

Abstract
Individuals with primary progressive aphasia (PPA) suffer a gradual decline in communication ability as a result of neurodegenerative disease. Language treatment shows promise as a means of addressing these difficulties but much remains to be learned with regard to the potential value of treatment across variants and stages of the disorder. We present two cases, one with semantic variant of PPA and the other with logopenic PPA, each of whom underwent treatment that was unique in its focus on training self-cueing strategies to engage residual language skills. Despite differing language profiles and levels of aphasia severity, each individual benefited from treatment and showed maintenance of gains as well as generalization to untrained lexical items. These cases highlight the potential for treatment to capitalize on spared cognitive and neural systems in individuals with PPA, improving current language function as well as potentially preserving targeted skills in the face of disease progression.
Keywords: primary progressive aphasia, rehabilitation, treatment, naming, lexical retrieval, logopenic variant, semantic dementia
1. INTRODUCTION
Primary progressive aphasia (PPA) is a neurological condition wherein speech and language deteriorate as a result of neurodegenerative disease affecting areas of the brain that support communication. Three variants of PPA are now widely accepted by the clinical and research communities (Gorno-Tempini et al., 2011). These include a semantic variant (svPPA), with degradation of the semantic system that results in loss of word and object knowledge; a logopenic variant (lvPPA), with impairments in naming and repetition that are phonological in nature; and a nonfluent/agrammatic variant (nfvPPA), which is characterized by syntactic impairments and motor speech deficits.
PPA is associated with atrophy affecting the language-dominant (typically left) hemisphere to a greater extent than the non-dominant hemisphere (Gorno-Tempini et al., 2004; Grossman et al., 1996; Hodges, Patterson, Oxbury, & Funnell, 1992; Mesulam, 1982). Each of the three variants of PPA is characterized by distinct patterns of atrophy and the unique speech-language syndromes that emerge are understood to reflect the topography of damage in the brain (Gorno-Tempini et al., 2011). The multimodal semantic deficits observed in svPPA are associated with atrophy in the antero-lateral temporal lobe (left greater than right), a region widely viewed to be a cortical “hub” for word and object concepts (Hodges & Patterson, 2007; Lambon Ralph, Sage, Jones, & Mayberry, 2010). By contrast, in lvPPA, atrophy is observed in posterior perisylvian cortex in the left hemisphere, a region implicated in phonological processes critical to comprehension and production of language (Gorno-Tempini et al., 2008; Henry & Gorno-Tempini, 2010). Finally, individuals with the nonfluent variant present with atrophy in left inferior frontal regions implicated in speech production and grammar (Wilson et al., 2010a).
Lexical retrieval impairment arises in each of the three variants of PPA, however, anomia is a prominent and early feature in the semantic and logopenic variants only, with sparing of word retrieval in nfvPPA until relatively advanced stages (Gorno-Tempini et al., 2011; Gorno-Tempini et al., 2004). In svPPA, degraded semantic knowledge is thought to weaken access to intact phonological representations (Lambon Ralph, McClelland, Patterson, Galton, & Hodges, 2001). By contrast, individuals with lvPPA present with phonological deficits (diminished phonological working memory and phonological paraphasias) and largely spared semantic processing (Gorno-Tempini et al., 2008; Wilson et al., 2010b). This profile suggests that lexical retrieval in these patients may be disrupted at a post-semantic or phonological stage. As such, conceptual knowledge is intact and available, but phonological representations are insufficiently accessed or assembled, as is observed in individuals with phonological impairments in the context of aphasia due to stroke (Lambon Ralph, Moriarty, & Sage, 2002; Schwartz, Dell, Martin, Gahl, & Sobel, 2006).
Relative to the hundreds of studies examining treatment for speech and language impairments resulting from vascular lesions, the treatment literature in PPA is rather modest. The bulk of this work has addressed naming difficulty in svPPA, with only a couple of studies examining treatment in lvPPA. In svPPA, most studies have implemented treatment protocols wherein a picture or definition was rehearsed in conjunction with the written word form to encourage co-activation of semantic and orthographic/phonological representations (Graham, Patterson, Pratt, & Hodges, 1999; Graham, Patterson, Pratt, & Hodges, 2001; Heredia, Sage, Lambon Ralph, & Berthier, 2009; Mayberry, Sage, Ehsan, & Lambon Ralph, 2011; Snowden & Neary, 2002). This approach has also been modified to include a personalized or autobiographical cue, in hopes of capitalizing on relatively spared episodic memory systems to support word retrieval (Jokel, Rochon, & Leonard, 2002; Jokel, Rochon, & Leonard, 2006; Snowden & Neary, 2002). Treatment outcomes from these studies reveal significantly improved naming for trained items, with some degree of maintenance up to six months post-treatment in two cases (Heredia et al., 2009; Jokel et al, 2006). Together, this work served to confirm that relearning of verbal labels in individuals with svPPA is possible. However, gains were typically item- and context-specific, suggesting that retrieval of lexical items becomes reliant on episodic memory when semantic representations are degraded. Notably, this type of learning may have unintended consequences, with residual input from a degraded semantic system resulting in training-induced semantic errors, as evidenced by over-generalization of relearned labels to semantically-related items (Mayberry, Sage, Ehsan, & Lambon Ralph, 2011).
Other work with svPPA utilized more elaborated cueing hierarchies to prompt or support lexical retrieval (Bier et al., 2009; Dressel et al., 2010; Jokel, Rochon, & Anderson, 2010; Jokel & Anderson, 2012; Newhart et al., 2009). These studies, which incorporated a variety of semantic, phonological, and orthographic cues, report improvements in naming performance, with generalization to untrained items in some cases (Jokel, Rochon, & Anderson, 2010; Jokel & Anderson, 2012) and maintenance of gains for two or more months post-treatment in several studies (Dressel et al., 2010; Jokel, Rochon, & Anderson, 2010; Jokel & Anderson, 2012). These findings indicate that a variety of cueing modalities may be beneficial in svPPA. In fact, a study directly comparing the effects of semantic versus phonological cueing approaches found both to have therapeutic value for a single participant with svPPA (Dressel et al., 2010). That study also reported changes in activation patterns on post-treatment fMRI, indicating that both semantic and phonological approaches resulted in training-induced functional reorganization of the language network.
Studies of naming treatment for individuals with the logopenic variant of PPA (lvPPA) are more limited, with only a handful of published cases. In addition to their participant with svPPA, Newhart and colleagues (2009) implemented their cueing hierarchy with an individual diagnosed with lvPPA. Their treatment, which involved written naming, searching for target items in a training notebook, reading, and repetition, resulted in significant improvement for trained items and generalization to untrained words, which the authors attributed to improved access to phonological word forms. Another study examined effects of a brief but intensive treatment for lexical retrieval in an individual with lvPPA, which included semantic elaboration training and massed practice in the context of generative naming tasks (Beeson et al., 2011). The treatment resulted in significant and generalized improvements in naming that were observed up to six months after treatment. In addition, functional MRI documented pre- to post-treatment changes in brain activation patterns that suggested increased engagement of preserved regions of the language network after treatment.
