

Abstract
This study aimed to analyze the patterns of antipsychotic prescription to patients with schizophrenia in Korea. Using the Health Insurance Review & Assessment Service-National Patients Sample (HIRA-NPS), which was a stratified sampling from the entire population under the Korean national health security system (2009), descriptive statistics for the patterns of the monopharmacy and polypharmacy, neuropsychiatric co-medications, and prescribed individual antipsychotic for patients with schizophrenia were performed. Comparisons of socioeconomic and clinical factors were performed among patients prescribed only with first- and second-generation antipsychotics. Of 126,961 patients with schizophrenia (age 18-80 yr), 13,369 were prescribed with antipsychotic monopharmacy and the rest 113,592 with polypharmacy. Two or more antipsychotics were prescribed to 31.34% of the patients. Antiparkinson medications (66.60%), anxiolytics (65.42%), mood stabilizers (36.74%), and antidepressants (25.90%) were co-medicated. Patients who were prescribed only with first-generation antipsychotics (n=26,254) were characterized by significantly older age, greater proportion of male, higher proportion of medicaid, higher total medical cost, lower self-payment cost, and higher co-medication rates of antiparkinson agents and anxiolytics than those who were prescribed only with second-generation antipsychotics (n=67,361). In this study, it has been reported substantial prescription rates of first-generation antipsychotics and antipsychotic polypharmacy and relatively small prescription rate of clozapine to patients with schizophrenia. Since this study has firstly presented the patterns of antipsychotic prescription to schizophrenic patients in Korean national population, the findings of this study can be compared with those of later investigations about this theme.
Graphical Abstract
Keywords: Schizophrenia, Antipsychotics, Prescribing Patterns, Korea
INTRODUCTION
Antipsychotic medications have been the main therapeutic approaches for schizophrenia, and their diversity can represent the current options of antipsychotic therapies. Since chlorpromazine had been introduced to psychiatric realms in the 1950s, haloperidol, loxapine, perphenazine, molindone and other first-generation antipsychotics followed chlorpromazine in the 1960s. However, first-generation antipsychotics have resulted in several adverse effects including tardive dyskinesia, and less therapeutic effects on the negative symptoms and cognitive deficits of schizophrenia. Clozapine, which was produced as the first atypical antipsychotics in 1971 and consigned into oblivion because of occurrence of agranulocyotsis, was reintroduced in 1989.Moreover, development of second-generation antipsychotics have been followed in the 1990s (risperidone, olanzapine, quetiapine and ziprasidone) and the 2000s (aripiprazole and paliperidone) (1, 2). Superior efficacy and effectiveness of second-generation antipsychotics compared with first-generation antipsychotics have been consistently demonstrated. However, costs of second-generation antipsychotics have been 10 times more than those of first-generation antipsychotics. These cost differences have been one of contributors to relatively low prescription of antipsychotics in some countries. Moreover, the mental health system, traditional medicines, clinicians or patients' preferences, overall socioeconomic or cultural underpinnings and other factors have also influenced the patterns of antipsychotic prescription to patients with schizophrenia (3).
Because the clinical trials for second-generation antipsychotics have been usually designed by a form of case-control study, the pharmacological treatment algorithms for schizophrenia are needed to apply the findings of clinical trials to clinical practices and maximize cost-effectiveness for pharmacological treatment. In a similar vein, the Korean Medication Algorithm for schizophrenia was firstly published in 2001 and revised in 2006 (4, 5). Although many clinical practice guidelines for schizophrenia have been published in many countries or organizations, there have been usually discrepancies between the guideline statement and prescription patterns in clinical practice. Hence, the investigations for the patterns of antipsychotic prescription to patients with schizophrenia in Korea can reveal the overall prescribing patterns and evaluate the degree of implementation to pharmacological treatment guideline for schizophrenia. Sometimes, the findings from the data of university-affiliated hospitals were presented in Korea. Kwon et al. (1) reported that, of the 825 schizophrenic outpatients with 862 total antipsychotic prescriptions at a university-affiliated hospital, 88.1% were prescribed with second-generation antipsychotics, risperidone was most frequently prescribed (39.0%). Choi et al. (6) presented that, of the 467 schizophrenic inpatients at a university-affiliated hospital from 2001 to 2008, 56.1% were discharged with a polypharmacy regimen and the prescribing rate of antipsychotic polypharmacy was significantly increased with passage of time. In addition, Shim et al. (7) presented that, of schizophrenic inpatients at a university-affiliated hospital, the prescription of second-generation antipsychotics represented a significant proportional increase of 2009-2010 over 2003-2004 and 1997. These trends of antipsychotic prescription patterns could correspond to the first and revised editions of Korean Medication Algorithm for schizophrenia. However, the findings from university-affiliated hospitals commonly had a limitation which could not represent the national status in Korea. Moreover, to our knowledge, the patterns of antipsychotic prescription to patients with schizophrenia were rarely studied from the national data of Korea.
The Health Insurance Review & Assessment Service - National Patients Sample (HIRA-NPS) is a stratified sampling from the entire population data under the national health security system in Korea, 2009, and has been developed to increase the feasibility of clinical data of the national health security system for public health research (8, 9). Hence, using the HIRA-NPS which reflect the entire population, we aimed to reveal the patterns of antipsychotic prescription to patients with schizophrenia in Korea. More specifically, this study aimed to answer the following question: 1) How many of patients with schizophrenia in Korea (2009) were prescribed with the monopharmacy and polypharmacy? 2) Which medications were used in the antipsychotic monopharmacy to patients with schizophrenia? 3) Which antipsychotics and neuropsychiatric co-medications were used in the polypharmacy to patients with schizophrenia? What patterns of antipsychotics and neuropsychiatric co-medications prescription to patients with schizophrenia were used? 4) Which socioeconomic and clinical variables were significantly different in a comprehensive comparison among patients prescribed only with first- and second-generation antipsychotics?
