microglobulin
- PDMS
Polydimethylsiloxane
- RBC
Red blood cells
- FOV
Field-of-view
- SNR
Signal-to-noise ratio
- Hb
Hemoglobin
- ECG
Electrocardiogram
- BP
Blood pressure
- FDA
Food and Drug Administration
- CE
Conformité Européenne
- ESH
European Society of Hypertension
- NFC
Near-field communication
- RR
Radar responsive
- RFID
Radio frequency identification device
- IF
Interstitial fluid
Footnotes
Published in the topical collection Multiplex Platforms in Diagnostics and Bioanalytics with guest editors Günter Peine and Günther Proll.
Conflicts of Interest Statement A.O. is the co-founder of a start-up company (Holomic LLC) which aims to commercialize computational imaging and sensing technologies licensed from UCLA. O.M is currently employed by the same start-up company.
References
- [1]. [Accessed 4 July 2013]; http://www.itu.int/net/pressoffice/press_releases/2012/70.aspx#.UNl_qnfInjs.
- [2]. [Accessed 4 July 2013]; http://mobithinking.com/mobile-marketing-tools/latest-mobile-stats.
- [3].McGeough CM, O'Driscoll S. IEEE Transactions on Biomedical Circuits and Systems. 2013. Camera Phone-Based Quantitative Analysis of C-Reactive Protein ELISA. DOI: 10.1109/TBCAS.2012.2234122. [DOI] [PubMed] [Google Scholar]
- [4].Lu Y, Shi S, Qin J, Lin B. Low cost, portable detection of gold nanoparticle-labeled microfluidic immunoassay with camera cell phone. Electrophoresis. 2009;30:579–582. doi: 10.1002/elps.200800586. [DOI] [PubMed] [Google Scholar]
- [5].Coskun AF, Wong J, Khodadadi D, Nagi R, Tey A, Ozcan A. A personalized food allergen testing platform on a cellphone. Lab Chip. 2013;13:636–640. doi: 10.1039/c2lc41152k. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Zhu H, Sikora U, Ozcan A. Quantum dot enabled detection of Escherichia coli using a cell-phone. Analyst. 2012;137:2541–2544. doi: 10.1039/c2an35071h. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7]. [Accessed on 4 July, 2013]; www.gentag.com.
- [8].You DJ, Park TS, Yoon J-Y. Cell-phone-based measurement of TSH using Mie scatter optimized lateral flow assays. Biosens. Bioelectron. 2013;40:180–185. doi: 10.1016/j.bios.2012.07.014. [DOI] [PubMed] [Google Scholar]
- [9].Mudanyali O, Dimitrov S, Sikora U, Padmanabhan S, Navruz I, Ozcan A. Integrated Rapid-Diagnostic-Test Reader Platform on a Cellphone. Lab Chip. 2012;12:2678–2686. doi: 10.1039/c2lc40235a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10]. [Accessed on 4 July, 2013]; www.mobileassay.com.
- [11].Cooper DC, Callahan B, Callahan P, Burnett L. Nature Precedings. 2012. Mobile Image Ratiometry: A New Method for Instantaneous Analysis of Rapid Test Strips. DOI: 10.1038/npre.2012.6827.1. [Google Scholar]
- [12].Cooper DC. Nature Precedings. 2012. Mobile Image Ratiometry for the Detection of Botrytis cinerea (Gray Mold) DOI: 10.1038/npre.2012.6989.1. [Google Scholar]
- [13]. [Accessed on 4 July, 2013]; http://www.cdc.gov/features/dsfoodnet/.
- [14].Scharff RL. Economic burden from health losses due to foodborne illness in the United States. J. Food Prot. 2012;75:123–131. doi: 10.4315/0362-028X.JFP-11-058. [DOI] [PubMed] [Google Scholar]
- [15].Lillehoj PB, Huang M-C, Truong N, Ho C-M. Rapid electrochemical detection on a mobile phone. Lab Chip. 2013 doi: 10.1039/c3lc50306b. DOI: 10.1039/c3lc50306b. [DOI] [PubMed] [Google Scholar]
- [16]. [Accessed on 4 July, 2013]; www.ihealth99.com.
- [17]. [Accessed on 4 July, 2013]; www.progical.com.
