

Abstract
Objective
To perform a more sophisticated analysis of previously published data that advances the understanding of the efficacy of pedestrian countdown signal (PCS) installation on pedestrian-motor vehicle collisions (PMVCs), in the city of Toronto, Canada.
Methods
This is an updated analysis of the same dataset from Camden et al. A quasi-experimental design was used to evaluate the effect of PCS on PMVC. A Poisson regression analysis, using a one-group comparison of PMVC, pre-PCS installation to post-PCS installation was used, controlling for season and temporal effects. The outcome was the frequency of reported PMVC (January 2000–December 2009). Similar models were used to analyse specific types of collisions defined by age of pedestrian, injury severity, and pedestrian and vehicle action. Incidence rate ratios with 95% CI are presented.
Results
This analysis included 9262 PMVC, 2760 during or after PCS installation, at 1965 intersections. There was a 26% increase in the rate of collisions, pre to post-PCS installation (incidence rate ratio=1.26, 95% CI 1.11 to 1.42).
Conclusions
The installation of PCS at 1965 signalised intersections in the city of Toronto resulted in an increase in PMVC rates post-PCS installation. PCSs may have an unintended consequence of increasing pedestrian-motor vehicle collisions in some settings.
Introduction
In 2005–2006, there were 6708 emergency room visits and 967 hospitalisations for pedestrian injuries in Ontario.1 In addition, 342 pedestrians were killed by motor vehicle collisions across Canada.2 In 2010, there were 2159 reported pedestrian collisions in Toronto, of which 973 occurred at intersections.3 Pedestrian countdown signals (PCSs) are modifications to traditional pedestrian crossing signals that provide a digital countdown of the seconds remaining to cross the street at intersections. The installation of PCS in the City of Toronto was to provide supplemental information to pedestrians to assist with street crossing, not to provide motor vehicles with information to change driving behaviour in relation to traffic signals.4 The policy implications if PCSs are effective are considerable, given that they are a relatively inexpensive retrofit into many traffic environments. Other municipalities (eg, New York City) are installing thousands of PCSs with the stated intent to reduce pedestrian injuries.5
A previous analysis of the City of Toronto dataset used in this paper with the same senior author, found a null effect of PCSs on the rate of pedestrian-motor vehicle collisions (PMVCs).6 The previous analysis was performed without controlling for temporal effects or adjusting for seasonality. This was a limitation of the original analysis, given the potential for secular trends within the 10-year data collection period. In addition, there are considerable differences in vehicle and pedestrian traffic flow and visibility by season, particularly within the winter months. In this paper, we present an updated analysis of the same dataset from Camden et al.6 This reanalysis demonstrates the value of controlling for potential confounders to enhance the interpretation and understanding of the efficacy of PCS installation for injury prevention.
This study examined the frequency of PMVC before and after installation of PCS in the City of Toronto over a 10-year period. The main objective was to determine whether PCSs were associated with any change in PMVCs, controlling for seasonal and temporal effects. The potential for benefit exists if pedestrians use the PCS timer displays to make safer road crossing decisions. Conversely, the potential for harm exists if PCSs cause pedestrians to rush or drivers to accelerate in response to the timer display. Either possibility may enhance the likelihood of a collision.
Methods
The study took place in the City of Toronto, Canada. Intersections with traffic signals where PCSs were installed during the study period (January 2000–December 2009) were eligible for inclusion. Data were extracted from MVC police reports filed by the City of Toronto, Transportation Services Division. Records were excluded: (1) if the collision occurred on private property or inside a parking lot (2) if the collision occurred before a traditional signal was installed at the intersection; (3) if the collision occurred outside a 30-metre radius of the intersection; (4) if the collision occurred on the same day of PCS installation; (5) if the collision occurred at an intersection with less than 6 months duration between the installation of the traditional traffic signal and the PCS; (6) if the associated location code (eg, intersection/mid-block) was missing. The ethics review board at the Hospital for Sick Children provided ethics approval.
