

Abstract
Purpose
Adult intussusception is uncommon, but an organic lesion is found to be the lead point in 75% to 90% of the cases. This study was designed to review our experience with adult intussusception and to determine if there are any preoperative predictive factors for a malignant lead point.
Methods
Thirty-three patients over 15 years of age were diagnosed with intussusceptions through operative finding over a period of 20 years. We reviewed the medical records of these patients retrospectively, and preoperative predictive factors of malignant lead points were analyzed.
Results
The preoperative diagnosis of intussusception had been made correctly in 86% of the cases, and computed tomography could find a lead point in 79%. A causative organic lesion was found in 29 patients (88%) pathologically; 16 cases (48%) were due to benign tumors, and 13 (39%) were due to malignant tumors. A malignant lead point was present in four of 21 enteric (20%) versus nine of 13 colonic intussusceptions (75%). The period from symptom appearance to hospital visit showed a more chronic nature in malignant neoplasm than in benign neoplasm (P = 0.006), and the location of causative organic lesion showed significant difference between benign and malignant groups (P = 0.003).
Conclusion
Adult intussusceptions are commonly secondary to a pathologic lead point, and a computed tomography is an effective diagnostic tool for finding a lead point preoperatively. The chronic nature of the disease presentation and colonic location of the lead point may suggest a malignant neoplasm.
Keywords: Adult intussusception, Predictive factors, Malignant lead point
INTRODUCTION
Intussusception is defined as a condition where a segment of bowel is telescoping inside the adjacent intestinal segment. Also, it is known as an important cause of acute intestinal obstruction in infants under 2 years of age. However, intussusception in adults is unusual, contributing to only 5% of all intussusception and 1%-5% of all cases of intestinal obstructions [1,2,3]. The causes of intussusception are rarely identified in infants, but in adults, 75%-90% of the cases have a causative factor in which a malignant neoplasm constitutes 65%-70% of intussusception in the large intestine, and 30% in the small intestine [2,3,4,5,6]. Diagnosis is not easy due to the chronic nature and nonspecific symptoms. However, abdominal sonography and computed tomography make preoperative diagnosis possible. Surgical resection is widely accepted as treatment of choice for intussusception in adults, but the range of resection and the necessity of manual reduction is still in dispute depending on the nature of the primary lesion [1,3,5]. The authors investigated the clinical symptoms, diagnostic methods, and pathologic characteristics of adult intussusception in attempts to understand the precise methods of preoperative diagnosis and the predictive factors of the malignant lead point.
METHODS
We reviewed a total of 33 patients over the age of 15 who were diagnosed for intussusception and had undergone surgery between December 1994 and April 2013. The study was done retrospectively, based on medical records of age and sex, clinical symptoms and signs, duration of symptoms and length of hospital stay, diagnostic method, clinical type and cause of intussusception, and surgical methods. A chi-square test was used for analysis of categorical variables, and an independent t-test was used to perform univariate analysis for continuous variables. All analysis was done through PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered significant on the basis of two-sided tests.
RESULTS
Age and sex
Among total of 33 cases, 17 (52%) were female. The mean age was 57 years old, and the distribution was from 15 to 92 years of age.
Clinical symptoms and signs
Patients presenting intermittent abdominal pain and abdominal discomfort were most common, found in 30 cases (90%), followed by tenderness, rebound tenderness, nausea/vomiting, hematochezia, diarrhea and constipation. There was one case (3%) where the patient was asymptomatic in which the intussusception was diagnosed incidentally during check up colonoscopy and was found to be caused by cecal cancer. The period from appearance of symptom to hospital visit was less than seven days in 18 cases (55%), 8-14 days in two cases (6%), 15-90 days in seven cases (21%), and over 90 days in five cases (15%).
Diagnostic methods
Preoperative diagnosis of the intussusception was made in 28 cases (85%) whereas the remaining five cases (15%) were diagnosed with mechanical bowel obstruction. Computed tomography was performed in 29 cases, and in 25 cases (86%) the correct diagnosis was made for intussusception. Also, the lead point was found in 23 cases, and it was confirmed by surgery in 22 cases, accounting for a sensitivity of 95% and specificity of 75%.
Types of intussusception
We classified the intussusceptions into small-intestine type, ileocecal type, ileocolic type, and colocolic type according to the anatomical location. The small-intestine type was divided again into jejunojejunal type and ileoileal type. Based on our classification, small-intestine type was found in 19 cases (58%), jejunojejunal type in 10 cases (30%), ileoileal type in nine cases (28%), ileocecal type in one case (3%), ileocolic type in three cases (9%), and colocolic type in 10 cases (30%), respectively.
