

Abstract
Background and Purpose
Susceptibility-weighted imaging (SWI) has been shown to be superior in its ability to demonstrate brain mineralization than other conventional MR imaging. The goal of our study was therefore to assess the frequency and extent of putaminal hypointensity in parkinsonian variant MSA using SWI.
Methods
11 patients with multiple system atrophy-parkinsonian type (MSA-p), 30 patients with Parkinson’s disease (PD), and age matched 30 controls were investigated using 3 Tesla MRI. The pattern of putaminal hypointensity was measured using a visual grading scale and scored from 0 to 3.
Results
Hemi- or bilateral putaminal hypointensity (a score of ≥ 2) and hyperintense rim were recognized in 81.8% and 54.5% of 11 MSA-p, respectively. The scores of putaminal hypointensity of MSA-p were significantly higher than other groups (p < 0.001), a score of ≥ 2 differentiated MSA-p from other groups. And all five patients with early disease stage also showed these characteristic findings.
Conclusions
SWI appears to be useful for depicting putaminal hypointensity even in early stage of MSA-p. This finding suggests that iron deposition associated putaminal degeneration can occur early in the disease process.
Keywords: Multiple system atrophy, Putamen, Susceptibility-weighted imaging
It is challenging to distinguish patients with the Parkinson variant of multiple system atrophy (MSA-p) from those with Parkinson’s disease (PD) in early stages of the disease.1 The evaluation of putaminal changes using brain MRI has been shown to be useful in the differential diagnosis of PD and MSA-p.
Typical alterations predominately found in MSA-p patients include putaminal atrophy and a hyperintense lateral rim corresponding to neuronal cell loss and gliosis in this area.2 The ability of T2*-weighted gradient echo (T2*W) sequences to detect the paramagnetic effects of iron deposition in the putamen has been discussed in previous studies.3,4 However, these characteristic MRI features are predominantly found in cases in advanced stages of disease. Moreover, conventional MRI sequences are not sensitive enough to detect subtle putaminal alterations in early disease stages. Currently, diffusion-weighted MRI5 and MRI-based volumetric measurements6 are useful methods for evaluating subtle putaminal pathology, but these methods are not practical for use in daily clinical practice as they require advanced analysis techniques. Thus, the development of a simpler method for evaluating putaminal changes is necessary.
A newer MRI technique, susceptibility weighted imaging (SWI), is more sensitive for the detection of brain mineralization, including iron deposition, than conventional MRI sequences.7 Additionally, SWI creates better anatomic images in which the basal ganglia structures are easily visible. The goal of our study was therefore to develop a simple method for evaluating putaminal changes in patients with MSA-p by SWI that could aid in the differential diagnosis from PD.
Methods
Subjects
Eleven patients with MSA-p, thirty patients with PD, and thirty age-matched controls were enrolled. Patients who had been diagnosed with either MSA or PD and followed-up at Pusan National Univeristy Yangsan Hospital underwent 3-T MRI between March 2009 and August 2010 and had no nondegenerative structural lesions on brain MRI. Clinical diagnoses of MSA and PD were made according to the consensus statement by Gilman et al.8 and the UK Parkinson’s Disease Society Brain Bank Clinical Diagnostic Criteria,9 respectively. This was a retrospective study of data housed at our hospital. The privacy of patients was completely protected, and the study was approved by the institutional ethics committee.
MRI protocol and image analysis
All brain MRI was performed using the 3 Tesla MRI system (Verio, Siemens, Germany). The axial scans were set parallel to the intercommissural line. The following sequences were performed routinely: axial T2-weighted images, axial fluid attenuated inversion recovery images, axial T1-weighted images, and susceptibility-weighted images. The following imaging parameters were used for the SWI sequence: TR = 28 ms, TE = 20 ms, Flip angle = 20°, matrix size = 320 × 240, and slice thickness = 2 mm.
The signal intensity of each putamen and the localization of abnormality on SWI were evaluated separately by two raters, a neurologist (L.J.H) and a neuroradiologist (B.S.K). In cases of discrepancy between grades assigned by the two raters, the final grade for analysis was decided by consensus between the two raters. The SWI slice in which the putamen was best visualized was used. The putaminal signal intensity and distribution was assessed and scored as follows: Grade 0: similar to CSF intensity; Grade 1: condensed lineal lateral margin without a posterolateral gradient, greater than CSF intensity; Grade 2: marked hypointensity with a posterolateral gradient, similar to the vein of Galen; Grade 3: marked postereolateral to anteromedial hypointensity (Figure 1). If the scores of the two sides (right/left) differed, the higher score of the more hypointense nucleus and the mean score of both sides were included in the analysis. Other parameters such as hyperintense putaminal rim and hyperintensity of the pons (“hot cross bun” sign) on T2-weighted images, and brain stem and cerebellar atrophy were also included.