All police-reported PMVCs were mapped onto City of Toronto street centre lines using ArcGIS, ArcMap V.10. ArcGIS was used to match collision data to intersections where PCS were installed. The unit of analysis was intersection-month. The outcome of interest was the number of reported PMVCs. Covariates included year, season and baseline PMVC rate. Specific analysis was conducted with respect to age, injury severity, pedestrian right-of-way and vehicle action (a turning vehicle compared with vehicle moving through the intersection). Age was categorised as children and youth (ages 0–15 years), adults (ages 16–59 years) and older adults (ages >60 years).7 Injury severity was categorised based on Toronto Police Service injury classification: no injury; minimal injury (no medical attention); minor injury (emergency department treatment only); major injury (hospital admission); and fatal injury. Previous research shows misclassification of injury severity by police report most commonly involves minor injury.8–10 Therefore, minimal and minor injury classifications were combined. Major and fatal injuries were also combined due to the low number of fatal injuries. Season was categorised as summer (April–September) or winter (October–March). Right of way and vehicle action was determined by police report. Vehicle action was coded as either a turning or a throughway collision.
Statistical analysis
Statistical analyses were completed using PROC GENMOD in SAS V.9.3. To determine the effectiveness of PCSs, a comparison between pre-PCS installation to post-PCS installation was examined based on incidence rate ratios (IRRs). The unit of analysis was intersection-month, using preinstallation as the reference condition. The data from 2007–2009 formed the basis of this analysis; therefore, each intersection provided observations before and after PCS installation. For each intersection and season, the preinstallation monthly average count of all collisions from the previous 7 years (2000–2006) was determined. These averages were used as a covariate for the observations from 2007–2009 for the corresponding intersection and season. The other covariates were year of observation as a discrete variable (2007, 2008, 2009), and season (summer, winter). A repeated measures Poisson regression model was used to estimate the IRR of collisions per intersection-month, with 95% confidence intervals (CIs). Generalised estimating equations with an exchangeable correlation structure were used to fit the models. Analyses of specific types of collisions, defined by the age of the pedestrian, injury severity, and pedestrian and vehicle action were performed using similar models. The level of statistical significance was set a priori, at 5%.
Results
Pedestrian countdown signals
During the study period (November 2007–December 2009), 2078 PCSs were installed in the City of Toronto. Twenty-six (26.1%) per cent of the PCSs were installed in 2007; 69.8% in 2008; and 4.0% in 2009. In total, 113 intersections were excluded because the time period between the installation of the PCS and the traditional traffic signal was less than 6 months. This left a total of 1965 intersections included in the analysis.
Pedestrian-motor vehicle collisions
There were 23 428 PMVCs reported during the 10-year study period. Collisions excluded were: (1) parking lot or private property collisions (n=289), (2) collisions occurring prior to the installation of a traditional traffic signal (n=385), (3) collisions occurring outside a 30-meter buffer area of PCS installation (n=10 486), (4) collisions occurring the same day as the PCS installation (n=3), (5) collisions at intersections with less than 6 months between the installation of PCS from a traditional traffic signal (n=19), and (6) collisions with the associated location code missing (n=2984). The final dataset included 9262 collisions. There were 226 records with missing data for age; these were excluded from the age-specific analysis. There were a total of 2760 PMVCs included in the analysis of the data from 2007–2009. Figure 1 shows the rate of all collisions per 100-intersection-month (IM) from 2000–2006 and 2007–2009. Table 1 provides the overall frequency of collisions by PCS installation (pre, post) and by season (summer, winter), together with IRRs and 95% CIs. Table 2 summarises the IRRs of collisions by age, injury severity, pedestrian and vehicle action, post-PCS installation.
Figure 1.
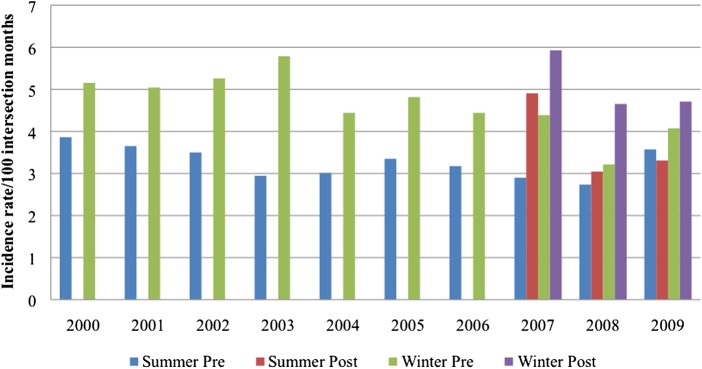
Incidence rates of all pedestrian-motor vehicle collisions in the City of Toronto, 2000–2009.