- [18].Oberding JW, Geiger GE, White KD, Ward RN. Blood glucose meter/modem interface arrangement. US Patent Application, Publication No. US 7,181,350 B2. 2007
- [19].Vashist SK, Zheng D, Al-Rubeaan K, Luong JHT, Sheu F-W. Technology behind commercial devices for blood glucose monitoring in diabetes management: a review. Anal. Chim. Acta. 2011;703:124–136. doi: 10.1016/j.aca.2011.07.024. [DOI] [PubMed] [Google Scholar]
- [20].Vashist SK. Non-invasive glucose monitoring technology in diabetes management: a review. Anal. Chim. Acta. 2012;750:16–27. doi: 10.1016/j.aca.2012.03.043. [DOI] [PubMed] [Google Scholar]
- [21].Preechaburana P, Gonzalez MC, Suska A, Filippini D. Surface plasmon resonance chemical sensing on cell phones. Angew. Chem. 2012;124:11753–11756. doi: 10.1002/anie.201206804. [DOI] [PubMed] [Google Scholar]
- [22].Breslauer DN, Maamari RN, Switz NA, Lam WA, Fletcher DA. Mobile Phone Based Clinical Microscopy for Global Health Applications. PLoS ONE. 2009;4:e6320. doi: 10.1371/journal.pone.0006320. DOI: 10.1371/journal.pone.0006320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Smith ZJ, Chu K, Espenson AR, Gryshuk A, Molinaro M, Dwyre DM, Lane S, Matthews D, Wachsmann-Hogiu S. Cell-Phone-Based Platform for Biomedical Device Development and Education Applications. PLoS ONE. 2011;6:e17150. doi: 10.1371/journal.pone.0017150. DOI:10.1371/journal.pone.0017150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24]. [Accessed 4 July 2013]; www.holomic.com.
- [25].Mudanyali O, Tseng D, Oh C, Isikman SO, Sencan I, Bishara W, Oztoprak C, Seo S, Khademhosseini B, Ozcan A. Compact, Light-weight and Cost-effective Microscope based on Lensless Incoherent Holography for Telemedicine Applications. Lab Chip. 2010;10:1417–1428. doi: 10.1039/c000453g. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Tseng D, Mudanyali O, Oztoprak C, Isikman SO, Sencan I, Yaglidere O, Ozcan A. Lensfree microscopy on a cellphone. Lab Chip. 2010;10:1787–1792. doi: 10.1039/c003477k. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Bishara W, Sikora U, Mudanyali O, Su T-W, Yaglidere O, Luckhart S, Ozcan A. Holographic pixel super-resolution in portable lensless on-chip microscopy using a fiber-optic array. Lab Chip. 2011;11:1276–1279. doi: 10.1039/c0lc00684j. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Zhu H, Yaglidere O, Su T-S, Tseng D, Ozcan A. Cost-effective and compact wide-field fluorescent imaging on a cell-phone. Lab Chip. 2011;11:315–322. doi: 10.1039/c0lc00358a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Zhu H, Mavandadi S, Coskun AF, Yaglidere O, Ozcan A. Optofluidic Fluorescent Imaging Cytometry on a Cell Phone. Anal. Chem. 2011;83:6641–6647. doi: 10.1021/ac201587a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Zhu H, Sencan I, Wong J, Dimitrov S, Tseng D, Nagashima K, Ozcan A. Cost-effective and rapid blood analysis on a cell-phone. Lab Chip. 2013;13:1282–1288. doi: 10.1039/c3lc41408f. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Shen L, Hagen JA, Papautsky I. Point-of-care colorimetric detection with a smartphone. Lab Chip. 2012;12:4240–4243. doi: 10.1039/c2lc40741h. [DOI] [PubMed] [Google Scholar]
- [32]. [Accessed on 4 July, 2013]; www.alivecor.com.
- [33]. [Accessed on 4 July, 2013]; www.cellscope.com.
- [34]. [Accessed on 4 July, 2013]; http://web.media.mit.edu/~pamplona/NETRA/.
- [35].Wong C. Cell-phone compatible wireless stethoscope. US Patent Application, Publication No. US 2012/0190303 A1. 2012
- [36].Kadlec M, You D, Wong PK. Proceedings of μTAS. 2011. A cell phone-based microphotometric system for rapid antimicrobial resistance profiling at the point-of-care; pp. 1167–1169. [Google Scholar]
- [37]. [Accessed on 4 July, 2013]; www.glucomo.com.