Figure 1.
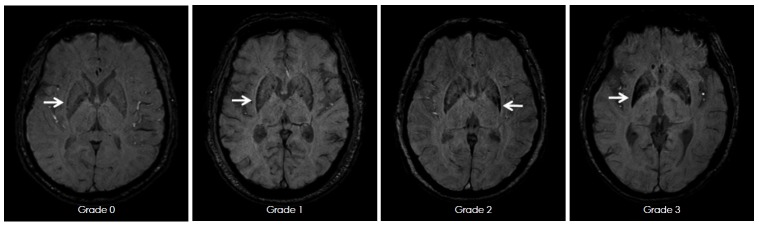
Axial SWI images demonstrate increasing grades of putaminal hypointensity (indicated by white arrows, grades 0 to 3). SWI: susceptibility weighted imaging.
Statistical analysis was carried out using SPSS software (version 12.0, SPSS, Chicago, IL, USA). The Krunskal-Willis test was used to assess differences in patient characteristics. The Mann-Whitney U test was used to compare the grade of putaminal hypointensity between groups. The Spearman’s rank correlation coefficient was used to evaluate the correlation between age or clinical scales and the grade of putaminal hypointensity. To verify the reproducibility of the findings, the inter-rater reliability was evaluated by calculating Cohen’s kappa.
Results
There were no significant differences in mean age, sex distribution, and disease duration among the MSA-p, PD, and control groups (Table 1). The inter-rater reliability for putaminal hypointensity was good (Cronbach’s alpha = 0.8). The scores corresponding to the grade of putaminal hypointensity on each sequence are summarized in Table 1. The scores (both higher and mean scores) of putaminal hypointensity in the MSA-p group were significantly higher than in the PD and control groups (p < 0.001). There were no significant differences in putaminal hypointensity scores between the PD and control groups. Hemi- or bilateral putaminal hypointensity (a score ≥ 2) and a posterolateral hyperintense rim were recognized in 81.8%, and 54.5% of the 11 MSA-p cases, respectively; all five patients with disease duration shorter than one year also showed these characteristic putaminal hypointensity (Figure 2). Three cases demonstrated hypointensity on SWI (a score ≥ 2) without a posterolateral hyperintense rim. Atrophy in the brain stem and cerebellum and the “hot cross bun” sign were found in 7 and 2 subjects, respectively. There was no correlation between putaminal scores and age, disease duration, or severity using UPDRS-motor scores in MSA-p subjects. In 6 subjects, the region of the putamen that was contralateral to the more severely affected limb was more hypointense than that on the ipsilateral side.
Table 1.
Demographic characters and SWI scores of the subject groups
| MSA-P (n=11) | PD (n=30) | Controls (n=30) | |
|---|---|---|---|
| Demograhic characteristics | |||
| Mean (SD) age (years) | 61.3 (5.8) | 62 (8.8) | 60.2 (7.1) |
| Male/Female | 3/8 | 14/16 | 14/16 |
| Mean (SD) disease duration (years) | 2.4 (1.9) | 1.9 (1.48) | |
| Putaminal hypointensity, N × 2 | |||
| Grade 0 | 0 | 32 | 36 |
| Grade 1 | 10 | 27 | 23 |
| Grade 2 | 6 | 1 | 1 |
| Grade 3 | 6 | 0 | 0 |
| Higher score (mean ± SD) | 2.18 ± 0.68* | 0.47 ± 0.51 | 0.43 ± 0.57 |
| Mean score (mean ± SD) | 1.81 ± 0.75* | 0.48 ± 0.52 | 0.42 ± 0.53 |
p<0.001 vs. PD and Controls.
N: number of the putamen evaluated, SD: standard deviation, SWI: susceptibility weighted imaging, MSA-P: multiple systematrophy.
Figure 2.