Location and pathology of the primary lesion
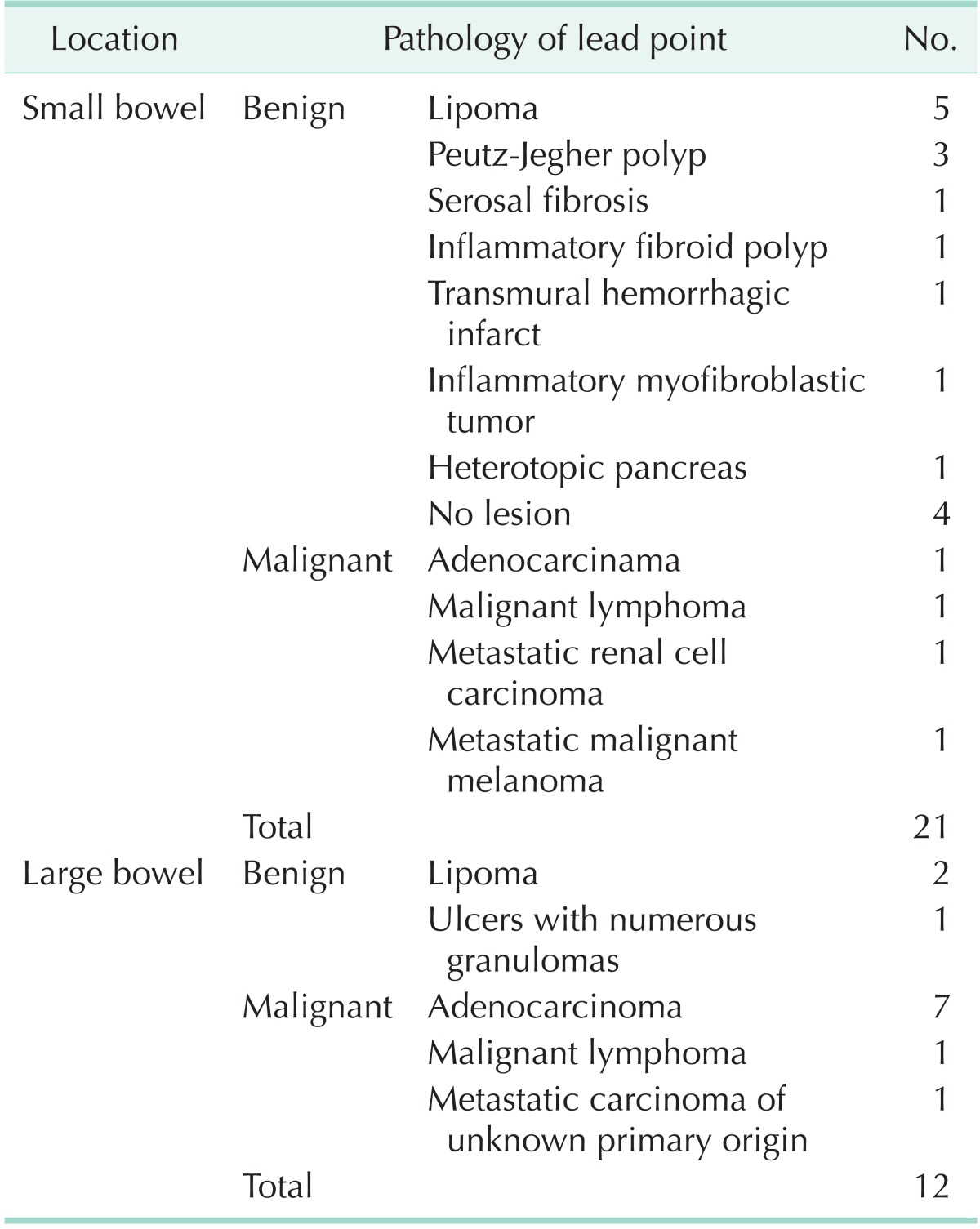
The primary lesion was found to be a neoplasm in 29 out of 33 cases (88%). The neoplasm was located in the small intestine in 17 cases (52%), and in the colon in 12 cases (36%). Out of 21 cases where a neoplasm was found in the small intestine, 17 cases (80%) were benign and four cases (20%) were malignant. A benign neoplasm of the colon was found in three cases (25%), and a malignant neoplasm was found in nine cases (75%) (Table 1).
