

Abstract
Many depressed adolescents experience difficulty regulating their emotions. These emotion regulation difficulties appear to emerge in part from socialization processes within families and then generalize to other contexts. However, emotion dysregulation is typically assessed within the individual, rather than in the social relationships that shape and maintain dysregulation. In this study, we evaluated concordance of physiological and observational measures of emotion dysregulation during interpersonal conflict, using a multilevel actor-partner interdependence model (APIM). Participants were 75 mother-daughter dyads, including 50 depressed adolescents with or without a history of self-injury, and 25 typically developing controls. Behavior dysregulation was operationalized as observed aversiveness during a conflict discussion, and physiological dysregulation was indexed by respiratory sinus arrhythmia (RSA). Results revealed different patterns of concordance for control versus depressed participants. Controls evidenced a concordant partner (between-person) effect, and showed increased physiological regulation during minutes when their partner was more aversive. In contrast, clinical dyad members displayed a concordant actor (within-person) effect, becoming simultaneously physiologically and behaviorally dysregulated. Results inform current understanding of emotion dysregulation across multiple levels of analysis.
Keywords: Emotion dysregulation, respiratory sinus arrhythmia (RSA), depression, dyadic conflict
Adolescent depression is a pervasive and impairing condition characterized in part by emotion dysregulation and sensitivity to interpersonal conflict (Allen, Kuppens, & Sheeber, 2012). The prevalence rate of depression increases markedly during adolescence (Lewinsohn, Hops, Roberts, Seeley, & Andrews, 1993), making this an opportune stage to observe the dynamic interplay of emotion dysregulation and interpersonal stress. Considerable socialization of both conflict resolution strategies and emotion regulation/dysregulation occurs within family relationships (Eisenberg, 2000; Morris, Silk, Steinberg, Myers, & Robinson, 2007). Parents and children shape one another’s behaviors, emotions, and physiological responses through dyadic interaction patterns that occur thousands of times across development (see e.g., Patterson, Dishion, & Bank, 1984). Thus, parent-child conflict represents an ideal context in which to observe emerging regulatory strategies.
Emotion regulation comprises biological and social processes. However, few studies have examined both simultaneously. This is unfortunate given evidence that emotion regulation develops through interpersonal mechanisms (Cassidy, 1994; Coan, 2010; Crowell, Skidmore, Rau, & Williams, 2013). A variety of labels have been applied to social processes that promote emotion regulation, including attunement, co-regulation, external regulation, synchrony, and mutual regulation (Coan, 2010; Helm, Sbarra, & Ferrer, 2012; Hughes, Crowell, Uyeji, & Coan, 2012). Regardless of the label used, the regulatory power of social relationships is well documented; vocal cues, touch, instrumental support, and emotion coaching are potent sources of regulation for infants and children (see Campos, Campos, & Barrett, 1989, for a review). Such co-regulation may be especially important in childhood and early adolescence, before neural systems implicated in top-down volitional modulation of affect have matured fully (see e.g., Beauchaine & McNulty, 2013). Yet even in adulthood, co-regulation within relationships contributes to better self-control, health, and interpersonal connectedness (Coan, Kasle, Jackson, Schaefer, & Davidson, 2013; Diamond & Aspinwall, 2003; Pietromonaco, Uchino, & Dunkel Schetter, 2013). Thus, social relationships serve powerful self-regulatory functions (Hofer, 1995; Hughes, et al., 2012).
In most studies, emotion is assessed intrapersonally (e.g., Reis, Collins, & Berscheid, 2000), and emotion regulation is described as a set of processes through which an individual—either volitionally or automatically—modulates the intensity, duration, or valance of an emotion to meet contextual demands (Cole, Martin, & Dennis, 2004; Gross, 1998). According to nearly every theory, emotions are described as coordinated behavioral, physiological, and cognitive response tendencies (e.g., Ekman & Friesen, 1976). For example, anxiety facilitates survival-related behavior and physiological activation in response to threat. When the threat is removed or appraised differently, behavioral and physiological recovery should occur (Cole et al., 2004; Gross, 1998). However, stimulus conditions are rarely so simple or circumscribed. Rather, biological, social, behavioral, and cognitive systems each act upon one another to produce dynamic emotional states, and regulation (or dysregulation) of these states. This has led many scholars to promote multi-method, multiple-levels-of-analysis approaches to the study of emotion and emotion regulation (Beauchaine & McNulty, 2013; Beauchaine & Gatzke-Kopp, 2012; Calkins, 2010). As a result, we now have a richer understanding of the complexity that follows from gathering data across multiple levels of analysis.
Concordance: A Multimethod Approach
Concordance can be defined as a coordinated response across subjective, cognitive, expressive, and physiological measures of emotion (see e.g., Hollenstein & Lanteigne, this issue; Marsh, Beauchaine, & Williams, 2008). According to functionalist accounts, concordance reflects emotional wellbeing, whereas discordance may indicate vulnerability to psychopathology (Ekman, 1999; Levenson, 1994). However, after several decades of empirical study, evidence in support of this theory is inconsistent (Marsh et al., 2008; Lanteigne, Flynn, Eastabrook, & Hollenstein, 2012). This has led some to conclude that emotional response systems are only loosely or probabilistically correlated, and that concordance may only be observed during the experience of very strong emotions, or in specific contexts (Cacioppo, Berntson, & Klein, 1992; Mauss et al., 2005; Reisenzein, 2000). Notably, these arguments apply to intrapersonal concordance. Assessing interpersonal concordance is even more complicated, since each participant’s behavioral and physiological responses are affected by both endogenous experiences and partner behaviors.
In addition, much of the existing literature has tested concordance hypotheses during tasks designed to elicit specific, discrete emotions (e.g., anger or sadness; Hubbard et al., 2004; Reisenzein, Studtmann, & Horstmann, 2013). In these study designs, emotion regulatory efforts could disrupt attempts to measure concordance, producing inconsistent results (Butler et al., this issue; Mauss, 2005). Thus, there are two distinct and conflicting hypotheses that follow from research with typical controls. On the one hand, healthy participants should show greater concordance across measures of emotion relative to clinical participants because concordance presumably reflects wellbeing (Marsh et al., 2008). On the other hand, controls may evidence less concordance if they have better emotion regulation skills and are actively regulating or suppressing their expressions (Mauss, 2005).
The Present Study
In the present study, we examined minute-to-minute concordance across physiological and behavioral markers of emotion dysregulation during a mother-daughter conflict task. We also explored how patterns of concordance/discordance differ between typical mother-daughter dyads (controls) and those in which the daughter is depressed (clinical). We operationalized behavior dysregulation as observed aversiveness during conflict, and physiological dysregulation as respiratory sinus arrhythmia (RSA) reactivity. Unique to this study, we model concordance simultaneously within each dyad member (e.g., concordance between the mother’s RSA and her own aversive behavior) and between members (e.g., concordance between the mother’s RSA and her adolescent’s aversive behavior). This is a more thorough test of concordance within an interpersonal stress paradigm than most studies conducted to date.
