

Abstract
Background
Burnout syndrome can be defined as long-term work stress resulting from the interaction between constant emotional pressure associated with intense interpersonal involvement for long periods of time and personal characteristics. We investigated the prevalence/propensity of Burnout syndrome in clinical nurses, and the factors related to Burnout syndrome-associated such as socio-demographic characteristics, work load, social and family life, leisure activities, extra work activities, physical activities, and work-related health problems.
Method
We conducted a cross-sectional, quantitative, prospective epidemiological study with 188 surgical clinic nurses. We used the Maslach Burnout Inventory (MBI), which is a socio-demographic questionnaire and the most widely used instrument to assess Burnout syndrome (three basic dimensions: emotional exhaustion, despersonalization and professional underachievement). The socio-demographic profile questionnaire wascomposed of questions regarding identification, training, time at work, work characteristics and personal circumstances.
Results
The prevalence of Burnout syndrome was higher (10.1%) and 55, 4% of subjects had a propensity to develop this syndrome. The analysis of the socio-demographic profile of the nurse sample studied showed that most nurses were childless married women, over 35 years of age, working the day shift for 36 hours weekly on average, with 2-6 years of post-graduation experience, and without extra employments. Factors such as marital status, work load, emotion and work related stress aggravated the onset of the syndrome.
Conclusion
The prevalence and propensity of Burnout syndrome were high. Some factors identified can be useful for the adoption of preventive actions in order to decrease the prevalence of the clinical nurses Burnout syndrome.
Keywords: Burnout, Professional, Syndrome, Nursing
Background
Nurses are commonly exposed to stress due to work overcharge [1-3]. In this context, Burnout syndrome can be defined as long-term work stress resulting from the interaction between constant emotional pressure associated with intense interpersonal involvement for long periods of time and personal characteristics. Frequent Burnout syndrome symptoms include emotional exhaustion and development of negative attitudes and feelings towards work colleagues as well as to their own professional achievement [4].
Even though, Burnout syndrome is detected in professionals from various areas, prevalence is particularly high in service and care workers, especially health and care ones [5]. Among those, nurses have been the subject of several studies, because they experience constant stressful labor situations, working in direct contact with patients who have different expectations and degrees of suffering. For instance, a study conducted in Europe in 2011 showed that approximately 30% of nurses surveyed reported being exhausted or fatigued due to work activities [6,7]. In addition, a British study found that approximately 42% of nurses in England reported to be suffering from Burnout, whereas in Greece approximately 44% of nurses reported a feeling of dissatisfaction at work and a desire to leave work. Lower prevalence was reported in a survey in Germany, which estimated that 4.2% of that worker population was affected by Burnout [6-8].
However, few studies in Brazil have investigated only nurses. In most cases, the number of professionals in the institutions investigated is relatively small, leading to the joint study of nurses, technicians, and assistants, whose professional activities differ in nature, complexity, and emotional overload. Thus, it is difficult to determine the exact prevalence of this condition among nurses in Brazil. Moreover, studies on Burnout syndrome in Brazil have largely overlooked high-quality institutions that constantly strive to obtain health care quality certifications. Thus, it is not known, for instance, whether the prevalence of the syndrome among nurses in high-quality institutions differs from that observed in other institutions. That knowledge is necessary to identify factors associated with the onset of the syndrome and to develop plans for prevention and control.
In this study, we investigated the prevalence/propensity of Burnout syndrome in clinical nurses, and the factors related to Burnout syndrome associated, such as socio-demographic characteristics, work load, social and family life, leisure activities, extra work activities, physical activities, and work-related health problems. Nurses with and without Burnout syndrome, or Burnout propensity were compared.
Methods
We conducted a cross-sectional, quantitative, prospective epidemiological study with 188 surgical clinic nurses. The study was conducted from August to October 2012. One individual refused to participate in the study, and twelve nurses were on sick leave. The study site is a large private hospital in the city of São Paulo, considered the best hospital in Latin America and a benchmark in quality and excellence [9].
We used the Maslach Burnout Inventory (MBI), which is a socio-demographic questionnaire and the most widely used instrument to assess Burnout syndrome [10].
