

Abstract
Objective Attention-based coping strategies for pain are widely used in pediatric populations. The purpose of this study was to test a novel mindful attention manipulation on adolescent’s experimental pain responses. Furthermore, the relationship between state mindfulness and experimental pain was examined. Methods A total of 198 adolescents were randomly assigned to a mindful attention manipulation or control group prior to an experimental pain task. Participants completed measures of state mindfulness immediately prior to the pain task, and situational catastrophizing and pain intensity following the task. Results Overall the manipulation had no effect on pain. Secondary analysis showed that meditation experience moderated the effect of the manipulation. State mindfulness predicted pain outcomes, with reductions in situational catastrophizing mediating this relationship. Conclusions The mindful attention manipulation was effective among adolescents with a regular meditation practice. State mindfulness was related to ameliorated pain responses, and these effects were mediated by reduced catastrophizing.
Keywords: adolescents, meditation, mindfulness, pain, pain catastrophizing
Pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage” (International Association for the Study of Pain, 1979, p. 249). Acute pain due to illness, injury, and medical procedures as well as everyday bumps and bruises are a frequent occurrence among adolescents and children (Cummings, Reid, Finley, McGrath, & Ritchie, 1996; Perquin et al., 2000). Pain is influenced by more than the extent of physical injury, and the way in which young people cope with the sensory and emotional aspects of pain significantly impacts their pain experience (Asmundson, Noel, Petter, & Parkerson, 2012). Attention-based coping strategies are widely used in the management of both recurrent and acute pain in pediatric populations (Noel, Petter, Parker, & Chambers, 2012; Uman, Chambers, McGrath, & Kisely, 2008). Coping strategies designed to take attention away from painful stimuli (e.g., distraction) have a strong evidence base for acute pain (Uman et al., 2008). It is hypothesized that these manipulations are effective because attending to an alternative stimulus limits attentional resources available to process pain (Johnson, 2005). However, it has been theorized that when pain is viewed as highly threatening it may place such a strong demand on attention that the effects of distraction will be reduced (Eccleston & Crombez, 1999). Evidence with pediatric populations has supported the claim that the effects of distraction are reduced when pain is viewed as highly threatening. In particular, the tendency to catastrophize about pain appears to reduce the use and effectiveness of distraction among children and adolescents during acute pain, and attempts to use distraction may actually worsen pain (Verhoeven, Goubert, Jaaniste, Van Ryckeghem, & Crombez, 2011). Pain catastrophizing refers to the tendency to magnify the threat value of pain, to feel helpless in the face of pain, and to ruminate about pain, and this variable plays a central role in psychological models of pediatric chronic pain (e.g., Asmundson et al., 2012). Because painful sensations may place such a strong demand on attentional resources, researchers have argued that coping strategies which direct attention towards pain in an adaptive manner may be more effective for young people who are high in catastrophizing (Verhoeven et al., 2011).
There is evidence among adults that directing attention towards painful stimuli mindfully may offer benefit in both acute (Zeidan, Gordon, Merchant, & Goolkasian, 2010) and chronic pain (Chiesa & Serretti, 2011) contexts. Mindfulness involves paying attention, on purpose, to present moment experience, in a nonjudgmental and accepting manner (Kabat-Zinn, 1996). This nonjudgmental focus on present-moment experience appears to be a potentially fruitful avenue in helping adolescents attend to pain adaptively. Mindfulness combines aspects of attention-based coping strategies that direct attention towards pain, such as sensory-focused (e.g., Fanurik, Zeltzer, Roberts, & Blount, 1993; Piira, Hayes, Goodenough, & von Baeyer, 2006) and acceptance-based (Hayes et al., 1999) manipulations which have been found to ameliorate acute pain. Standard mindfulness-based interventions are 8 weeks in duration and place a strong emphasis on daily meditation practice (Carmody & Baer, 2009), requiring more time and resources than the brief attention-based coping strategies such as distraction.
Shortened mindfulness interventions for acute pain appear beneficial among adults. For example, Zeidan and colleagues (2010) found that three 20-min sessions of mindfulness training decreased pain intensity during an experimental pain task. Although employing shorter than typical mindfulness interventions, this study still required participants to attend multiple training sessions, requiring more resources than brief distraction-based interventions. It is also important to note that findings with adults may not generalize to youth based on important differences in the development of attentional, cognitive, and emotional regulation abilities (Semple, Lee, & Miller, 2006). Most importantly, meta-cognitive and self-regulation skills which are central to the use of mindfulness continue to develop throughout the adolescent years (Dahl, 2004). Indeed, many of the brain regions hypothesized to be involved in the application of mindfulness to pain such as the the dorso-lateral prefrontal cortex and the orbitofrontal cortex (Zeidan, Grant, Brown, McHaffie, and Coghill, 2012) are among the last brain regions to fully develop (Gogtay et al., 2004). Encouragingly, standard length mindfulness-based interventions have been found to be effective among adolescent psychiatric populations (Biegel, Brown, Shapiro, & Schubert, 2009). In addition, a recent study of children aged 10–14 years found that a set of mindful attention instructions administered prior to and during an experimental pain task was successful in directing attention towards pain, and no significant differences were found between this manipulation and a more traditional distraction-based manipulation (Petter, Chambers, & Chorney, 2013). However, this study lacked a control group, and it remains unclear whether this type of manipulation is more effective than youth’s typical coping responses. Furthermore, this previous study did not examine the potential role of meditation experience in moderating the impact of this type of mindfulness manipulation. This is a potentially important avenue of research given the belief within the field of mindfulness research that attending to unpleasant stimuli in a mindful manner is a skill that may need to be developed through a regular meditation practice (Kabat-Zinn, 2003).