MATERIALS AND METHODS
Data and subjects
For analyses of data and subjects, we used the HIRA-NPS (serial number: HIRA-NPS-2009-0082). The HIRA-NPS was a stratified sample, according to sex and age interval of 5 yr, from entire national population (about 46 million persons) which was reflected by the health insurance data of hospitals and clinics under the Korean national health security system in 2009. The HIRA-NPS included all the medical treatment and prescription data for one year (2009) of 700 thousand inpatients and 400 thousand outpatients in Korea. The sample size of HIRA-NPS was estimated by annual total medical cost per a patient, which had maximum variance. Since the margin of error was defined by 0.5% standard deviation of mean annual medical cost per a patient of entire population, the sampling rates of inpatients and outpatients were 13 and 1 percents respectively. Because of an independent design for the stratified sampling, the entire population was estimated by the separated weighting, which was composed of 7.69 times of inpatient samples and 100 times of outpatient samples in the HIRA-NPS. The validity of HIRA-NPS was confirmed from the estimated treated prevalence and hypoglycemic agent use patterns of patients with diabetes mellitus. Prescription-based analyses of the HIRA-NPS revealed significant differences as compared with those of the Korean national population, whereas patient-based analyses of the HIRA-NPS corresponded to those of the Korean national population. Therefore, the patient-based analyses of clinical epidemiological studies in Korea had been often investigated using the HIRA-NPS (8, 9). Hence, using the HIRA-NPS, we conducted the patient-based analyses of the patterns of antipsychotic prescription to schizophrenic patients in Korea.
Using the HIRA-NPS, patients with schizophrenia was operationally defined as following criteria: 1) diagnoses of schizophrenia (F20), paranoid schizophrenia (F20.0), hebephrenic schizophrenia (F20.1), catatonic schizophrenia (F20.2), undifferentiated schizophrenia (F20.3), post-schizophrenic depression (F20.4), residual schizophrenia (F20.5), simple schizophrenia (F20.6), other schizophrenia (F20.8) or schizophrenia, unspecified (F20.9) by the 6th revision of Korean Standard Classification of Diseases (KCD-6) (10) which had been developed with the reference of the 10th version of International Classification (ICD-10) (11), 2) presence of at least once or more antipsychotic prescribing by psychiatrist, and 3) age from 18 to 80 yr. Hence, we excluded schizophrenic patients who were 1) prescribed with antipsychotics by clinicians beyond psychiatrists or Oriental doctors, 2) treated only with non-pharmacological methods including electroconvulsive therapy, and transcranial magnetic stimulation, and 3) age less than 18 or more than 80 yr.
Antipsychotics and neuropsychiatric co-medications
Operational definition was also applied to antipsychotics. Of psychotrophic agents which were listed as the 117 code according to the drug classification of Ministry of Health and Welfare of Korea at 1 July 2013 (12), 25 medications were considered antipsychotics. Hence, the antipsychotic prescribed included following: first-generation antipsychotics such as bromperidol, chlorpromazine, chlorprothixene, haloperidol, levomepromazine, levosulpride, loxapine, melperone, mesoridazine, molindone, nemonapride, perphenazine, pimozide, sulpride, thioridazine, thiothixene, and trifluoperazine; and second-generation antipsychotics such as amisulpride, aripiprazole, blonanserin, olanzapine, paliperidone, quetiapine, risperidone, ziprasidone, and zotepine. The introduction of clozapine in the development history of antipsychotics was a dividing standard into first- and second-generation medications. Aripiprazole has been sometimes regarded as third-generation antipsychotics, as its dopamine-serotonin stabilizing mechanism has been different from other second-generation antipsychotics (13). However, to cover the efficient statistical analysis, aripiprazole was classified as second-generation antipsychotics according to list of Tandon et al. (14) which was approved antipsychotics around the world, 2007.
Neuropsychiatric co-medications were classified into mood stabilizers, antidepressants, anxiolytics and antiparkinson medications. Of anticonvulsants which were listed as the 113 code according to the drug classification of Ministry of Health and Welfare of Korea (12), 27 medications were considered mood stabilizers. And, of psychotrophic agents which were listed as the 117 code according to the drug classification of Ministry of Health and Welfare of Korea (12), 25 medications were considered anxiolytics. Finally, of other central nervous system agents which were listed as the 119 code according to the drug classification of Ministry of Health and Welfare of Korea (12), 7 medications were considered antiparkinson agents.
Index prescription period
Because same prescribing pattern to each patient with schizophrenia is not usually persistent yearly, construction of the 'index prescription period' is needed. We set the 'index prescription period' of each patient with schizophrenia, which was defined by the longest maintenance period of same prescribing pattern including antipsychotics regardless of its dosage chlorpromazine equivalent. If different prescription patterns were maintained for the same duration in different periods of 2009, 'index prescription period' was constructed by the period of latter prescribing pattern. Thus, using the 'index prescription period,' we presented the patterns of antipsychotic prescription to patients with schizophrenia.
Socioeconomic and clinical variables
From health insurance data of the HIRA-NPS, socioeconomic and clinical variables were collected as the following listed variables: age (18-29, 30-39, 40-49, 50-59, 60-60, or 70-80 yr), gender, public insurance scheme (health insurance, medicaid, or veteran healthcare), total medical cost, self-payment cost, insurer-payment cost, subtype (F20, F20.1-F20.9) and treatment type (inpatient, or outpatient). In the HIRA-NPS, inpatient was defined by those who had ever been admitted to hospital in 2009, whereas outpatient was defined by those who had never been hospitalized and were treated only at outpatient clinic.
Polypharmacy, antipsychotic polypharmacy and augmentation
Polypharmacy was defined here as the prescription of 2 or more psychotrophic agents with 'index prescription period.' Antipsychotic polypharmacy was defined as the prescription of 2 or more antipsychotic medications (15). Augmentation strategy was defined as the prescription of another neuropsychiatric co-medications including mood stabilizers, antidepressants, anxiolytics and antiparkinson agents in addition to antipsychotics (16).
Statistical analysis
By separate weightings in- and outpatients of the HIRA-NPS, the weighted values of persons were rounded off of decimal points. The descriptive statistics for frequency and patterns of monopharmacy and polypharmacy, frequency of neuropsychiatric co-medications including mood stabilizers, antidepressants, anxiolytics, and antiparkinson medications, and frequency of antipsychotic prescription to patients with schizophrenia in Korea were presented. A comprehensive comparison of socioeconomic and clinical data was performed among patients prescribed only with first- and second-generation antipsychotics (chi-square test for discrete variables and independent t-test for continuous variables). Significance was set at P<0.01 (two-tailed) for all tests, to reduce familywise error due to multiple comparisons. All statistical analyses were performed using the survey analysis of the Statistical Analysis System (SAS, version 9.1; SAS Institute Inc, Cary, NC, USA).
Ethics statement
This study was approved by the institutional review board of Yong-In Mental Hospital (receipt number: 2013-40). Informed consent was waived by the board.