The MBI assesses how workers experienced their work, according to three conceptual dimensions: emotional exhaustion, depersonalization and personal accomplishments. The most widely used version of the MBI was established in 1986, it began to be used only for the evaluation of the frequency, since the existence of high correlation between the two scales was detected, and many studies found higher correlation (r = 0.80) [11-13].
The internal consistency of the three dimensions of the inventory is satisfactory, as it has a Cronbach’s alpha ranging from 0.71 to 0.90 and test-retest coefficients ranging from 0.60 to 0.80 in periods of up to one month [14].
In Brazil there were several attempts to translate, adapt and validate the MBI, since the researchers were concerned with overcoming the limitations of the low internal consistencies of the factors depersonalization and personal accomplishments, however, the MBI has been applied in more than 90% of the studies on Burnout worldwide [15]. According to some authors, there was success in the development of MBI as a tool for the assessment of Burnout in Brazil as indices of reliability Alpha Cronbach’s of 0.8014 [16-18].
The Maslach Burnout Inventory (MBI) assesses three basic dimensions: emotional exhaustion (low: scores lower than 19; intermediate: 19–26; and high: scores greater than 27); depersonalization (low: scores lower than 6; intermediate: 6–9; and high: scores greater than 10); and professional underachievement, which is inverse to the former two dimensions (low: scores greater than 40; intermediate: 34–49; and high: scores lower than or equal to 33) [19]. The socio-demographic profile questionnaire is composed of a set of close-ended, multiple-choice, and open-ended questions, covering different spheres of life of the subject: identification (sex, marital status, age, children), training, time at work, work characteristics (employment status, time at work, other jobs, number of working hours per day, shift, weekly rest, work impressions, pleasant and unpleasant work attributes), personal circumstances (work related health problems, non-work related activities, dedication to family on weekends, symptoms, and a self-assessment on stress).
The questionnaires were administered after nurses had signed the informed consent form and approved by the Ethical Committee in Research (CAAE n° 04793112.4.3001.0071).
The data were described by absolute frequencies and percentages. The comparisons between genders and work shifts were performed using Pearson’s chi-square test or Fisher’s exact test in cases where expected frequencies were lower than five. The analyses were performed using SPSS statistical software (SPSS Inc. Released 2008. SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc.). Significance level was set at 5%.
Results
High prevalence of Burnout syndrome
The detection of the three dimensions that characterize Burnout syndrome (concurrent emotional tiredness, depersonalization, and professional underachievement) or of one or two of those dimensions (indicative of predisposition to the syndrome) is shown in Figure 1. Approximately 10% of the studied population had Burnout syndrome, and over half the nurses interviewed had a propensity to develop the syndrome (presence of one or two dimensions). We observed the prevalence, in decreasing order, of high emotional exhaustion, professional underachievement, and depersonalization.
Figure 1.
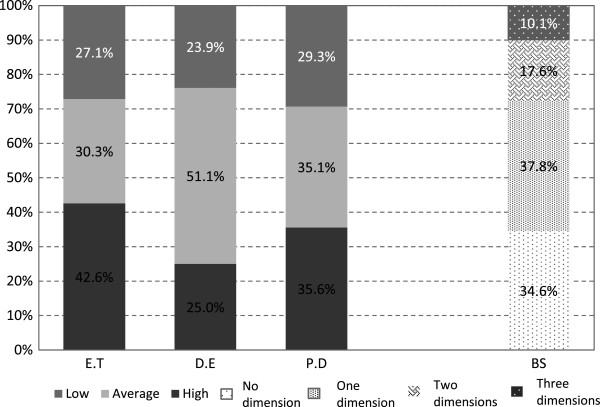
Burnout syndrome dimensions in clinical nurses from August to October 2012 at Albert Einstein Jewish Hospital, São Paulo, Brazil. ET = Emotional tiredness. DE = Depersonalization. PD = Professional underachievement. BS = Burnout syndrome.
The analysis of the socio-demographic profile of the nurse population studied showed that most nurses were childless married women, over 35 years of age, with knowledge of Burnout syndrome, working the day shift and 36 hours weekly on average, with 2-6 years since graduation, and without additional employments (Table 1).