The hypothesis that instructing adolescents to attend mindfully during a pain task will ameliorate pain responses is based on the assumption that a state of nonjudgmental present-moment awareness may buffer against secondary evaluations of physical sensations (i.e., catastrophizing) that increase pain severity (Campbell et al., 2010). On a theoretical level, a state of mindfulness appears antithetical to catastrophizing, which involves negative secondary processing of physical sensations as well as the individual’s ability to tolerate those sensations. Evidence indicates that trait mindfulness (the tendency to be mindful over time) is associated with physical and psychological well-being among adolescents (Brown, West, Loverich, & Biegel, 2011; Greco, Baer, & Smith, 2011), and is a unique predictor of a number of outcomes in adult chronic pain populations (McCracken & Keogh, 2009), and that pain catastrophizing may mediate the relationship between mindfulness and chronic pain outcomes (Cassidy, Atherton, Robertson, Walsh, & Gillett, 2012). However, to-date the relationship between state mindfulness, catastrophizing, and pain has not been examined in the acute pain context. Based on theoretical work and findings related to chronic pain, it appears that state mindfulness may be associated with reductions in catastrophic thinking during acute pain, and through this relationship, may be associated with lower levels of perceived pain intensity and increased pain tolerance.
The primary purpose of this project was to examine the effects of a brief mindful attention manipulation on experimental pain among adolescents. The manipulation was hypothesized to result in increased levels of state mindfulness, decreased catastrophic thoughts during the decreased pain intensity and increased tolerance (Hypothesis 1). Furthermore, it was hypothesized that trait levels of pain catastrophizing would moderate the effects of this manipulation on the outcomes of pain intensity and pain tolerance, such that the manipulation would be more effective among adolescents higher in trait pain catastrophizing (Hypothesis 2). This prediction is based on theoretical and experimental studies which have hypothesized that individuals high in catastrophizing may find directing attention away from pain to be difficult and thus would benefit from manipulations which direct attention towards pain (Eccleston & Crombez, 1999; Verhoeven et al., 2011). Secondary analyses examining the moderating role of previous meditation experience were also conducted given evidence with adult populations that previous meditation experience may moderate the ability to attend mindfully to pain (Grant & Rainville, 2009), Specifically, it was hypothesized that the intervention would be more effective among adolescents with a regular meditation practice such that those who received the mindful attention manipulation would reported decreased pain intensity and increased pain tolerance (Hypothesis 3). Additionally, this study examined the relationship between state mindfulness and experimental pain outcomes. Based on theory and findings with chronic pain, it was hypothesized that higher state mindfulness would result in lowered pain intensity and increased pain tolerance, and that these relationships would be mediated by reductions in catastrophic thinking during the pain task (Hypothesis 4).
Method
The data presented in this manuscript were collected as part of a larger study examining two independent research questions. The purpose of the present study was to examine the effect of a brief mindful attention manipulation and state mindfulness on experimental pain. The other study (Petter, Chambers, McGrath, & Dick, 2013) examined the relationship between trait mindfulness and real world and experimental pain. Methods presented below contain details relevant to the present study. Ethical approval for this study was obtained from the health centre research ethics board.
Design
The design of the current study was a randomized between-subjects design. Participants were randomly assigned using a random number generator to either the mindful attention manipulation or a control group before taking part in the experimental pain task.
Participants
Participants were adolescents recruited through advertisements placed in the community. Specific efforts were made to recruit adolescents with a range of meditation experiences. Advertisements were therefore placed in local meditation centers, yoga studios, and mailing lists to local meditation groups. In addition, a local private school that includes regular meditation practice as part of its curriculum allowed student to take part through the school. Advertisements indicated that the study was examining what influences pain in young people, and some forms of advertisement indicated that teenagers with meditation experience were being sought to take part. Exclusionary criteria for this study were as follows: (1) inability to read and write in English; (2) uncorrected vision or hearing impairment; (3) a diagnosis of attention-deficit / hyperactivity disorder; (4) a health-related medical condition, which could be made worse by placing a limb in cold water (e.g., circulation disorders, heart problems, injuries to the arms or hands); or (5) having previously taken part in a study involving the cold pressor task. Children with chronic health conditions that are not known to be made worse by exposure to cold water were included in the study.
Before enrollment in the study, exclusionary criteria were assessed by a screening interview with participants. No adolescents withdrew following enrolment. One minor adverse event was reported with a participant reporting light-headedness following the pain task. In this case, after having the participant lie down and drink fruit juice, the symptoms subsided. Due to this deviation in protocol this participant was removed from analysis. One more participant was also excluded due to their inability to fully understand the questionnaire materials and answer questions competently as noted by the researcher who observed this participant.
Final data analysis included 198 adolescents (132 females) aged 13–18 years (Mage= 15.99 years, SD = 1.89) and were predominantly White (n = 172) with married parents (n= 131). The majority of patients were recruited through the community (n = 175) with the rest of the sample recruited through a local school (n= 23).
Apparatus
Cold Pressor Task
The cold pressor is a technique for inducing pain in children and adolescents (Birnie, Noel, Chambers, von Baeyer, & Fernandez, 2011). The participant places his/her nondominant hand up to the wrist in cold water for a maximum of 4 min (5°C water was used). Based on current recommendations, participants were not informed of this 4-min ceiling (Birnie, Petter, Noel, Boerner, & Chambers, 2012). Before taking part in the cold pressor task, participants were told to leave their hand in the water for as long as they could even if it was uncomfortable, but to remove it when it hurt too much. The device used for the purposes of this study was a RU-200 Techne Dip Cooler with water temperature controlled by a Techne TE-10D Liquid Bath Thermoregulator.
