

Abstract
Background:
Throughout the world, a large number of surveys have been carried out to find the prevalence of dementia with variable results.
Aims:
This study was to generate data on the prevalence of dementia and to generate a hypothesis on the differential distribution across populations.
Materials and Methods:
Four settings identified for the purpose of this study included a migrant, urban, rural, and tribal. The study was conducted in two phases: 1) A screening phase and 2) a clinical phase, on 2,000 individuals above 60 years of age. To complete the required sample of 2,000 elderly individuals, 500 individuals were approached from each site. Nobody refused to participate.
Results:
A total of 32/2,000 (1.6%) elderly individuals were classified as demented. No case of dementia was reported from tribal population. A look at sex differential reveals that majority (21/32; 66%) of individuals identified as demented were females. As age advanced scores on cognitive screen decreased with elders above 80 years of age showing lowest scores. Out of 32, 18 (56%) of patients classified as demented were more than 80 years of age.
Conclusion:
The findings of this study are in agreement with previous studies which point towards differential distribution of dementia across populations.
Keywords: Dementia, Migrant, Rural, Urban, Tribal
Introduction
Aging is a global phenomenon. It has picked up momentum in low-income countries of Asia, Latin America, and Africa. India is no exception to this and is undergoing a rapid demographic transition now. It is important to note that this rapid demographic change is happening along with fast-paced social restructuring. India is home to more than 76 million people aged 60 years and above.[1] This age group, currently comprising only 7.4% of the population, is expected to grow dramatically in the next few decades. It is estimated that there are already approximately 1.5 million people affected by dementia in India, and this number is likely to increase by 300% in the next 4 decades.[2] Dementia is an emerging public health problem and a major cause of disability and mortality among the elderly. Throughout the world, a large number of surveys have been carried out to find the prevalence of dementia with variable results.[3,4,5,6,7,8] All results show a marked increase in the prevalence of this disorder with increase in age. The evidence on prevalence of dementia in India has expanded considerably in the last few decades. However, the evidence is not uniformly scattered across the country. Data on the prevalence of dementia is lacking in many regions of the country and the studies have reported widely varying estimates of prevalence. On one hand, this wide variability across populations poses difficulties to provide a consistent overview for the whole country; while on the other, it opens areas for research in understanding the cause for this variability in first place. This understanding may go a long way in arriving at the population risk for differential distribution. The current study was primarily aimed at generating data on the prevalence of dementia and to generate a hypothesis on the differential distribution across populations.
Materials and Methods
The study was a part of a project to estimate the prevalence of dementia in four geographically defined habitations in Himachal Pradesh state of India. The study was conducted after obtaining approval from institution ethics committee. The state of Himachal Pradesh situated in the northwestern Himalayas extends between 32°22’-33°12’N, and 75°45’-79°04’E covering an area of 56,090 km2. Topography of the state is dominantly mountainous with the altitude ranging between 350 and 6,975 m. The state has a total population of 6,856,509 and 90.2% people live in rural setup.
The four settings identified for the purpose of this study included a migrant, urban, rural, and tribal. Five hundred individuals above 60 years of age were included from each geographical site giving us a target sample size of 2,000. A sample size of 2,000 would allow estimation of a typical dementia prevalence of 4.5% (standard error 0.9%).[9]
The study was conducted in two phases: 1) A screening phase and 2) a clinical phase. The screening also involved a detail of the sociodemographic profile of study population.
Screening
All subjects were screened and a subset identified for the detailed clinical evaluation after screening. Trained interviewers administered a standardized Hindi cognitive screening battery, used in a previous study on largely illiterate elderly population in India.[3]
This Hindi version of cognitive screen (Hindi Mental State Examination (HMSE)) was used in urban, rural, and migrant population. For the tribal population, a modified version of cognitive screen was used. The screen used on tribal population, had to be reliable and valid and as comparable as possible in content, format, and relative level of difficulty to the cognitive screen (HMSE) used in urban, rural, and migrant populations. For this purpose a modified version of MMSE was developed. The details are provided elsewhere.[10]
The screening phase consisted of a cross-sectional comprehensive two-phase survey of all residents aged 60 years and older. A house-to-house survey was conducted to identify individuals eligible for inclusion in the study. All eligible individuals present in their homes on the day of survey and who gave their consent to participate were included in the study. Nobody refused to participate in the study. In this way a total of 500 consecutive individuals were identified for the purpose of this study from each selected geographical site to be included in the sample for the purpose of this study.