Table 1.
Etiology of intussusception
Treatment
The hospital stay of the patients was of 5 to 38 days. Fifteen cases of small-intestinal type intussusception were treated with resection and anastomosis, and polypectomy and tumorectomy were performed in one case each. Only manual reduction was performed in two cases. A manual reduction was performed before the resection in six out of the 15 cases of resection and anastomosis. In all cases of ileocecal type and ileocolic type, and in six out of 10 cases of the colocolic type, right hemicolectomy was performed. For the rest, low anterior resection, Hartmann's operation, transverse colectomy, and right hemicolectomy were performed.
Analysis of predictive factors
In order to analyze the preoperative predictive factors of a malignant lead point, we divided patients into benign and malignant groups through postoperative pathologic diagnosis. Age, sex, anemia, and obstruction symptoms did not show a significant difference. However, the period from symptom appearance to hospital visit (acute, less than 14 days; chronic, over 14 days) showed a more chronic nature in the malignant neoplasm than in the benign neoplasm (P = 0.006), and neoplasms found in the colon showed statistically significant higher rates of malignancy (P = 0.003) (Table 2).
Table 2.
Predictive factors of malignant lead point
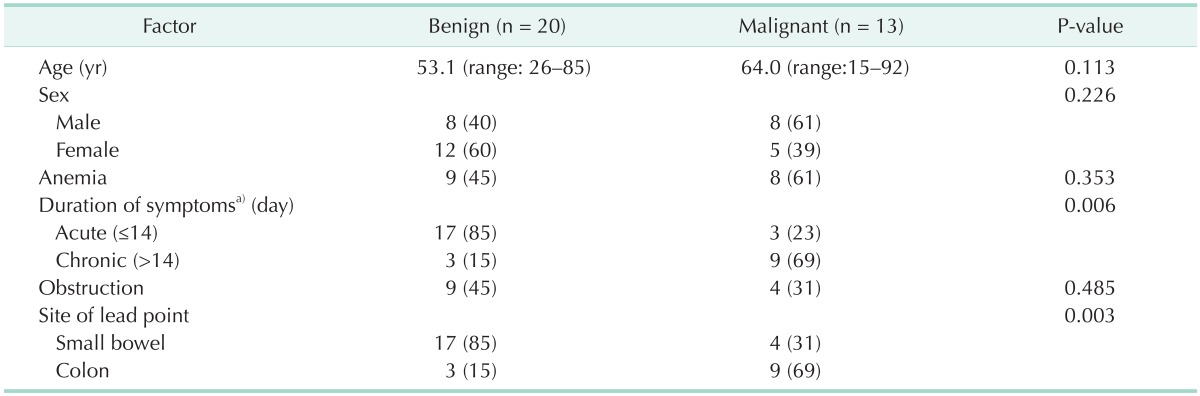
Values are presented as median (range) or number (%).
a)One case was excluded because it was found by colonoscopy incidentally.
DISCUSSION
Intussusception in infants usually presents an acute nature along with characteristic features such as intermittent abdominal pain, abdominal mass and currant jelly stool. However, adult intussusception rarely shows these characteristic symptoms, but instead tends to have a chronic nature and shows nonspecific symptoms related to partial intestinal obstruction. With respect to symptoms, intermittent abdominal pain was most common, followed by nausea/vomiting, and it was reported that hematochezia accounted for 8 to 26% [5,6,7,8]. Also, in our study, abdominal pain was the most common symptom, present in 30 cases (90%), followed by nausea/vomiting in nine cases (27%), and hematochezia in five cases (16%). There was one case (3%) where the patient was asymptomatic in which the intussusception was diagnosed incidentally during check up. The diameter of the adult intestine is larger than that in infants. Therefore, the majority of the cases tended to show chronic progression rather than acute symptoms of total intestinal obstruction. However, Erkan et al. [9] reported increasing cases of patients presenting acute symptoms compared to the past, and we also experienced 20 cases (61%) where the patients visited the hospital sooner than 14 days after the emergence of first symptom.