Experimental Conditions
Mindful Attention Manipulation
Prior to the cold pressor, participants in this condition listened to an audio recording with instructions guiding them through a mindful attention exercise. This manipulation was based on a mindfulness practice originally designed by Jon Kabat-Zinn (1996), adapted for use with adolescents by Gina Biegel (2010), and was modified by the first author (M.P.) for the experimental pain context. Prior to the pain task, participants were asked to do the following, in sequence: (1) sit in an upright and relaxed posture, (2) bring their awareness to the physical sensations throughout their body, (3) notice the mind’s tendency to judge sensations, and to gently let go of judgment, (4) bring their awareness to their breath without changing the breath, (5) notice when they became distracted, acknowledge what caught their attention, and bring their awareness back to the breath, (6) gently move their awareness into their arm, (7) simply notice and accept the feelings that arose throughout their arm, and (8) once again notice when they became distracted, and to return their awareness to their arm. After this 10-min recording finished, participants were asked to fill out the state mindfulness measure. After completing the questionnaires, the recording instructed participants to use this mindful attention during the pain task. Participants also received standard cold pressor instructions. A copy of the mindful attention script is available from the first author.
Control Condition
Participants in the control condition listened to an audio recording asking them to read quietly for 10 min, and were provided with a selection magazines to read during that time. After reading for 10 min, participants were asked to stop and fill out the questionnaire assessing state mindfulness. After filling out the questionnaire, participants were then given standard instructions for the cold pressor task.
Measures
Pain Catastrophizing
The 13-item Pain Catastrophizing Scale (PCS) (Sullivan, Bishop, & Pivik, 1995) was used. This measure assesses an individual’s tendency to catastrophize when in pain (e.g., “When I have pain, I feel I can’t go on”). Answers are given on a 5-point Likert scale with higher scores reflecting higher levels of pain catastrophizing. In this study simplified anchors were used on the Likert scale (e.g., “not at all” = 0, to “extremely” = 4), and the stem “When I have pain” was placed in front of each item. The PCS is a widely used measure in pain research and in this sample showed excellent internal consistency with α = .904.
Meditation Experience
To assess mediation experience, a brief interview was created for the purpose of this study asking participants whether they had ever meditated before and whether they currently meditated. Participants who currently meditated were then asked how long they had been meditating, and how frequently they meditated.
State Mindfulness
The seven-item state version of the Mindful Attention and Awareness Scale (MAAS-S) (Brown, Ryan, & Creswell, 2007) was used. The measure assessed mindfulness following group assignment (e.g., “I found myself preoccupied with the future or the past”). Answers are given on a 7-point Likert scale with scores ranging from 0 to 36 and higher scores reflecting higher levels of state mindfulness. The scaled showed good internal consistency with α = .798.
State Catastrophizing
The six-item Situational Catastrophizing Questionnaire (SCQ; Campbell et al., 2010) was used. The scale assesses how much an individual was catastrophizing during experimental pain (e.g., “I thought the pain might overwhelm me”). Items are answered on a 5-point Likert scale and scores range from 0 to 24 with higher scores indicating higher levels of state catastrophizing. The scale had good internal consistency with α = .880.
Pain Intensity
A verbally administered 11-point numerical rating scale (NRS-11) was used to measure pain intensity. Adolescents were instructed to rate their average and worst pain on a scale of 0 (“No Pain”) to 10 (“The Worst Possible Pain”). These types of numerical rating scales are well validated for use with pediatric populations (von Baeyer et al., 2009).
Pain Tolerance
Pain tolerance times were recorded by the experimenter in the room as the time that the adolescent placed their hand in the water until it was removed (up to 4 min). Video recordings of tolerance times were double-checked by an experimenter blind to the experimental group. Agreement between the two raters was r = .995, p < .001. In three cases, times could not be double-checked due to problems with video equipment.
Post Cold Pressor Manipulation Check
Participants were asked to indicate how often they noticed thoughts about their arm during the pain task (consistent with the mindful attention manipulation) and how often they tried to distract themselves during the pain task (inconsistent with the mindful attention manipulation). Answers were given on a 5-point Likert scale.
Procedure
Participants completed the initial screening interview and provided informed consent either at a research centre at a local tertiary care hospital or at their school. They initially completed the measure of trait pain catastrophizing and questions about meditation experience. They then moved to a separate room to complete the cold pressor task. At this point, participants were randomly assigned to their experimental group and received instructions accordingly. During the entire cold pressor task, an experimenter remained seated behind the participants. After the mindful attention manipulation or silent reading, participants completed the measure of state mindfulness before receiving standard cold pressor instructions. Following withdrawal of the limb during the cold pressor, or after reaching the 4-min ceiling, participants reported their average pain intensity, completed the measure of situational catastrophizing and the manipulation check. They then received a $20 honorarium if they took part at the research centre or had $20 donated to a school fundraiser on their behalf if they took part through their school.
Results
Data Analytic Plan
Less than 1% of items were missing from the questionnaire data. A single imputation using the expectation maximization algorithm was therefore utilized to replace these missing items (Enders, 2001) using Missing Values Analysis with SPSS 20. Because the pain tolerance variable had an extreme negative skew (due to ceiling effects), this variable was dichotomized into whether or not participants reached the 4-min ceiling and was not included in the correlation analyses.
To begin, a series of between-group comparisons using one-way between subjects ANOVA’s and chi-square analyses were conducted to determine if the there were differences between youth who did and did not have a regular meditation practice. A regular meditation practice was defined as meditating at least once a week, for at least 1 year. All other participants were classified as “nonmeditators”. This cut-off point was used, as extensive practice may be necessary to see moderating effects of meditation experience (Grant & Rainville, 2009). These analyses were also conducted to examine whether experimental groups differed on any baseline characteristics. Because of an uneven sex distribution in experimental groups, sex was controlled for in analyses. Between-subjects ANCOVAs controlling for sex were then conducted on the manipulation check outcomes.