- [38]. [Accessed on 4 July, 2013]; http://web.mit.edu/press/2010/moca-source-code.html.
- [39].Kenyon JI, Poropatich R, Holtel MR. Cell Phones in Telehealth and Otolaryngology. Otolaryngologic Clinica of North America. 2011;44:1351–1358. doi: 10.1016/j.otc.2011.08.013. [DOI] [PubMed] [Google Scholar]
- [40].Martinez AW, Phillips ST, Carrilho E, Thomas SW, III, Sindi H, Whitesides GM. Simple Telemedicine for Developing Regions: Camera Phones and Paper-Based Microfluidic Devices for Real-Time, Off-Site Diagnosis. Anal. Chem. 2008;80:3699–370. doi: 10.1021/ac800112r. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Bhatti N, Baker H, Marguier J, Berclaz J, Susstrunk S. Proc. SPIE Mobile Multimedia/Image Processing, Security, and Applications 2010, SPIE Vol. 7708, Paper No. 7708-01. 2010. Cell Phones as Imaging Sensors. 2010. [Google Scholar]
- [42].Bellina L, Missoni E. Mobile cell-phones (M-phones) in telemicroscopy: increasing connectivity of isolated laboratories. Diagnostics Pathology. 2009;4:19. doi: 10.1186/1746-1596-4-19. DOI: 10.1186/1746-1596-4-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [43].Montes JM, Medina E, Gomez-Beneyto M, Maurino J. A short message service (SMS)-based strategy for enhancing adherence to antipsychotic medication in schizophrenia. Psychiatry Res. 2012;200:89–95. doi: 10.1016/j.psychres.2012.07.034. [DOI] [PubMed] [Google Scholar]
- [44].Lester RT, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomized trial. Lancet. 2010;376:1838–1845. doi: 10.1016/S0140-6736(10)61997-6. [DOI] [PubMed] [Google Scholar]
- [45].Thomas MA, Narayan PR, Christian C. Mitigating gaps in reproductive health reporting in outlier communities of Kerala, India—A mobile phone-based health information system. Health Policy and Technology. 2012;1:69–76. [Google Scholar]
- [46].Lamel SA, Haldeman KM, Ely H, Kovarik CL, Pak H, Armstrong AW. Application of mobile teledermatology for skin cancer screening. J. Am. Acad. Dermatol. 2012;67:576–581. doi: 10.1016/j.jaad.2011.11.957. [DOI] [PubMed] [Google Scholar]
- [47].Benhamou P-Y, Melki V, Boizel R, Perreal F, Quesada J-L, Bessieres-Lacombe S, Bosson J-L, Halimi S, Hanaire H. 1 year efficacy and safety of Web-based follow-up using cellular phone in type 1 diabetic patients under insulin pump therapy: the PumpNet study. Diabetes & Metabolism. 2007;33:220–226. doi: 10.1016/j.diabet.2007.01.002. [DOI] [PubMed] [Google Scholar]
- [48]. [Accessed on 4 July, 2013]; http://www.kff.org/insurance/upload/7670-03.pdf.
- [49]. [Accessed on 4 July, 2013]; http://www.managedcaremag.com/archives/0905/0905.diagnosis.html.
- [50]. [Accessed on 4 July, 2013]; http://blog.safeguard.com/index.php/2013/03/06/3-ways-diagnostics-can-cut-healthcare-costs-and-improve-patient-outcomes.
- [51]. [Accessed on 4 July, 2013]; http://www.iom.edu/Reports/2012/Best-Care-at-Lower-Cost-The-Path-to-Continuously-Learning-Health-Care-in-America.aspx.
- [52].Shapira N. Women's higher health risks in the obesogenic environment: a gender nutrition approach to metabolic dimorphism with predictive, preventive, and personalised medicine. The EPMA Journal. 2013;4:1. doi: 10.1186/1878-5085-4-1. DOI:10.1186/1878-5085-4-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [53].Shortell SM. Bridging the Divide Between Health and Health Care. JAMA. 2013;309:1121–1122. doi: 10.1001/jama.2013.887. [DOI] [PubMed] [Google Scholar]
- [54].Shirasu M, Touhara K. The scent of disease: volatile organic compounds of the human body related to disease and disorder. J Biochem. 2011;150:257–266. doi: 10.1093/jb/mvr090. [DOI] [PubMed] [Google Scholar]