

Abstract
We describe an infant with respiratory distress due to bilateral dacryocystoceles and dacryocystitis who was successfully treated with urgent bilateral endoscopic marsupialization.
A male infant was brought to our outpatient department 7 days after birth, with red, acutely inflamed swellings near the medial canthal area of both eyes. From birth, there had been bluish swelling near the medial canthal area, and redness and swellings developed within 3 days. On physical examination, the child was afebrile but showed respiratory distress with coarse breathing sound. That day, the infant was admitted and treated with intravenous cefotaxime 150 mg. After withholding oral intake for appropriate preoperative fasting, urgent bilateral probing with endoscopy was done. On endoscopy, huge bilateral congenital dacryocystoceles were found. Because of its huge size, the inferior surface of the cyst was touching the nasal floor, which made probe unable to perforate the wall of dacryocystocele. Therefore, an endoscopy-assisted marsupialization of dacryocystoceles and bicanalicular silicone intubation were performed. Both swellings and erythema subsided within 48 hours postoperatively, and the patient was discharged after 72 hours from treatment.
Key Words: Bilateral dacryocystitis, bilateral dacryocystoceles, endoscopic marsupialization, respiratory distress
Congenital dacryocystocele is an uncommon congenital anomaly in infants and children, and 12% to 25% of patients affected have bilateral lesions.1–4 Secondary dacryocystitis frequently develops within days or weeks.
However, bilateral dacryocystoceles with bilateral acute dacryocystitis, occurring within the first year of life, have rarely been observed.5 The incidence of acute dacryocystitis, shortly after birth, is extremely rare in that only a few cases have been reported in the world, especially the bilateral case.6 Because infants are obligate nasal breathers within the first 3 weeks, congenital dacryocystocele may cause dyspnea, especially in bilateral huge cases.7