Respiratory sinus arrhythmia
Respiratory sinus arrhythmia is often used as a psychophysiological index of emotion regulation capacity (see Beauchaine, 2001; Beauchaine, 2012; Porges, Doussard-Roosevelt, Portales, & Greenspan, 1996). Interest in RSA follows from polyvagal theory (PVT; Porges, 1995), including its application to both normative development of emotion regulation (e.g., Hinnant, Elmore-Staton, & El-Sheikh, 2011) and the development of emotion dysregulation in psychopathology (e.g., Beauchaine, 2001; Beauchaine, Gatzke-Kopp, & Mead, 2007). According to PVT, parasympathetic efference to the heart (from the nucleus ambiguous through the vagus nerve) serves to inhibit fight/flight (F/F) responding and promote adaptive behaviors, including social affiliation (Beauchaine et al., 2007; Porges, 2007).
When faced with conspecifics, mammals must decide quickly whether to affiliate, initiate F/F behaviors, or withdraw/freeze (Porges, 2003). Affiliation requires sustained attention, which is served through increased vagal activity. In contrast, conflict requires rapid mobilization of sympathetically-mediated cardiac output, which is often accompanied by vagal withdrawal (see Beauchaine, 2001; Beauchaine et al., 2007; Porges, 1995). Following from these functional relations, estimates of vagal activity and reactivity may serve as a peripheral measures of self-regulation in contexts of interpersonal interactions. Increases in vagal activity may mark better regulation in the service of social affiliation, whereas decreases in vagal activity often reflect compromised regulatory capacity1.
Behavioral dysregulation
Behaviorally, emotion regulation is often measured through self-reports or observational coding. Analytic approaches vary, but many scholars suggest that emotion and its regulation should be assessed independently (Cole et al., 2004). However, this presents a measurement challenge because participants often anticipate their emotional reactions and modify their responses accordingly (e.g., through cognitive reinterpretation or avoiding the situation). In contrast, emotion dysregulation is easier to identify and measure behaviorally. According to one useful definition, dysregulated emotions are characterized by four central features: (1) they persist for too long and attempts at regulation are ineffective; (2) they interfere with appropriate behavior; (3) they are inappropriate to the context; and/or (4) they change too abruptly or too slowly (Cole, Hall, & Hajal, 2013). Thus, whereas emotion regulation often occurs internally, emotion dysregulation can be observed and coded objectively. In a laboratory conflict discussion, for example, dysregulation might be defined by escalating negative emotional exchanges that are less responsive to self- or co-regulation attempts.
Hypotheses
Following from this review, we seek to characterize minute-to-minute concordance across physiological (RSA reactivity) and behavioral (observed aversiveness) dysregulation during conflict. We define concordance as the minute-to-minute covariation of physiology and observed behavior. In contrast, discordance is defined as the lack of an association across levels of analysis. As noted above, we are interested in both intra- and interpersonal concordance. Indeed, physiological dysregulation during conflict could be tied to one’s own behavior (i.e., an actor effect) or the behavior of one’s partner (i.e., a partner effect). Furthermore, patterns of concordance may differ based upon group status.
Intrapersonal concordance
Clinical depression is often characterized by ruminative self-focus that is non-responsive to external modulation (e.g., Pyszcynski & Greenberg, 1987). This suggests that depressed participants should show concordance between their own behavioral and physiological dysregulation. In addition, several studies indicate that depressed children, adolescents, and adults exhibit RSA withdrawal in response to stress, consistent with theories that vagal withdrawal is associated with poor emotion regulation (e.g., Boyce et al., 2001; Carney et al., 2000; Crowell et al., 2005). Thus, for depressed participants we predicted a negative association between their own aversive behavior and RSA reactivity (i.e., increased aversiveness corresponding with RSA withdrawal; concordance). We also predicted a concordant within-person response for mothers of depressed participants, given familiality of both depression and emotion dysregulation (Cummings & Davies, 1994). For control participants and their mothers, we hypothesized that there would be no association between the participant’s aversive behavior and their own RSA reactivity (i.e., discordance).
Interpersonal concordance
Recently, many scholars have become interested in understanding dyadic emotional exchanges rather than individual emotional response systems (see e.g., Butler & Randall, 2013). Whether the context is parent-child, spousal, sibling, or therapist-client, emotions often occur within relationships. Until recently, methods for assessing dyadic emotion have lagged behind theories of their effects on relationships. However, this has begun to change due to advanced statistical techniques and reduced costs of psychophysiological data collection. For example, the temporal interpersonal emotion system (TIES) model (Butler, 2011) describes current approaches to assessing behavioral, physiological, and subjective aspects of emotion within dyads. Butler describes relationships as dynamic, self-organizing systems in which present states are affected by relationship structure, past states (e.g., current levels of conflict are similar to past levels of conflict), and moment-to-moment feedback processes. In other words, emotional responses of one person depend upon emotional states of the other, and these associations are dependent upon the nature of the relationship: a three-way interaction.
In control mother-daughter dyads, physiological responses are likely to track with partner—rather than one’s own—behavior. This would follow from theories that healthy relationships are characterized by high responsiveness to one another’s emotional cues (e.g., Coan et al., 2013). Furthermore, according to polyvagal theory, social orienting and attentiveness to partner behavior would be marked by increases in RSA. Thus, we hypothesized that members of control dyads would show a positive association between their partner’s behavior and their own RSA (i.e., between-person concordance). Similarly, we theorized that the clinical dyads would show no association between partner behavior and RSA (i.e., discordance), consistent with theories of depressive self-focus (Pyszcynski & Greenberg, 1987).
Method
Participants
Participants included 75 female adolescents, ages 13-17 years, who were enrolled in one of three groups: depressed + self-injuring (SII), depressed with no self-injury history (DPR), and control (CTR). Both SII and DPR adolescents met Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (American Psychiatric Association, 2000) criteria for major depression, and were aggregated as a single clinical group for or all analyses. Initially, 84 mother-teen dyads were enrolled and completed some study procedures. However, nine participants had insufficient data to be analyzed due to inability/refusal to return for the physiological assessment (n=4), failure of physiological equipment (n=3), or arriving with a guardian other than the biological mother (n=2), which resulted in the final sample of 75. These nine did not differ from the overall sample on any demographic or diagnostic variables, all Fs < 1.07, all ps > 0.29, all η2 < 0.02.
Inclusion and exclusion criteria, participant demographics, and screening procedures are detailed elsewhere (see Crowell et al., 2012). Briefly, the mean age of participants was 16.1 years (SD=1.3). The sample was 70.2% Caucasian, 7.1% African American, 6.0% Asian American, 4.8% Latina, 1.2% Native American, and 10.7% of mixed racial/ethnic heritage. Due to potential effects on psychophysiological recordings, adolescents and parents were excluded if they were taking beta blockers, mood stabilizers, benzodiazepines, or had taken recreational drugs (confirmed via urinalysis). Adolescents who were taking prescription stimulants (n=3) were included if the parent and adolescent agreed to a 36-hr washout prior to assessment. No parents were taking stimulants. Participants completed two assessments and were given $20 for completing Visit 1 and an additional $40 after completing Visit 2. Study procedures were approved by the institutional review board at Seattle Children’s Hospital. Written informed assent and consent were obtained from adolescents and mothers, respectively.