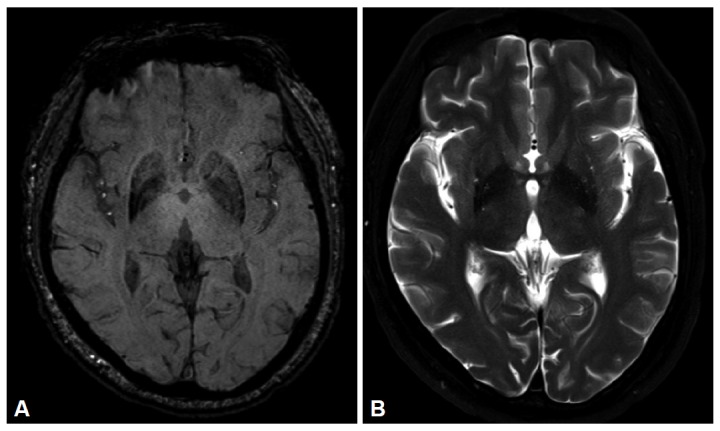
A 51-year-old male with parkinsonian variant of multiple system atrophy. Axial SWI (A) shows marked hypointensity in right putamen (Grade 2). On T2-weighted image (B), putaminal hypointensity is subtle compared with SWI. SWI: susceptibility weighted imaging.
Discussion
Assessing the “posterolateral” putaminal margin is important for distinguishing patients with MSA-p from those with PD in the early disease stages.2,10,11 Pathologic study indicates that patients with MSA-p display neuronal cell loss, gliosis, and ferritin and Fe (3+) deposition predominantly in the posterior areas of the putamen.12,13,14 Several studies have shown that a posterolateral hyperintense rim corresponding to gliosis is the hallmark of putaminal abnormality on MRI.15,16 However, the slit-like hyperintense rim is present in normal subjects, especially in 3 Tesla MRI, after which it becomes increasingly vague.17,18 In our cases, a posterolateral hyperintense rim was not a better marker of MSA-p than putaminal hypointensity due to its relatively low sensitivity, especially in early stages of the disease.
A pilot study using 1.5T MRI provided evidence for the diagnostic potential of SWI in differentiating PD, PSP, and MSA-p groups.19 However, in contrast to our results, putaminal hypointensity on SWI did not differentiate MSA-p and PD. According to their grading system, the putaminal signal abnormalities were focused only on the signal intensity. The characteristic pattern of putaminal mineralization with a lateral to medial gradient was ignored. In our experience, isolated lineal hypointensity in the lateral putaminal margin without a posterolateral gradient on SWI is a nonspecific finding and is commonly observed in age-related physiological mineralization. Our data suggest that the pattern consisting of posterolateral putaminal hypointensity with a striking lateral to medial gradient on SWI is a highly specific sign of MSA-p.
The characteristic putaminal hypointensity on SWI was observed in most of the MSA-p patients with early disease stage. This finding suggests that putaminal iron deposition can occur early in the disease process, which coincides with previous pathological observations.12 This may also explain why we did not observe a relationship between putaminal signal loss and disease duration.
Our study is limited by the absence of pathologic diagnosis. The lack of postmortem definite diagnosis increases the likelihood of misdiagnosis in some patients. Two patients with MSA did not reveal abnormal findings on SWI, although their clinical symptoms were consistent with MSA-p. Previous studies also reported a lack of abnormality on T2*W sequences for some patients.3 Additional studies that evaluate SWI-pathologic correlations with larger samples are still needed.
In conclusion, the simple visual assessment of putaminal abnormalities on SWI might be valuable for differentiating MSA-p from PD and healthy subjects in daily clinical practice. SWI appears to be useful for depicting putaminal hypointensity, even in patients with disease duration shorter than one year, suggesting that putaminal iron deposition can occur early in the disease process.
Acknowledgments
This study was sponsored with a grant from the Pusan National University Yangsan Hospital Research Grant (2010).
Footnotes
The authors have no financial conflicts of interest.