RESULTS
General characteristics of patients with schizophrenia in Korea, 2009
Socioeconomic and clinical features of 126,961 (standard deviation [SD], 2,330.46) patients with schizophrenia were presented in Table 1. The mean age was 44.08 yr (standard error [SE], 0.27; 95% confidence interval [CI], 43.54-45.00), and about half of subjects were female (51.00%; SE, 1.10), diagnosed as paranoid schizophrenia (F20.0, 48.03%; SE, 1.08), treated as outpatient (54.90%; SE, 0.98), and publically insured as health insurance (58.80%; SE, 1.00). And, the mean total medical cost were USD 3,209 (SE, 63.00; KRW 3,529,823, SE, 68,797.00), the mean self-payment cost USD 279 (SE, 7.00; KRW 306,578; SE, 7,931.00), and the mean insurer-payment cost USD 2,905 (SE, 57.00; KRW 3,195,854; SE, 62,941.00).
Table 1.
General characteristics of patients with schizophrenia (n = 126,961; SD, 2,330.46)
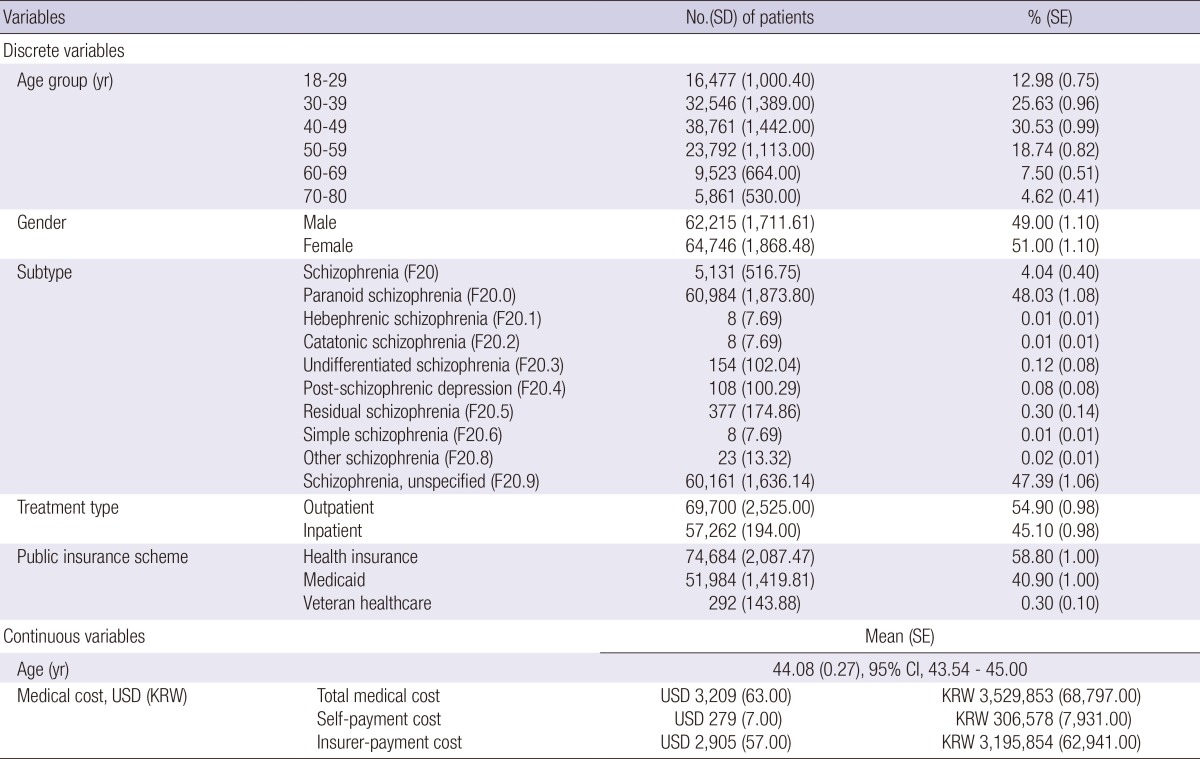
Average exchange rate 1 USD=1,100 KRW in 2009. KRW, Korea Republic Won; USD, United States Dollar.
Total antipsychotic prescription to patients with schizophrenia
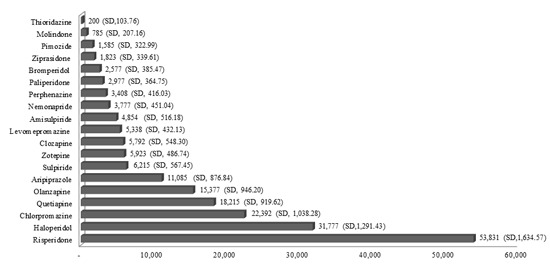
To present the patterns of total antipsychotic prescription to patients, we allowed the duplication of number of antipsychotic agents in a case prescribed with 2 or more agents of antipsychotics in the 'index prescription period.' As shown in Fig. 1, of total number of prescribed antipsychotic medications (n=197,930; SD, 2,784.13), risperidone (n=53,831; SD, 1,634.57; 27.20%, SE, 0.73), haloperidol (n=31,777; SD, 1,291.43; 16.05%, SE, 0.61), chlorpromazine (n=22,392; SD, 1038.28; 11.31%, SE, 0.50), quetiapine (n=18,215; SD, 919.62; 9.20%, SE, 0.45), olanzapine (n=15,377; SD, 946.20; 7.77%, SE, 0.46), aripiprazole (n=11,085; SD, 876.84; 5.60%, SE, 0.43), sulpride (n=6,215; SD, 567.45; 3.14%, SE, 0.28), zotepine (n=5,923; SD, 486.74; 2.99%, SE, 0.24), clozapine (n=5,792; SD, 486.74; 2.93%, SE, 0.27), and others were prescribed, in order of frequency, in Korea, 2009. Overall second-generation antipsychotics were prescribed 119,877 times (SD, 2,113.41; 60.57%, SE, 1.82), whereas first-generation antipsychotics were prescribed 78,053 times (SD, 1,847.32; 39.43%, SE, 1.10).
Fig. 1.

Antipsychotic prescription to patients with schizophrenia (n = 197,930; SD, 2,784.13).
Monopharmacy and polypharmacy to patients with schizophrenia
As shown in Fig. 2, only about one tenth (n=133,369; SD, 954.86; 10.53%, SE, 0.71) of subjects were prescribed with antipsychotic monopharmacy. About half (n=73,800; SD, 1,945.57; 58.13%, SE, 1.05) were prescribed with augmentation (combining antipsychotics with neuropsychiatric co-medications). Moreover, about one third (n=1,754; SD, 324.71; 29.96%, SE, 0.94) were prescribed with antipsychotic polypharmacy and augmentation (combining antipsychotics with another antipsychotics and neuropsychiatric co-medications), and 1.38% (SE, 0.25; n=38,038; SD, 1,318.97) were prescribed with antipsychotic polypharmacy (combining antipsychotics with another antipsychotics). For the neuropsychiatric co-medications of 126,961 patients with schizophrenia, as shown in Fig. 2, 66.60% (SE, 1.52) were prescribed with antiparkinson medications, 65.42% (SE, 1.44) anxiolytics, 36.74% (SE, 1.09) mood stabilizers, and 25.90% (SE, 1.03) antidepressants.