Taken together, research suggests that implementation of appropriate behavioral intervention may result in improved language performance in PPA. As described above, various forms of naming treatment, incorporating both semantic and phonological approaches, have proven beneficial. The reports that demonstrated stronger generalizability and durability of gains typically engaged multiple central language processing components (semantics, phonology, and orthography; Beeson et al., 2011; Newhart et al., 2009; Jokel & Anderson, 2012) and two of these studies (Beeson et al., 2011; Newhart et al., 2009) were unique in training the use of strategies such as semantic and orthographic self-cueing, which were intended to promote generalization. In this paper, we examine a treatment protocol designed to train a sequence of self-directed cueing strategies to aid in word retrieval for both trained and untrained items.
We describe implementation and outcomes of language treatment for two individuals with PPA, one with svPPA and another with lvPPA. The two syndromes differ with regard to location of neurodegeneration and specific aspects of the language phenotype. They have in common, however, the salient feature of anomia. In treating these two individuals, we aimed to capitalize on spared cognitive and neural systems by implementing treatment that promoted the use of residual semantic, phonological, and orthographic information. The two participants were treated in different laboratories, using protocols that were similar but not identical, accommodating the unique needs of each individual and the constraints of each context. The cases are presented here as a means to illustrate treatment methods and outcomes that are promising for this population.
2. METHODS
2.1 Participants and Assessment Measures
The two individuals who participated in this study were each evaluated with comprehensive measures of speech, language, and cognition (Table 1). In addition, they received high-resolution brain scans that were analyzed using voxel-based morphometry (VBM) to reveal the pattern of cortical atrophy relative to healthy controls (for detailed methods and VBM results, see supplemental online material). For this report, we focus on the behavioral characteristics and imaging findings that served to confirm the progressive aphasia profile and establish language performance prior to the implementation of treatment.
Table 1.
Demographic data and pre-treatment performance of participants with primary progressive aphasia of the semantic variant (SV) and the logopenic variant (LV).
| Semantic PPA (SV) | Logopenic PPA (LV) | Normative Data Mean Score (SD) | |
|---|---|---|---|
| Age | 60 | 54 | - |
| Education (years) | 20 | 12 | - |
| WAB Aphasia Quotient (100) | 90.2 | 69.4 | ≥93.8 |
| Information content (10) | 9 | 8 | - |
| Fluency (10) | 9 | 6 | - |
| Comprehension (10) | 10 | 8.6 | - |
| Repetition (10) | 9.6 | 6.1 | - |
| Naming (10) | 7.5 | 6 | - |
| Boston Naming Test (60) | 19 | 27 | 54.9a (4.3) |
| Pyramids & Palm Trees: Pictures (52) | 47 | 52 | 50.9b (1.14) |
| Pyramids & Palm Trees: Written (52) | 48 | 52 | 50.8b (1.38) |
| MMSE (30) | 29 | 20 | 28c (2.4) |
| Digit Span Forward | 8 | 3 | 7.2d (0.9) |
| Digit Span Backward | 4 | 2 | 5.4d (1.3) |
| ABRSe Reading: Words | 96.3% | 96.3% | 98.8%b (3.6; ) |
| ABRS Reading: Nonwords | 90.0% | 80.0% | 95.6%b (7.3) |
| ABRS Spelling: Words | 82.5% | 32.5% | 95.5%b (10.4) |
| ABRS Spelling: Nonwords | 60.0% | 40.0% | 91.1%b (15.9) |
Normative Data for males ages 25–88 years, from Tombaugh, T.N. & Hubiey, A.M. (1997).
Normative data from University of Arizona Aphasia Research Project; 34 healthy adults, mean age = 62.9 (11.4), range 34–85; mean education = 15.8 years (2.8), range 12–22 years. Male: Female 13:21
MMSE Norms for ages 50–54 from Crum, R., Anthony, J., Bassett, S. & Folstein, M. (1993).
Normative data from UCSF Memory and Aging Center Bedside Neuropsychological Screen (Kramer et al., 2003)
Arizona Battery for Reading and Spelling (ABRS; Beeson & Rising, 2010)
2.1.1 Case 1: Semantic Variant (SV)
SV was a 60-year-old left-handed man who reported a year-and-a-half history of language difficulty. A doctor of veterinary medicine, he had 20 years of education and was still working at the time of the initial evaluation. SV was in the process of arranging his retirement due to increasing difficulty with word retrieval and his growing uncertainty regarding word meanings, in particular, those related to diagnosing and treating the animals under his care. At the time of the initial evaluation at the University of Arizona, SV’s primary complaint was impaired word retrieval, which he described as “when I’m talking, the next word disappears out of my brain.” He also described increasing difficulty with spelling, indicating that he was an excellent speller prior to the onset of his current deficits. SV’s conversational speech was fluent, with pauses for lexical retrieval, and some circumlocution during instances of anomia. Family history revealed that SV’s mother had early onset dementia in her sixties.
A comprehensive neuropsychological evaluation was completed 4 months prior to SV’s evaluation in our lab. The report from this evaluation indicated average intellectual functioning with a relative weakness in verbal convergent reasoning. Severely impaired confrontation naming was noted, as was mildly impaired verbal fluency. SV’s performance on the neuropsychological battery also revealed low average to mildly impaired performance on verbal and visual memory tasks, and performance on visual construction tasks ranging from low average to superior.
2.1.1.1 Behavioral and Imaging Characteristics
At the time of his initial evaluation at the University of Arizona, SV demonstrated no evidence of apraxia of speech or dysarthria. With regard to language, his performance on the Western Aphasia Battery (WAB; Kertesz, 1982) was consistent with mild anomic aphasia (Table 1; Aphasia Quotient = 90.2). His spontaneous speech was fluent, with normal grammar, and he demonstrated frequent circumlocution and word substitutions during instances of anomia. Naming impairment was particularly evident on the Boston Naming Test (BNT; Kaplan, Goodglass & Weintraub 2001), on which he correctly produced only 19 of 60 items, and the object naming subtest of the WAB (39/60 points; 11/20 objects named without cues). During instances of lexical retrieval difficulty, SV often stated he could not recall the word (39% of errors on the BNT). In other instances, he made comments that did not contain meaningful semantic information (e.g., “I have this at home”; 10% of errors). He provided meaningful semantic information in some cases (34% of errors), but this information typically consisted of a single semantic feature (a racquet is “used in sports”; a harp is “a musical instrument”) that rarely prompted retrieval of the correct name.
Several semantic tests were administered to examine the status of SV’s conceptual knowledge. He demonstrated impairment on the picture and written versions of the Pyramids and Palm Trees Test (PPT; Howard & Patterson, 1992) (< 1st percentile). His semantic difficulty was also evident on the Similarities subtest of the Wechsler Adult Intelligence Scale-IV (WAIS-IV; Wechsler, 2008), which requires a description of commonalities between two words (16th percentile).
