

Abstract
Reconstruction of the upper lip requires symmetrical reconstruction of hairy male skin according to the aesthetic principle. A moderate defect of the upper lip had nonhairy skin on the upper one-third and hairy skin on the lower two-thirds in a Korean man. A hairy preauricular free flap is useful for correcting superficial-thickness skin defects of the upper lip, when local and regional flaps are not applicable. This flap was harvested from hairy posterior sideburn skin of the preauricular area including a vascular pedicle of superficial temporal artery and vein. The superficial temporal artery and vein were anastomosed with the facial artery and vein in the nasolabial fold area. The trapdoor marginal scar of this free flap required marginal scar revision and debulking twice during the postoperative course. A moderate partial-thickness defect of the upper lip in the male patient can be aesthetically restored using this free flap.
Key Words: Upper lip, cicatrix, hair, free tissue flap
Whether the defect is the result of trauma or tumor, the upper lip has been reconstructed using a variety of techniques using scalp skin grafts,1 local flaps,2–7 regional hairy skin flaps,8,9 or free scalp flaps.10,11 Various methods of reconstruction based on the size of the defect, its location, its depth, and its racial and sex characteristics have been reported.2–4
Nonhairy skin flaps may require additional hair follicle transplantation for aesthetic refinement. Korean men do not want large beard reconstructions using scalp flaps. However, the author recommended a hairy preauricular free flap to correct a moderate defect of the upper lip. The patient was satisfied with the aesthetic improvement of his upper lip after the operation.
Clinical Report
A 45-year-old patient sustained a hypertrophic scar contracture of the upper part of the left upper lip due to a car accident. The patient underwent excised release of his scar, and a full-thickness skin graft was harvested from the posterior auricular skin. However, the grafted skin of the upper lip was not aesthetically pleasing (Fig. 1).
FIGURE 1.

A preoperative view of the upper lip shows a depressed grafted deformity of the lateral lip including the left philtral column. A hypertrophic marginal scar distorts the beard hairs.
Under general anesthesia, the depressed grafted skin was completely excised, and the wound measured 2 × 2.5 cm. The moderate defect of the upper lip had nonhairy skin on the upper one-third and hairy skin on the lower two-thirds. After creation of the defect, an incision was made between the nose and corner of the mouth along the nasolabial border. Sharp dissection was preferred. The first structures observed were the zygomaticus major and the levator labii superioris muscles; in some cases, they look like 1 muscle. The continuation of the facial artery lies under these 2 muscles. Preparation for end-to-end anastomosis was preferred. The vein is not located superficially; therefore, dissection of the vein started between the lateral side of the incision and the levator labii superioris muscle. The direction of the dissection was toward the angle of the mandible or the mandibular notch. The facial vein was found deep between these structures and beside or in the Bichat fat pad. Ligation of the cranial portion of the vein was conducted to position it more superficially for end-to-end anastomosis12 (Fig. 2A).
FIGURE 2.
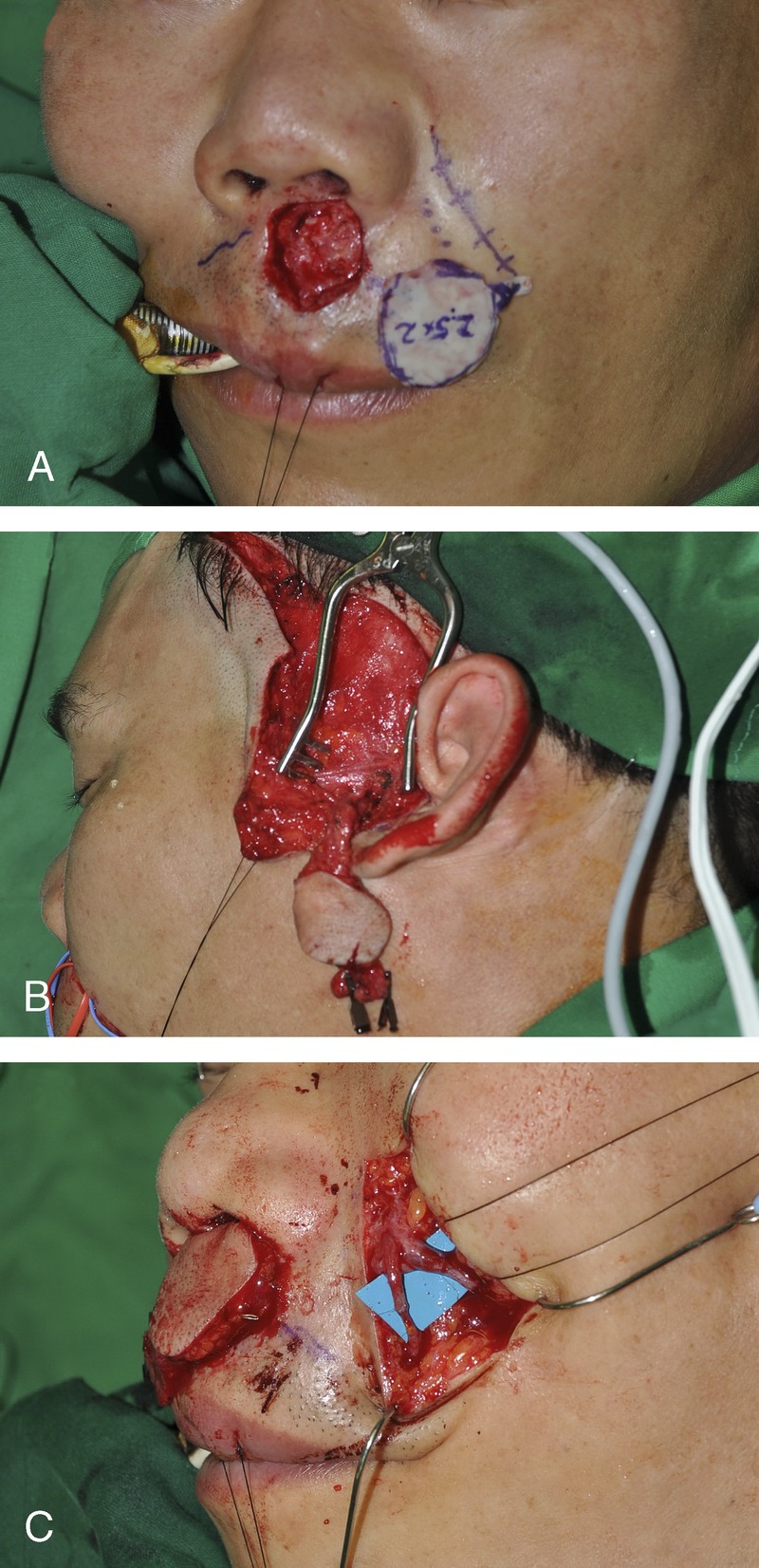