Procedure
At Visit 1, adolescents and their mothers completed diagnostic interviews and self-report measures to confirm presence of depression (clinical group) or no psychopathology (controls). These measures are reported elsewhere and are not the focus of the current study (see Crowell et al., 2012). Adolescents and mothers were then scheduled to return approximately 2 weeks later to participate in a psychophysiological assessment, including a conflict discussion. This assessment was conducted in a sound-attenuated room that was monitored with audio-video recording equipment. Prior to the discussion, both dyad members completed the Issues Checklist (Prinz, Foster, Kent, & O’Leary, 1979), a 44-item questionnaire used to identify a discussion topic (e.g., chores, privacy). Responses on the checklist were rated on frequency, ranked from 1 (never) to 5 (very often), and intensity, ranked from 0 (calm) to 40 (intense). A trained research assistant then chose a topic based on the best match between the adolescent and mother on severity and frequency. For all dyads, the selected topic did not exceed an intensity level of 20, which resulted in intense discussions but also minimized the possibility of extreme distress.
Psychophysiological Assessment
Electrocardiograph (ECG) signals were obtained through a spot electrode configuration, described by Qu, Zhang, Webster, and Tompkins (1986), and sampled at 1 kHz using a BioPac MP100 system (Goleta, CA). RSA was indexed by extracting the high frequency component (>.15 Hz) of the R-R time series using MindWare software (Mindware Technologies, Ltd., Gahanna, OH, USA). Electrocardiographic data were first collected during a 2 min resting baseline. Next, the research assistant re-entered the room and revealed the discussion topic. Adolescents and their mothers were instructed to maintain conversation for the full 10 min, and to limit unnecessary movement. Electrocardiographic data were collected during the entire discussion task, and change scores were calculated for each minute by subtracting the baseline score from the discussion task score. This enabled us to evaluate concordance between RSA reactivity and behavior across ten 1-min epochs. Although greater temporal resolution might be preferred, 1 min is often considered to be a minimum length for spectral analysis of high frequency heart rate variability (Berntson et al., 1997). Conversations were videotaped for behavioral coding.
Coding
The Family and Peer Process Code (FPPC; Stubbs, Crosby, Forgatch, & Capaldi, 1998) is a microanalytic behavioral coding system used to score dyadic behavior moment-to-moment. With the FPPC, raters assign a numerical code that represents the speaker, verbal behavior, and affect of each utterance. The code changes when there is a shift on any of these dimensions. The FPPC contains 25 content codes describing verbal behaviors, and 6 affect codes including 2 positive, 1 neutral, and 3 negative codes. Affect codes can be reduced into a 3-point scale (positive, neutral, negative). This results in a total of 25 content × 3 affect combinations. In order to examine aversiveness, we followed a strategy developed and validated by Snyder and colleagues (1994) and tested in a sample of adolescent females (Crowell, Baucom et al., 2013). Each of the 75 codes (25 content × 3 affect) was reduced into a single number on a 10-point scale ranging from highly positive utterances (0) to coercive or attacking utterances (9).
Coding was conducted by two trained research assistants who received approximately 15 hrs per week of training on the FPPC following a multi-step process. First, coders were required to review the manual and become familiarized with the codes. Second, several tapes were reviewed and discussed code-by-code. Those tapes were acquired from other lab projects and had been scored in advance by the lead author. Third, the coders and lead author met and coded three criterion tapes as a group. Fourth, coders coded three additional criterion tapes without assistance, and discrepancies were discussed at the following meeting. Finally, coders were assigned three tapes per week including one shared tape—used to prevent observer drift and resolve coder disagreements. Coders were required to meet a minimum 10-key typing speed of 8,000 keystrokes per hour with 95% accuracy. Reliability between coders was calculated on raw data (i.e., prior to collapsing into the 10-point scale). Consistent with published work (Snyder et al., 1994), reliability was κ = .76 for content and κ = .69 for affect. Coders were blind to study hypotheses and group status.
Analytic Plan
Concordance between psychophysiology and behavior was conceptualized as within-epoch associations between RSA and aversiveness during the mother-daughter conflict discussion. As outlined above, the discussion was 10 min, which was subdivided into ten 1-min epochs. RSA reactivity (i.e., change scores) and mean aversiveness were modeled for each minute of the discussion. To examine concordance across psychophysiology and behavior both between and within dyad members, we used a multilevel actor-partner interdependence model (APIM; Kenny, Kashy, & Cook, 2006). We selected a multilevel approach because such models account for multiple forms of nesting (e.g., multiple measures from both mother and teen) and allow for unbalanced data including families with missing epochs. All analyses were conducted in HLM™, version 7.00 (Raudenbush, Bryk, & Congdon, 2011).
Actor-partner interdependence models are particularly advantageous for analyzing within-and between-person behavioral and physiological concordance, because they allow for simultaneous estimation of actor effects (e.g., effects of teen aversive behavior on teen RSA) and partner effects (e.g., effects of mother aversive behavior on teen RSA) for both family members. Including actor and partner effects in the same model allows for interpreting actor effects as representing an association within a dyad member, while accounting the same association between members and vice versa for partner effects. Additionally, APIM permits examination of between-family differences in concordance, so a single MLM can be used to test within-family effects (short-term concordance between aversive behavior and RSA within a given epoch), and between-family effects (i.e., differences in short-term concordance across families and group).
We followed procedures recommended by Kashy and Donnellan (2012) to create a two-intercept, repeated measures APIM model for distinguishable dyads by regressing each person’s RSA change score onto her own aversive behavior within an epoch (the actor effect), the other family member’s aversive behavior within an epoch (the partner effect), each family member’s average aversive behavior across the entire conversation (to capture the overall tone of the relationship; Butler, 2011), group (-.5 = control, .5 = clinical), and the two-way and three-way interactions between aversive behavior within an epoch, average aversive behavior, and group (clinical vs. control) as illustrated in the following equations:
with random effects, u1j and u2j, included on the intercepts for teen (β1j) and mother (β2j) respectively2. All Level-1 predictors were person-mean centered, and all continuous Level-2 predictors were grand-mean centered prior to creation of interaction terms and for analysis (Enders & Tofighi, 2007). Including average aversiveness and group at Level 2 allowed us to model how the overall tone of the relationship and group status affected Level 1 concordance, consistent with Butler’s (2011) review.
Results
The theoretical model we tested is depicted in Figure 1. As illustrated, we modeled both the concordance of the emotional system within each person (actor effects) while simultaneously accounting for concordance across persons (partner effects). Two-way interactions test the Group × Minute-to-minute Aversiveness in predicting RSA. Three-way interactions test the Group × Minute-to-minute Aversiveness × Average Aversiveness on RSA. Although we could have constructed the reverse model (RSA predicting Aversiveness), we decided to predict RSA from behavior because participants can more easily observe one another’s behavior than physiological responses. All statistical tests were conducted in a single model. Results from the full APIM are presented in Table 1.
Figure 1.
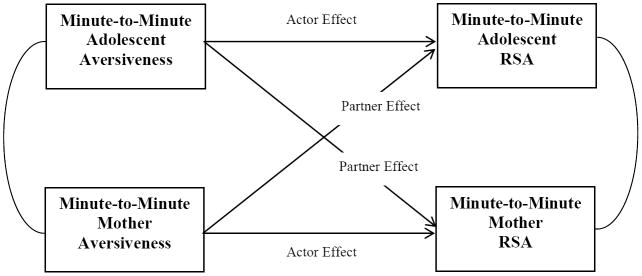
Level 1 model examining minute-to-minute concordance between behavioral and physiological dysregulation
Note: Group status, average aversiveness, and the group × average aversiveness interaction are modeled at Level 2 of the APIM. In this model, two- and three-way interactions occur across Level 1 and Level 2. Two-way interactions test group × minute-to-minute aversiveness on RSA. Three-way interactions test group × average aversiveness × minute-to-minute aversiveness on RSA.