SV’s single-word reading was relatively strong (77/80 correct for words; 18/20 for nonwords), but spelling performance was poorer (66/80 correct for real words) and likely impaired relative to pre-morbid performance, per SV’s report of changes in spelling ability. Most spelling errors were on low frequency, irregularly spelled words, which SV spelled in a phonologically-plausible manner (e.g., vage for vague; yaut for yacht). Despite a phonological approach to spelling real words, SV demonstrated some difficulty spelling nonwords (12/20; example errors include molfer for mofer and scraight for squate). He had no difficulties with visual processing of orthographic stimuli, as judged on tests of letter-form knowledge (e.g., letter orientation judgments and lexical decision tasks) from the Psycholinguistic Assessment of Language Performance in Aphasia (PALPA; Kay, Lesser, & Coltheart, 1992).
SV’s marked anomia and mild written language impairment were observed in the context of relatively preserved memory and nonverbal cognition. Performance on the Mini-Mental State Examination (MMSE; Folstein, Folstein, & McHugh, 1975) was within normal limits (29/30). Nonverbal visual problem solving was well preserved, as measured by the Coloured Progressive Matrices (Raven, Court, & Raven, 1990) with a score of 33/36 (~75th percentile). Performance on the Warrington Recognition Memory Test (Warrington, 1984) was similar for words and faces, with scores of 46/50 and 44/50, respectively (~75th percentile for each task).
The analysis of SV’s high-resolution brain scan revealed significant cortical atrophy in the left anterior temporal lobe (see supplemental material). The atrophy pattern and cognitive-linguistic profile were consistent with the semantic variant of PPA, as highlighted in Table 2. The extent of atrophy and the behavioral profile reflected a relatively early stage of the disease process.
Table 2.
Behavioral characteristics and imaging findings associated with semantic and logopenic variants of PPA (Gorno-Tempini et al., 2011) relative to participants SV and LV.
| Features Common to Semantic and Logopenic Variants | SV | LV |
|---|---|---|
| Behavioral Characteristics
| ||
| impaired naming | Y | Y |
| preserved motor speech control | Y | Y |
| preserved grammatical competence | Y | Y |
|
Features associated with Semantic variant
| ||
| Behavioral Characteristics
| ||
| impaired single word comprehension | Y | N |
| poor object knowledge | N | N |
| surface dyslexia/dysgraphia | Y | N |
| spared repetition | Y | N |
| Imaging findings
| ||
| asymmetrical (L>R) anterior temporal lobe atrophy and/or hypometabolism | Y | N |
|
Features associated with Logopenic variant
| ||
| Behavioral Characteristics
| ||
| poor repetition of sentences and phrases | N | Y |
| phonological errors in speech | N | Y |
| spared single-word comprehension and object knowledge | N | Y |
| Imaging findings
| ||
| left posterior perisylvian/temporoparietal atrophy and/or hypometabolism | N | Y |
2.1.2. Participant 2: Logopenic Variant PPA (LV)
LV was a 54 year-old left-handed man who reported a five-year history of word-finding difficulties. He had a high-school education and worked as head of maintenance at a major retail chain until the high communication demands of his job became too burdensome. He was on disability leave for approximately two years prior to initiation of this study. LV and his wife reported that they initially noted word-finding problems independent of problems with either recent or remote memory. He also reported initial difficulty with retaining auditorily presented information, such as strings of numbers.
LV was first seen at the Memory and Aging Center at the University of California, San Francisco, for a multidisciplinary evaluation two years prior to his participation in this study. At that time, clinical history and neurological and neuropsychological evaluations documented a progressive decline in language function with relatively fluent speech, intact grammar and motor control for speech, and frequent pauses for word finding. Phonological paraphasias were noted in spontaneous speech and confrontation naming. Formal testing confirmed significant deficits in auditory-verbal working memory and only minor difficulties in the domains of episodic memory and executive functions.
2.1.2.1. Behavioral and Imaging Characteristics
At the time of this study, a comprehensive assessment of speech, language, and cognition confirmed the presence of a fluent aphasia of moderate severity with frequent word-finding pauses, naming errors, and phonological paraphasias (Table 1). WAB Aphasia Quotient was 69.4, with a profile similar to vascular conduction aphasia. Consistent with this type of aphasia, repetition and comprehension of longer and more complex sentences were impaired Confrontation naming measures confirmed significant impairment of lexical retrieval, including the BNT (7/15 on short BNT; 27/60 on the long form) and WAB object naming subtest (38/60; 11/20 items named without cues). The pattern of responses for BNT items not named correctly on the first attempt was as follows: no response (34%); circumlocutions without relevant semantic content (11%); circumlocutions with correct semantic information (7%); phonological paraphasias/partial phonological information (32% that did not result in a self-cue; 16% that did). There was no evidence of apraxia of speech or dysarthria on the Motor Speech Evaluation (Wertz, LaPointe, & Rosenbek, 1984). Semantic testing revealed ceiling performance on the PPT as well as word-picture matching and auditory synonym judgment measures from the Psycholinguistic Assessment of Language Performance in Aphasia (PALPA; (Kay, Lesser, & Coltheart, 1992). Single-word reading of real words was relatively preserved (77/80), with greater impairment on nonwords (16/20). Writing-to-dictation was significantly impaired, however, for both real and nonwords (13/40 real words and 8/20 nonwords). Spelling of real words often resulted in phonologically implausible attempts (e.g., coute for count) and errors on nonwords were typically lexicalizations of the target (e.g., book for boke).
LV’s performance on the MMSE was impaired (20/30). Forward and backward digit span (3 and 2 digits respectively) were also abnormal (less than 1st percentile), indicating deficits in auditory-verbal working memory. Despite difficulties with verbal and nonverbal memory (28th percentile on the California Verbal Learning Test-delayed recall (Delis, Kramer, Kaplan, & Ober, 2000) and <5th percentile on recall of a complex figure (Possin, Laluz, Alcantar, Miller, & Kramer, 2011)), an interview with the patient and caregiver revealed that LV’s activities of daily living were limited primarily by his language impairment.
In summary, the pre-treatment behavioral evaluation confirmed that LV had significant impairment of lexical retrieval abilities in the context of relatively spared semantic knowledge, syntactic skills, and motor control for speech. Less prominent deficits were observed in non-verbal cognitive functioning. Results of the analysis of LV’s MRI scan (see supplemental material) revealed significant atrophy in the left posterior temporal lobe, with extension anteriorly into the mid-superior temporal gyrus. The angular gyrus and middle frontal gyrus in the left hemisphere were also involved. As indicated in Table 2, the pattern of atrophy and the behavioral characteristics demonstrated by this participant were consistent with the logopenic variant of PPA.
2.2. Treatment
The treatment approach implemented for both participants was designed to train lexical retrieval strategies that engage and strengthen residual semantic, orthographic, and phonological knowledge. The exact procedures were tailored to each participant, but employed a common approach referred to as the Lexical Retrieval Cascade Treatment, developed at the University of Arizona, that provides a sequence of tasks to guide the engagement, strengthening, and active use of central components of language processing. Table 3 summarizes the cueing hierarchy used for each participant, beginning with training semantic self-cueing techniques and progressing through orthographic and phonemic self cues.
Table 3.