Table 1.
Frequency and incidence rate ratios of all collisions by pedestrian countdown signal (PCS) installation (pre, post) and by season (summer, winter)
| Collision type | Total I-M* | I-M (≥1 collision) | # of collisions | IRR(95% CI) (adjusted for covariates)† | p Value |
|---|---|---|---|---|---|
| All collisions | |||||
| Pre-PCS | 42 904 | 935 | 1023 | 1 | |
| Post-PCS | 29 619 | 1548 | 1737 | 1.26 (1.11 to 1.42) | <0.001 |
| Summer | 36 406 | 1041 | 1142 | 1 | |
| Winter | 36 117 | 1442 | 1618 | 1.19 (1.09 to 1.31) | <0.001 |
*Intersection-months.
†Covariates include: year, season and baseline pedestrian-motor vehicle rate.
IRR, incidence rate ratio.
Table 2.
Incidence rate ratios of collisions by age, injury severity, pedestrian and vehicle action, post-pedestrian countdown signal (PCS) installation
| Collision type | Adjusted* IRR (95% CI) | p Value |
|---|---|---|
| Total | 1.26 (1.11 to 1.42) | <0.001 |
| Age, years | ||
| Child (0–15 years) | 0.96 (0.69 to 1.33) | 0.797 |
| Adult (16–59 years) | 1.34 (1.15 to 1.56) | <0.001 |
| Older adult (>59 years) | 1.14 (0.88 to 1.49) | 0.321 |
| Injury severity | ||
| No injury | 0.95 (0.55 to 1.63) | 0.850 |
| Minor or minimal | 1.25 (1.09 to 1.42) | 0.001 |
| Fatal or major | 1.51 (1.06 to 2.16) | 0.023 |
| Pedestrian crossing | ||
| Right of way | 1.19 (1.03 to 1.38) | 0.019 |
| Without right of way | 1.30 (0.98 to 1.74) | 0.078 |
| Vehicle crossing | ||
| Right turn (PED† ROW‡) | 1.20 (0.937 to 1.54) | 0.149 |
| Right turn (No PED ROW) | 1.26 (0.569 to 2.78) | 0.568 |
| Left turn (PED ROW) | 1.01(0.914 to 1.32) | 0.314 |
| Left turn (No PED ROW) | 1.11 (0.575 to 2.15) | 0.755 |
| Straight (PED ROW) | 1.70 (1.09 to 2.64) | 0.025 |
| Straight (No PED ROW) | 1.34 (0.996 to 1.80) | 0.057 |
*Adjusted for temporal effects, season and baseline average pedestrian-motor vehicle rate.
†Pedestrian.
‡Right of way.
IRR, incidence rate ratio; PED, Pedestrian.
Overall, there was a 26% increase in the rate of collisions, pre-PCS installation to post-PCS installation (IRR=1.26, 95% CI 1.11 to 1.42). There was also an increase in the rate of collisions by season, where the winter months demonstrated a 19% increase in collision rate (IRR=1.19, 95% CI 1.09 to 1.31). The majority of collisions (n=1955) involved adults (ages 16–59 years), where there was a 34% increase in the rate of collisions, pre-PCS installation to post-PCS installation (IRR=1.34, 95% CI 1.15 to 1.56). There were statistically significant increases in the rate of collisions, post-PCS installation, for minor/minimal injury (IRR=1.25, 95% CI 1.09 to 1.42) and major/fatal injury (IRR=1.51, 95% CI; 1.06 to 2.16). There was a statistically significant increase in collision rate with pedestrian crossing, in right of way crossing (IRR=1.19, 95% CI 1.03 to 1.38) and statistically insignificant increases in non-right of way crossing (IRR=1.30, 95% CI 0.98 to 1.74). Finally, statistically significant increases in collision rates were observed for vehicles proceeding straight through the intersection (IRR=1.70, 95% CI 1.09 to 2.64), but not for any other type of vehicle crossing.