Table 1.
Socio-demographic characteristics of clinical nurses from August to October 2012 at Albert Einstein Jewish Hospital, São Paulo, Brazil
| Variables | n (%) |
|---|---|
|
Sex |
|
|
Man |
31 (16) |
|
Woman |
137 (83) |
|
Age |
|
|
20 a 25 |
17 (9) |
|
26 a 30 |
54 (29) |
|
31 a 35 |
55 (29) |
|
35+ |
62 (33) |
|
Work shift |
|
|
Day |
111 (59) |
|
Night |
77 (41) |
|
Marital status |
|
|
Married |
103 (55) |
|
Single |
71 (38) |
|
Separated |
3 (2) |
|
Divorced |
10 (5) |
|
Widowed |
1 (0.5) |
|
Children |
|
|
Yes |
84 (45) |
|
No |
104 (55) |
|
Time since graduation (years) |
|
|
< 2 |
17 (9) |
|
2–6 |
80 (43) |
|
7–9 |
73 (39) |
|
> 20 |
18 (10) |
|
Work hours |
|
|
36 |
172 (92) |
|
> 36 |
16 (9) |
|
The nurse has other employment |
|
|
Yes |
15 (8) |
| No | 173 (92) |
Table 2 also shows that most subjects interviewed did not have other activities other than work, with no or rare weekends devoted exclusively to family, leisure activities, and social life. Regarding the prevalence of work-related diseases, most subjects reported having no problems. Among the subjects who reported having health problems, the main work-related health complaints were musculoskeletal pain and emotional complaints.
Table 2.
Extra-work activities, health problems, and health complaints reported by clinical nurses from August to October 2012 at Albert Einstein Jewish Hospital, São Paulo, Brazil
| Variables | n (%) |
|---|---|
| Extra-work activities |
|
|
YES |
87 (46) |
|
NO |
101 (54) |
| Which ones? |
|
| Sport |
36 (41) |
| Leisure |
6 (7) |
| Voluntary and religious activities |
4 (2) |
| Home |
18 (20) |
| Education |
28 (30) |
| Other |
11 (13) |
| Health problems |
|
| YES |
50 (27) |
|
NO |
136 (73) |
| Work related health complaints |
|
| Musculoskeletal pain |
24 (48) |
| Emotional complaints |
20 (40) |
| Headache |
7 (14) |
| Other |
7 (14) |
| Did not answer | 1 (2) |
Comparisons between subjects with Burnout propensity and Burnout syndrome and subjects without Burnout syndrome
According to Table 3 the simultaneous presence of the three dimensions (emotional exhaustion, depersonalization, and professional underachievement) indicates the occurrence of Burnout syndrome, whereas the presence of one or two dimensions indicates a propensity to develop the syndrome, which has a great impact on the work activity and worker life. The proportion of women was higher in subjects with Burnout propensity than in subjects without the syndrome, but no significant differences were observed between the two groups (p = 0.169).
Table 3.