Cueing hierarchy used for lexical retrieval training
| Lexical Retrieval Cascade | |
|---|---|
| Present picture for Naming | |
| 1. Semantic Self-Cue | Prompt semantic description with, “Tell me about it.”
|
| 2. Orthographic Self-Cue | Request written production of the target word, “Can you write the word?”
|
| 3. Phonemic Self-Cue | Pointing to first grapheme (written either by participant or clinician), “Think of the sound this letter makes. Now try to say the word.” |
| 4. Oral Reading | If unable to produce the spoken name or to write the word independently, the written name is provided.
|
| 5. Repetition | When necessary, the spoken model of the word is provided for repetition. |
| 6. **Semantic plausibility judgments | Ask yes/no questions regarding semantic features of target (x5).
|
| 7. **Recall | Ask for recall of two semantic features plus spoken/written name |
|
| |
| Homework Protocols | |
| 1. SV | Lexical Retrieval Cascade steps 1–3
|
| 2. LV | Modified Copy and Recall Treatment (CART; Beeson & Egnor, 2006)
|
LV only
2.2.1. Stimulus selection
Twenty imageable, low frequency items were targeted for training. For this study, the items were selected from a standard set of 60 items based on the participants’ interests and performance on baseline probes. Specifically, items were selected that were not named correctly on at least 2 of 3 attempts prior to treatment.
2.2.2. Training criteria and data collection
The twenty items were trained in four sets of five, using a multiple baseline design. Criterion for mastery was set at 80% or greater accuracy on a given set in a single session (LV) or two consecutive sessions (SV). Performance on all twenty items was probed at the beginning of each treatment session, prior to any treatment activities, and only those items named correctly, either spontaneously or with overt self-cues, were scored as correct. No cues were provided by the clinician during the pre-treatment probes. For participant LV, one set of five items was probed but remained untrained. This set was matched with trained sets for word length (in letters and phonemes), imageability, frequency, and age of acquisition. Generalization was also examined by re-administration of naming tests, including the BNT and the object naming subtest of the WAB.
2.3. Treatment Implementation and Outcomes
2.3.1. Participant 1: SV
SV participated in four weeks of treatment, with sessions occurring twice weekly for one hour, for a total of 8 hours of direct contact with the clinician. SV also completed at least 30 minutes of homework five days per week, totaling approximately 20 total hours of homework. During treatment sessions, he was guided through the lexical retrieval cascade for each item in the targeted set. At baseline, SV’s error performance on items to be trained was similar to his performance on the BNT; he either stated he did not know the item (11% of errors), provided information without semantic content (26% of errors), provided correct semantic information that did not cue naming (57% of errors), and in a few cases, provided partial orthographic information (e.g., “it starts with…”) that did not cue naming (6% of errors). Once treatment on a particular set was initiated, SV was typically able to retrieve the name of each targeted item spontaneously, or during the semantic self-cueing stage. During treatment sessions, it was notable that SV’s recall of personal experiences with items appeared more beneficial for self-cueing naming than semantic circumlocution. For example, SV could indicate that a scorpion was an insect found in the desert, but often would not be able to provide the name until he described an experience, such as, “a friend of mine was out hiking and put her hand down on a scorpion.” SV also occasionally benefitted from using orthographic self-cues, as he could at times generate at least partial orthography, which led him to the correct spoken name (e.g., he might write scor and then say, “scorpion”). Despite the use of overt self-cueing during treatment sessions as items were being trained, SV rarely used overt self-cueing during probes; that is, once he relearned a target name, he provided that name spontaneously during probes without demonstrating overt strategy use.
Multiple baseline data for SV’s performance on the lexical retrieval cascade are shown in Figure 1. His performance was relatively stable over the first 3 pre-treatment probes, but as treatment was implemented for set 1, he showed some improvement in lexical retrieval for untrained sets. This upward drift in performance suggested generalization of lexical retrieval strategies to untrained items. As shown in Figure 1, SV demonstrated mastery of each trained set within two sessions, and maintained good performance for the duration of the training period. To estimate the treatment effect size, the change in the level of performance on the last three maintenance scores for each set of words was compared to the three probes collected before any treatment began (only the first three baseline points were used due to the upward drift in sets 2-4 following the onset of treatment for set 1), and d-statistics were calculated for each set. The weighted effect size for all trained sets was 7.22 (see Beeson & Robey, 2006, for calculation details). At one month post treatment, SV named items in sets 1–3 with 100% accuracy and named 3/5 items on the last set trained. Four months after the completion of the Lexical Retrieval Cascade Treatment, SV returned to 100% accuracy on all four sets.
Figure 1.

Multiple-baseline data for SV’s performance during and after lexical retrieval training. Phases of treatment are separated by vertical lines, including baseline, treatment sessions, maintenance sessions, and follow-up probes at 1 and 4 months after the completion of treatment.
f/u = follow-up
combined d = 7.22
We implemented a second phase of treatment for participant SV, which employed generative naming tasks similar to those used in previous studies of lexical retrieval training in individuals with PPA (Beeson et al. 2011; Graham, Patterson, Pratt, & Hodges, 1999; Henry, Beeson, & Rapcsak, 2008). The procedures followed those described in Beeson et al. (2011), and outlined in Table 4. This phase of treatment was intended to further strengthen the use of strategies trained with the lexical retrieval cascade. Generative naming ability for twelve semantic categories was probed. Six categories were entered into training (three living and three non-living) while six semantically matched categories were probed but not trained. For this phase of treatment, SV was seen daily for two-hour treatment sessions occurring five days per week for 12 sessions, over two and a half weeks, along with approximately one hour of daily homework (~12 hours total).
Table 4.
Generative naming treatment protocol used with participant SV
| Generative Naming Treatment | |
|---|---|
| 1. Baseline Probes |
|
| 2. Treatment |
|
| 3. Homework |
|
| 4. Maintenance |
|
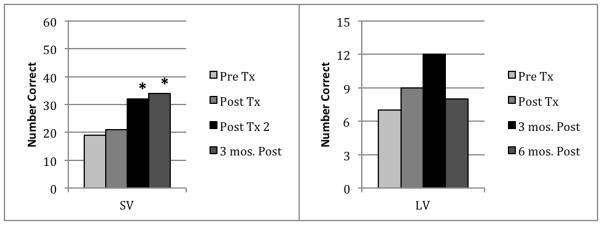
Immediately following treatment, SV showed a significant increase in the number of items that he was able to generate in trained categories, and he maintained this for at least three months following treatment (see Figure 2). This improvement was statistically significant when tested using a time (pre-tx vs. post-treatment) by condition (trained vs. untrained) ANOVA. Follow up tests confirmed significantly more items generated after treatment, F(1,47) = 78.28, p<0.001, for both trained and untrained categories, with better performance in trained versus untrained categories, ANOVA, F(1,47) = 16.26, p<0.001.
Figure 2.

SV’s performance on generative naming for pre-treatment, maintenance, 1 month following treatment, and three months following treatment. For ease of display, trained and untrained sets were averaged separately for each treatment phase.
*Significant improvement relative to pre-treatment performance; f/u = follow-up.