Fig. 2.

Monopharmacy and polypharmacy to patients with schizophrenia (n = 126,961; SD, 2,330.46).
More specifically, as shown in Table 2, 13,369 (SD, 814.23) subjects who were prescribed with antipsychotic monopharmacy were pharmaceutically managed with olanzapine (26.87%; SE, 3.31), risperidone (22.32%; SE, 3.01), quetiapine (14.21%; SE, 2.31), aripiprazole (10.41%; SE, 2.44), clozapine (9.67%; SE, 2.17), haloperidol (5.41%; SE, 1.51), chlorpromazine (4.55%; SE, 1.49) and other antipsychotics in order of frequency. As shown in Table 3, of 113,592 (SD, 2,180.16) subjects who were prescribed with polypharmacy, about half (48.57%; SE, 5.69) were pharmaceutically managed with second-generation antipsychotics and neuropsychiatric co-medications. As shown in Fig. 3, combining first-generation antipsychotic with neuropsychiatric co-medications and combining first-generation antipsychotics with second-generation antipsychotics and neuropsychiatric co-medications were prescribed with the frequencies of 16.40% (SE, 2.84) and 13.82% (SE, 3.11), respectively. Moreover, the frequency rates of subjects who were prescribed with 3 or more and 4 or more agents of antipsychotics were 4.35% (SE, 1.28) and 0.36% (SE, 0.02), respectively.
Table 2.
Patterns of monopharmacy to patients with schizophrenia (n = 13,369; SD, 814.23)
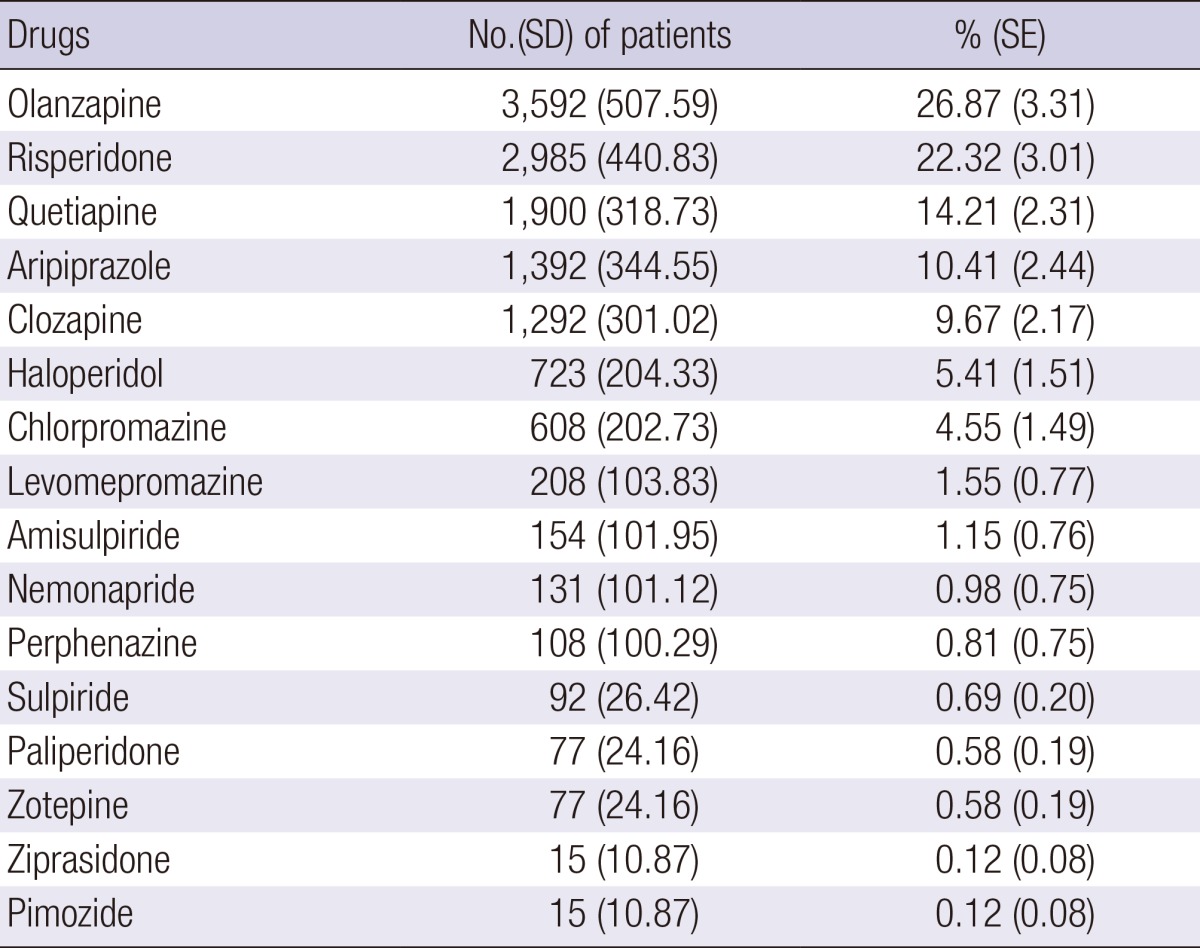
Table 3.