In this clinical report, we present an infant with bilateral dacryocystoceles with bilateral acute dacryocystitis, causing respiratory distress.
CLINICAL REPORT
A 7-day-old male infant presented to the author, with bilateral red, acutely inflamed swellings near the medial canthal area of both eyes (Fig. 1A). His parents had noted that bluish swelling had been presented near the medial canthal area from birth and that redness and swelling developed gradually within 3 days.
FIGURE 1.
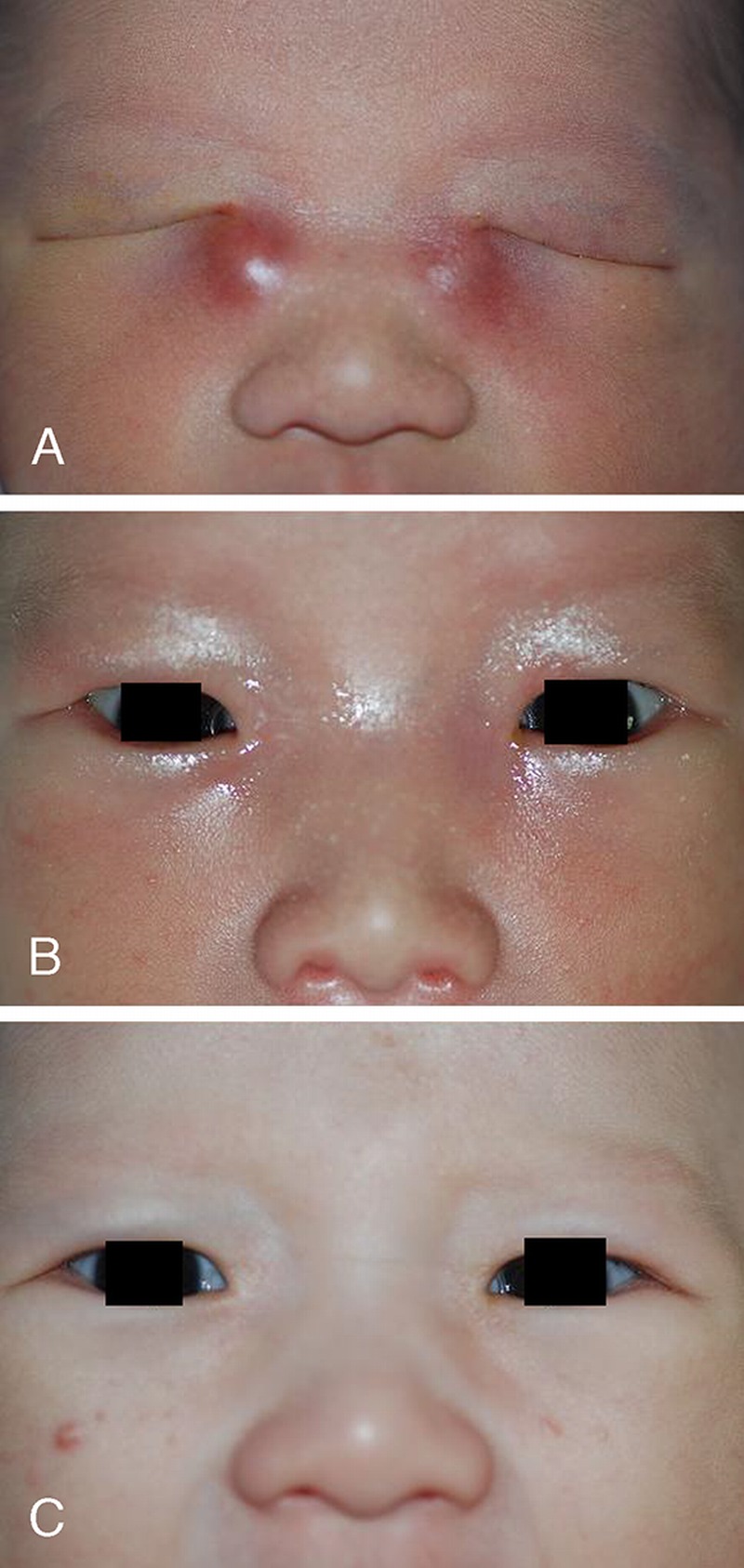
A, Photograph of an infant with a red, acutely inflamed swelling near the medial canthal area of both eyes before the surgery. B, Photograph of 1 day after the operation. C, Photograph of 2 days after the operation.
On physical examination, the child was afebrile but showed respiratory distress with coarse breathing sound. Bilateral tense and acute inflammatory swellings were found in the region of the lacrimal sac with edema and erythema of the surrounding skin and eyelids.
Suspected to have bilateral dacryocystoceles with bilateral dacryocystitis, the infant was admitted and treated with intravenous cefotaxime 150 mg. That day, after withholding oral intake for appropriate preoperative fasting, the authors attempted bilateral probing with 0.65-mm probe with endoscopy under desflurane anesthesia. On endoscopy, huge bilateral intranasal cysts were found (Figs. 2A, B). Because of its huge size, the inferior surface of the cyst was touching the nasal floor, which made probe, via the nasolacrimal duct, unable to perforate the wall. Therefore, an endoscopy-assisted marsupialization of dacryocystoceles and bicanalicular silicone intubation were attempted. After the right dacryocystocele was excised with a microscissor, the probe was observed beneath the inferior turbinate with endoscopy. The remaining cyst was also excised. Pus was expressed from the cyst, and the culture of which was collected sterilely. A 0.02% Mitomycin C packing was done for 5 minutes. Right bicanalicular silicone intubation was done. The same procedures were also performed in the left side (Figs. 2C, D).
FIGURE 2.