Comparisons between subjects with Burnout propensity and Burnout syndrome and subjects without Burnout syndrome and demographiccharacteristics, work aloud and health problems from August to October 2012 at Albert Einstein Jewish Hospital, São Paulo, Brazil
| |
Dimension classification |
|
||||||
|---|---|---|---|---|---|---|---|---|
| |
No dimension |
Propensity |
P |
Burnout |
p | |||
| N | % | N | % | N | % | |||
|
Sex |
|
|||||||
| Man |
14 |
45,2 |
14 |
45,2 |
0,169 |
3 |
9,7 |
0,751 |
| Woman |
51 |
32,5 |
90 |
57,3 |
16 |
10,2 |
||
|
Work shift |
|
|||||||
| Day |
46 |
41,4 |
55 |
49,5 |
0,021 |
10 |
9,0 |
0,140 |
| Night |
19 |
24,7 |
49 |
63,6 |
9 |
11,7 |
||
|
Age |
|
|||||||
| 20 a 25 yrs |
4 |
23,5 |
9 |
52,9 |
0,290 |
4 |
23,5 |
0,249 |
| 26 a 30 yrs |
15 |
27,8 |
35 |
64,8 |
4 |
7,4 |
||
| 31 a 35 yrs |
19 |
34,5 |
30 |
54,5 |
6 |
10,9 |
||
| ➢ 35 yrs |
27 |
43,5 |
30 |
48,4 |
5 |
8,1 |
||
|
Marital status |
|
|||||||
| Married |
41 |
39,8 |
53 |
51,5 |
0,007 |
9 |
8,7 |
0,327 |
| Single |
15 |
21,1 |
47 |
66,2 |
9 |
12,7 |
||
| Separeted |
2 |
66,7 |
1 |
33,3 |
0 |
0,0 |
||
| Divorced |
6 |
60,0 |
3 |
30,0 |
1 |
10,0 |
||
| Widove |
1 |
100,0 |
0 |
0,0 |
0 |
0,0 |
||
|
Children |
|
|||||||
| No |
32 |
30,8 |
60 |
57,7 |
0,283 |
12 |
11,5 |
0,285 |
| Yes |
33 |
39,3 |
44 |
52,4 |
7 |
8,3 |
||
|
Weekly hours |
|
|||||||
| 36 hrs |
56 |
33,3 |
93 |
55,4 |
0,995 |
19 |
11,3 |
0,327 |
| Others workload |
6 |
37,5 |
10 |
62,5 |
0 |
0,0 |
||
|
Weekends are devoted exclusively to family, social life and lesure activities |
|
|||||||
| Never |
1 |
25,0 |
2 |
50,0 |
0,411 |
1 |
25,0 |
0,089 |
| Rarely or few times |
30 |
29,1 |
59 |
57,3 |
14 |
13,6 |
||
| Several times or almost always |
19 |
38,8 |
28 |
57,1 |
2 |
4,1 |
||
| Always |
15 |
46,9 |
15 |
46,9 |
2 |
6,3 |
||
|
Others employment |
|
|||||||
| No |
58 |
33,5 |
98 |
56,6 |
0,235 |
17 |
9,8 |
>0,99 |
| Yes |
7 |
46,7 |
6 |
40,0 |
2 |
13,3 |
||
|
Extra- work activities |
|
|||||||
| No |
41 |
40,6 |
46 |
45,5 |
0,017 |
14 |
13,9 |
0,392 |
| Yes |
24 |
27,6 |
58 |
66,7 |
5 |
5,7 |
||
|
Performance of physical activities |
|
|||||||
| No |
12 |
23,5 |
35 |
68,6 |
0,389 |
4 |
7,8 |
0,343 |
| Yes |
12 |
33,3 |
23 |
63,9 |
1 |
2,8 |
||
|
Work- related health problems |
|
|||||||
| No |
55 |
40,4 |
72 |
52,9 |
0,038 |
9 |
6,6 |
0,002 |
| Yes |
10 |
20,0 |
30 |
60,0 |
10 |
20,0 |
||
|
Pain |
|
|||||||
| No pain complaint |
60 |
37,3 |
87 |
54,0 |
0,380 |
14 |
8,7 |
0,073 |
| One pain complaint |
3 |
17,6 |
11 |
64,7 |
3 |
17,6 |
||
| Two pain complaints |
2 |
25,0 |
4 |
50,0 |
2 |
25,0 |
||
| Three pain complaints |
0 |
0,0 |
0 |
0,0 |
0 |
0,0 |
||
|
Emotional complaints |
|
|||||||
| No emotional complaints |
64 |
38,6 |
88 |
53,0 |
0,022 |
14 |
8,4 |
0,002 |
| One emotional complaint |
1 |
7,7 |
10 |
76,9 |
2 |
15,4 |
||
| Two or more emotional complaints |
0 |
0,0 |
4 |
57,1 |
3 |
42,9 |
||
|
Education activities |
|
|||||||
| No |
19 |
31,7 |
39 |
65,0 |
0,280 |
2 |
3,3 |
0,112 |
| Yes |
5 |
18,5 |
19 |
70,4 |
3 |
11,1 |
||
|
Home activities |
|
|||||||
| No |
21 |
30,4% |
44 |
63,8 |
0,370 | 4 |
5,8% |
0,553 |
| Yes | 3 | 16,7 | 14 | 77,8 | 1 | 5,6 | ||
Propensity = 1 or 2 dimensions.