Table 1.
Results of Actor-Partner Interdependence Model.
| Parameter | B | SE B | β |
|---|---|---|---|
| Teen intercept | |||
| Teen × Teen average aversiveness | -0.14 | 0.10 | -0.26 |
| Teen × Mother average aversiveness | -0.04 | 0.12 | -0.06 |
| Teen × Group | -0.15 | 0.18 | -0.16 |
| Teen × Teen average aversiveness × Group | 0.14 | 0.11 | 0.22 |
| Teen × Mother average aversiveness × Group | 0.16 | 0.14 | 0.21 |
|
| |||
| Teen momentary aversiveness actor effect | -0.03 | 0.03 | -0.03 |
| Teen momentary aversiveness actor effect × Teen average aversiveness | 0.04 | 0.02 | 0.05 |
| Teen momentary aversiveness actor effect × Mother average aversiveness | -0.05 | 0.04 | -0.06 |
| Teen momentary aversiveness actor effect × Group | 0.04 | 0.04 | 0.04 |
| Teen momentary aversiveness actor effect × Teen average aversiveness × Group | -0.08** | 0.03 | -0.08 |
| Teen momentary aversiveness actor effect × Mother average aversiveness × Group | 0.03 | 0.04 | 0.03 |
|
| |||
| Teen momentary aversiveness partner effect | 0.15*** | 0.04 | 0.13 |
| Teen momentary aversiveness partner effect × Teen average aversiveness | 0.02 | 0.03 | 0.02 |
| Teen momentary aversiveness partner effect × Mother average aversiveness | -0.12*** | 0.03 | -0.12 |
| Teen momentary aversiveness partner effect × Group | -0.14** | 0.05 | -0.10 |
| Teen momentary aversiveness partner effect × Teen average aversiveness × Group | -0.01 | 0.04 | -0.01 |
| Teen momentary aversiveness partner effect × Mother average aversiveness × Group | 0.12** | 0.04 | 0.10 |
|
| |||
| Mother intercept | |||
| Mother × Teen average aversiveness | 0.04 | 0.11 | 0.07 |
| Mother × Mother average aversiveness | -0.09 | 0.15 | -0.13 |
| Mother × Group | -0.01 | 0.20 | -0.01 |
| Mother × Teen average aversiveness × Group | -0.02 | 0.13 | -0.03 |
| Mother × Mother average aversiveness × Group | 0.06 | 0.17 | 0.08 |
|
| |||
| Mother momentary aversiveness actor effect | 0.03 | 0.05 | 0.03 |
| Mother momentary aversiveness actor effect × Teen average aversiveness | 0.01 | 0.06 | 0.01 |
| Mother momentary aversiveness actor effect × Mother average aversiveness | 0.08 | 0.06 | 0.08 |
| Mother momentary aversiveness actor effect × Group | -0.11* | 0.06 | -0.08 |
| Mother momentary aversiveness actor effect × Teen average aversiveness × Group | -0.02 | 0.07 | -0.02 |
| Mother momentary aversiveness actor effect × Mother average aversiveness × Group | -0.05 | 0.08 | -0.04 |
|
| |||
| Mother momentary aversiveness partner effect | -0.01 | 0.03 | -0.01 |
| Mother momentary aversiveness partner effect × Teen average aversiveness | -0.04 | 0.04 | -0.05 |
| Mother momentary aversiveness partner effect × Mother average aversiveness | -0.08** | 0.03 | -0.10 |
| Mother momentary aversiveness partner effect × Group | 0.01 | 0.04 | 0.01 |
| Mother momentary aversiveness partner effect × Teen average aversiveness × Group | 0.09 | 0.04 | 0.09 |
| Mother momentary aversiveness partner effect × Mother average aversiveness × Group | 0.11** | 0.03 | 0.12 |
Note: Robust standard errors reported;
p < .05,
p < .01,
p < .001.
Concordance between Teen Behavior and Teen RSA: Actor Effect
The actor effect refers to within-person concordance of aversiveness and RSA while accounting for the effect of partner aversiveness on RSA. When predicting teen RSA, a significant three-way interaction emerged for Teen’s Minute-to-minute aversiveness × Teen’s Average Aversiveness × Group (b = -0.08, p = 0.008). To interpret this effect, the interaction was decomposed by computing simple slopes for both the control and clinical groups at one SD above the mean, at the mean, and at one SD below the mean of teen’s average aversiveness. See Figure 2. This revealed that teens in the clinical group who were more aversive (i.e., the most aversive depressed adolescents) showed a concordant moment-to-moment association between behavior and RSA. Specifically, there was a negative association between aversiveness and RSA within epochs—RSA decreased during epochs in which these teens became more aversive (b = -0.08, p = 0.05). In other words, the most aversive depressed teens were physiologically dysregulated when their behavior was also dysregulated. However, minute-to-minute aversiveness was not related to RSA change for less aversive depressed teens or for teens in the control group. Thus, teens who were less aversive did not evidence within-person concordance between physiology and behavior.
Figure 2.

Three way interaction of within-person concordance for adolescents in the clinical group. Adolescents who were most aversive across the 10 min interaction task showed a negative association between minute-to-minute aversiveness and RSA reactivity.
Concordance between Mother Behavior and Mother RSA: Actor Effect
The actor effect for the mother is a test of within-person concordance between the mother’s behavior and her own RSA. There was a significant two-way interaction for mother Minute-to-minute Aversiveness × Group predicting mother RSA (b = -0.11, p = 0.04). Similar to the adolescents, mothers of depressed teens showed a negative association between aversiveness and behavior (b = -0.09, p = 0.003). Thus, clinical mothers showed expected within-person concordance between behavioral and emotional dysregulation, with RSA decreasing in epochs where their aversiveness increased. Control mothers, however, showed no minute-to-minute concordance between their behavior and their own RSA (b = 0.03, p = 0.57).
Concordance between Mother Behavior and Teen RSA: Partner Effect
The partner effect predicts teen RSA from mother behavior. A significant three-way interaction emerged for Mother Minute-to-minute Aversiveness × Mother Average Aversiveness × Group predicting teen RSA (b = 0.12, p = 0.008). This effect was decomposed as described above and is graphed in Figure 3. This revealed that teens in the control group whose mothers were less aversive showed a concordant RSA response to their mother’s aversiveness. However, as hypothesized, these teens showed RSA increases in epochs where their mothers became more aversive. This was true for control teens whose mothers scored low in aversiveness (b = 0.33, p = 0.001) or who were at the mean (b = 0.15, p = 0.001), but not for control teens whose mothers were highly aversive (b = -0.02, p = 0.5). There was no significant association between mother’s minute-to-minute aversiveness and teen RSA change scores for the clinical group.
Figure 3.

Three way interaction of between-person concordance for adolescents in the control group. When mothers scored low or at the mean on overall aversiveness across the 10 min interaction task, their adolescents showed a positive association between minute-to-minute aversiveness and RSA reactivity.