Discussion
The reanalyses of these data presents a more sophisticated statistical modelling approach than the model previously published. The original analysis by Camden et al6 failed to account for temporal and seasonal effects. The analytical approach used in this paper, controlling for temporal and seasonal effects, as well as baseline PMVC rates, enhances the interpretation of the data by allowing an unbiased assessment of the effect of PCS installation, in the city of Toronto.
This analysis demonstrated an increase in PMVC rates of 26% at intersections, post-PCS installation. The increase in PMVC rate was more pronounced in adults, and for severe and fatal collisions. These results controlled for baseline PMVC rate, season, as well as installation year.
These observations may be explained if the driver, the pedestrian, or both are choosing to enter an intersection when there is inadequate time for safe crossing. If pedestrians are hurrying, they may fail to adequately assess the traffic environment, or may complete the crossing during a ‘no walking’ phase. If drivers are hurrying, they may also fail to assess the environment, and/or increase their speed. Pedestrians may also perceive that the remaining posted time is sufficient for crossing, or make hasty decisions knowing the time required between light changes. To save time, pedestrians may assume a larger risk of crossing with less time available.
Our findings are inconsistent with the previous literature. Markowitz et al11 reported a decline in collisions with a similar decline in the control group, where they reported a 52% reduction in collisions post-PCS installation. This finding however, was based on the analysis of nine high collision intersections; effect size may have been partly due to a regression to the mean effect.11 An estimated baseline collision history was considered in the present study; and the differences in intersections with high versus low collision rates were accounted for in the analysis. Pulugurtha et al12 reported a decline in collision rate and found PCSs are most effective at high crash and high volume intersections. This may explain the differences in the effect size of PCS installation between studies. While PCSs appear to have an overall impact in the city of Toronto, it is possible that the effect of PCS is different by city. In our previous work,6 we reported an analysis of the same dataset and did not find a statistically significant effect from the installation of countdown timers.6 In that analysis, all of the intersection time from 2000 to 2006 was treated as uniform ‘preinstallation’ time, whereas the current analysis treats those years as baseline and draws pre–post comparisons within the 2007–2009 time period only. The current analysis also controls for season and reports specific analyses for age, injury severity, and vehicle and pedestrian action. Although the present analysis contradicts previous studies, we believe it to be the least biased estimate based on a large sample of actual collision data. We also believe that this type of enhanced modelling that controls for potential bias from temporal and seasonal effects, should be used in future research with these types of data.
Limitations of the present study include the non-randomised design, and the different traffic environments within the City of Toronto. In addition, reliable data on vehicle speed, vehicle volume and pedestrian volume were not available. Pedestrian countdown timers may have had effects on vehicle and pedestrian flow. For example, if pedestrians are entering the intersection later in the crossing phase they may block drivers intending either left or right turns, and this may change traffic flow. In addition, either more or fewer pedestrians may choose to use an intersection with a timer rather than crossing elsewhere. The overall effect observed may be absent or opposite in other traffic settings. We were not able to measure or control for the change in driver or pedestrian behaviour, pre-PCS installation to post-PCS installation, however, the collision rate increased equally for pedestrians with and without right of way. In addition, statistically significant increases in collision rates were seen for vehicles proceeding straight through the intersection, but not for turning vehicles.
Environmental modifications such as PCSs may be effective at providing additional information for pedestrians while crossing intersections if they require limited public education or regulatory enforcement of behaviour. If behaviour change in response to these signals is dangerous, the signals themselves can be modified. For example, lights could be reprogrammed to allow multidirectional pedestrian crossing with vehicles at a stopped position, or the timers could end earlier for pedestrians. An optimum pattern for signal use may vary across time and across location based on differing travel patterns; however, excessive complexity or variability in traffic signals may itself contribute to risk.
The optimal method to evaluate the effects of changes in traffic signals on collision rates is with randomised designs. Because the potential for harm has been demonstrated with this analysis, it is important that such an evaluation be carried out as rigorously as possible.
What is already known on the subject.
There are few studies that have examined the relationship between pedestrian countdown signals (PCSs) and pedestrian-motor vehicle collisions.
Previous work in this area has demonstrated inconsistent findings related to the safety benefit of PCS installation.
Previous work with these data, not controlling for season or temporal effects, suggested no increased benefit or harm with the installation of PCS.
What this study adds.