2.3.1.1. Post-Treatment Assessment and Generalization Effects
SV’s performance on the WAB stayed relatively stable over the course of treatment (AQ 90.2 to 90.8), with improvement noted on the object naming subtest (from 39 to 48 points out of 60, reflecting correct naming of 15 items out of 20 compared to 11 before treatment). SV was administered the BNT at four different time points: 1) prior to treatment, 2) following Lexical Retrieval Cascade Treatment, 3) following Generative Naming Treatment, and 4) three months after all treatment was completed (Figure 3). Correct responses increased from 19 to 21 to 32 (out of 60) over the course of treatment, and improved to 34/60 at the three month follow up. Overall, these changes were statistically significant as measured by a Cochran test, Q(3) = 19.585, p < 0.001. Pairwise comparisons with pre-treatment scores using a McNemar test indicated that the improvement was not significant immediately after the Cascade Treatment (S(1) = 0.333, p = 0.564), but improvements were significant after the generative naming protocol (S(1) = 8.895, p = 0.003) and three months following treatment (S(1) = 11.842, p < 0.001).
Figure 3.
Performance on the Boston Naming Test for PPA participants SV and LV.
*= significant change relative to pre-treatment performance
Whereas SV did not use overt self-cueing for the majority of his correct responses on the BNT, he demonstrated a notable change in error types, particularly following the Cascade Treatment. “I don’t know” responses decreased from 39% to 5% of total errors, while responses including a single unit of correct semantic information increased from 34% to 49%. An additional 21% of errors contained more than one correct unit of semantic information, or semantic plus orthographic information. For example, pre-treatment, SV’s response to “harmonica” was “It’s a musical instrument.” After he completed the Lexical Retrieval Cascade Treatment, he responded, “It’s a musical instrument. You put your mouth on it and blow. It starts with an ‘h’.”
SV also showed improved performance by four points on the picture version of the PPT, a test of semantic knowledge. General cognitive skills remained unimpaired, with a score of 30/30 on the MMSE post-treatment.
2.3.1.2. Self-Assessment of Change
In order to evaluate SV’s perspective on changes in his lexical retrieval skills following treatment, he completed a self-assessment questionnaire using a quantitative rating scale one week after treatment ended (Figure 4). In order to ensure comprehension of survey questions, items were presented in both written and auditory format and response choices were reviewed for each item. As documented, SV’s language impairment was quite mild and his reading and comprehension skills were sufficient to comprehend survey items. He rated all communication skills as “Better” or “Somewhat Better” than before treatment. SV provided anecdotes about using trained items in functional situations, such as commenting on the specific names of flowers (a category he had worked on in the second phase of treatment) in a neighbor’s garden. He also reported that he found himself, at times, completing entire conversations without notable word-finding difficulty, suggesting improved interactions with communication partners.
Figure 4.
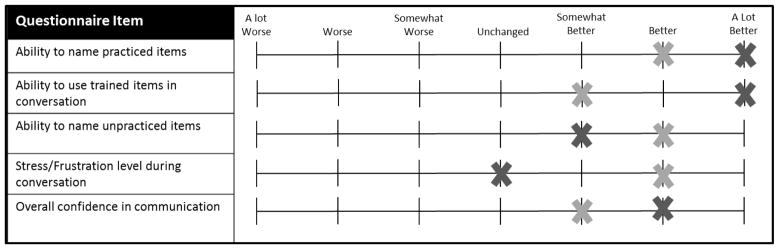
Results of post-treatment surveys completed by participants SV (light gray) and LV (dark gray).
2.3.2. Participant 2: LV
LV was treated using a modified version of the lexical retrieval cascade (Table 3). Because LV lived over 100 miles from San Francisco and was unable to drive, all but the first treatment session were conducted using videoconferencing software (Skype ©), which allows one to alternate between face-to-face viewing and sharing of the clinician’s computer screen (for showing pictures, providing orthographic cues, etc.). LV attended six treatment sessions conducted over a period of eight weeks (he was away on vacation for two weeks) for a total of six hours of clinician-administered treatment supplemented by approximately 18 hours of homework (three hours per week for six weeks).
As with SV, during treatment sessions LV was guided through the cueing hierarchy for each item in the targeted set. Pre-treatment performance on the set of training items revealed the following pattern for items that were not spontaneously and correctly named: a failure to provide any information (69%); circumlocutory responses devoid of semantic content (5%); circumlocutions with some relevant semantic information (2% that resulted in correct name and 7% that did not); phonological paraphasia or part-word responses (2% that resulted in correct name and 9% that did not); responses that contained correct semantic and phonological information (4%); and semantic paraphasias (2%). During training, LV was often responsive to the semantic self-cueing step. In the event that he could not name the item following this step, he was frequently able to retrieve part-word orthographic information for the item, which typically resulted in a self-generated phonemic cue and subsequently, production of the spoken word. Often, during practice, he would retrieve both semantic and orthographic information in the context of a single naming attempt, for example, saying, “I use it in the kitchen to flip pancakes and it starts with an ‘s’… let’s see… a spatula.” In fact, after the first treatment session, LV typically tried to retrieve both semantic and orthographic information without prompting from the clinician as soon as the pictured item was presented.
Whereas written naming was not the focus of treatment, rehearsal of written word forms was included in treatment sessions and in the homework protocol in hopes that improved access to orthographic information would serve to facilitate production of spoken words. We observed this to be the case, with improved generation of whole and part-word orthography during training sessions that facilitated production of phonemic cues and, in many instances, naming of the target.
LV was tested immediately after treatment and at 3 and 6 months post-treatment. In contrast to SV, who remained quite stable over the course of follow-up testing, LV experienced cognitive decline over the course of the study. His MMSE score declined from 20 to 12 (out of 30 possible points) from pre- to post-treatment. The score was 14 at the three-month follow-up, but declined to 10 at six months post-treatment. Thus, the treatment was administered in the context of an overall deterioration in cognitive function.
2.3.2.1. Direct Treatment Effects
Figure 5 shows multiple baseline data for spoken production of trained and untrained sets of words. Criterion was met in one or two sessions for each trained set and performance was maintained for the duration of the training period. As with SV, only the first three pre-treatment probes were compared to the post-treatment probes to calculate effect sizes, due to the upward drift in performance for the second two sets, which was suggestive of generalization of the lexical retrieval strategy after treatment was initiated. The weighted d statistic was 7.55 for all trained sets and 2.04 for the untrained set (pre-versus post-treatment performance). Performance on trained sets at one, two, three, and six-month follow-up assessments was maintained relative to post-treatment levels. The untrained set was assessed at two, three, and six-month time points; performance was above pre-treatment levels at each assessment.
Figure 5.

Multiple baseline data for LV’s spoken production of trained and untrained sets of words. Phases of treatment are separated by vertical lines, including baseline, treatment sessions, maintenance sessions, and follow-up probes at 1, 2, 3, and 6 months after the completion of treatment.
Probes not taken for untrained items at one month post treatment.
combined d for trained sets = 7.55
f/u = follow-up
Acquisition of written names for targets was less robust than spoken naming (see supplemental material), although the resulting effect size was relatively large (d=4.85). Trained sets were maintained at one month post treatment. Performance dropped at two and three-month follow-ups and was only slightly above baseline levels at the six month follow-up.