The interviews were conducted in participants homes with participants asked to provide informed written consent. Next of kin was asked to provide written agreement in the event of lack of capacity to consent. Further, 10% of individuals categorized as not having on the basis of cognitive screen were also evaluated clinically using the criteria that would have been used in case of a suspect of dementia.
A detailed history of the sociodemographic profile of study population was enquired.
Clinical evaluation and diagnosis
A score below 24 (out of a possible score of 30) on cognitive screen was considered as a suspect case of dementia and was evaluated for clinical diagnosis. Further 10% of non-demented individuals were also evaluated clinically. The selection of 10% non-demented individuals for clinical evaluation was similar to the process carried out for purpose of screening for presence of dementia. In this way every 10th elderly individual was included for clinical evaluation. The clinical evaluation was carried out by a psychiatrist with the help from an internist and two public health specialists. The internist (SR) has already worked on a similar study on Kashmiri migrants. The psychiatrist (SS) has been working in his area of expertise for last 15 years and has been involved in development of cognitive screen for tribal population. One of the public health experts (SKR) has already worked on the development of Kashmiri, Dogri and the cognitive screen for tribal population and the second public health specialist (AKB) has been working in his area of expertise for last 25 years and was involved in development of cognitive screen for tribal population. The clinical assessment of dementia involved a careful detailed clinical history to determine the precise features of intellectual loss if any. The subjects were examined for three categories of symptoms:
Cognitive or intellectual,
Functional, and
Psychiatric or behavioral.
An individual was to be confirmed as a case of dementia only after clinical evaluation. The clinical evaluation also meant a revisit to the cognitive screen scores by the clinical team and wherever a difference in scores between the field investigator and the clinical team was noticed, the score by the clinical team was taken as final.
Statistical analysis
The results have been expressed as percentages and analyzed using Statistical Package for Social Sciences (SPSS) 11.5 and chi-square test was used to find out statistical significance.
Results
A detail of the sociodemographic profile of study population has been provided in Table 1. It is seen that majority of the study population (37.3%) were young elderly in 60-64 years age group. A very high percentage (82.8%) was from joint family with 6.50 ± 3.38 as the number of family members. A majority (57.8%) of study population was illiterate. Out of 2,000; 1,348 individuals were currently married. A substantial number (31.7%) from the study population had lost his/her spouse. Table 2 shows the distribution of study subjects according to age groups among different study populations. It is seen that highest number of individuals above 80 years of age is found in tribal population (78/500) followed by rural population (62/500). Population above 80 years in migrant and urban population was almost similar (50/500 in migrant and 49/500 in rural). Table 3 provides details on the education status of the study population. It is seen that majority (440/500) individuals in tribal area were illiterate. This was followed by migrant and rural elderly (migrant 373/500 and 254/500 rural). The least number of elderly illiterates (89/500) was found in urban population. Table 4 shows the distribution of study subjects according to scores on cognitive screen. A total of 32/2,000 (1.6%) elderly individuals were classified as demented after clinical evaluation giving us an overall dementia prevalence of 1.6%. Out of these 32, seven individuals reported with a score of less than 17. It is seen that 16/500 (3.2%) of urban elderly scored less than 24.5 individuals out of these 16 scored less than 17 on cognitive screen. 7/500 (1.4%) of rural elderly reported a score of less than 24. No individual above 60 years of age from the rural area reported a score of less than 17. Similarly, 9/500 (1.8%) of elders reported a score of less than 24 from migrant population. Two out of these nine reported a score less than 17. No case of dementia was reported from tribal population. A look at sex differential reveals that majority (21/32; 66%) of individuals identified as demented were females.
Table 1.