To test Hypothesis 1 a single ANCOVA (controlling for sex) was conducted on the outcome variable of pain intensity. In addition a single logistic regression model was conducted to examine the effect of experimental group on the dichotomous pain tolerance outcomes.
To test Hypothesis 2, two moderation models using PROCESS for SPSS (Hayes, 2013) examined whether trait pain catastrophizing moderated the impact of experimental group on pain intensity and tolerance outcomes after controlling for sex.
To test Hypothesis 3, two moderation models using PROCESS for SPSS (Hayes, 2013) examined whether meditation experience moderated the effects of experimental group in predicting pain outcomes. Following moderation models, two independent samples t-tests and two chi-square analyses were used to examine the nature of the effects.
To test Hypothesis 4 a simple mediation model using PROCESS for SPSS was conducted. PROCESS is a computational procedure that provides coefficient estimates for total, direct, and indirect effects of variables using OLS regression for continuous outcomes and maximum likelihood logistic regression for dichotomous outcomes. A 95% bootstrap confidence interval for the indirect effect using 10,000 bootstrap samples was used with sex included as a covariate.
Power analysis based on the following values; alpha = .05, power = .80, and 198 participants showed that this study was adequately powered to detect a small to moderate effect (f= .22) for the main effects and interactions in the between group ANCOVA analysis, as well as a small – moderate effect (f2 = .07) in the hierarchical regression analysis.
Sample Characteristics
Among this sample, 48 adolescents (24%) had some form of meditation practice. Among these adolescents, 21 (11%) were classified as regular meditators. There was no difference between regular meditators and other adolescents on age [F(1,197) = .01, p= .913], There were more females in the regular meditator group than males [females = 18, males = 3, χ2 (1)= 3.83, p = .05]
Baseline Between Group Differences
There were no differences between experimental conditions on mean age [mindful attention: M = 16.02 years (SD = 1.90); control: M = 15.97 years (SD = 1.89), F(1,197) = .036, p = .851] or regular meditator status [χ2 (1) = .625, p = .493]. There were more males in the mindful attention group (n = 42) than the control group (n = 24) [χ2 (1) = 6.32, p < .05].
Manipulation Check
Participants in the mindful attention condition reported using distraction significantly less [mindful attention: M = 1.99 (SD = 1.38); control: M = 2.44 (SD = 1.36), F(2,195) = 5.78, p < .05, ηp2 = .029], and noticing their thoughts about their arm more [mindful attention: M = 2.83 (SD = 1.05); control: M = 2.51 (SD= 1.08), F(2,195) = 4.80, p < .05, ηp2 = .024].
Effect of Experimental Group on Pain Outcomes During the Cold Pressor (Hypothesis 1)
There were no differences between the two groups on the pain intensity outcome [mindful attention: M = 3.57, SD = 2.44; control: M = 3.42, SD = 2.53; F(2,195) = .025, p = .875, ηp2 = .000] or on the pain tolerance outcome [χ2 (1) = .01, p = .920].
Interaction of Experimental Group and Pain Catastrophizing on Pain Outcome Variables (Hypothesis 2)
There was no interaction between experimental group and trait pain catastrophizing in predicting pain intensity [ΔR2 = .023, F(1,193) = .49, p = .486] or tolerance (z = 1.33, p = .184).
Interaction of Experimental Group and Meditation Experience on Outcome Variables (Hypothesis 3)
Figure 1 illustrates the interaction between experimental group and meditation experience in predicting pain intensity during the cold pressor [ΔR2 = .037, F(1,193) = 7.42, p < .01]. Regular meditators in the mindful attention condition reported lower pain intensity than meditators in the control condition [t(19) = 2.39, p < .05], with no effect among nonmeditators [t(175) = .67, p = .51]. Logistic regression showed that the interaction of experimental group and meditation experience was also a predictor of the pain tolerance outcome (z = 1.96, p = .050). Chi-square analysis showed that the manipulation had no effect among nonmeditators [χ2 (1) = .292, p = .589]. Among regular meditators there was a marginal effect with individuals in the mindful attention condition (4 of 9; 44%) being more likely to reach ceiling than those in the control condition [1 of 12; 8%; χ2 (1) = 3.70, p = .055].
Figure 1.
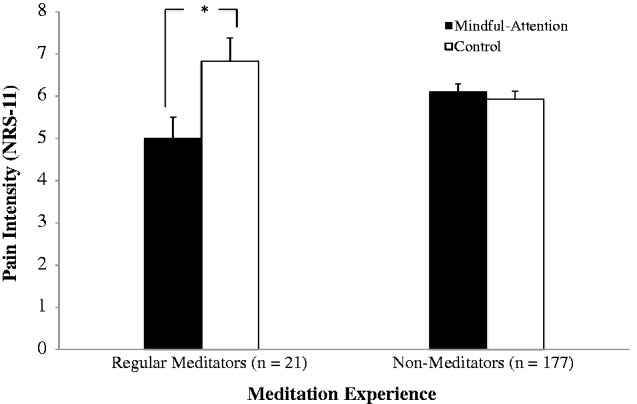
Mean pain intensity scores (NRS-11) based on experimental group and meditation experience. Error bars represent standard error. *p < .05.