2.3.2.2. Post-Treatment Assessment and Generalization Effects
Performance on the WAB improved slightly from pre- to post-treatment (69.4→72.6/100) with a decline slightly below baseline level at three months post-treatment (66.7) and a further decline significantly below baseline (57.5) at six months post-treatment. There was a gradual decline in repetition skills at each assessment, consistent with the diagnosis of lvPPA (pre-treatment = 6.1, post-treatment = 5.6/10, three months = 5.3/10, six months = 4.3/10). In addition, the rating for content of connected speech, which was stable from pre-treatment to post-treatment (8/10) and at the three month follow-up (7/10) declined during the interval from three to six months post-treatment (5/10). WAB comprehension scores were stable from pre-to post-treatment (8.6/10→8.9), with a slight decline at three months (7.85) and six months (7.65) post-treatment.
Measures of lexical retrieval for untrained items revealed some degree of generalization. LV was administered the 15-item BNT and WAB object naming tests post-treatment and at each follow-up (Figure 3). Correct responses on the BNT increased from 7 to 9 out of 15 (30/60 on the long form) after treatment, and improved to 12/15 at the three month follow up. At the six month follow-up, LV scored 8/15. Overall, these changes were marginally significant as measured by a Cochran’s test, Q(3) = 7.636, p=0.054. Of particular interest was the change in response types on items that could not be named correctly on the first attempt on the full BNT. After treatment, response attempts with meaningful semantic information increased from 7% to 51%, while the number of no responses declined from 34% to 9%. Circumlocutions with no meaningful semantic information were reduced from 11% to 9% and the occurrence of phonological paraphasias/partial phonological information declined from 48% pre-treatment to 15% post-treatment (with 9% resulting in a self-cue). Thus, although there was not a drastic change in overall BNT score at post-treatment, LV’s ability to provide meaningful information for unnamed items, rather than giving no or paraphasic responses, was greatly improved.
Correct responses on the WAB object naming subtest increased from 10 to 19 out of 20 after treatment, with a decline to 16/20 at three months post-treatment and 13/20 at six months post-treatment. These changes were significant overall, with a Cochran’s test, Q(3) = 12.27, p < 0.007. Pairwise McNemar tests confirmed significant change post-treatment, S(1) = 9, p < 0.003. Three month (p = 0.03) and six month (p = 0.32) follow-up scores were not significantly different from pre-treatment with Bonferroni correction.
In summary, LV showed improvement in lexical retrieval on trained and untrained items in response to treatment. There was some erosion of gains on generalization measures during the interval from three to six months post treatment, such that his performance was comparable to pre-treatment levels at six months post-treatment, despite clear progression of the disease.
2.3.2.3. Self-Assessment of Change
A self-assessment survey was administered to LV post-treatment in order to gauge treatment effects (Figure 4). He marked all but one item positively (from “Somewhat Better” to “A Lot Better”), the exception being a rating of “Unchanged” for frustration level during conversation, as LV indicated he had never been particularly frustrated. LV further indicated that while his confidence in communicating in conversations with friends and family was “Better,” he felt his communication with his primary communication partner (his wife) was “A Lot Better.”
3. Discussion
We have presented treatment outcomes for lexical retrieval training in two individuals with PPA, one with the semantic and the other with the logopenic variant. These two syndromes have in common a marked impairment of word retrieval; however, the underlying cause of the anomia differs, with degraded semantic knowledge in svPPA and impaired phonological processing in lvPPA. The treatment approach was designed to engage, in a structured fashion, residual semantic, orthographic, and phonological information. Treatment outcomes indicated that both participants improved their ability to consistently name a set of target nouns, and they showed maintenance of gains and generalization of the retrieval strategy to untrained items. The participants also reported functional benefit, including improved word retrieval during conversation, as well as greater confidence in communication.
Participant SV, with the semantic variant of PPA, not only demonstrated acquisition of trained items in response to treatment with the Lexical Retrieval Cascade, but showed generalization of self-cueing strategies to not-yet-trained sets. In addition, SV continued to improve on measures of lexical retrieval following a second phase of treatment designed to encourage use of self-cueing strategies during timed generative naming trials. This outcome offers promise that the treatment benefits of the Lexical Retrieval Cascade or similar approaches can be augmented by training with tasks that heighten lexical retrieval demands. The responsiveness of the participant with svPPA to this intervention stands in contrast to previous work suggesting that cueing strategies are of limited value to individuals with this disorder (Jefferies, Patterson, & Lambon Ralph, 2008). SV’s ability to use a strategic cueing approach to successfully facilitate naming is likely due to several factors. The first relates to the nature of the treatment itself. In contrast to many previous approaches, the Lexical Retrieval Cascade Treatment engages multiple residual cognitive mechanisms to support word retrieval, with a particular emphasis on self-cueing, rather than reliance on clinician-provided cues. In addition, our training approach encouraged associations between treatment items and episodic memory during naming attempts, as have previous naming treatments that have proven beneficial for individuals with svPPA (Jokel, Rochon, & Leonard, 2002; Jokel, Rochon, & Leonard, 2006; Snowden & Neary, 2002). As such, SV’s partially-degraded semantic representations were likely bolstered by episodic information, which he consistently drew upon during treatment sessions. Finally, SV’s semantic impairment was mild at the time of treatment. Thus, he was consistently able to draw upon residual semantic information for items that he could not name. This residual semantic information, in conjunction with partial phonological/orthographic information, allowed for lexical items to reach threshold for production in a manner that may not have been possible in an individual with more profound semantic loss.
The participant with the logopenic variant of PPA also showed a positive response to treatment for trained and untrained items, despite the fact that his overall cognitive skills declined during the six months that he was followed after treatment. His ability to name practiced items remained quite strong and performance on standardized naming tests at the last follow-up was comparable to pre-treatment performance. Thus, during a nine month period in which LV’s disease progressed rapidly and measurably, his ability to name objects did not decline substantially, suggesting a protective benefit from treatment.
Given the distinct levels of impairment in logopenic and semantic variants of PPA, it might be assumed that different treatment approaches are warranted. In fact, previous research suggested that individuals with different PPA variants may not respond to the same intervention (Henry, Beeson, & Rapcsak, 2008; Newhart et al., 2009). By design, the Lexical Retrieval Cascade Treatment engages each of the central components of language processing (semantics, phonology, and orthography), and has the potential to strengthen weakened domains and facilitate reliance on residual processing in individuals with varying profiles. In this study, both individuals benefited from self-cueing approach, with SV showing particular benefit from recall of personal experiences, and LV drawing upon residual phonological and orthographic information in conjunction with spared semantic representations.