REFERENCES
- 1.Wenning GK, Shlomo YB, Magalhães M, Daniel SE, Quinn NP. Clinical features and natural history of multiple system atrophy. Brain. 1994;117:835–845. doi: 10.1093/brain/117.4.835. [DOI] [PubMed] [Google Scholar]
- 2.Sitburana O, Ondo WG. Brain magnetic resonance imaging (MRI) in parkinsonian disorders. Parkinsonism Relat Disord. 2009;15:165–174. doi: 10.1016/j.parkreldis.2008.04.033. [DOI] [PubMed] [Google Scholar]
- 3.Kraft E, Trenkwalder C, Auer DP. T2*-weighted MRI differentiates multiple system atrophy from Parkinson’s disease. Neurology. 2002;59:1265–1267. doi: 10.1212/01.wnl.0000032757.66992.3c. [DOI] [PubMed] [Google Scholar]
- 4.Von Lewinski F, Werner C, Jörn T, Mohr A, Sixel-Döring F, Trenkwalder C. T2*-weighted MRI in diagnosis of multiple system atrophy. A practical approach for clinicians. J Neurol. 2007;254:1184–1188. doi: 10.1007/s00415-006-0496-1. [DOI] [PubMed] [Google Scholar]
- 5.Schocke MF, Seppi K, Esterhammer R, Kremser C, Jaschke W, Poewe W, et al. Diffusion-weighted MRI differentiates the Parkinson variant of multiple system atrophy from PD. Neurology. 2002;58:575–580. doi: 10.1212/wnl.58.4.575. [DOI] [PubMed] [Google Scholar]
- 6.Schulz JB, Skalej M, Wedekind D, Luft AR, Abele M, Voigt K, et al. Magnetic resonance imaging-based volumetry differentiates idiopathic Parkinson’s syndrome from multiple system atrophy and progressive supranuclear palsy. Ann Neurol. 1999;45:65–74. [PubMed] [Google Scholar]
- 7.Haacke EM, Mittal S, Wu Z, Neelavalli J, Cheng YC. Susceptiblilty-weighted imaging:Technical aspects and clinical application, part 1. Am J Neuroradiol. 2009;30:19–30. doi: 10.3174/ajnr.A1400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gilman S, Low PA, Quinn N, Albanese A, Ben-Shlomo Y, Fowler CJ, et al. Consensus statement on the diagnosis of multiple system atrophy. J Neurol Sci. 1999;163:94–98. doi: 10.1016/s0022-510x(98)00304-9. [DOI] [PubMed] [Google Scholar]
- 9.Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinicopathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55:181–184. doi: 10.1136/jnnp.55.3.181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ito S, Shirai W, Hattori T. Evaluating posterolateral linearization of the putaminal margin with magnetic resonance imaging to diagnose the Parkinson variant of multiple system atrophy. Mov Disord. 2007;22:578–581. doi: 10.1002/mds.21329. [DOI] [PubMed] [Google Scholar]
- 11.Lee JY, Yun JY, Shin CW, Kim HJ, Jeon BS. Putaminal abnormality on 3-T magnetic resonance imaging in early parkinsonism-predominant multiple system atrophy. J Neurol. 2010;257:2065–2070. doi: 10.1007/s00415-010-5661-x. [DOI] [PubMed] [Google Scholar]
- 12.Fearnley JM, Lees AJ. Striatonigral degeneration. A clinicopathological study. Brain. 1990;113:1823–1842. doi: 10.1093/brain/113.6.1823. [DOI] [PubMed] [Google Scholar]
- 13.Schwarz J, Weis S, Kraft E, Tatsch K, Bandmann O, Mehraein P, et al. Signal changes on MRI and increases in reactive microgliosis, astrogliosis, and iron in the putamen of two patients with multiple system atrophy. J Neurol Neurosurg Psychiatry. 1996;60:98–101. doi: 10.1136/jnnp.60.1.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Matsusue E, Fujii S, Kanasaki Y, Sugihara S, Miyata H, Ohama E, et al. Putaminal lesion in multiple system atrophy: postmortem MR pathological correlations. Neuroradiology. 2008;50:559–567. doi: 10.1007/s00234-008-0381-y. [DOI] [PubMed] [Google Scholar]
- 15.Schrag A, Good CD, Miszkiel K, Morris HR, Mathias CJ, Lees AJ, et al. Differentiation of atypical parkinsonian syndromes with routine MRI. Neurology. 2000;54:697–702. doi: 10.1212/wnl.54.3.697. [DOI] [PubMed] [Google Scholar]
- 16.Lee HA, Cho HI, Kim SS, Lee WY. Comparison of magnetic resonance imaging in subtypes of multiple system atrophy. Parkinsonism Relat Disord. 2004;10:363–368. doi: 10.1016/j.parkreldis.2004.04.008. [DOI] [PubMed] [Google Scholar]
- 17.Fujii S, Matsusue E, Kinoshita T, Sugihara S, Ohama E, Ogawa T. Hyperintense putaminal rim at 3T reflects fewer ferritin deposits in the lateral margin area of the putamen. Am J Neuroradiol. 2007;28:777–781. [PMC free article] [PubMed] [Google Scholar]
- 18.Lee WH, Lee CC, Shyu WC, Chong PN, Lin SZ. Hyperintense putaminal rim sign is not a hallmark of multiple system atrophy at 3T. Am J Neuroradiol. 2005;26:2238–2242. [PMC free article] [PubMed] [Google Scholar]
- 19.Gupta D, Saini J, Kesavadas C, Sarma PS, Kishore A. Utility of susceptibility-weighted MRI in differentiating Parkinson’s disease and atypical parkinsonism. Neuroradiology. 2010;52:1087–1094. doi: 10.1007/s00234-010-0677-6. [DOI] [PubMed] [Google Scholar]