Concordance between Teen Behavior and Mother RSA: Partner Effect
The partner effect for mother RSA is a test of how her physiology is affected by her teen’s behavior. A significant three-way interaction emerged for Teen Minute-to-minute Aversiveness × Mother Average Aversiveness × Group on mother RSA (b = 0.11, p = 0.001). Decomposition revealed that control mothers who scored low on aversiveness showed concordance between their daughter’s behavior and their own RSA (b = 0.10, p = 0.049). As anticipated, as their daughters became more aversive, mother RSA increased, suggesting better regulation in the face of aversive teen behavior. However, for control mothers who were highly aversive, an unanticipated finding emerged. These mothers showed decreasing RSA to their daughter’s aversive behavior (b = -0.12, p = 0.013), which we expected of clinical mothers. Figure 4 illustrates concordant and discordant response patterns in clinical versus control participants.
Figure 4.
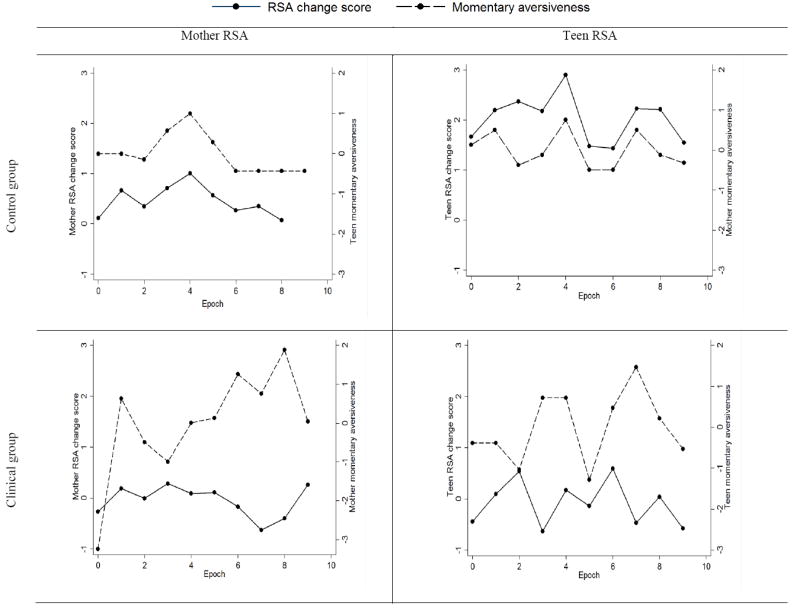
Plots of minute-to-minute aversiveness and RSA change scores.
Discussion
Developmental theorists assert that regulated and dysregulated behavior patterns emerge and persist within interpersonal relationships (Beauchaine & Zalewski, in press; Granic, Hollenstein, Dishion, & Patterson, 2003; Hollenstein, Granic, Stoolmiller, & Snyder, 2004). In some families, angry and coercive interactions are negatively reinforced over time because they are the most effective means of getting one’s needs met. These patterns often generalize to later peer and romantic relationships, contributing to interpersonal problems across development (Hughes et al., 2012; Kinsfogel & Grych, 2004). However, conflict is not necessarily problematic. In the context of a strong relationship, disagreement is an important step toward identifying and solving problems (Ubinger et al., 2013).Thus, emotional responses to anger or aversiveness may differ as a function of a person’s current emotional state, the nature of the relationship, and partner behavior in that moment.
Our findings revealed interesting patterns of concordance that were highly similar for mothers and daughters. In general, clinical participants showed physiological responses that tracked with their own behavior but not that of their partner. Furthermore, clinical participants generally showed the expected negative association between aversiveness and RSA. As behavior became more dysregulated, so did physiological responses. Control participants, on the other hand, had physiological response patterns that tracked with their partner’s behavior but not their own. In addition, they evidenced a distinct pattern of concordance, where they became physiologically more regulated in the face of aversive partner behavior. Although this is a concordant response, most researchers would assume the simple hypothesis—physiological and behavioral dysregulation should co-occur. Interestingly, emotion researchers have often theorized that unexpected patterns may emerge due to regulatory strategies (see Hollenstein and Lanteigne, this issue). However, there have been few studies that have examined whether this occurs naturally (i.e., regulation is not manipulated within the experiment) in response to complex social stimuli.
Decomposing these effects (see Figures 2 and 3) revealed more subtle differences in concordance as a function of the average aversiveness of dyad members across the interaction. Our interest in this was informed by theories that families are a dynamic system in which current states are likely to be highly similar to past states (Butler, 2011). Some developmental researchers have described these as “attractor states.” From this perspective, even though families could exhibit a limitless range of behavioral patterns, they often stabilize around a limited set of these possibilities (Granic & Hollenstein, 2003). We conceptualized average aversiveness as our index, albeit imperfect, of this phenomenon. Although best when measured dynamically, attractors can reflect “getting stuck” in certain states (see e.g., Hollenstein, Lichtwarck-Aschoff, & Potworowski, 2013). Such a phenomenon would be reflected in higher average aversiveness—revealing an important aspect of relationship quality.
As noted above, significant effects of average aversiveness were explored by examining differences between those who scored above, at, or below the mean. This allowed us to detect variability within group. For clinical dyads, only the most aversive depressed teens showed expected concordance between RSA and behavior—RSA decreases during minutes when they became more aversive. Post-hoc examination of the data revealed that this was not due to combining self-injuring and non-injuring participants into a single depressed sample (i.e., highly aversive teens were not only self-injurers; Fischer’s exact χ2=6.416, p = .171). This finding suggests that RSA decreases during stress were not a uniform response for depressed adolescents. Thus, some inconsistency in the literature on RSA and depression may be a function of variability within depressed samples (see Rottenberg, 2007 for a similar conclusion). One possibility is that RSA withdrawal to stress may only appear for depressed adolescents who are also dysregulated behaviorally.
Within the control group, there was also interesting variability. For teens whose mothers were less aversive, teen RSA increased with mother aversiveness. Similarly, in the same dyads where mothers were low on aversiveness, mother RSA increased in minutes when the teen became more aversive. This suggests that conflict may have provided an opportunity for self-regulation in dyads where the overall tone of the conflict was more positive. An interesting effect emerged, however, for control mothers who were most aversive. These mothers showed an effect similar to mothers in the clinical group. In minutes when their adolescent became more aversive, their RSA decreased. Thus, control mothers who were dysregulated behaviorally were also more likely to become dysregulated physiologically when their adolescent was more aversive, which may be due to unmeasured maternal psychopathology or emotion dysregulation.
Findings from this study should be interpreted in the context of several limitations. We tested a complicated APIM that included both two- and three-way interactions. We chose this model because it is consistent with theories of concordance and because the approach provides a parsimonious means of controlling for between-person effects when assessing within-person concordance and vice versa. However, it is important to replicate these two- and three-way interactions in future research. As with most psychophysiological studies, our sample size was likely underpowered to detect all higher order interactions. Some authors suggest that sample sizes of 200-1,000 would be required to ensure reliability and stability of findings (see Whisman & McClelland, 2005). In addition, our sample was all female and these results may not generalize to boys or fathers. Finally, our decision to combine self-injuring and depressed adolescents created a more heterogeneous depressed group and may have obscured some findings. We made an a priori decision to group clinical participants together in order to minimize the complexity of our statistical model and increase power to detect interactions. Self-injury and depression share features of emotion dysregulation and interpersonal distress and most studies of depression include similarly heterogeneous samples (e.g., Wilkinson, Kelvin, Roberts, Dubicka, & Goodyer, 2011). Thus, we did hypothesize nor test for distinct concordance patterns between depressed adolescents with and without a history of self-injury.