Burnout syndrome = 3 dimensions.
Propensity = 1 or 2 dimensions.
Burnout syndrome = 3 dimensions.
Bold is significant.
The proportion of subjects who work the night shift was higher in subjects with Burnout propensity than in subjects without the syndrome (p = 0.021).
The proportion of singles was higher in subjects with a propensity to develop the syndrome than in subjects without the syndrome (p = 0.007).
The proportion of nurses who have extra-work activities was higher in subjects with Burnout propensity that in subjects without the syndrome (p = 0.017).
The number of emotional complaints was higher in subjects with Burnout syndrome (p = 0.002) and Burnout propensity (p = 0.022) than in subjects without the syndrome.
The proportion of nurses with work related health problems was higher in subjects with Burnout than in those without the syndrome (p = 0.002).
As expected, the frequency of work related health problems differed significantly among the number of dimensions identified and was greater in subjects with Burnout syndrome. It should be noted that approximately 40% of subjects who reported having no health problems also showed no Burnout dimensions. Similarly, and as expected, we found a significant positive association between the number of emotional complaints and the incidence of Burnout (p= 0.038).
The number of subjects who perform physical activities was higher in subjects with Burnout propensity than in subjects without the syndrome, but no significant differences were observed (p = 0.389).
The number of subjects who never dedicate their weekends to family, leisure activities, and social life was higher in subjects with Burnout propensity than in subjects without the syndrome, but no significant differences were observed (p = 0.411).
Discussion
This study aimed to evaluate the prevalence of Burnout syndrome in a large sample of clinical nurses and possible socio-demographic factors and activities associated with the syndrome. Our results indicate that the prevalence of Burnout syndrome is high in this sample, which was predominantly composed of childless, women without additional employments, who rarely or occasionally dedicated weekends to family, leisure activities, and social life. Moreover, most subjects did not participate in educational or sport activities in addition to work, and reported having frequent health and emotional complaints.
This is the first study to establish the prevalence of Burnout syndrome in a group of Brazilian population composed exclusively of clinical nurses working in a hospital of renowned quality, with quality certifications for nursing professionals. Thus, our results should be useful for defining the behavior of the syndrome and possible changes in prevalence due to the adoption of specific prevention measures. Those measures should be beneficial not only to the individuals affected, but also to their health institutions as Burnout syndrome directly affects healthcare organizations, harming the quality of services and increasing the rate of dissatisfaction and absenteeism.
The prevalence of Burnout in this study was10.1% higher than in previous studies conducted in Brazil that range from 0 to 4.7% [8-10] and 49.7% in international studies [16-18].
One possible explanation for this difference is the heterogeneity of the sample population in previous studies, which included not only nurses, but also technicians and assistants. Because of the differences in work functions, in addition to the fact that they work at different hospital areas, the prevalence of Burnout may also differ among these professionals, negating a direct comparison with prevalence rates observed in this study, whose sample consisted of clinical nurses only.
It should also be noted that the nurses at the institution evaluated perform several activities after work hours and have to attend 53 hours of courses annually, in addition to participate in congresses and intra-sectoral audits.
This accumulation of tasks may determine the short time devoted to family, leisure activities, and social life, resulting in dissatisfaction, feelings of guilt and helplessness, reducing self-esteem and, at a more advanced stage, professional achievement.
The prevalence rate of Burnout was 10,1% in our sample population, our results also showed that more than half of the interviewees (55,4%) had a propensity to develop Burnout syndrome, especially among single, childless subjects.
The fact that most of the sample population was composed of women over 35 years of age may have influenced this result, because of the possible occurrence of feelings of inferiority and frustration in light of current cultural standards that still consider married women with children to be happier and more complete. Moreover, the lack of support and comfort from family may contribute to excessive dedication to work, thus increasing the propensity to Burnout.