The excision of deformed tissue creates a wound defect on the upper lip. This photograph shows the wound defect and its pattern (A). A hairy preauricular skin flap was harvested with a pedicle of superficial temporal vessels (B). A preauricular flap was inserted into the wound defect, and the flap pedicle was located in the subcutaneous tunnel. Anastomotic vessels of the nasolabial wound show a superficial temporal artery and a facial artery on the medial side, and a superficial temporal vein and a facial vein on the lateral side (C).
The outline of the free flap was drawn on the preauricular skin and the posterior portion of the hairy sideburn skin of the left side. The harvested flap included the superficial temporal artery and vein (Fig. 2B). Two and a half centimeters of the superficial temporal artery and vein was anastomosed to the facial artery and vein using microsurgical techniques (Fig. 2C). The nonhairy skin portion of the flap was placed in the upper portion of the defect at the nostril base. The hairy skin portion of the flap was placed in the lower portion of the defect surrounded by bearded skin. This free flap was adequately reconstructed to the defect. However, the trapdoor deformity of the elevated flap was a conspicuous shape.
Marginal scar revision and debulking were performed twice during the postoperative course. The result of this free flap achieved a symmetrical philtral column, hairy beard, and an adequate contour of the upper lip (Fig. 3A). The donor defect repaired directly, and its repaired scar was not prominent (Fig. 3B).
FIGURE 3.

This reconstructed upper lip demonstrated a good philtral ridge and harmonized hairy skin at the 3-year follow-up (A). The scar at the donor site is inconspicuous 3 years after surgery (B).
DISCUSSION
The excision of a wide cutaneous lesion of the lateral upper lip poses a dilemma. Closure of a partial-thickness excision of the lip distorts lip contour. Aesthetically and functionally, the upper lip is an important part of the face. Its aesthetic reconstruction is difficult because symmetrical reconstruction of the free border is required. Gonzalez-Ulloa13 developed a concept of aesthetic units or subunits of the face. Scars that match the aesthetic unit or subunits are the least conspicuous. The upper lip is divided into medial and lateral aesthetic subunits.14 The lateral aesthetic subunit is bordered by the philtral column, nostril, alar base, and nasolabial crease.
Whether the defect is the result of trauma or tumor, the lip can be reconstructed using a variety of techniques with skin grafts or local flaps. Reconstruction of a beard-bearing area of the upper lip used a hair-bearing, full-thickness scalp graft to migrate the follicle into the corium after preoperative epilation to induce the catagen phase of the hair cycle.1 For partial-thickness defects of the lip, a perialar crescent-shaped advancement flap,4 V-Y subcutaneously pedicled flap,6 nasolabial flap,5 and hatchet flap7 have been the main methods used for reconstruction. The hatchet flap and V-Y subcutaneously pedicled flaps are adaptable for a defect measuring up to 20 mm in diameter without causing a conspicuous distortion of the mouth.6,7 These local flaps can develop a trapdoor deformity and/or a hair shape distortion on the upper lip in male patients. Despite refinements in technique, the reconstructed upper lip is usually devoid of hair and is bordered by a visible scar.