Recently, there has been strong interest in understanding emotions in social contexts (Connell, Hughes-Scalise, Klostermann, & Azem, 2011; Helm et al., 2012; Skowron, Cipriano-Essel, Benjamin, Pincus, & Van Ryzin, 2013). When emotions occur while one is alone, traditional intrapersonal theories may apply. However, in intimate relationships and other social contexts, emotions might be better understood as dynamic interpersonal experiences (Granic, 2000). Human emotions most often occur within such interpersonal contexts. This has motivated researchers to begin examining emotional experiences of dyads statistically (see Butler, 2011 for an extensive review). In light of this, it is important for theories of concordance to expand beyond individual response systems to incorporate dyads and larger social systems.
In addition to informing theories of emotion and concordance, these findings may also influence parenting research and intervention. Many treatments emphasize strategies for minimizing conflict between parents and children (e.g., Kastner & Wyatt, 2009). However, it is possible that reducing conflict is less important than teaching strategies to self-regulate during and after a fight. Persons with better self-control may be quicker to “repair” following conflict (e.g., apologize, joke, or solve the problem; see also Granic et al., 2007). Moreover, for some families, avoiding conflict may leave underlying problems unaddressed and unresolved. Future research should examine emotions in more naturalistic settings (e.g., home) and in the context of both conflict and reconciliation. Such work could reveal important differences not only in how families fight but how they come together.
Highlights.
We examined emotion dysregulation during mother-daughter conflict for depressed and typical adolescents
We collected respiratory sinus arrhythmia and coded behavioral dysregulation minute to minute for both mothers and daughters
Depressed adolescents and mothers became physiologically more dysregulated during minutes where they became behaviorally dysregulated (within-person concordance)
Control adolescents and mothers became physiologically more regulated during minutes where their dyad partner became behaviorally dysregulated (between-person concordance)
Footnotes
Under appropriate stimulus conditions (e.g., control of posture, respiration, movement), vagal efference to the heart can be estimated by RSA and psychological interpretation is possible (see Ritz, 2009; Zisner & Beauchaine, in press). When ideal conditions are not met, RSA may nevertheless be a useful marker of clinical state. For example, deficiencies in RSA appear to index emotion dysregulation across a wide range of psychiatric disorders (see Zisner & Beauchaine, in press).
The difference between actor and partner is depicted in Figure 1, which illustrates the theoretical model tested by this formula.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Allen NB, Kuppens P, Sheeber LB. Heart rate responses to parental behavior in depressed adolescents. Biological Psychology. 2012;90:80–87. doi: 10.1016/j.biopsycho.2012.02.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4. Washington, DC: Author; 2000. text revision. [Google Scholar]
- Beauchaine TP. Vagal tone, development, and Gray’s motivational theory: Toward an integrated model of autonomic nervous system functioning in psychopathology. Development and Psychopathology. 2001;13:183–214. doi: 10.1017/S0954579401002012. [DOI] [PubMed] [Google Scholar]
- Beauchaine TP. Physiological markers of emotion and behavior dysregulation in externalizing psychopathology. Monographs of the Society for Research in Child Development. 2012;77:79–86. doi: 10.1111/j.1540-5834.2011.00665.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Gatzke-Kopp L, Mead HK. Polyvagal theory and developmental psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology. 2007;74:174–184. doi: 10.1016/j.biopsycho.2005.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Gatzke-Kopp LM. Instantiating the multiple levels of analysis perspective in a program of study on externalizing behavior. Development and Psychopathology. 2012;24:1003–1018. doi: 10.1017/S0954579412000508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, McNulty T. Comorbidities and continuities as ontogenic processes: Toward a developmental spectrum model of externalizing psychopathology. Developmental and Psychopathology. 2013;25:1505–1528. doi: 10.1017/S0954579413000746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beauchaine TP, Zalewski M. Physiological and developmental mechanisms of emotional lability in coercive relationships. In: Dishion TJ, Snyder JJ, editors. Oxford handbook of coercive relationship dynamics. New York: Oxford University Press; in press. [Google Scholar]
- Berntson GG, Bigger JT, Eckberg DL, Grossman P, Kaufmann PG, Malik M, Van der Molen MW, et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology. 1997;34:623–648. doi: 10.1111/j.1469-8986.1997.tb02140.x. [DOI] [PubMed] [Google Scholar]
- Butler EA. Temporal interpersonal emotion systems: The “TIES” that form relationships. Personality and Social Psychology Review. 2011;15:367–393. doi: 10.1177/1088868311411164. [DOI] [PubMed] [Google Scholar]
- Butler EA, Randall AK. Author reply: Coregulation is a state of a temporal interpersonal emotion system. Emotion Review. 2013;5:213–214. doi: 10.1177/1754073912451632. [DOI] [Google Scholar]
- Cacioppo JT, Berntson GG, Klein DJ. What is an emotion? The role of somatovisceral afference, with speical emphasis on somtovisceral “illusions”. In: Clark MS, editor. Emotion and social behavior. Thousand Oaks, CA: Sage; 1992. pp. 63–89. [Google Scholar]
- Calkins SD. Commentary: Conceptual and methodological challenges to the study of emotion regulation and psychopathology. Journal of Psychopathology and Behavioral Assessment. 2010;32:92–95. doi: 10.1007/s10862-009-9169-6. [DOI] [Google Scholar]
- Campos JJ, Campos RG, Barrett KC. Emergent themes in the study of emotional development and emotion regulation. Developmental Psychology. 1989;25:394–402. doi: 10.1037/0012-1649.25.3.394. [DOI] [Google Scholar]
- Carney RM, Freedland KE, Stein PK, Skala JA, Hoffman P, Jaffe AS. Change in heart rate and heart ratve variability during treatment for depression in patients with coronary heart disease. Psychosomatic Medicine. 2000;62:639–647. doi: 10.1097/00006842-200009000-00007. [DOI] [PubMed] [Google Scholar]
- Cassidy J. Emotion regulation: Influences of attachment relationships. Monographs of the Society for Research in Child Development. 1994;59:228–249. doi: 10.1111/j.1540-5834.1994.tb01287.x. [DOI] [PubMed] [Google Scholar]
- Coan JA. Adult attachment and the brain. Journal of Social and Personal Relationships. 2010;27:210–217. doi: 10.1177/0265407509360900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coan JA, Kasle S, Jackson A, Schaefer HS, Davidson RJ. Mutuality and the social regulation of neural threat responding. Attachment and Human Development. 2013;15:303–315. doi: 10.1080/14616734.2013.782656. doi:org/10.1080/14616734.2013.782656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole PM, Hall SE, Hajal NJ. Emotion dysregulation as a risk factor for psychopathology. In: Beauchaine TP, Hinshaw SP, editors. Child and adolescent psychopathology. 2. Hoboken, NJ: Wiley; 2013. pp. 341–373. [Google Scholar]