In addition to their deficits arising due to breakdown of distinct cognitive processes (semantic versus phonological) required for naming, the participants also represented different severities of aphasia and disease. SV was one and one half years post onset of initial symptoms, with a MMSE score of 29/30. LV, on the other hand, was five years post onset, with a MMSE score of 20/30 at the time treatment was initiated. Imaging findings indicate a much greater extent and degree of atrophy in LV’s brain relative to SV, corroborating the clinical picture. Thus, our findings in these two participants suggest that use of a multi-modal naming cascade for treatment of anomia can be beneficial not only across PPA syndromes, but also aphasia severity levels. This approach may be adapted to suit the progression of the illness and evolution of aphasia, such that different levels of cueing are emphasized during successive stages of PPA for each individual. Treatment gains are likely to be greatest, however, in individuals in the mild-to-moderate range of severity who are able to master strategic aspects of lexical retrieval training.
It was impressive to note that our participants showed robust gains for trained items as well as maintenance of gains for several months post-treatment. These gains were observed after relatively few sessions with the clinician (eight in the case of SV and six for LV). However, it should be emphasized that the significant improvements observed in these two cases were attributable to the combined effects of structured treatment sessions and daily homework exercises that involved rehearsal of retrieval strategies and repeated spoken and written production of targets. In this study and others, we have observed that individuals with PPA, even those with greater severity of aphasia and some degree of concomitant cognitive deficits, can be trained to reliably complete homework assignments (Beeson et al., 2011; Henry et al. 2008). Homework may provide additional daily stimulation, allowing clinicians to increase the intensity of treatment in a structured manner. The nature of homework may vary, as we have illustrated here, by incorporating aspects of training used in sessions with the clinician, or by using supplemental approaches such as Copy and Recall Treatment (CART) (Beeson, Hirsch, & Rewega, 2002; Beeson & Egnor, 2006)
The treatment methods employed with SV and LV were nearly identical; however, for LV, treatment was administered largely via the Internet using Skype © software. We were encouraged by his treatment response, which was similar in magnitude to that of our other participant (d statistics = 7.22 for SV and 7.55 for LV), suggesting that treatment administered via videoconference may be a viable alternative for individuals who otherwise cannot be seen by a clinician. Face-to-face treatment continues to be the preferred mode of delivery, given that it allows for a greater degree of interactivity and flexibility. It is also likely that some individuals with progressive aphasia will be unable or unwilling to master the few technical competencies that the use of videoconferencing software entails. Nonetheless, treatment delivered via the Internet may prove to be an effective means of broadening the reach of clinical efforts to support those with language decline due to PPA.
In summary, we have provided accounts of successful naming treatment in two individuals with PPA, one with semantic and the other with logopenic variant. Their positive responses to treatment provide additional evidence in support of efforts to rehabilitate speech and language deficits in this population. Findings indicate that a strategic training approach, emphasizing self-directed retrieval of residual linguistic knowledge, can have lasting and generalized effects, even in the face of the inevitable decline that comes with PPA. Such an approach capitalizes on spared cognitive and neural systems, emphasizing strategies that are most productive and beneficial for a given individual. This approach has the potential to empower individuals with PPA to communicate using their strengths, reinforcing not only specifically targeted vocabulary, but a set of communication strategies that are more broadly beneficial.
Supplementary Material
HIGHLIGHTS.
Two individuals with progressive aphasia underwent a novel treatment for naming.
Participants had differing language profiles and levels of aphasia severity.
One participant with logopenic and one with semantic variant PPA participated.
Treatment was unique in its focus on training self-cueing strategies for naming.
Each individual benefited and showed maintenance and generalization of gains.
Acknowledgments
This work was supported by grants R01 DC007646 (PMB), and F32 DC 010945 (MLH) from the NIH/NIDCD, R01 NS050915 (MLGT) from the NIH/NINDS, and P01AG019724 (BLM) from the NIH/NIA. The authors thank Benno Gesierich, Maria Luisa Mandelli, and Lauren Clark for their assistance with this paper.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Beeson PM, Egnor H. Combining treatment for written and spoken naming. Journal of the International Neuropsychological Society. 2006;12(06):816–827. doi: 10.1017/S1355617706061005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beeson PM, Hirsch FM, Rewega MA. Successful single-word writing treatment: Experimental analyses of four cases. Aphasiology. 2002;16(4):473–491. [Google Scholar]
- Beeson PM, King RM, Bonakdarpour B, Henry ML, Cho H, Rapcsak SZ. Positive effects of language treatment for the logopenic variant of primary progressive aphasia. Journal of Molecular Neuroscience. 2011;45:724–736. doi: 10.1007/s12031-011-9579-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bier N, Macoir J, Gagnon L, Van der Linden M, Louveaux S, Desrosiers J. Known, lost, and recovered: Efficacy of formal-semantic therapy and spaced retrieval method in a case of semantic dementia. Aphasiology. 2009;23(2):210–235. [Google Scholar]
- Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based norms for the mini-mental state examination by age and educational level. JAMA: The Journal of the American Medical Association. 1993;269(18):2386–2391. [PubMed] [Google Scholar]
- Delis D, Kramer J, Kaplan E, Ober B. California Verbal Learning Test. 2. San Antonio, Tx: The Psychological Corporation; 2000. [Google Scholar]
- Dressel K, Huber W, Frings L, Kümmerer D, Saur D, Mader I, et al. Model-oriented naming therapy in semantic dementia: A single-case fMRI study. Aphasiology. 2010;24(12):1537–1558. [Google Scholar]
- Folstein MF, Folstein SE, McHugh PR. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. Journal of Psychiatric Research. 1975;12(3):189–198. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, et al. Classification of primary progressive aphasia and its variants. Neurology. 2011;76(11):1006–1014. doi: 10.1212/WNL.0b013e31821103e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorno-Tempini ML, Brambati SM, Ginex V, Ogar J, Dronkers NF, Marcone A, et al. The logopenic/phonological variant of primary progressive aphasia. Neurology. 2008;71(16):1227–1234. doi: 10.1212/01.wnl.0000320506.79811.da. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorno-Tempini ML, Dronkers NF, Rankin KP, Ogar JM, Phengrasamy L, Rosen HJ, et al. Cognition and anatomy in three variants of primary progressive aphasia. Annals of Neurology. 2004;55(3):335–346. doi: 10.1002/ana.10825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham KS, Patterson K, Pratt KH, Hodges JR. Relearning and subsequent forgetting of semantic category exemplars in a case of semantic dementia. Neuropsychology. 1999;13(3):359–380. doi: 10.1037//0894-4105.13.3.359. [DOI] [PubMed] [Google Scholar]