In males, when part of the facial hair-bearing area has to be resurfaced, the problem of beard reconstruction arises. For large, hair-bearing, partial-thickness defects of the upper lip, visor flaps8 and submental flaps9 have been used for reconstruction. These result in a good growth of hair but also lead to a thick, prosthetic-like immobile upper lip.
The transfer of large hair-bearing tissue to the upper lip restores the normal moustache territory and provides a modicum of camouflage to the midface. Free occipital hair-bearing flaps10 and free superficial temporal artery hair-bearing flaps11 were used in the reconstruction of the upper lip. The recipient vessels of these free flaps prefer the facial vessels in the angular and submandibular areas. It is a 1-stage operation, involves minimal donor-site morbidity, and uses hair-bearing scalp, which is not usually affected by male-pattern baldness.
My patient developed a 2 × 2.5-cm defect of the left lateral part of the upper lip. This defect combined nonhairy skin on the upper one-third and hairy skin on the lower two-thirds (Fig. 2A). My procedure resulted in an excellent aesthetic appearance. However, this free flap had upward hair growth that was in contrast with the surrounding normal hairy skin.
Footnotes
There were no external sources of funding provided for this project.
The authors report no conflicts of interest.
REFERENCES
- 1. Clodius L, Smahel J. Resurfacing denuded areas of the beard with full thickness scalp graft. Br J Plast Surg 1979; 32: 295– 299 [DOI] [PubMed] [Google Scholar]
- 2. Iwahira Y, Maruyama Y, Yoshitake M. A miniunit approach to lip reconstruction. Plast Reconstr Surg 1994; 93: 1282– 1285 [DOI] [PubMed] [Google Scholar]
- 3. Velasco VS, Martínez SA, Díez ME, et al. Hemiphiltrum rotated flap. Ann Plast Surg 2003; 50: 480– 483 [DOI] [PubMed] [Google Scholar]
- 4. Webster JP. Crescentic perialar cheek excision for upper lip flap advancement with a short history of upper lip repair. Plast Reconstr Surg 1955; 16: 434– 464 [DOI] [PubMed] [Google Scholar]
- 5. Georgiade NG, Mladick RA, Thorne FL. The nasolabial tunnel flap. Plast Reconstr Surg 1969; 43: 463– 466 [DOI] [PubMed] [Google Scholar]
- 6. Hurwitz DJ. Composite upper lip repair with V-Y advancement flaps. Plast Reconstr Surg 1990; 85: 120– 122 [DOI] [PubMed] [Google Scholar]
- 7. Kuwahara M, Yurugi S, Mashiba K, et al. Aesthetic reconstruction of a defect in the skin of the upper lip using a hatchet flap. J Plast Surg Hand Surg 2012; 46: 80– 84 [DOI] [PubMed] [Google Scholar]
- 8. Hafezi F, Naghibzadeh B, Nouhi A. Facial reconstruction using visor scalp. Burns 2002; 28: 679– 683 [DOI] [PubMed] [Google Scholar]
- 9. Demir Z, Kurtay A, Sahin U, et al. Hair-bearing submental artery island flap for reconstruction of mustache and beard. Plast Reconstr Surg 2003; 112: 423– 429 [DOI] [PubMed] [Google Scholar]
- 10. Walton RL, Bunkis J. A free occipital hair-bearing flap for reconstruction of the upper lip. Br J Plast Surg 1983; 36: 168– 170 [DOI] [PubMed] [Google Scholar]
- 11. Lyons GB, Milroy BC, Lendvay PG, et al. Upper lip reconstruction: use of the free superficial temporal artery hair-bearing flap, Br J Plast Surg 1989; 42: 333– 336 [DOI] [PubMed] [Google Scholar]
- 12. Oh SJ, Jeon MK, Koh SH. Nasolabial facial artery and vein as recipient vessels for midface microsurgical reconstruction. J Craniofac Surg 2011; 22: 789– 791 [DOI] [PubMed] [Google Scholar]
- 13. Gonzalez-Ulloa M. Restoration of the face covering by means of selected skin in regional aesthetic units. Br J Plast Surg 1956; 9: 212– 221 [DOI] [PubMed] [Google Scholar]
- 14. Burget GC, Menick FJ. Aesthetic restoration of one-half the upper lip. Plast Reconstr Surg 1986; 78: 583– 593 [DOI] [PubMed] [Google Scholar]