Radiologic examination is usually needed for diagnosis of intussusception. Abdominal ultrasonography and computed tomography are commonly used to visualize the intussuscepted mass, bowel wall edema, mesentery inside the hollow viscus, target-sign, and the sausage-shaped appearance which are diagnostic features of intussusception. Recent developments of technology improved the sensitivity and specificity of the diagnostic tools. This helps to locate and measure the size of the lead point before going into surgery. Along with increase in use of computed tomography, reports are increasing of nonsymptomatic intussusception and small intestinal intussusception without lead points, arousing controversy in whether or not surgical intervention is needed for these patients. However, there is no dispute on the need of surgical treatment for intussusception with the lead point [10,11,12,13,14]. In our study, five out of nine ultrasonographic exams and 25 out of 29 computed tomographic exams diagnosed intussusception preoperatively, and the lead point was identified in 23 cases with successful diagnosis in 22 cases confirmed after surgery. Computed tomography is not only a fitting tool for diagnosing intussusception, but also for identifying the presence of the lead point.
Neoplasm is a major cause of intussusception with other factors such as inflammatory bowel disease, postoperative adhesion, and Mekel's diverticulum. Out of 54%-85% of the neoplasms reported, malignant neoplasm accounts for 20%-50%. Neoplasms found in the small intestine are mostly benign, but large intestinal neoplasms are more frequently malignant. Many cases of malignant neoplasms found in the small intestine are of a metastatic neoplasm. Malignant neoplasm in the large intestine are reported to be 63%-68%, and the most common cause is adenocarcinoma [1,5,7,8,15,16,17,18,19]. In our study, 29 cases (88%) were of a neoplasm, and 13 cases (39%) turned out to be malignant. A malignant neoplasm was found in four out of 17 cases (24%) with lead point in the small intestine while nine out of 12 neoplasms (75%) were malignant in the colonic location of the lead point.
Preoperative diagnosis is very important in determining the therapeutic plan and in predicting the prognosis. Diagnosis of the lead point is crucial in deciding the optimal management also. Thus, preoperative discrimination of the malignancy is very helpful in choosing a future course of management. Many cases of pathologic lead points in large bowel intussusceptions are already known to be malignant lesions. Also, Goh et al. [16] reported that a malignancy may be attributed to an increased propensity for bleeding in the site of malignancy; 32% with malignant pathology versus 16% with benign pathology had rectal bleeding or melena or presence of anemia due to chronic disease in patients with cancer [18,20]. In our study, we could not confirm age and anemia as preoperative predictive factors of a malignant lead point. However, a pathologic lead point of the large bowel (P = 0.003) and a chronic nature of symptoms (P = 0.006) were predictive factors for the malignancy, and it was statistically significant. Therefore, a malignancy should be considered in adult intussusception patients who were found with a lead point in the large bowel and who have a chronic nature of the symptoms.
There is still controversy concerning the treatment of adult intussusceptions, but since most cases occur as a secondary result, we insist that surgical bowel resection be needed. However, recent reports claim that conservative observation may be sufficient for intussusception without a lead point. If an evident cause for intussusception exists, surgical bowel resection must be considered. However, since small-intestinal intussusception is mostly benign in cause, manual reduction could be considered, but large intestinal intussusception is mostly caused by malignant neoplasms so bowel resection without manual reduction should be a prior option [3,5,6,7,8,10,11,12,13,14,15,16,19]. Manual reduction minimizes bowel resection which can prevent short bowel syndrome, but excessive attempts should be avoided in order to prevent bowel perforation or bowel edema. In our study, 29 cases (88%) of bowel resection were performed, and two cases (6%) were treated only with manual reduction.
In conclusion, most adult intussusceptions are secondary to a causative factor. Computed tomography is an effective tool in diagnosing intussusception and locating the lead point. A chronic nature of disease presentation and colonic location of lead point may suggest the presence of a malignant neoplasm.