Mediation of Relationship Between State Mindfulness and Pain Through Catastrophizing (Hypothesis 4)
Results of the mediation analysis showed that the total effect of state mindfulness on pain intensity was significant with a path coefficient of −.075 (SE = .023), p < .01, the direct effect of state mindfulness on pain intensity was not significant with a path coefficient of −.014 (SE = .023), p = .536, and the indirect effect of state mindfulness on pain intensity through state catastrophizing was −.061 (Boot SE = .014; 95% CI = −.091 to −.037) indicating a significant effect. A Sobel test showed that the mediation path was significantly different from zero (z = −4.43, p < .001). A summary of the path analysis can be found in Figure 2. The total effect of mindfulness on pain tolerance was not significant [.025 (SE = .029), z = .865, p = .387], the direct effect of mindfulness on pain tolerance was not significant [−.040 (SE = .034), z= −1.157, p = .247], however the indirect effect of state mindfulness on pain tolerance through state catastrophizing was significant [.067(SE = .02) 95% CI .033 to .117]. A Sobel test revealed that the mediation path was significantly different from zero (z= 3.52, p < .001).
Figure 2.
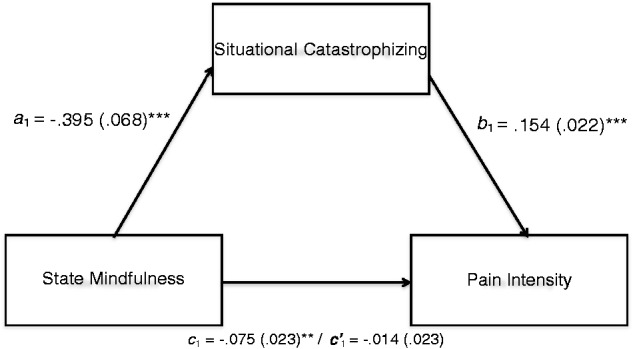
Path coefficients for the mediation model of the total, direct, and indirect effects of state mindfulness (MAAS-S) on pain intensity (NRS-11) through situational catastrophizing (SCQ). Standard errors are in parenthesis. **p < .01; ***p < .001.
Discussion
Attention-based coping strategies which direct attention away from a painful stimulus have a strong evidence-base for ameliorating acute pain in pediatric populations (Uman et al., 2008). However, as with any intervention, distraction is not effective for all youth. Researchers have found that among youth who are high in pain catastrophizing and thus view pain as highly threatening, distraction-based interventions may be less effective (Verhoeven et al., 2011). It has been proposed that given the strong demand on attention that painful sensations exert among high catastrophizers, that manipulations that direct attention towards pain in an adaptive manner may be more beneficial (Verhoeven et al., 2011). The primary purpose of this study was to examine the effects of a brief mindful attention manipulation on pain in adolescents, and to investigate whether the effects of this manipulation were moderated by adolescents’ pain catastrophizing. It was hypothesized that the manipulation would mitigate experimental pain outcomes relative to a control condition. However, results indicated that overall the manipulation had no effect on pain outcomes, and trait pain catastrophizing was not a moderator. Secondary analyses showed that adolescents’ meditation experience was a significant moderator of the effects of experimental group. This interaction was driven by the finding that adolescents with a regular meditation practice benefited from the mindful attention instructions, while those without regular meditation experience did not.
The finding that this type of brief mindful attention manipulation had no effect on experimental pain outcomes is counter to previous work in pediatric and adult populations which has found that coping strategies which direct attention towards pain in an objective and nonjudgmental manner are helpful in reducing pain and its associated distress (e.g., Hayes et al., 1999; Piira et al., 2006; Zeidan et al., 2010). One potentially important difference between the current study and previous work with pediatric populations is that participants in previous research (e.g., Petter et al., 2013; Piira et al, 2006) have received ongoing instructions throughout the pain task. However, in the current study instructions were only presented prior to the task, with participants cued to use the previously practiced skill during the pain task. This decision was made in order to reduce the potential analgesic effects of distraction that may have been provided by listening to an audio recording during the pain task. Among adolescents relatively naïve to mindfulness practice this brief manipulation appears to have provided an adequate level of instruction to reduce the use of distraction and heighten awareness of thoughts during the pain task as evidenced by our manipulation check, but was not extensive enough to provide any sort of analgesic effect.
The lack of a moderating effect of trait catastrophizing was also contrary to expectations. Theoretical work on the relationship between pain and attention has hypothesized that when pain is viewed as highly threatening that distraction-based interventions may be less effective (Eccleston & Crombez, 1999), and alternative coping strategies which direct attention towards pain may be more beneficial (Verhoeven et al., 2011). Although some researchers have found that manipulations which direct attention towards a painful stimulus are more effective among individuals high in fear of pain, and distraction is more effective among those low in fear of pain (Roelofs, Peters, van der Zijden, & Vlaeyen, 2004), findings in this field have not been consistent. For example, recent studies have found that interventions, which direct attention towards a painful stimulus in an accepting manner, are more effective than distraction when the threat value of pain was low, but not high (Jackson, Yang, Li, Chen, & Huang, 2012). In the pediatric pain field, researchers have found that the effect of attention-based coping strategies may be moderated by youth’s typical coping style. Specifically, coping strategies that are “matched” to youth’s typical coping style (i.e., using sensory-focused strategies for youth who attend to pain, and distraction for youth who prefer to distract themselves from pain) may be more effective (Fanurick et al., 1993; Piira et al., 2006), although this finding is also inconsistent (Petter et al., 2013). Given these inconsistent findings it appears possible that effectiveness of attention-based manipulations on pain outcomes are moderated by a complex interaction of biopsychosocial variables as well as features of the manipulation.