Sociodemographic profile of study population
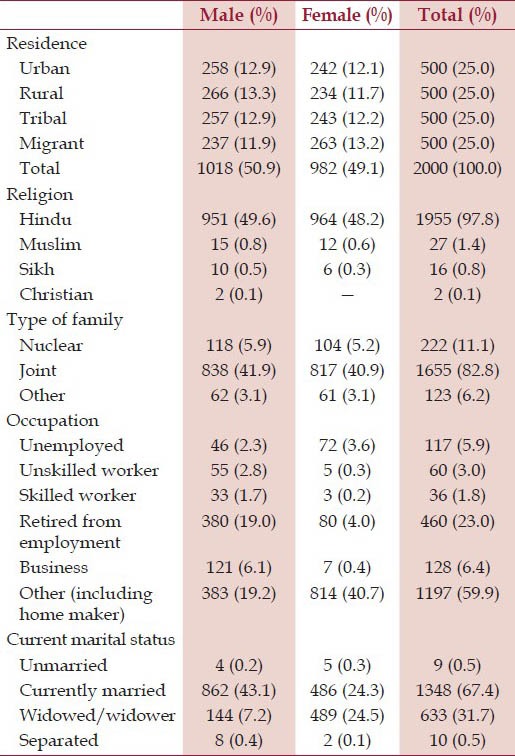
Table 2.
Distribution of study subjects according to age among different study populations
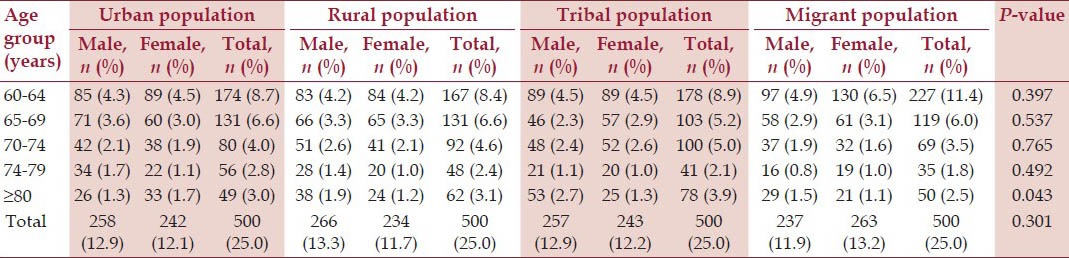
Table 3.
Distribution of study subjects according to education status among different study populations
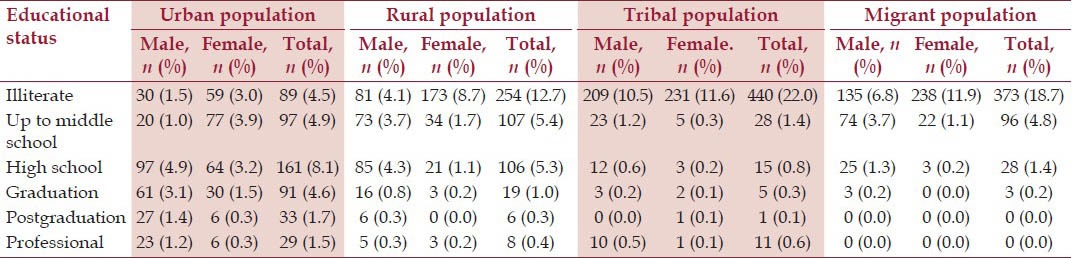
Table 4.
Distribution of study subjects according to cognitive screen among different study populations

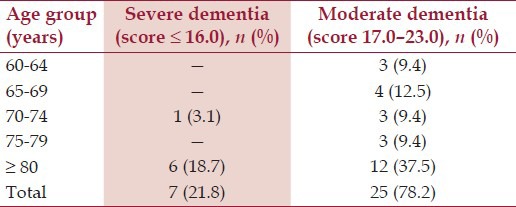
As age advanced scores on cognitive screen decreased with elders above 80 years of age showing lowest scores. 18/32 (56%) of patients classified as demented were more than 80 years of age [Table 5].
Table 5.