Our results also indicate that the frequency of emotional and health (mainly musculoskeletal pain) complaints was, as expected, higher in individuals affected by the syndrome. These findings are consistent with the high rates of sick leave associated with Burnout, and confirm the expectation that the emotional stress generated by the complexity of nursing work and the direct contact with patients who experience different degrees of suffering and have different expectations can lead to emotional overload in these professionals [19,20].
We also observed that the propensity to develop the syndrome was higher among nurses working the night shift – an expected result considering that these professionals have no regular sleeping and eating patterns. Moreover, feelings of inadequacy may be present, because while everyone else is working, this professional sleeps, performing his/her activities outside the regular routine adopted by society. Thus, the creation of flexible work schedules and measures to adopt a different policy for professionals who work at night could help reduce the prevalence of the syndrome.
Regarding the factors that may help prevent Burnout such as physical activity, we observed no significant differences in the propensity (or prevalence) of Burnout between nurses who performed and did not perform such activities. Even though physical activity is associated with numerous health benefits, it can become another burden for individuals burdened with other work activities.
It is not possible to establish a causal relationship between the frequency of sports practice and the prevalence of Burnout because of the retrospective nature of our study and the possibility that this factor may interact with other factors that were not analyzed. Thus, we believe that sports should be encouraged in a healthy way, so that they can be recognized as a source of pleasure and satisfaction.
We also observed that a higher frequency of educational and home activities were associated with the propensity to develop the syndrome. This result is consistent with the notion that such activities could represent an additional study and work overload for these professionals, negatively affecting – at least in the short term – their physical and emotional health. Thus, individuals who also study and manage their homes may not perceive the positive aspects of these additional activities, and consider their work stressful.
This study has some limitations. Even though the onset of Burnout is a consequence of the interaction between stress and constant work overload and personal, lifestyle, and personality traits, this study did not evaluate individual variables such as how subjects perceive work and their expectations towards work, as well as personal and personality traits that tend to prevent Burnout. Thus, future studies that evaluate such characteristics may provide subsidies for the development of prevention strategies that consider both institutional measures and personal and lifestyle interventions to be made by each professional.
Conclusion
The prevalence and propensity for Burnout syndrome was higher specially among women, single and childless subjects. Regarding the individuals who suffer from Burnout syndrome a direct connection was made to health problems related to work. Individuals who did not have any dimension did not report any health problems associated with work.
Working during night, being single and developing activities outside the work was present in individuals who were prone to the syndrome.
Emotional complaints were present in both: Burnout and propensity.
Physicaly active female individual who dedicated time to family and social life were equally as prone to the condition as those who did not and showed no significant statistical difference.
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors participated in the acquisition of data and revision of the manuscript. All authors determined the design, interpreted the data and drafted the manuscript. All authors read and gave final approval for the version submitted for publication.
Contributor Information
Vivian F Ribeiro, Email: vifinotti@yahoo.com.br.
Celso Ferreira Filho, Email: ferreira-celso@uol.com.br.
Vitor E Valenti, Email: vitor.valenti@marilia.unesp.br.
Marcelo Ferreira, Email: marceloferreira@gmail.com.
Luiz Carlos de Abreu, Email: luizcarlos@usp.br.
Tatiana Dias de Carvalho, Email: carvalho.td1@gmail.com.
Valdelias Xavier, Email: eliasfisio@uol.com.br.
JapyAngeli de Oliveira Filho, Email: japyoliveira@epm.br.
Pedro Gregory, Email: gregoryp@gmail.com.
Eliseth Ribeiro Leão, Email: eliseth.leao@einstein.br.
Natascha G Francisco, Email: franciscong@yahoo.com.
Celso Ferreira, Email: celsoferreira@epm.br.
Acknowledgements
The funding body provided financial support to make all procedures and in the decision to submit the manuscript for publication.