The finding that meditation experience moderated the effects of this manipulation is consistent with the argument that more practice may be necessary for individuals to benefit from mindfulness-based manipulations. Although shortened mindfulness-based interventions have been shown to reduce experimental pain among adults (Zeidan et al., 2010, 2011), evidence suggests that the more an individual engages in mindfulness-based meditation practices, the more benefits they experience from these types of interventions (Carmody & Baer, 2008). Theoretical work in the field of mindfulness has also placed a strong emphasis on meditation practice as a form of mental training which is necessary to reduce the reactive states of mind that typically dominate consciousness and can heighten distress during aversive experiences (Bishop et al., 2007). Although all individuals may have the capability to attend mindfully to present-moment experience, meditation practice may be necessary for the development of this skill (Kabat-Zinn, 1996). This finding may also be consistent with previous research that has found that “matched” coping strategies are more effective among young people (Fanurick et al., 1993; Piira et al., 2006). Specifically, youth with a meditation practice may typically direct their attention towards pain, and thus may benefit from a manipulation consistent with this tendency.
This study has potential implications for clinicians interested in the application of mindfulness-based interventions with adolescents experiencing pain. For example, if mindfulness practices are incorporated into the treatment of pain among youth it may be important for clinicians to understand that increasing awareness of physical sensations of pain and cognitive reactions to those sensations may not provide any analgesic effects until adolescents have had sufficient experience with mindfulness practice. However, it is possible that once the ability to attend mindfully has been developed, cueing may be sufficient to cause this skill to be activated during an acute pain. However, it is important to temper any conclusions regarding the clinical applications of this research given the experimental design, and the lack of a main effect for the manipulation.
Despite the finding that the mindful attention manipulation did not benefit meditation naïve adolescents, present moment awareness (i.e., state mindfulness) was found to ameliorate negative cognitive reactions to pain. Specifically, state mindfulness was a predictor of lower levels of pain intensity, and this relationship was mediated by reductions in catastrophic thinking during the task. Furthermore, although state mindfulness was not found to be associated with higher pain tolerance it was shown to have an indirect relationship with pain tolerance through state catastrophizing. These results are consistent with adult literature which has shown that present-moment awareness in the general population is associated with decreases in negative affect across a range of activities (both enjoyable and distressing; Brown, Ryan, & Creswell, 2007), and adolescent research which has found the tendency to be mindful in daily life is associated with increased psychological well-being, and decreases in somatic complaints (Greco et al., 2011). However, this is the first study in a pediatric population to demonstrate how mindfulness results in better coping during an aversive experience, showing that reductions in catastrophic thinking may be an important mechanism by which mindfulness impacts acute pain This finding is consistent with mindfulness theory, which postulates that present-moment awareness is antithetical to anxious and catastrophic thinking patterns (Bishop et al., 2004).
Although this study offers some unique findings into the effects of a brief mindfulness-based manipulation for acute pain, and the relationship between state mindfulness and experimental pain outcomes among adolescents, several limitations need to be acknowledged. First, this study was conducted with a group consisting mainly of White females recruited from the community, and it is unknown whether the observed results are generalizable outside of that population. Furthermore, the results concerning the interaction of meditation experience and the mindful attention manipulation were examined with a unique group of adolescent who attend a private school that incorporates a daily meditation practice in its curriculum, and underwent testing in their school setting rather than the laboratory. This difference in study setting represents a potential confounding factor, and combined with the relatively low number of adolescents with a regular meditation practice (n= 21), it is unclear whether these results would generalize to other adolescents with meditation experience.
Furthermore, an experimental pain task was used to study this manipulation as these paradigms offer a high degree of internal validity given that the location and duration of stimulus can be controlled. However, this may also have resulted in lower levels of catastrophizing than would be present in less predictable “real-world” pain situations, once again limiting the generalizability of the findings. Finally, although statistically significant differences were found between experimental groups on our manipulation check, the effect of the intervention appeared to be relatively weak. Once again it is possible that the intervention itself was too weak to see between group differences on other variables. Future research examining the influence of mindfulness among adolescents from more varied backgrounds and in a variety of contexts will be necessary to confirm this relationship. In addition, it will be necessary to conduct longitudinal research with meditation naïve adolescents to examine whether the development of a meditation practice leads to altered effects of manipulations such as those in the mindful attention condition.
Despite these limitations, this is the first study to examine the effects of a brief mindful attention manipulation and state mindfulness on acute experimental pain among adolescents. These results suggest that a brief mindful attention manipulation which does not offer ongoing instruction does not benefit adolescents relatively naïve to meditation, but that among adolescents with a regular meditation practice this manipulation can significantly ameliorate pain outcomes. Furthermore, this study has highlighted the impact of state mindfulness on the pain experience of adolescents, suggesting that increased state mindfulness is beneficial for adolescents undergoing acute pain, and that reductions in catastrophic thinking may be the active mechanism in this regard. Taken together, these findings suggest that future research in the field of adolescent pain directly examining the effects of more extensive mindfulness-based interventions that involve regular meditation practice is warranted. Research in this field has the potential to make a significant contribution to help researchers and clinicians assist adolescents who may have to cope with pain on a regular basis.
Acknowledgments
The authors would like to thank Bryanne Harris, Leah Wofsy, and Kynan Brown for their valuable research assistance, as well as Dr. Raymond Klein, Jonathan Fawcett, and Melanie Noel for their assistance in developing this study and manuscript.
Funding
This work was supported by a Canadian Institutes of Health Research Doctoral Award and an honorary Killam Predoctoral Scholarship to Mr. Petter. The research was supported by an IWK Health Centre Category A Research Grant, and a Dalhousie Department of Psychiatry Research Grant. Mr. Petter is also a trainee member of Pain in Child Health, a strategic research training initiative of the Canadian Institutes of Health Research. This work was also supported by a Canadian Institutes of Health Research Operating Grant and a Canada Foundation for Innovation grant awarded to Dr. Chambers. Drs. Chambers and McGrath are supported by Canada Research Chairs.