Distribution of study subjects according to cognitive screen among different age groups
Discussion
Dementia is characterized by loss of or decline in memory and other cognitive abilities and reduces the lifespan of affected people.[2,11] In 2005, it was estimated that 24.3 million people worldwide and 1.8 million people in India are affected with dementia.[2] In India, the number of people with Alzheimer's disease and other dementias is increasing every year because of the steady growth in the older population and stable increment in life expectancy and it is expected to increase two-fold by 2030 and three-fold by 2050.[2] Dementia is often associated with physical, mental, and financial burden and evidence suggests that elderly people with dementia in developing countries do not often utilize healthcare services, and when they do, the healthcare system is often ill-prepared to provide quality services for dementia.[12] Around 10-37% of the elderly population with dementia in developing countries are classified as having potentially vulnerable living circumstances requiring long-term and specialized care.[13] 93.1 million older people over 60 years of age, globally were estimated to be living with dementia; an overall prevalence of 1.6%.[11] The Delphi consensus estimated that in India, 3.7 million people aged over 60 have dementia.[2]
The data obtained from present study reveals an overall prevalence rate of 1.6% for dementia among elderly individuals 60 years and above. Several community-based urban and rural studies on dementia from different parts of India have documented rates varying from 1.02 to 3.36% above 60-65 years of age.[3,4,5,6,7,8] Our study therefore is reflective of the trend in prevalence rates observed across India. However, these rates are comparatively less in comparison to higher prevalence of dementia in developed countries, which ranges between 5 and 10% after 60-65 years of age.[14]
In last few decades, with demographic ageing proceeding rapidly in all regions worldwide, interest began to focus on prevalence of dementia in low- and middle-income countries (LMIC).[15] This primarily because of the fact that two-thirds of all people aged 65 years and older were living in LMIC, with rapid increase predicted.[16] Two studies funded by the National Institute of Ageing—the US-Nigeria study[17] and the Indo-US study[3]—suggested an age-specific prevalence of dementia that was only between a quarter and a fifth of that typically recorded in developed countries. Therefore, there appeared to be a clear cut divide in the prevalence of dementia between high- and low-income countries.
A population-based, cross-sectional survey conducted in Latin America, India, and China have arrived at crude prevalence rate ranging from 0.8% in rural India to 4.6% in urban Latin America.[15] The prevalence in urban India was 0.9%; while in China, it was 2.4% in rural and 3% in urban areas.[15] The same study compared its estimates with that of pooled estimates from EURODEM meta-analysis. The comparison revealed that the prevalence in urban Latin American sites was about four-fifths of that in Europe, in the Chinese sites it was just over half, and that in rural Latin American and Indian sites only between a quarter and a fifth.[15] As per a study conducted in North India, diabetes, depression, hyperhomocysteinemia, hyperlipidemia, APOE ε4 gene, body mass index (BMI), use of saturated fatty acids, pickles in diet, urban living, and lack of exercise were associated with independent risk of dementia.[18] The fact that India still remains a predominantly rural nation, with 75% of population living in rural areas may be a factor responsible for lower prevalence of dementia. This factor is substantiated by the fact that dementia is more common in urban India as compared to rural India.
But is dementia uniformly distributed across a LMIC like India? Wide community-based studies point to the contrary. Further in 2007 and 2008, studies were conducted on ethnic Kashmiris settled in Jammu district of J&K, after their migration from Kashmir in 1990 in the wake of militancy related conflict in Kashmir region of J&K.[19,20] These studies revealed dementia in a substantial number of the migrant Kashmiri Pandits. However, dementia appeared to be very rare in the native Kashmiri population as per an earlier study conducted in 1986 in Kashmir valley, prior to the onset of militancy.[21] In 2010, a study conducted among two population groups (ethnically different) living within the same geographical region of north India revealed a significant difference in prevalence of dementia among individuals aged 60 years and above.[22]
The present study reveals similar findings with a wide variation in prevalence of dementia among different population groups studied. Interestingly as per our study, dementia appears to be rare in tribal elderly. This despite the fact that elders above 80 years of age (age group which contributes the most to overall prevalence of dementia) are in highest numbers in the tribal population group in our study. This probably points to the fact that age per se is not the only cause of dementia. This point is further highlighted by the fact dementia is much more common in urban (with the least number of elderly above 80 years of age) and migrant population in comparison to rural population. The fact that urban areas record higher prevalence of dementia than rural population is in agreement with earlier studies conducted across India.[3,4,5,6,7,8]
What exactly accounts for this differential distribution of dementia across populations? Adverse social outcomes such as social disengagement, differences in lifestyle, differences in life expectancy, differences in health awareness and healthcare delivery systems, differences in geographical distribution of cerebrovascular disease risk factors, genetic and environmental differences, and nutritional status may be the factors contributing to this difference. The presence of variety of foods like barley, wheat, maize, and phulan as staple foods in tribal area as compared to largely wheat- and rice-dependent populations in rural and urban India may also be a factor. The fact that the prevalence of dementia increases steadily with age and higher prevalence is seen among older women than men explains the effect of difference in life expectancy as a cause for differential distribution.