Patterns of polypharmacy to patients with schizophrenia (n = 113,592; SD, 2,180.16)
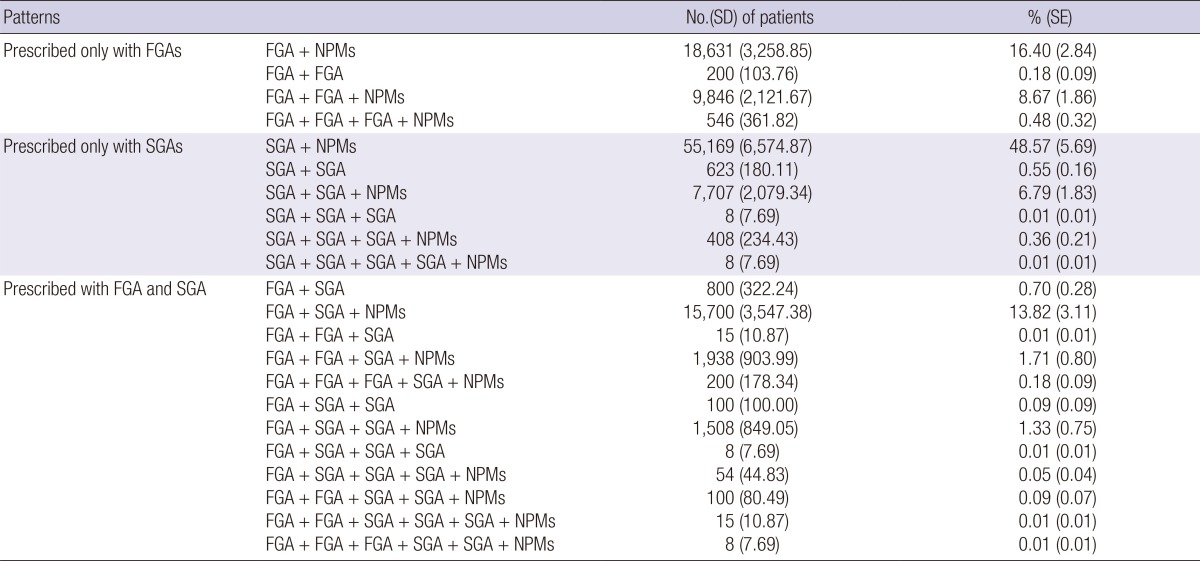
FGA, first-generation antipsychotics; SGA, second-generation antipsychotics; NPMs, neuropsychiatric co-medications (beyond antipsychotics) including mood stabilizers, antidepressants, anxiolytics, or anti-parkinson medications.
Fig. 3.

Neuropsychiatric co-medications (n = 126,961; SD, 2,330.46).
Comparison between subjects who were prescribed only with first- and second-generation antipsychotics
For efficient statistical analyses, the subjects who were prescribed with combination of first- and second-generation antipsychotics were excluded in the χ2 test for discrete variables and independent t-test for continuous variables. Hence, we compared the socioeconomic and clinical variables among schizophrenic patients prescribed only with first- (n=26,254; SD, 1,241.00; 28.04%, SE, 1.17) and second-generation antipsychotics (n=67,361; SD, 1,862.00; 71.96%, SE, 1.17), as shown in Table 4. The subjects who were prescribed only with first-generation antipsychotics were older (t=1.13, P<0.0001), higher total medical cost (t=5.93, P<0.0001), lower self-payment cost (t=-11.80, P<0.0001), and higher insurer-payment cost (t=7.42, P<0.0001) than those prescribed only with second-generation antipsychotics. In addition, those prescribed only with first-generation antipsychotics were characterized by greater proportion of male (χ2=6.905, P=0.009), higher proportion of medicaid (χ2=366.247, P<0.0001), higher prescription rates of antiparkinson medications (χ2=60.259, P<0.0001) and anxiolytics (χ2=149.193, P<0.001), and lower prescription rates of mood stabilizers (χ2=142.459, P<0.0001) and antidepressant (χ2=173.787, P<0.001) than those prescribed only with second-generation antipsychotics. However, differences of subtype (χ2=1.346, P=0.246) and in- or out-patient status (χ2=0.065, P=0.799) were not significant between the two groups.
Table 4.
Comparison between schizophrenic patients prescribed only with first- and second-generation antipsychotics (n = 93,615; SD, 2,084.00)
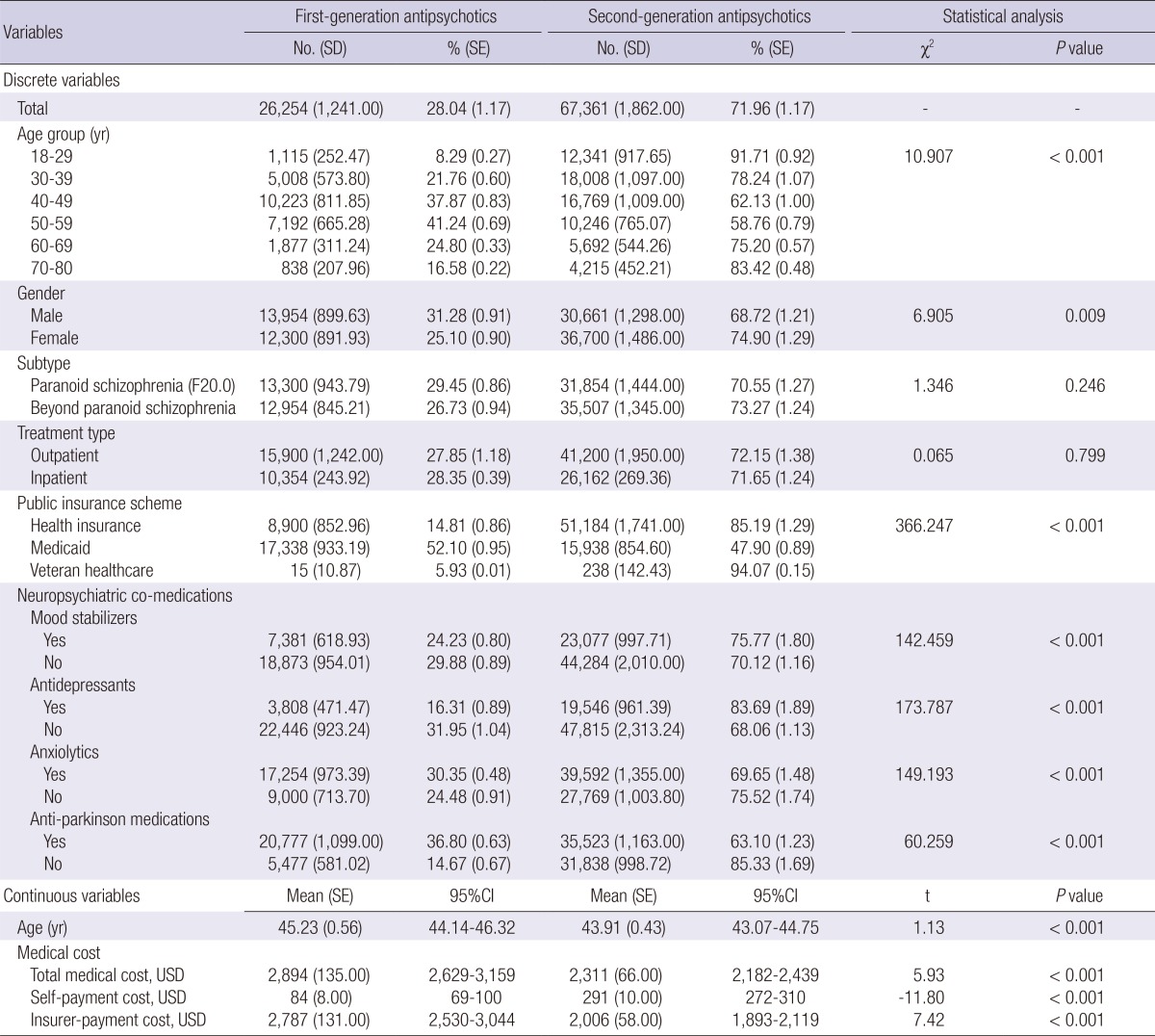
Average exchange rate 1 USD=1,100 KRW in 2009. USD, United States Dollar.