References
- Godoy MT, Bouttelet D. Rethinking the care provided to nursing woman. J Hum Growth Dev. 2004;14:63–68. [Google Scholar]
- Mello DF, Rocha SM, Scochi CG, Lima RA. The nursing care to preterm and low birth weight infant in home follow up. J Hum Growth Dev. 2000;10:49–60. [Google Scholar]
- Madeira LM. The child’s discharge: implications for nursing. J Hum Growth Dev. 1994;4:5–11. [Google Scholar]
- Carlotto MS, Palazzo LS. Burnout syndrome and associated factors: an epidemiologic study of teachers. Cad Saúde Pública. 2006;22:1017–1026. doi: 10.1590/s0102-311x2006000500014. [DOI] [PubMed] [Google Scholar]
- Nogueira MCF, Ramalho MA. Study in psychology. Maringa. 2007;12:123–132. [Google Scholar]
- Sermeus W, Linda HA, Koen VH, Anne MR, Peter G, Moreno-Casbas MT. RN4CAST consortium. BMC Nurs. 2011;10:6. doi: 10.1186/1472-6955-10-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galindo RH, Feliciano KVO, Lima RAS, Souza AI. Burnout syndrome among nurses in a general hospital in the city of Recife. Rev Esc Enferm. 2012;46:420–427. doi: 10.1590/S0080-62342012000200021. [DOI] [PubMed] [Google Scholar]
- Moreira DS, Magnano R, Sakae TM, Magajewski FRL. Prevalence of the syndrome of Burnout in nursing from a large hospital in southern Brazil. CadsaúdePública. 2009;25:1559–1568. doi: 10.1590/s0102-311x2009000700014. [DOI] [PubMed] [Google Scholar]
- Franca FM, Ferrari R. Burnout syndrome and sócio demographic nursing staff. Acta Paul Enferm. 2009;22:192–197. doi: 10.1590/S0103-21002009000200012. [DOI] [Google Scholar]
- Lautert L. The professional burnout: empirical study with nurses work in hospitals. Gaúcha de Enfermagem. 1997;18:133–144. [PubMed] [Google Scholar]
- Porto GG, Carneiro SC, Vasconcelos BC, Nascimento MM, Leal JL. Burnout syndrome in oral and maxillofacial surgeons: a critical analysis. Int J Oral Maxillofac Surg. 2014;12:S0901-5027(14)00062-9. doi: 10.1016/j.ijom.2013.10.025. [DOI] [PubMed] [Google Scholar]
- Tamayo MR. Federal Universityof Paraíba (Org.), III Congresso Norte-Nordeste de Psicologia 2003. Anais. João Pessoa: UFPB; 2003. Validation of the Maslach Burnout Inventory. [Abstract] [Google Scholar]
- Carlotto MS, Câmara SG. Factor analysis of the Maslach Burnout Inventory (MBI) in a sample of teachers from private institutions. Stud Psychol. 2004;9:499–505. [Google Scholar]
- Maslach C. Understanding Burnout. Cienc Trab. 2009;11:37–43. [Google Scholar]
- Schaufeli WB, Enzmann D. The Burnout Campanionto Study and Practice: A Critical Analysis. London: Taylor and Francis; 1998. [Google Scholar]
- Albaladejo R, Villanueva R, Ortega P, Astasio P, Calle ME, Domingues V. Síndrome Del Burnout em El persona de enfermeria em um hospital de Madrid. Rev Espanõla Salud Pública. 2004;78:506–516. doi: 10.1590/s1135-57272004000400008. [DOI] [PubMed] [Google Scholar]
- Poghosyan L, Clarke SP, Finlayson M, Aiken LH. Nurse Burnout and qualyt of care: cross- national investigation in six countries. Res Nursing Health. 2010;33:288–298. doi: 10.1002/nur.20383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanrahan NP, Aiken LH, McClaine L, Hanlon AL. Relationship between psychiatric nurse work environment and nurse Burnout in acute care general hospital. Issues Mental Health Nur. 2010;31:198–207. doi: 10.3109/01612840903200068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gómez MMN, Dodino CN, Aponte CF, Caycedo CE, Riveros MP, Martinez MPM. Relationship between psychological profile, quality of life and stress em person nursing care. Rev Univers Psych. 2005;4:63–75. [Google Scholar]
- Hertel R. Burnout and theme d-surg nurse. Med-Surg Matters. 2009;18:1. [Google Scholar]