Conflicts of interest: None declared.
References
- Asmundson G J G, Noel M, Petter M, Parkerson H A. Pediatric fear- avoidance model of chronic pain: Foundation, application, and future directions. Pain Research and Management. 2012;17:397–405. doi: 10.1155/2012/908061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biegel G. The stress reduction workbook for teens: Mindfulness skills to help you deal with stress. Oakland, CA: New Harbinger Publications; 2010. [Google Scholar]
- Biegel G M, Brown K W, Shapiro S L, Schubert C M. Mindfulness-based stress reduction for the treatment of adolescent psychiatric outpatients: A randomized clinical trial. Journal of Consulting and Clinical Psychology. 2009;77:855–866. doi: 10.1037/a0016241. [DOI] [PubMed] [Google Scholar]
- Birnie K A, Noel M, Chambers C T, von Baeyer C L, Fernandez C V. The cold pressor task: Is it an ethically acceptable pain research method in children? Journal of Pediatric Psychology. 2011;36:1071–1081. doi: 10.1093/jpepsy/jsq092. [DOI] [PubMed] [Google Scholar]
- Birnie K, Petter M, Noel M, Boerner K E, Chambers C T. A systematic review of the cold pressor task in pediatric pain research. The Journal of Pain. 2012;13:817–826. doi: 10.1016/j.jpain.2012.06.005. [DOI] [PubMed] [Google Scholar]
- Bishop S R, Lau M, Shapiro S, Carlson L, Anderson N D, Carmody J, Segal Z V, Abbey S, Speca M, Velting D, Devins G. Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice. 2004;11:230–241. [Google Scholar]
- Brown K, West A, Loverich T, Biegel G. Assessing adolescent mindfulness: Validation of an adapted mindful attention awareness scale in adolescent normative and psychiatric populations. Psychological Assessment. 2011;23:1023–1033. doi: 10.1037/a0021338. [DOI] [PubMed] [Google Scholar]
- Brown K W, Ryan R M, Creswell J D. Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychological Inquiry. 2007;18:211–237. [Google Scholar]
- Campbell C, Kronfli T, Buenaver L, Smith M, Berna C, Haythornthwaite J, Edwards R. Situational versus dispositional measurement of catastrophizing: Associations with pain responses in multiple samples. The Journal of Pain. 2010;11:443–453.e2. doi: 10.1016/j.jpain.2009.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carmody J, Baer R. Relationships between mindfulness practice and levels of mindfulness, medical and psychological symptoms and well-being in a mindfulness-based stress reduction program. Journal of Behavioral Medicine. 2008;31:23–33. doi: 10.1007/s10865-007-9130-7. [DOI] [PubMed] [Google Scholar]
- Carmody J, Baer R. How long does a mindfulness-based stress reduction program need to be? A review of class contact hours and effect sizes for psychological distress. Journal of Clinical Psychology. 2009;65:627–638. doi: 10.1002/jclp.20555. [DOI] [PubMed] [Google Scholar]
- Cassidy E L, Atherton R J, Robertson N, Walsh D A, Gillett R. Mindfulness, functioning and catastrophizing after multidisciplinary pain management for chronic low back pain. Pain. 2012;153:644–650. doi: 10.1016/j.pain.2011.11.027. [DOI] [PubMed] [Google Scholar]
- Chiesa A, Serretti A. Mindfulness-based interventions for chronic pain: A systematic review of evidence. Journal of Alternative and Complimentary Medicine. 2011;17:83–93. doi: 10.1089/acm.2009.0546. [DOI] [PubMed] [Google Scholar]
- Cummings E A, Reid G J, Finley G A, McGrath P J, Ritchie J A. Prevalence and source of pain in pediatric inpatients. Pain. 1996;68:25–31. doi: 10.1016/S0304-3959(96)03163-6. [DOI] [PubMed] [Google Scholar]
- Dahl R E. Adolescent brain development: A period of vulnerabilities and opportunities. Keynote address. Annals of the New York Academy of Sciences. 2004;1021:1–22. doi: 10.1196/annals.1308.001. [DOI] [PubMed] [Google Scholar]
- Eccleston C, Crombez G. Pain demands attention: A cognitive-affective model of the interruptive function of pain. Psychological Bulletin. 1999;125:356–366. doi: 10.1037/0033-2909.125.3.356. [DOI] [PubMed] [Google Scholar]
- Enders C K. A primer on maximum likelihood algorithms available for use with missing data. Structural Equation Modeling. 2001;8:128–141. [Google Scholar]
- Fanurik D, Zeltzer L K, Roberts M C, Blount R L. The relationship between children’s coping styles and psychological interventions for cold pressor pain. Pain. 1993;53:213–222. doi: 10.1016/0304-3959(93)90083-2. [DOI] [PubMed] [Google Scholar]
- Gogtay N, Giedd J N, Lusk L, Hayashi K M, Greenstein D, Vaituzis A C, Nugent T F, 3rd, Herman D H, Clasen L S, Toga A W, Rapoport J L, Thompson P M. Dynamic mapping of human cortical development during childhood through early adulthood. Proceedings of the National Academy of Sciences of the United States of America. 2004;101:8174–8179. doi: 10.1073/pnas.0402680101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant J, Rainville P. Pain sensitivity and analgesic effects of mindful states in zen meditators: A cross-sectional study. Psychosomatic Medicine. 2009;71:106–114. doi: 10.1097/PSY.0b013e31818f52ee. [DOI] [PubMed] [Google Scholar]
- Greco L, Baer R, Smith G. Assessing mindfulness in children and adolescents: Development and validation of the child and adolescent mindfulness measure (camm) Psychological Assessment. 2011;23:606–614. doi: 10.1037/a0022819. [DOI] [PubMed] [Google Scholar]