ACKNOWLEDGEMENTS
The present research was conducted by the research fund of Dankook University in 2013.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Azar T, Berger DL. Adult intussusception. Ann Surg. 1997;226:134–138. doi: 10.1097/00000658-199708000-00003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Donhauser JL, Kelly EC. Intussusception in the adult. Am J Surg. 1950;79:673–677. doi: 10.1016/0002-9610(50)90333-3. [DOI] [PubMed] [Google Scholar]
- 3.Begos DG, Sandor A, Modlin IM. The diagnosis and management of adult intussusception. Am J Surg. 1997;173:88–94. doi: 10.1016/S0002-9610(96)00419-9. [DOI] [PubMed] [Google Scholar]
- 4.Reijnen HA, Joosten HJ, de Boer HH. Diagnosis and treatment of adult intussusception. Am J Surg. 1989;158:25–28. doi: 10.1016/0002-9610(89)90309-7. [DOI] [PubMed] [Google Scholar]
- 5.Weilbaecher D, Bolin JA, Hearn D, Ogden W., 2nd Intussusception in adults. Review of 160 cases. Am J Surg. 1971;121:531–535. doi: 10.1016/0002-9610(71)90133-4. [DOI] [PubMed] [Google Scholar]
- 6.Akçay MN, Polat M, Cadirci M, Gencer B. Tumor-induced ileo-ileal invagination in adults. Am Surg. 1994;60:980–981. [PubMed] [Google Scholar]
- 7.Wang N, Cui XY, Liu Y, Long J, Xu YH, Guo RX, et al. Adult intussusception: a retrospective review of 41 cases. World J Gastroenterol. 2009;15:3303–3308. doi: 10.3748/wjg.15.3303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chang CC, Chen YY, Chen YF, Lin CN, Yen HH, Lou HY. Adult intussusception in Asians: clinical presentations, diagnosis, and treatment. J Gastroenterol Hepatol. 2007;22:1767–1771. doi: 10.1111/j.1440-1746.2007.04907.x. [DOI] [PubMed] [Google Scholar]
- 9.Erkan N, Haciyanli M, Yildirim M, Sayhan H, Vardar E, Polat AF. Intussusception in adults: an unusual and challenging condition for surgeons. Int J Colorectal Dis. 2005;20:452–456. doi: 10.1007/s00384-004-0713-2. [DOI] [PubMed] [Google Scholar]
- 10.Tresoldi S, Kim YH, Blake MA, Harisinghani MG, Hahn PF, Baker SP, et al. Adult intestinal intussusception: can abdominal MDCT distinguish an intussusception caused by a lead point? Abdom Imaging. 2008;33:582–588. doi: 10.1007/s00261-007-9328-8. [DOI] [PubMed] [Google Scholar]
- 11.Sundaram B, Miller CN, Cohan RH, Schipper MJ, Francis IR. Can CT features be used to diagnose surgical adult bowel intussusceptions? AJR Am J Roentgenol. 2009;193:471–478. doi: 10.2214/AJR.08.1801. [DOI] [PubMed] [Google Scholar]
- 12.Olasky J, Moazzez A, Barrera K, Clarke T, Shriki J, Sohn HJ, et al. In the era of routine use of CT scan for acute abdominal pain, should all adults with small bowel intussusception undergo surgery? Am Surg. 2009;75:958–961. [PubMed] [Google Scholar]
- 13.Onkendi EO, Grotz TE, Murray JA, Donohue JH. Adult intussusception in the last 25 years of modern imaging: is surgery still indicated? J Gastrointest Surg. 2011;15:1699–1705. doi: 10.1007/s11605-011-1609-4. [DOI] [PubMed] [Google Scholar]
- 14.Rea JD, Lockhart ME, Yarbrough DE, Leeth RR, Bledsoe SE, Clements RH. Approach to management of intussusception in adults: a new paradigm in the computed tomography era. Am Surg. 2007;73:1098–1105. [PubMed] [Google Scholar]
- 15.Yang JD, Lee MR, Kim JH. Adult Intussusception: diagnosis and treatment. J Korean Soc Coloproctol. 2007;23:416–419. [Google Scholar]
- 16.Goh BK, Quah HM, Chow PK, Tan KY, Tay KH, Eu KW, et al. Predictive factors of malignancy in adults with intussusception. World J Surg. 2006;30:1300–1304. doi: 10.1007/s00268-005-0491-1. [DOI] [PubMed] [Google Scholar]
- 17.Kim SJ, Park CH, Kim YM, Kim SY, Chun SY, Kwon CW, et al. A clinical review of the intussusception in adult. Intest Res. 2012;10:183–188. [Google Scholar]
- 18.Kim KH, Lee IK, Lee YS, Kim DH, Park JK, An CH, et al. Analysis of the diagnostic maneuver and timing of operation in adult intussusception. J Korean Surg Soc. 2007;73:419–423. [Google Scholar]
- 19.Yun SO, Namgung H, Lee CH, Park DG. Intussusception in adults. J Korean Soc Coloproctol. 2004;20:199–204. [Google Scholar]
- 20.Marinis A, Yiallourou A, Samanides L, Dafnios N, Anastasopoulos G, Vassiliou I, et al. Intussusception of the bowel in adults: a review. World J Gastroenterol. 2009;15:407–411. doi: 10.3748/wjg.15.407. [DOI] [PMC free article] [PubMed] [Google Scholar]