DISCUSSION
Using the HIRA-NPS, the patterns of antipsychotic prescription to 126,961 patients with schizophrenia (62,215 men and 64,746 women) in the Korean national population in 2009 is presented by estimate. Most of all, the findings of this study is characterized by higher prescription rates of first-generation antipsychotics (39.43%) in the total pharmaceutical prescriptions (n=197,930) as compared with the previous results which have been reported from the university-affiliated hospitals in Korea. As mentioned earlier in the introduction, Kwon et al. (1) have presented that only 11.9% of antipsychotic prescriptions (n=862) for the schizophrenic outpatients (n=825) at a university-affiliated hospital in Korea, 2002, are prescribed with first-generation antipsychotics. The results from the data of other university-affiliated hospital have presented that prescription rates of first-generation antipsychotics of 2003-2004 (2.0%) and 2009-2010 (1.1%) are significantly lower than 1997 (24.5%) in the patients with schizophrenia and other psychotic disorders. Hence, we can make the reasoning that attending physicians of the mental hospitals or psychiatric clinics in Korea prescribe more the first-generation antipsychotics to schizophrenic patients than those of the university-affiliated or general hospitals. The first results from Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) have presented that there is no substantial difference of the effectiveness, side effect, and quality of life which were identified between perphenazine and second-generation antipsychotics (17, 18). However, the prescription rate of perphenazine is only 1.72% (SE, 0.21) of total antipsychotic prescriptions in this study. Therefore, the findings of this study may be affected by socioeconomic factors and mental health system and policy in Korea. Moreover, the Research on Asia Psychotropic Prescription (REAP) studies have demonstrated the under-prescription of second-generation antipsychotics in East Asian region/countries including China, Hong Kong, Japan, Korea, Singapore and Taiwan (3). Of total antipsychotic prescriptions in this study, risperidone, haloperidol, chlorpromazine, quetiapine, olanzapine, aripiprazole, sulpride and so on are prescribed in frequency of prescription rate, whereas, of monopharmacy patterns, olanzapine, risperidone, quetiapine, aripriprazole, clozapine, haloperidol, chlorpromzine and so on are prescribed in frequency of prescription rate. Thus, it can be suggested that haloperidol and chlorpromazine, as the add-on medications, have been usually prescribed to schizophrenic patients in clinical psychiatry of Korea.
Notably, prescription rates of antipsychotic polypharmacy are 31.34% in this study. This rate is also higher than 9.0% of 467 schizophrenic inpatients at a general hospital in Korea, 2001 to 2008 reported by Choi et al. (6). In addition, it is remarkable that the prescription rates of 3 or more and 4 or more agents of antipsychotics are 4.35% and 0.36%, respectively, in this study. Although the Korean Medication Algorithm for schizophrenia (2006) (5) recommended clozapine or antipsychotic polypharmacy for the patients with refractory schizophrenia, the algorithm tended to prefer clozapine than antipsychotic polypharmacy. The CATIE has found that clozapine is more efficacious than other second-generation antipsychotics in treatment-refractory schizophrenia (19, 20). However, prescription rate of clozapine is only 2.93% (SE, 0.27) of total antipsychotic prescriptions in this study. The REAP studies have demonstrated that clozapine is prescribed as stable proportion across the three surveys from 2001 to 2009, ranging from 14.5% to 15.9%, and its use significantly increased over time in Korea (21). Kwon et al. (1) have reported that 29.0% of total antipsychotic prescriptions to schizophrenic outpatients at a university-affiliated hospital in Korea, 2002, are occupied with clozapine. Choi et al. (6) have also reported that 12.4% of 467 schizophrenic inpatients are prescribed with clozapine at a general hospital from 2001 to 2008. Hence, there may be a possibility that, because of risk of agranulocytosis, antipsychotic polypharmacy is more preferred than clozapine as the pharmaceutical treatment for refractory schizophrenic patients in clinical practice of Korea. Moreover, the renewing edition of Korean clinical practice guideline for schizophrenic patients may be needed to include the reasonable recommendations of clozapine for refractory individuals, and monopharmacy for those who are receiving antipsychotic polypharmacy, which has been suggested by Essock et al. (22).
In addition, as compared with schizophrenic patients who have been prescribed only with second-generation antipsychotics, those who prescribed only with first-generation antipsychotics are characterized by significantly older age, more men, more medicaid, higher total medical cost, lower self-payment cost, higher co-medication rates of antiparkinson agents and anxiolytics and lower co-medication rates of mood stabilizers and antidepressants. Results from the CATIE have demonstrated that first-generation antipsychotics cause more severe extrapyramidal symptoms and tardive dyskinesia and less metabolic adverse effects than second-generation antipsychotics (17, 23). Moreover, it is remarkable that prescribing tendency for first-generation antipsychotics is not associated with subtypes of schizophrenia and in- or outpatient status. Due to its relatively high price, lower prescription rates of mood stabilizers or antidepressants may be caused by poor socioeconomic conditions of those who have been prescribed only with first-generation antipsychotics. In addition, amelioration of the extrapyramidal effects dominantly caused by first-generation antipsychotics may contribute to higher prescription rates of antiparkinson agents or anxiolytics. On the other hand, anxiolytics have also a possibility that it has been used to treat agitation, anxiety, and insomnia symptoms of schizophrenia in this study. Medical treatment for schizophrenia in Korea has been characterized by inpatient oriented treatment, long length of hospitalization, and poor psychosocial treatment as compared with the USA or European countries. Hence, we can make an inference that patterns of antipsychotic prescription to schizophrenic patients may be controlled under the government policy of the medical treatment for schizophrenia in Korea (24). The CATIE demonstrated that first-generation antipsychotics are more cost-effective than second-generation antipsychotics (25, 26). Hence, the findings of present study have suggested a possibility that economic factors influence on first-generation antipsychotic prescriptions to chronic schizophrenia patients who are men, relatively old or cared by medicaid in Korean national population, 2009. Korean Medication Algorithm for schizophrenia (2006) (5) has focused on the preferences of second-generation antipsychotics as the first-line agents and clozapine for treatment-refractory patients. Overall, substantial prescription rate of first-generation antipsychotics and relatively minimal rate of clozapine in this study tend to be inconsistent with pharmaceutical recommendations of Korean Medication Algorithm for schizophrenia. It has been reported that psychiatrists' implementation of clinical practice guideline in Korea can be hindered by the individual factors, such as lack of awareness and lack of familiarity, and external factors, such as lack of support for mental health services and general attitudes toward guideline necessity (27). Thus, the Korean health insurance system's strict regulation for antipsychotic prescriptions to patients with schizophrenia should be alleviated. In addition, the implementation programs of the clinical practice guideline on schizophrenia from the National Institute for Clinical Experience (NICE) (28) may be needed to be applied to the renewing edition of Korean clinical practice guideline for schizophrenic patients.