- Cole PM, Martin SE, Dennis TA. Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child Development. 2004;75:317–333. doi: 10.1111/j.1467-8624.2004.00673.x. [DOI] [PubMed] [Google Scholar]
- Connell AM, Hughes-Scalise A, Klostermann S, Azem T. Maternal depression and the heart of parenting: Respiratory sinus arrhythmia and affective dynamics during parent–adolescent interactions. Journal of Family Psychology. 2011;25:653–662. doi: 10.1037/a0025225. [DOI] [PubMed] [Google Scholar]
- Crowell S, Beauchaine T, Hsiao R, Vasilev C, Yaptangco M, Linehan M, McCauley E. Differentiating adolescent self-injury from adolescent depression: Possible implications for borderline personality development. Journal of Abnormal Child Psychology. 2012;40:45–57. doi: 10.1007/s10802-011-9578-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crowell SE, Baucom BR, McCauley E, Potapova NV, Fitelson M, Barth H, Beauchaine TP, et al. Mechanisms of contextual risk for adolescent self-injury: Invalidation and conflict escalation in mother–child interactions. Journal of Clinical Child and Adolescent Psychology. 2013;42:467–480. doi: 10.1080/15374416.2013.785360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Crowell SE, Beauchaine TP, McCauley E, Smith C, Stevens AL, Sylvers PD. Psychological, physiological, and serotonergic correlates of parasuicidal behavior among adolescent girls. Development and Psychopathology. 2005;17:1105–1127. doi: 10.1017/s0954579405050522. doi:10.10170S0954579405050522. [DOI] [PubMed] [Google Scholar]
- Crowell SE, Skidmore CR, Rau HK, Williams PG. Psychosocial stress, emotion regulation, and resilience in adolescence. In: O’Donohue WT, Benuto LT, Toole LW, editors. Handbook of Adolescent Health Psychology. New York: Springer; 2013. pp. 129–142. [Google Scholar]
- Davies PT, Cummings EM. Marital conflict and child adjustment: An emotional security hypothesis. Psychological Bulletin. 1994;116:387–411. doi: 10.1037/0033-2909.116.3.387. [DOI] [PubMed] [Google Scholar]
- Diamond LM, Aspinwall LG. Emotion regulation across the life span: An integrative perspective emphasizing self-regulation, positive affect, and dyadic processes. Motivation and Emotion. 2003;27:125–156. doi: 10.1023/A:1024521920068. [DOI] [Google Scholar]
- Eisenberg N. Emotion, regulation, and moral development. Annual Review of Psychology. 2000;51:665–697. doi: 10.1146/annurev.psych.51.1.665. [DOI] [PubMed] [Google Scholar]
- Ekman P. An argument for basic emotions. Cognition and Emotion. 1992;6:169–200. [Google Scholar]
- Ekman P. Basic emotions. In: Dalgeish T, Power M, editors. Handbook of Cognition and Emotion. New York: Wiley; 1999. [Google Scholar]
- Ekman P, Friesen WV. Measuring facial movement. Environmental Psychology and Nonverbal Behavior. 1976;1:56–75. [Google Scholar]
- Enders CK, Tofighi D. Centering predictor variables in cross-sectional multilevel models: A new look at an old issue. Psychological Methods. 2007;12:121–138. doi: 10.1037/1082-989X.12.2.121. [DOI] [PubMed] [Google Scholar]
- Fortunato C, Gatzke-Kopp L, Ram N. Associations between respiratory sinus arrhythmia reactivity and internalizing and externalizing symptoms are emotion specific. Cognitive, Affective, and Behavioral Neuroscience. 2013;13:238–251. doi: 10.3758/s13415-012-0136-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granic I, Hollenstein T. Dynamic systems methods for models of developmental psychopathology. Development and Psychopathology. 2003;15:641–669. doi: 10.1017/S0954579403000324. [DOI] [PubMed] [Google Scholar]
- Granic I, Hollenstein T, Dishion TJ, Patterson GR. Longitudinal analysis of flexibility and reorganization in early adolescence: A dynamic systems study of family interactions. Developmental Psychology. 2003;39:606–617. doi: 10.1037/0012-1649.39.3.606. [DOI] [PubMed] [Google Scholar]
- Gross JJ. The emerging field of emotion regulation: An integrative review. Review of General Psychology. 1998;2:271–299. doi: 10.1037/1089-2680.2.3.271. [DOI] [Google Scholar]
- Helm JL, Sbarra D, Ferrer E. Assessing cross-partner associations in physiological responses via coupled oscillator models. Emotion. 2012;12:748–762. doi: 10.1037/a0025036. [DOI] [PubMed] [Google Scholar]
- Hinnant JB, Elmore-Staton L, El-Sheikh M. Developmental trajectories of respiratory sinus arrhythmia and pre-ejection period in middle childhood. Developmental Psychobiology. 2011;53:59–68. doi: 10.1002/dev.20487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofer MA. Hidden regulators: Implications for a new understanding of attachment, separation, and loss. In: Goldberg S, Muir R, Kerr J, editors. Attachment theory: Social, developmental, and clinical perspectives. New York: Routledge; 1995. pp. 203–230. [Google Scholar]
- Hollenstein T, Granic I, Stoolmiller M, Snyder J. Rigidity in parent-child interactions and the development of externalizing and internalizing behavior in early childhood. Journal of Abnormal Child Psychology. 2004;32:595–607. doi: 10.1023/B:JACP.0000047209.37650.41. [DOI] [PubMed] [Google Scholar]
- Hubbard JA, Parker EH, Ramsden SR, Flanagan KD, Relyea N, Dearing KF, Smithmyer CM, Simons RF, Hyde CT. The relations among observational, physiological, and self-report measures of children’s anger. Social Development. 2004;13:14–39. doi: 10.1111/j.1467-9507.2004.00255.x. [DOI] [PubMed] [Google Scholar]
- Hughes AE, Crowell SE, Uyeji L, Coan JA. A developmental neuroscience of borderline pathology: Emotion dysregulation and social baseline theory. Journal of Abnormal Child Psychology. 2012;40:21–33. doi: 10.1007/s10802-011-9555-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kashy DA, Donnellan MB. Conceptual and methodological issues in the analysis of data from dyads and groups. In: Deaux K, Snyder M, editors. The Oxford Handbook of Personality and Social Psychology. New York: Oxford; 2012. pp. 209–238. [Google Scholar]
- Kastner LS, Wyatt J. Getting to calm: Cool-headed strategies for parenting tweens and teens. Seattle, WA: ParentMap; 2009. [Google Scholar]
- Kenny DA, Kashy DA, Cook WL. Dyadic data analysis. New York: Guilford; 2006. [Google Scholar]
- Kinsfogel KM, Grych JH. Interparental conflict and adolescent dating relationships: Integrating cognitive, emotional, and peer influences. Journal of Family Psychology. 2004;18:505–515. doi: 10.1037/0893-3200.18.3.505. [DOI] [PubMed] [Google Scholar]
- Lanteigne DM, Flynn JJ, Eastabrook JM, Hollenstein T. Discordant patterns among emotional experience, arousal and expression in adolescence: Relations with emotion regulation and internalizing problems. Canadian Journal of Behavioural Science. 2012 doi: 10.1037/a0029968. [DOI] [Google Scholar]
- Levenson RW. Human emotions: A funcitonal view. In: Ekman P, Davidson RJ, editors. The nature of emotion: Fundamental questions. New York: Oxford University Press; 1994. pp. 123–126. [Google Scholar]