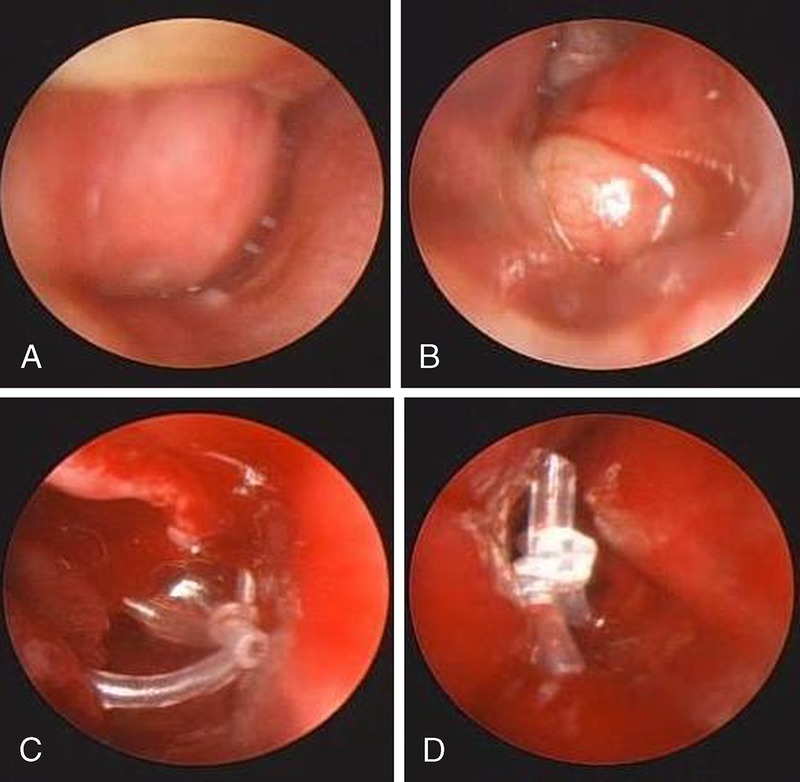
Endoscopic view of right dacryocystocele (A) and left dacryocystocele (B) before the surgery. Endoscopic view of right (C) and left (D) marsupialized dacryocystoceles.
Pathologic analysis demonstrated that the cyst was lined by ciliated cuboidal epithelium with acute inflammation, and the definite diagnosis was dacryocystoceles with dacryocystitis. Methicillin-resistant Staphylococcus aureus was found at the culture.
Both swellings and erythema subsided within 48 hours postoperatively, and the patient was permitted to be discharged after 72 hours from treatment (Fig. 1B, C). Three days later, the infant was followed up in the outpatient department. Swellings and erythema of both sides resolved and the silicone tube was in place.
DISCUSSION
In dacryocystocele, the lacrimal drainage system is obstructed both proximally at the level of the common canaliculus and distally at the level of the valve of Hasner.8,9 With distal obstruction, fluids in the lacrimal sac and nasolacrimal duct cannot drain, expansion of sac develops, and the valve of Rosenmuller can be collapsed. Thus, proximal obstruction at the junction of the common canaliculus and lacrimal sac is functional.3,8,10 Fluid keeps entering the system but does not drain into the nasal cavity, forming the dacryocystocele.3
A congenital dacryocystocele presents as an enlarged blue cystic lacrimal sac in the medial canthal area, epiphora, and high tear meniscus height at birth.8,9 Secondary infection producing mucopurulent discharge or cellulitis can occur.9 A dacryocystocele often presents as an intranasal mass in the anterior inferior meatus.9 The differential diagnosis includes capillary hemangioma, solid dermoid, dermoid cyst, encephalocele, meningoencephalocele, nasal glioma, lymphangioma, and heterotopic brain.11,12 Thus, infants with medial canthal mass have to be evaluated with a detailed ophthalmologic examination and nasal endoscopy.9 Ultrasonography may be helpful in ruling out the vascular and cystic lesion, and computed tomography as well as magnetic resonance imaging may assist in differentiating a potential intracranial connection.9
Mansour et al1 studied 54 cases of patients with a congenital dacryocystocele and showed strong female preponderance (73%) and unilateral involvement (88%). The natural course of congenital dacryocystoceles is variable, which makes treatment strategies controversial. Nasal obstruction and respiratory distress can occur in infants with bilateral dacryocystoceles because infants are obligate nasal breathers.7 Parents of infants with dacryocystoceles should be carefully asked about symptoms of nasal congestion, snoring respirations, tachypnea, and breathing difficulty with feeding.7 Infants with dacryocystoceles should have surgical treatment on an urgent basis if there is a cyst in the nose and nasal obstruction.8 Three surgical treatment options exist for congenital dacryocystoceles: simple probing, probing assisted by endoscopy, as well as nasal endoscopy and marsupialization of the dacryocystocele.9 Endoscopy can visualize and help marsupializing the dacryocystocele, resulting in decompression of the lacrimal system distally as well as identification and treatment of contralateral dacryocystocele.12,13
Bilateral congenital dacryocystoceles, with bilateral acute dacryocystitis, are a very rare case; there have been only a few cases reported in the world, and not a single case was reported in Korea.