There are several limitations in this study. First, convergence rate of real disease entity and medical record diagnosis in the Health Insurance Review & Assessment Service (HIRA) is 70% in 2003. Hence, there was a limited accuracy of diagnosis in this study. Second, the composition of HIRA-NPS is characterized by small ratio of outpatient sample as compared with inpatient sample. Relatively high standard deviation or standard error is usually presented in the weighted data of outpatient sample. Third, the clinical data of HIRA-NPS are not detailed. The clinical factors influencing on the patterns of antipsychotic prescriptions to schizophrenic patients are not comprehensively analyzed. Fourth, Hamann et al. (29) studied treatment patterns of patients according to distinctive regularity of medication (once only outpatient prescription; short-term outpatient treatment; long-term patients with interruptions of outpatient treatment; continuous long-term patients with outpatient treatment). In this study, patterns of antipsychotic prescription are not analyzed by treatment-based dividing of 'index prescription period.' Thus, we crudely present patterns of antipsychotic prescription to schizophrenic patients. Fifth, the clinical significance of the statistical differences between subjects prescribed only with first- and second-generation antipsychotics may be minimal; there was a possibility that these effects may be secondary consequences of the large sample size or the operational inclusion criteria. Sixth, we do not analyze the relationship between antipsychotic prescribing patterns and psychosocial interventions including supportive psychotherapy, cognitive behavioral therapy, psychiatric rehabilitation, and community mental health service. Seventh and finally, the prescription patterns of long-acting injectable antipsychotics (LAIs) to patients with schizophrenia were not demonstrated. Since the LAIs can increase adherence to a treatment regimen, clinical implications for the LAIs are currently re-emphasized (30). Despite several limitations, our study has a number of virtues. Using the HIRA-NPS, this study is a pioneering investigation about the patterns of antipsychotic prescription to schizophrenic patients in Korean national population. Hence, the findings of this study, as the baseline data, can be compared with those of later investigations about this theme. Using HIRA-NPS, this study reveal substantial prescription rates of first-generation antipsychotics and antipsychotic polypharmacy and relatively small prescription rate of clozapine in the patients with schizophrenia in Korea, 2009. Most of all, prescription of first-generation antipsychotics is regarded as the being affected mainly by socioeconomic factors or mental health system in Korea. Hence, we make a suggestion that feasibility of Korean Medication Algorithm for schizophrenia (2006) may be somewhat limited. Moreover, the further study about the differences of patterns of antipsychotic prescription in Korean patients with acute versus chronic schizophrenia can be needed.
Footnotes
The authors have no conflicts of interest to disclose.
We would like to thank Mrs. Hwa-Young Kim for her valuable help with the statistical analysis. This study was supported by a grant from Otsuka Schizophrenia Research Grant for Young Psychiatrists (2012), Korean Society for Schizophrenia Research.
References
- 1.Kwon JS, Kim ET, Ha TH, Roh KS, Choi JS, Kim YS. Drug prescribing patterns of outpatients with schizophrenia in a university hospital. J Korean Neuropsychiatr Assoc. 2003;42:683–690. [Google Scholar]
- 2.Carpenter WT, Jr, Davis JM. Another view of the history of antipsychotic drug discovery and development. Mol Psychiatry. 2012;17:1168–1173. doi: 10.1038/mp.2012.121. [DOI] [PubMed] [Google Scholar]
- 3.Chong MY, Tan CH, Fujii S, Yang SY, Ungvari GS, Si T, Chung EK, Sim K, Tsang HY, Shinfuku N. Antipsychotic drug prescription for schizophrenia in East Asia: rationale for change. Psychiatry Clin Neurosci. 2004;58:61–67. doi: 10.1111/j.1440-1819.2004.01194.x. [DOI] [PubMed] [Google Scholar]
- 4.Ahn YM, Kwon JS, Bahk WM, Kim CE, Park JI, Lee SY, Yi JS, Lee CH, Jang HS, Jun DI, et al. The feasibility test of Korean medication algorithm for the treatment with schizophrenic patients (II) : the problem for applying algorithm to the real clinical situation and opinion of revision. Korean J Psychopharmacol. 2006;17:35–49. [Google Scholar]
- 5.Ahn YM, Lee HS, Kim YS, Kwon JS. Korean Medication Algorithm for Schizophrenia. In: Lee HS, editor. Clinical Neuropsychopharmacology. Seoul: ML Communications Co. Ltd.; 2008. pp. 731–742. [Google Scholar]
- 6.Choi HJ, Jung SH, Kang MH, Lee JS, Bae JN, Kim CE. Antipsychotics prescribing patterns of patients with schizophrenia admitted to Korean general hospital psychiatric unit: 2001 to 2008. Clin Psychopharmacol Neurosci. 2011;9:17–22. doi: 10.9758/cpn.2011.9.1.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shim IH, Woo YS, Jun TY, Kim KS, Bahk WM. Changes in antipsychotic drug usage in the psychiatric inpatients at a university hospital between 1997, 2003-2004 and 2009-2010. Korean J Psychopharmacol. 2012;23:57–64. [Google Scholar]
- 8.Lee HJ, Lee TJ. Impact of price control on drug expenditure and factors associated with the drug switching among statins: analysis of HIRA-NPS data. Health Policy Manag. 2013;23:112–123. [Google Scholar]
- 9.Ha JE, Bae JH. Reasons for extraction of permanent teeth in Korea. J Korean Acad Oral Health. 2012;36:32–37. [Google Scholar]
- 10.Statistics Korea. Korean Standard Classification of Diseases. Seoul: Statistics Korea; 2010. [Google Scholar]
- 11.World Health Organization. The ICD-10 classification of mental and behavioural disorders, clinical descriptions and diagnostic guidelines. Geneva: World Health Organization; 1992. [Google Scholar]
- 12.Korean Index of Medical Specialties. [accessed on 1 July 2013]. Available at http://www.kimsonline.co.kr/051_Judge/genpricehistory.aspx.