- Lewinsohn PM, Hops H, Roberts RE, Seeley JR, Andrews JA. Adolescent psychopathology: I. Prevalence and incidence of depression and other DSM-III—R disorders in high school students. Vol. 102. US: American Psychological Association; 1993. pp. 133–144. [DOI] [PubMed] [Google Scholar]
- Linehan MM. Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford; 1993. [Google Scholar]
- Marsh P, Beauchaine TP, Williams B. Dissociation of sad facial expressions and autonomic nervous system responding in boys with disruptive behavior disorders. Psychophysiology. 2008;45:100–110. doi: 10.1111/j.1469-8986.2007.00603.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mauss IB, Levenson RW, McCarter L, Wilhelm FH, Gross JJ. The tie that binds? Coherence among emotion experience, behavior, and physiology. Emotion. 2005;5:175–190. doi: 10.1037/1528-3542.5.2.175. [DOI] [PubMed] [Google Scholar]
- Morris AS, Silk JS, Steinberg L, Myers SS, Robinson LR. The role of the family context in the development of emotion regulation. Social Development. 2007;16:361–388. doi: 10.1111/j.1467-9507.2007.00389.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nock MK. Self-injury. 2010;6:339–363. doi: 10.1146/annurev.clinpsy.121208.131258. [DOI] [PubMed] [Google Scholar]
- Pang KC, Beauchaine TP. Longitudinal patterns of autonomic nervous system responding to emotion evocation among children with conduct problems and/or depression. Developmental Psychobiology. doi: 10.1002/dev.21065. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patterson GR, DeBaryshe BD, Ramsey E. A developmental perspective on antisocial behavior. American Psychologist. 1989;44:329–335. doi: 10.1037/0003-066X.44.2.329. [DOI] [PubMed] [Google Scholar]
- Patterson GR, Dishion TJ, Bank L. Family interaction: A process model of deviancy training. Aggressive Behavior. 1984;10:253–267. [Google Scholar]
- Pietromonaco PR, Uchino B, Dunkel Schetter C. Close relationship processes and health: Implications of attachment theory for health and disease. Health Psychology. 2013;32:499–513. doi: 10.1037/a0029349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porges SW. Orienting in a defensive world: Mammalian modifications of our evolutionary heritage. A polyvagal theory. Psychophysiology. 1995;32:301–318. doi: 10.1111/j.1469-8986.1995.tb01213.x. [DOI] [PubMed] [Google Scholar]
- Porges SW. Emotion: An evolutionary by-product of the neural regulation of the autonomic nervous system. Annals New York Academy of Sciences. 1997;807:62–77. doi: 10.1111/j.1749-6632.1997.tb51913.x. [DOI] [PubMed] [Google Scholar]
- Porges SW. The polyvagal theory: Phylogenetic contributions to social behavior. Physiology and Behavior. 2003;79:503–513. doi: 10.1016/s0031-9384(03)00156-2. http://dx.doi.org/10.1016/S0031-9384(03)00156-2. [DOI] [PubMed] [Google Scholar]
- Porges SW. The polyvagal perspective. Biological Psychiatry. 2007;74:116–143. doi: 10.1016/j.biopsycho.2006.06.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Porges SW, Doussard-Roosevelt JA, Portales AL, Greenspan SI. Infant regulation of the vagal brake predicts child behavior problems: A psychobiological model of social behavior. Developmental Psychobiology. 1996;29:697–712. doi: 10.1002/(SICI)1098-2302(199612)29:8<697::AID-DEV5>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- Prinz RJ, Foster S, Kent RN, O’Leary KD. Multivariate assessment of conflict in distressed and nondistressed mother-adolescent dyads. Journal of Applied Behavior Analysis. 1979;12:691–700. doi: 10.1901/jaba.1979.12-691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qu M, Zhang Y, Webster JG, Tompkins WJ. Motion artifact from spot and band electrodes during impedance cardiography. IEEE Transactions on Bio-medical Engineering. 1986;33:1029–1036. doi: 10.1109/TBME.1986.325869. [DOI] [PubMed] [Google Scholar]
- Raudenbush SW, Bryk AS, Congdon RT. HLM 7: Hierarchical linear and nonlinear modeling. Chicago: Scientific Software International; 2011. [Google Scholar]
- Reis HT, Collins WA, Berscheid E. The relationship context of human behavior and development. Psychological Bulletin. 2000;126:844–872. doi: 10.1037/0033-2909.126.6.844. [DOI] [PubMed] [Google Scholar]
- Reisenzein R. Exploring the strength of association between the components of emotion syndromes: The case of surprise. Cognition and Emotion. 2000;8 doi: 10.1080/026999300378978. [DOI] [Google Scholar]
- Reisenzein R, Studtmann M, Horstmann G. Coherence between emotion and facial expression: Evidence from laboratory experiments. Emotion Review. 2013;5:16–23. doi: 10.1177/1754073912457228. [DOI] [Google Scholar]
- Ritz T. Studying noninvasive indices of vagal control: The need for respiratory control and the problem of target specificity. Biological Psychology. 2009;80:158–168. doi: 10.1016/j.biopsycho.2008.08.003. [DOI] [PubMed] [Google Scholar]
- Rottenberg J. Cardiac vagal control in depression: A critical analysis. Biological Psychology. 2007;74:200–211. doi: 10.1016/j.biopsycho.2005.08.010. http://dx.doi.org/10.1016/j.biopsycho.2005.08.010. [DOI] [PubMed] [Google Scholar]
- Rottenberg J, Chambers AS, Allen JJB, Manber R. Cardiac vagal control in the severity and course of depression: The importance of symptomatic heterogeneity. Journal of Affective Disorders. 2007;103:173–179. doi: 10.1016/j.jad.2007.01.028. http://dx.doi.org/10.1016/j.jad.2007.01.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skowron EA, Cipriano-Essel E, Benjamin LS, Pincus AL, Van Ryzin MJ. Cardiac vagal tone and quality of parenting show concurrent and time-ordered associations that diverge in abusive, neglectful, and non-maltreating mothers. Couple and Family Psychology: Research and Practice. 2013;2:95–115. doi: 10.1037/cfp0000005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder J, Edwards P, McGraw K, Kilgore K. Escalation and reinforcement in mother-child conflict: Social processes associated with the development of physical aggression. Development and Psychopathology. 1994;6:305–321. http://dx.doi.org/10.1017/S0954579400004600. [Google Scholar]
- Stubbs J, Crosby L, Forgatch MS, Capaldi DM. Family and peer process code: A synthesis of three Oregon Social Learning Center behavior codes. Oregon Social Learning Center; Eugene, OR: 1998. [Google Scholar]
- Ubinger ME, Handal PJ, Massura CE. Adolescent adjustment: The hazards of conflict avoidance and the benefits of conflict resolution. Psychology. 2013;4:50–58. doi: 10.4236/psych.2013.41007. [DOI] [Google Scholar]
- Wilkinson P, Kelvin R, Roberts C, Dubicka B, Goodyer I. Clinical and psychosocial predictors of suicide attempts and nonsuicidal self-injury in the adolescent depression antidepressants and psychotherapy trial (ADAPT) American Journal of Psychiatry. 2011;168:495–501. doi: 10.1176/appi.ajp.2010.10050718. [DOI] [PubMed] [Google Scholar]
- Zisner AR, Beauchaine TP. Psychophysiological methods and developmental psychopathology. In: Cicchetti D, editor. Developmental psychopathology. 3. Hoboken, NJ: Wiley; in press. [Google Scholar]