In this case, dacryocystoceles protruded along the direction of the lacrimal duct endonasally, beneath the inferior turbinate, and led to nasal obstruction with respiratory distress, especially when feeding.7 We had to urgently manage the infant with endoscopy-assisted marsupialization because bilateral congenital dacryocystoceles with bilateral dacryocystitis caused respiratory distress. Our case shows that probing alone may not be enough to treat huge dacryocystocele because its huge size makes inferior surface of the dacryocystocele, touching the nasal floor. We agree with Teixeira et al3 that an infant who has dacryocystoceles and respiratory distress must be treated through the wide marsupialization of the dacryocystoceles urgently.
Footnotes
The authors report no conflicts of interest.
REFERENCES
- 1. Mansour AM, Cheng KP, Mumma JV, et al. Congenital dacryocele. A collaborative review. Ophthalmology 1991; 98: 1744– 1751 [DOI] [PubMed] [Google Scholar]
- 2. Cavazza S, Laffi GL, Lodi L, et al. Congenital dacryocysticele: diagnosis and treatment. Acta Otorhinolaryngol Ital 2008; 28: 298– 301 [PMC free article] [PubMed] [Google Scholar]
- 3. Teixeira CC, Dias RJ, Falcão-Reis FM, et al. Congenital dacryocystocele with intranasal extension. Eur J Ophthalmol 2005; 15: 126– 128 [PubMed] [Google Scholar]
- 4. Han BL, Shin HS. Dacryocystocele with congenital unilateral lacrimal puncta agenesis in an adults. J Craniofac Surg 2013; 24: 1242– 1243 [DOI] [PubMed] [Google Scholar]
- 5. Lipton J, Jacobs N, Rosen ES. Bilateral acute dacryocystitis in an infant. Br J Hosp Med 1987; 38: 251. [PubMed] [Google Scholar]
- 6. Berson D, Landau L. Bilateral acute dacryocystitis in a premature infant. J Pediatr Ophthalmol Strabismus 1978; 15: 168– 169 [DOI] [PubMed] [Google Scholar]
- 7. Teymoortash A, Hesse L, Werner JA, et al. Bilateral congenital dacryocystocele as a cause of respiratory distress in a newborn. Rhinology 2004; 42: 41– 44 [PubMed] [Google Scholar]
- 8. Becker BB. The treatment of congenital dacryocystocele. Am J Ophthalmol 2006; 142: 835– 838 [DOI] [PubMed] [Google Scholar]
- 9. Shashy RG, Durairaj VD, Holmes JM, et al. Congenital dacryocystocele associated with intranasal cysts: diagnosis and management. Laryngoscope 2003; 113: 37– 40 [DOI] [PubMed] [Google Scholar]
- 10. Woo KI, Kim YD. Four cases of dacryocystocele. Korean J Ophthalmol 1997; 11: 65– 69 [DOI] [PubMed] [Google Scholar]
- 11. Shields JA, Shields CL. Orbital cysts of childhood-classification, clinical features, and management. Surv Ophthalmol 2004; 49: 281– 299 [DOI] [PubMed] [Google Scholar]
- 12. Roy D, Guevara N, Santini J, et al. Endoscopic marsupialization of congenital nasolacrimal duct cyst with dacryocoele. Clin Otolaryngol Allied Sci 2002; 27: 167– 170 [DOI] [PubMed] [Google Scholar]
- 13. Ram B, Barras CW, White PS, et al. The technique of nasendoscopy in the evaluation of nasolacrimal duct obstruction in children. Rhinology 2000; 38: 83– 86 [PubMed] [Google Scholar]