- 13.Stahl SM. Dopamine system stabilizers, aripiprazole, and the next generation of antipsychotics, part 1, "Goldilocks" actions at dopamine receptors. J Clin Psychiatry. 2001;62:841–842. doi: 10.4088/jcp.v62n1101. [DOI] [PubMed] [Google Scholar]
- 14.Tandon R, Belmaker RH, Gattaz WF, Lopez-Ibor JJ, Jr, Okasha A, Singh B, Stein DJ, Olie JP, Fleischhacker WW, Moeller HJ. World Psychiatric Association Pharmacopsychiatry Section statement on comparative effectiveness of antipsychotics in the treatment of schizophrenia. Schizophr Res. 2008;100:20–38. doi: 10.1016/j.schres.2007.11.033. [DOI] [PubMed] [Google Scholar]
- 15.Chang JG, Roh D, Kim CH. Recent trends of antipsychotics polypharmacy in schizophrenia. Korean J Psychopharmacol. 2013;24:137–146. [Google Scholar]
- 16.Chung YK. Augmentation strategies for the treatment of schizophrenia. J Korean Soc Biol Psychiatry. 1998;5:149–154. [Google Scholar]
- 17.Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, Keefe RS, Davis SM, Davis CE, Lebowitz BD, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353:1209–1223. doi: 10.1056/NEJMoa051688. [DOI] [PubMed] [Google Scholar]
- 18.Koranek AM, Smith TL, Mican LM, Rascati KL. Impact of the CATIE trial on antipsychotic prescribing patterns at a state psychiatric facility. Schizophr Res. 2012;137:137–140. doi: 10.1016/j.schres.2012.01.043. [DOI] [PubMed] [Google Scholar]
- 19.McEvoy JP, Lieberman JA, Stroup TS, Davis SM, Meltzer HY, Rosenheck RA, Swartz MS, Perkins DO, Keefe RS, Davis CE, et al. Effectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatment. Am J Psychiatry. 2007;163:600–610. doi: 10.1176/ajp.2006.163.4.600. [DOI] [PubMed] [Google Scholar]
- 20.Lewis SW, Barnes TR, Davies L, Murray RM, Dunn G, Hayhurst KP, Markwick A, Lloyd H, Jones PB. Randomized controlled trial of effect of prescription of clozapine versus other second-generation antipsychotic drugs in resistant schizophrenia. Schizophr Bull. 2006;32:715–723. doi: 10.1093/schbul/sbj067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Xiang YT, Wang CY, Si TM, Lee EH, He YL, Ungvari GS, Chiu HF, Shinfuku N, Yang SY, Chong MY, et al. Clozapine use in schizophrenia: findings of the Research on Asia Psychotropic Prescription (REAP) studies from 2001 to 2009. Aust N Z J Psychiatry. 2011;45:968–975. doi: 10.3109/00048674.2011.607426. [DOI] [PubMed] [Google Scholar]
- 22.Essock SM, Schooler NR, Stroup TS, McEvoy JP, Rojas I, Jackson C, Covell NH Schizophrenia Trials Network. Effectiveness of switching from antipsychotic polypharmacy to monotherapy. Am J Psychiatry. 2011;168:702–708. doi: 10.1176/appi.ajp.2011.10060908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jones PB, Barnes TR, Davies L, Dunn G, Lloyd H, Hayhurst KP, Murray RM, Markwick A, Lewis SW. Randomized controlled trial of the effect on Quality of Life of second- vs first-generation antipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1) Arch Gen Psychiatry. 2006;63:1079–1087. doi: 10.1001/archpsyc.63.10.1079. [DOI] [PubMed] [Google Scholar]
- 24.Chang SM, Cho SJ, Jeon HJ, Hahm BJ, Lee HJ, Park JI, Cho MJ. Economic burden of schizophrenia in South Korea. J Korean Med Sci. 2008;23:167–175. doi: 10.3346/jkms.2008.23.2.167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rosenheck RA, Leslie DL, Sindelar J, Miller EA, Lin H, Stroup TS, McEvoy J, Davis SM, Keefe RS, Swartz M, et al. Cost-effectiveness of second-generation antipsychotics and perphenazine in a randomized trial of treatment for chronic schizophrenia. Am J Psychiatry. 2006;163:2080–2089. doi: 10.1176/ajp.2006.163.12.2080. [DOI] [PubMed] [Google Scholar]
- 26.Davies LM, Lewis S, Jones PB, Barnes TR, Gaughran F, Hayhurst K, Markwick A, Lloyd H CUtLASS team. Cost-effectiveness of first- v. second-generation antipsychotic drugs: results from a randomised controlled trial in schizophrenia responding poorly to previous therapy. Br J Psychiatry. 2007;191:14–42. doi: 10.1192/bjp.bp.106.028654. [DOI] [PubMed] [Google Scholar]
- 27.Yang J, Han C, Yoon HK, Pae CU, Kim MJ, Park SY, Ahn J. Experiences and barriers to implementation of clinical practice guideline for depression in Korea. BMC Psychiatry. 2013;13:150. doi: 10.1186/1471-244X-13-150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Pilling S, Price K. Developing and implementing clinical guidelines: lessons from the NICE schizophrenia guideline. Epidemiol Psichiatr Soc. 2006;15:109–116. doi: 10.1017/s1121189x00004309. [DOI] [PubMed] [Google Scholar]
- 29.Hamann J, Ruppert A, Auby P, Pugner K, Kissling W. Antipsychotic prescribing patterns in Germany: a retrospective analysis using a large outpatient prescription database. Int Clin Psychopharmacol. 2003;18:237–242. doi: 10.1097/00004850-200307000-00006. [DOI] [PubMed] [Google Scholar]
- 30.Jeong HG, Lee MS. Long-acting injectable antipsychotics in first-episode schizophrenia. Clin Psychopharmacol Neurosci. 2013;11:1–6. doi: 10.9758/cpn.2013.11.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]