- Graham KS, Patterson K, Pratt KH, Hodges JR. Can repeated exposure to” forgotten” vocabulary help alleviate word-finding difficulties in semantic dementia? An illustrative case study. Neuropsychological Rehabilitation. 2001;11(3–4):429–454. [Google Scholar]
- Grossman M, Mickanin J, Onishi K, Hughes E, D’Esposito M, Ding XS, et al. Progressive nonfluent aphasia: Language, cognitive, and PET measures contrasted with probable alzheimer’s disease. Journal of Cognitive Neuroscience. 1996;8(2):135–154. doi: 10.1162/jocn.1996.8.2.135. [DOI] [PubMed] [Google Scholar]
- Henry ML, Beeson PM, Rapcsak SZ. Treatment for lexical retrieval in progressive aphasia. Aphasiology. 2008;22(7):826–838. doi: 10.1080/02687030701820055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Henry ML, Gorno-Tempini ML. The logopenic variant of primary progressive aphasia. Current Opinion in Neurology. 2010;23(6):633–637. doi: 10.1097/WCO.0b013e32833fb93e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heredia CG, Sage K, Lambon Ralph MA, Berthier M. Relearning and retention of verbal labels in a case of semantic dementia. Aphasiology. 2009;23(2):192–209. [Google Scholar]
- Hodges JR, Patterson K. Semantic dementia: A unique clinicopathological syndrome. The Lancet Neurology. 2007;6(11):1004–1014. doi: 10.1016/S1474-4422(07)70266-1. [DOI] [PubMed] [Google Scholar]
- Hodges JR, Patterson K, Oxbury S, Funnell E. Semantic dementia: Progressive fluent aphasia with temporal lobe atrophy. Brain. 1992;115(6):1783–1806. doi: 10.1093/brain/115.6.1783. [DOI] [PubMed] [Google Scholar]
- Jefferies E, Patterson K, Lambon Ralph MA. Deficits of knowledge vs. executive control in semantic cognition: Insights from cued naming. Neuropsychologia. 2008;46:649–658. doi: 10.1016/j.neuropsychologia.2007.09.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jokel R, Rochon E, Leonard C. Therapy for anomia in semantic dementia. Brain and Cognition. 2002;49(2):241–244. [PubMed] [Google Scholar]
- Jokel R, Anderson ND. Quest for the best: Effects of errorless and active encoding on word re-learning in semantic dementia. Neuropsychological Rehabilitation. 2012;22(2):187–214. doi: 10.1080/09602011.2011.639626. [DOI] [PubMed] [Google Scholar]
- Jokel R, Rochon E, Anderson ND. Errorless learning of computer-generated words in a patient with semantic dementia. Neuropsychological Rehabilitation. 2010;20(1):16–41. doi: 10.1080/09602010902879859. [DOI] [PubMed] [Google Scholar]
- Jokel R, Rochon E, Leonard C. Treating anomia in semantic dementia: Improvement, maintenance, or both? Neuropsychological Rehabilitation. 2006;16(3):241–256. doi: 10.1080/09602010500176757. [DOI] [PubMed] [Google Scholar]
- Kaplan E, Goodglass H, Weintraub S. Boston Naming Test. Philadelphia: Lippincott, Williams and Wilkins; 2001. [Google Scholar]
- Kay J, Lesser R, Coltheart M. PALPA: Psycholinguistic Assessments of Language Processing in Aphasia. Hove: Lawrence Erlbaum Associates Ltd; 1992. [Google Scholar]
- Kramer JH, Jurik J, Sha SJ, Rankin KP, Rosen HJ, Johnson JK, et al. Distinctive neuropsychological patterns in frontotemporal dementia, semantic dementia, and alzheimer disease. Cognitive and Behavioral Neurology. 2003;16(4):211–218. doi: 10.1097/00146965-200312000-00002. [DOI] [PubMed] [Google Scholar]
- Lambon Ralph MA, McClelland JL, Patterson K, Galton CJ, Hodges JR. No right to speak? The relationship between object naming and semantic impairment: Neuropsychological evidence and a computational model. Journal of Cognitive Neuroscience. 2001;13(3):341–356. doi: 10.1162/08989290151137395. [DOI] [PubMed] [Google Scholar]
- Lambon Ralph MA, Moriarty L, Sage K. Anomia is simply a reflection of semantic and phonological impairments: Evidence from a case-series study. Aphasiology. 2002;16(1–2):56–82. [Google Scholar]
- Lambon Ralph MA, Sage K, Jones RW, Mayberry EJ. Coherent concepts are computed in the anterior temporal lobes. Proceedings of the National Academy of Sciences. 2010;107(6):2717–2722. doi: 10.1073/pnas.0907307107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mayberry EJ, Sage K, Ehsan S, Lambon Ralph MA. Relearning in semantic dementia reflects contributions from both medial temporal lobe episodic and degraded neocortical semantic systems: Evidence in support of the complementary learning systems theory. Neuropsychologia. 2011;49:3591–3598. doi: 10.1016/j.neuropsychologia.2011.09.010. [DOI] [PubMed] [Google Scholar]
- Mesulam MM. Slowly progressive aphasia without generalized dementia. Annals of Neurology. 1982;11(6):592–598. doi: 10.1002/ana.410110607. [DOI] [PubMed] [Google Scholar]
- Newhart M, Davis C, Kannan V, Heidler-Gary J, Cloutman L, Hillis A. Therapy for naming deficits in two variants of primary progressive aphasia. Aphasiology. 2009;23, 7(8):823–834. [Google Scholar]
- Possin KL, Laluz VR, Alcantar OZ, Miller BL, Kramer JH. Distinct neuroanatomical substrates and cognitive mechanisms of figure copy performance in Alzheimer’s disease and behavioral variant frontotemporal dementia. Neuropsychologia. 2011;49(1):43–48. doi: 10.1016/j.neuropsychologia.2010.10.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raven JC, Court JH, Raven J. Coloured Progressive Matrices. Oxford: Oxford Psychologists Press; 1990. [Google Scholar]
- Schwartz MF, Dell GS, Martin N, Gahl S, Sobel P. A case-series test of the interactive two-step model of lexical access: Evidence from picture naming. Journal of Memory and Language. 2006;54(2):228–264. doi: 10.1016/j.jml.2006.05.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snowden JS, Neary D. Relearning of verbal labels in semantic dementia. Neuropsychologia. 2002;40(10):1715–1728. doi: 10.1016/s0028-3932(02)00031-3. [DOI] [PubMed] [Google Scholar]
- Tombaugh TN, Hubiey AM. The 60-item Boston Naming Test: Norms for cognitively intact adults aged 25 to 88 years. Journal of Clinical and Experimental Neuropsychology. 1997;19(6):922–932. doi: 10.1080/01688639708403773. [DOI] [PubMed] [Google Scholar]
- Warrington EK. Warrington Recognition Memory Test. Windsor, England: Nfer-Nelson Publishing; 1984. [Google Scholar]
- Wechsler D. Wechsler Adult Intelligence Scale. 4. San Antonio, TX: The Psychological Corporation; 2008. [Google Scholar]
- Wertz RT, LaPointe LL, Rosenbek JC. Apraxia of speech in adults: The disorder and its management. New York: Grune and Stratton; 1984. [Google Scholar]
- Wilson SM, Dronkers NF, Ogar JM, Jang J, Growdon ME, Agosta F, et al. Neural correlates of syntactic processing in the nonfluent variant of primary progressive aphasia. The Journal of Neuroscience. 2010a;30(50):16845–16854. doi: 10.1523/JNEUROSCI.2547-10.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson SM, Henry ML, Besbris M, Ogar JM, Dronkers NF, Jarrold W, et al. Connected speech production in three variants of primary progressive aphasia. Brain. 2010b;133(7):2069–2088. doi: 10.1093/brain/awq129. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.