Probably the missing link in dementia research is on minimum understanding on the cause for differential prevalence of dementia across populations. In this there seems to be little understanding of the environmental and lifestyle factors linked to dementias. Prevalence and incidence of AD seems to be much lower in some developing regions like India. Further prevalence of dementia appears to be lower in less urbanized areas in India. Therefore, it appears that some environmental risk factors are much less prevalent in these settings in comparison to developed and urbanized areas.
Limitations
In spite of care to be methodologically accurate, we may have missed on some individuals suffering from cognitive impairment. This could be because of a relatively smaller sample studied. A larger study sample than the one used in this study may have been useful in providing us with a better understanding on the prevalence of dementia. This could also be the reason for our inability to find a single case of dementia from tribal area. Also, the fact that the study in tribal area was conducted on transhumant agro-pastoralists, wherein a caregiver is more likely than not to carry a patient of dementia with him and therefore may not be found at Bharmour.
Conclusions
To date, most of the research on dementia has been carried out in high-income countries and research on dementia is restricted to few centers in India. This study captures the prevalence of dementia in tribal, rural, migrant, and urban population simultaneously. The findings from this study will open up opportunities in our health system and start service innovation to increase the efficiency and effectiveness of care for patients with dementia in our settings.
Recommendations
There is an urgent need to improve the awareness and understanding of dementia across all levels of society as a step towards improving the quality of life of people with dementia and their caregivers. Awareness raising campaigns relevant to context and audience should be developed in consultation with people with dementia, their families, and other stakeholders.
Footnotes
Source of Support: Indian Council of Medical Research (ICMR)
Conflict of Interest: None declared.
References
- 1.Census of India. Govt. of India, Ministry of home affairs, office of the registrar general and census commissioner, India. [Accessed January 6, 2014]. at http://www.who.int/healthinfo/statistics/bod_dementia.pdf .
- 2.Ferri CP, Prince M, Brayne C, Brodaty H, Fratiglioni L, Ganguli M, et al. Global prevalence of dementia: A Delphi consensus study. Lancet. 2005;366:2112–7. doi: 10.1016/S0140-6736(05)67889-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Chandra, Ganguli M, Pandav R, Johnston J, Belle S, DeKosky ST. Prevalence of Alzheimer's disease and other dementias in rural India: the Indo-US study. Neurology. 1998;51:1000–8. doi: 10.1212/wnl.51.4.1000. [DOI] [PubMed] [Google Scholar]
- 4.Shaji I, Promodu K, Abraham T, Roy KJ, Verghese A. An epidemiological study of dementia in a rural community in Kerala, India. Br J Psychiatry. 1996;168:745–9. doi: 10.1192/bjp.168.6.745. [DOI] [PubMed] [Google Scholar]
- 5.Bharucha NE, Bharucha EP, Bharucha AE, Bhise AV, Schoenberg BS. Prevalence of Parkinsons's disease in the Parsi community of Bombay, India. Arch Neurol. 1988;45:1321–3. doi: 10.1001/archneur.1988.00520360039008. [DOI] [PubMed] [Google Scholar]