This is a reanalysis of population-based data that describes the effectiveness of PCS at reducing pedestrian-motor vehicle collisions, over a 10-year period.
The present study provides evidence that suggests potential harm related to PCS installation.
Rigorous evaluation of public health interventions such as the installation of PCS that are designed to reduce the impact of pedestrian-motor vehicle collisions should be conducted, alongside implementation of changes in traffic signals that may affect pedestrian safety.
Acknowledgments
The authors would like to thank Michael P Brady (City of Toronto) for providing the data, in addition to his assistance. We would also like to acknowledge Ben Escott for his contribution to the data configurations that contributed to this analysis.
Correction notice: This article has been made Open Access since published Online First.
Contributors: SAR: assisted with interpretation of the data, writing and editing of the manuscript, and final approval and submission of the version to be published. ARW: analysis and interpretation of data, revision of the manuscript, final approval of the version to be published. LR and AC: assisted with interpretation of the data, revision of the manuscript, and final approval and submission of the version to be published. RB: original conception and design, involved in GIS data processing, revision of the manuscript, final approval of the version to be published. CM: original conception and design, revision of the manuscript, final approval of the version to be published. AH: original conception and design, writing and revision of the manuscript, final approval of the version to be published.
Funding: Funding for this work was provided by a Canadian Institute for Health Research Operating Grant: Population Health Intervention Research (SEC-117116).
Competing interests: None.
Ethics approval: Ethics approval was provided by the ethics review board of the Hospital for Sick Children.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Ontario Injury Prevention Resource Centre. Pedestrian Injuries. 2009. [cited 9 September 2013]. http://www.oninjuryresources.ca/downloads/compass/2009-03-0ICompass-pedestrians5.pdf. [Google Scholar]
- 2. Transport Canada. Canadian Motor Vehicle Traffic Collision Statistics: 2009. [cited 9 September 2013]. http://www.tc.gc.ca/eng/roadsafety/tp-tp3322-2009-1173.htm#t3. [Google Scholar]
- 3. City of Toronto. Pedestrian Collision Summary Leaflet – December 2010. 2011. Transportation Services, Traffic Management Centre, Traffic Safety Unit. [cited 9 September 2013]. http://www.toronto.ca/transportation/publications/brochures/2010_ped.pdf. [Google Scholar]
- 4.City of Toronto. Traffic—Pedestrian countdown signals. Toronto, ON: [cited 29 May 2013] http://www.toronto.ca/transportation/traffic/countdown_signals.htm [Google Scholar]
- 5.Solomonow S. NYC DOT announces installation of pedestrian countdown signals at high pedestrian crah locations. 2011. [cited 25 March 2013]. http://www.nyc.gov/html/dot/html/pr2011/pr11_32.shtml
- 6.Camden A, Buliung R, Rothman L, et al. The impact of pedestrian countdown signals on pedestrian-motor vehicle collisions: a quasi-experimental study. Inj Prev 2012;18:210–15 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. World Health Organization. Global Status Report on Safety: Time for Action. 2009. [cited 9 September 2013]. http://whqlibdoc.who.int/publications/2009/9789241563840_eng.pdf. [Google Scholar]
- 8.Agran PF, Castillo DN, Winn DG. Limitations of data compiled from police reports on pediatric pedestrian and bicycle motor vehicle events. Accid Anal Prev 1990;22:361–70 [DOI] [PubMed] [Google Scholar]
- 9.Rosman DL, Knuiman MW. A comparison of hospital and police road injury data. Accid Anal Prev 1994;26:215–22 [DOI] [PubMed] [Google Scholar]
- 10.Sciortino S, Vassar M, Radetsky M, et al. San Francisco pedestrian injury surveillance: mapping, under-reporting, and injury severity in police and hospital records. Accid Anal Prev 2005;37:1102–13 [DOI] [PubMed] [Google Scholar]
- 11.Markowitz F, Sciortino S, Fleck J, et al. Pedestrian countdown signals: experience with an extensive pilot installation. Institute of Transporation Engineers, 2006 [Google Scholar]
- 12.Pulugurtha SS, Desai A, Pulugurtha NM. Are pedestrian countdown signals effective in reducing crashes? Traffic Inj Prev 2010;11:632–41 [DOI] [PubMed] [Google Scholar]