- Hayes AF. An introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York, NY: Guilford Press; 2013. [Google Scholar]
- Hayes S C, Bissett R T, Korn Z, Zettle R D, Rosenfarb I S, Cooper L D, Grundt A M. The impact of acceptance versus control rationales on pain tolerance. The Psychological Record. 1999;49:33–47. [Google Scholar]
- IASP. Pain terms: A list with definitions and notes on usage. Recommended by the IASP subcommittee on taxonomy. Pain. 1979;6:249. [PubMed] [Google Scholar]
- Jackson T, Yang Z, Li X, Chen H, Huang X. Coping when pain is a potential threat: The efficacy of acceptance versus distraction. European Journal of Pain. 2012;16:390–400. doi: 10.1002/j.1532-2149.2011.00019.x. [DOI] [PubMed] [Google Scholar]
- Johnson M H. How does distraction work in the management of pain? Current Pain and Headache Reports. 2005;9:90–95. doi: 10.1007/s11916-005-0044-1. [DOI] [PubMed] [Google Scholar]
- Kabat-Zinn J. Full catastrophe living: How to cope with stress, pain and illness using mindfulness meditation. London, UK: Piatkus; 1996. [Google Scholar]
- Kabat-Zinn J. Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice. 2003;10:144–156. [Google Scholar]
- McCracken L, Keogh E. Acceptance, mindfulness, and values-based action may counteract fear and avoidance of emotions in chronic pain: An analysis of anxiety sensitivity. The Journal of Pain. 2009;10:408–415. doi: 10.1016/j.jpain.2008.09.015. [DOI] [PubMed] [Google Scholar]
- Noel M, Petter M, Parker J A, Chambers C T. Cognitive behavioral therapy for pediatric chronic pain: The problem, research, and practice. Journal of Cognitive Psychotherapy. 2012;26:143. [Google Scholar]
- Perquin C W, Hazebroek-Kampschreur A A J M, Hunfeld J A M, Bohnen A M, van Suijlekom-Smit L W A, Passchier J, van der Wouden J C. Pain in children and adolescents: A common experience. Pain. 2000;87:51–58. doi: 10.1016/S0304-3959(00)00269-4. [DOI] [PubMed] [Google Scholar]
- Petter M, Chambers C T, Chorney J M L. Comparing distraction and mindfulness-based attention for cold-pressor pain in children. Pain Research and Management. 2013;18:39–45. doi: 10.1155/2013/857045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petter M, Chambers C T, McGrath P J, Dick B D. The role of trait mindfulness in the pain experience of adolescents. The Journal of Pain. 2013;14:1709–1718. doi: 10.1016/j.jpain.2013.08.015. [DOI] [PubMed] [Google Scholar]
- Piira T, Hayes B, Goodenough B, von Baeyer C L. Effects of attentional direction, age, and coping style on cold-pressor pain in children. Behaviour Research and Therapy. 2006;44:835–848. doi: 10.1016/j.brat.2005.03.013. [DOI] [PubMed] [Google Scholar]
- Roelofs J, Peters M L, van der Zijden M, Vlaeyen J W. Does fear of pain moderate the effects of sensory focusing and distraction on cold pressor pain in pain-free individuals? The Journal of Pain. 2004;5:250–256. doi: 10.1016/j.jpain.2004.04.001. [DOI] [PubMed] [Google Scholar]
- Semple R J, Lee J, Miller L F. Mindfulness-based cognitive therapy for children. In: Baer R A, editor. Mindfulness-based treatment approaches: Clinician's guide to evidence base and applications. San Diego, CA: Elsevier Academic Press; 2006. pp. 143–166. [Google Scholar]
- Sullivan M J L, Bishop S R, Pivik J. The pain catastrophizing scale: Development and validation. Psychological Assessment. 7:524–532. [Google Scholar]
- Uman L S, Chambers C T, McGrath P J, Kisely S. A systematic review of randomized controlled trials examining psychological interventions for needlerelated procedural pain and distress in children and adolescents: An abbreviated Cochrane review. Journal of Pediatric Psychology. 2008;33:842–854. doi: 10.1093/jpepsy/jsn031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verhoeven K, Goubert L, Jaaniste T, Van Ryckeghem D M, Crombez G. Pain catastrophizing influences the use and effectiveness of distraction in schoolchildren. European Journal of Pain. 2011;16:256–267. doi: 10.1016/j.ejpain.2011.06.015. [DOI] [PubMed] [Google Scholar]
- von Baeyer C, Spagrud L, McCormick J, Choo E, Neville K, Connelly M. Three new datasets supporting use of the numerical rating scale (NRS-11) for children's self-reports of pain intensity. Pain. 2009;143:223–227. doi: 10.1016/j.pain.2009.03.002. [DOI] [PubMed] [Google Scholar]
- Zeidan F, Gordon N S, Merchant J, Goolkasian P. The effects of brief mindfulness meditation training on experimentally induced pain. The Journal of Pain. 2010;11:199–209. doi: 10.1016/j.jpain.2009.07.015. [DOI] [PubMed] [Google Scholar]
- Zeidan F, Grant J A, Brown C A, McHaffie J G, Coghill R C. Mindfulness meditation-related pain relief: Evidence for unique brain mechanisms in the regulation of pain. Neuroscience Letters. 2012;520:165–173. doi: 10.1016/j.neulet.2012.03.082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeidan F, Martucci K, Kraft R, Gordon N, McHaffie J, Coghill R. Brain mechanisms supporting the modulation of pain by mindfulness meditation. The Journal of Neuroscience. 2011;31:5540–5548. doi: 10.1523/JNEUROSCI.5791-10.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]