- 6.Rajkumar S, Kumar S, Thara R. Prevalence of dementia in a rural setting: A report from India. Int J Geriatr Psychiatry. 1997;12:702–7. doi: 10.1002/(sici)1099-1166(199707)12:7<702::aid-gps489>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- 7.Rajkumar S, Kumar S. Prevalence of dementia in the community: A rural-urban comparison from Madras, India. Aust J Aging. 1996;15:9–13. [Google Scholar]
- 8.Shaji I, Bose S, Verghese A. Prevalence of dementia in an urban population in Kerala, India. Br J Psychiatry. 2005;186:136–40. doi: 10.1192/bjp.186.2.136. [DOI] [PubMed] [Google Scholar]
- 9.Lobo A, Launer LJ, Fratiglioni L, Anderson K, Di Carlo A, Breteler MM, et al. Prevalence of dementia and major subtypes in Europe: A collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000;54:S4–9. [PubMed] [Google Scholar]
- 10.Raina SK, Raina S, Chander V, Grover A, Singh S, Bhardwaj A. Development of a cognitive screening instrument for tribal elderly population of Himalayan region in Northern India. J Neurosci Rural Pract. 2013;4:147–53. doi: 10.4103/0976-3147.112744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mathers C, Matilde Leonardi. Global burden of dementia in the year 2000. Summary of methods and data sources. World Health Organization. [Accessed January 6, 2014]. at: http://www.who.int/healthinfo/statistics/bod_dementia.pdf .
- 12.Dias A, Patel V. Closing the treatment gap for dementia in India. Indian J Psychiatry. 2009;51(Suppl 1):S93–7. [PMC free article] [PubMed] [Google Scholar]
- 13.Prince MJ. The 10/66 dementia research group - 10 years on. Indian J Psychiatry. 2009;51(Suppl 1):S8–15. [PMC free article] [PubMed] [Google Scholar]
- 14.Canadian study of health and ageing: Study methods and prevalence of dementia. Can Med Assoc J. 1994;150:899–13. [PMC free article] [PubMed] [Google Scholar]
- 15.Llibre Rodriguez JJ, Ferri CP, Aco;sta D, Guerra M, Huang Y, Jacob KS, et al. 10/66 Dementia Research Group. Prevalence of dementia in Latin America, India, and China: A population -based cross- sectional survey. Lancet. 2008;372:464–74. doi: 10.1016/S0140-6736(08)61002-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Prince M. The need for research on dementia in developing countries. Trop Med Int Health. 1997;2:993–1000. doi: 10.1046/j.1365-3156.1997.d01-156.x. [DOI] [PubMed] [Google Scholar]
- 17.Hendrie HC, Osuntokun BO, Hall KS, Ogunniyi AO, Hui SL, Unverzagt FW, et al. Prevalence of Alzheimer's disease and dementia in two communities: Nigerian Africans and African Americans. Am J Psychiatry. 1995;152:1485–92. doi: 10.1176/ajp.152.10.1485. [DOI] [PubMed] [Google Scholar]
- 18.Tripathi M, Vibha D, Gupta P, Bhatia R, Srivastava MV, Vivekanandhan S, et al. Risk factors of dementia in North India: A case-control study. Aging Ment Health. 2012;16:228–35. doi: 10.1080/13607863.2011.583632. [DOI] [PubMed] [Google Scholar]
- 19.Raina S, Razdan S, Pandita KK, Raina S. Prevalence of dementia among Kashmiri migrants. Ann Indian Acad Neurol. 2008;11:106–8. doi: 10.4103/0972-2327.41878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Raina SK, Pandita KK, Razdan S. Incidence of dementia among Kashmiri migrants. Ann Indian Acad Neurol. 2009;12:154–6. doi: 10.4103/0972-2327.56313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Razdan S, Koul RL, Motta A, Koul S, Bhatt RK. Prevalence and pattern of major neurological disorders in rural Kashmir(India) in 1986. Neuroepidemiology. 1994;13:113–9. doi: 10.1159/000110368. [DOI] [PubMed] [Google Scholar]
- 22.Raina S, Razdan S, Pandita KK. Prevalence of dementia in ethnic Dogra population of Jammu district - A comparison survey. Neurol Asia. 2010;15:65–9. [Google Scholar]